
Fluorescence Imaging Using Enzyme-Activatable Probes for Detecting Diabetic Kidney Disease and Glomerular Diseases

 , and
, and
Abstract
:1. Introduction
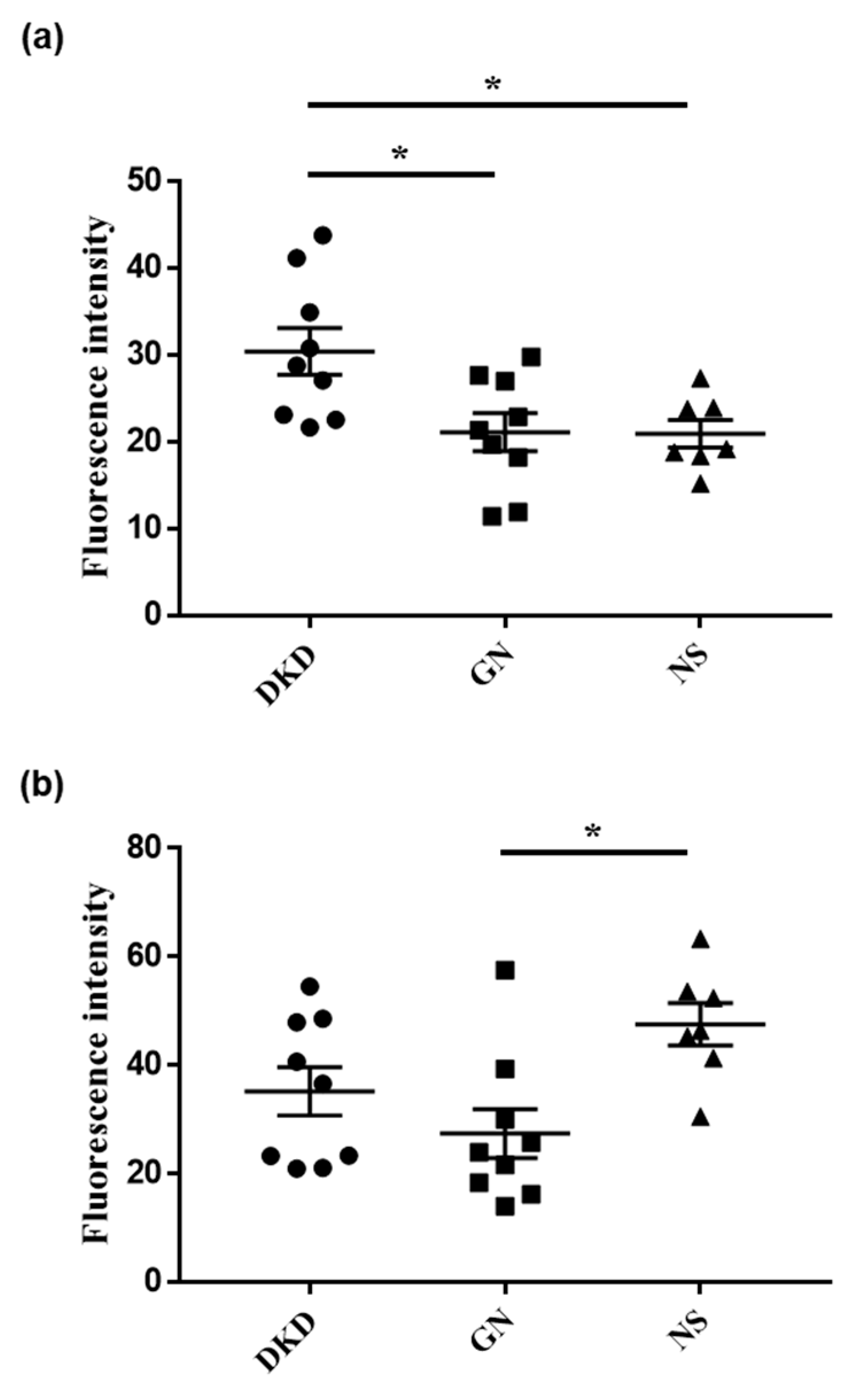
2. Results
3. Discussion
4. Materials and Methods
4.1. Study Population
4.2. Activatable Fluorescent Probe
4.3. Fluorescence Imaging
4.4. Statistical Analysis
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Xie, Y.; Bowe, B.; Mokdad, A.H.; Xian, H.; Yan, Y.; Li, T.; Maddukuri, G.; Tsai, C.Y.; Floyd, T.; Al-Aly, Z. Analysis of the Global Burden of Disease study highlights the global, regional, and national trends of chronic kidney disease epidemiology from 1990 to 2016. Kidney Int. 2018, 94, 567–581. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takata, T.; Isomoto, H. Pleiotropic Effects of Sodium-Glucose Cotransporter-2 Inhibitors: Renoprotective Mechanisms beyond Glycemic Control. Int. J. Mol. Sci. 2021, 22, 4374. [Google Scholar] [CrossRef] [PubMed]
- Takata, T.; Koda, M.; Sugihara, T.; Sugihara, S.; Okamoto, T.; Miyoshi, K.; Matono, T.; Hosho, K.; Mae, Y.; Iyama, T.; et al. Renal shear wave velocity by acoustic radiation force impulse did not reflect advanced renal impairment. Nephrology 2015, 21, 1056–1062. [Google Scholar] [CrossRef]
- Urano, Y.; Sakabe, M.; Kosaka, N.; Ogawa, M.; Mitsunaga, M.; Asanuma, D.; Kamiya, M.; Young, M.R.; Nagano, T.; Choyke, P.L.; et al. Rapid Cancer Detection by Topically Spraying a γ-Glutamyltranspeptidase–Activated Fluorescent Probe. Sci. Transl. Med. 2011, 3, 110ra119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Onoyama, H.; Kamiya, M.; Kuriki, Y.; Komatsu, T.; Abe, H.; Tsuji, Y.; Yagi, K.; Yamagata, Y.; Aikou, S.; Nishida, M.; et al. Rapid and sensitive detection of early esophageal squamous cell carcinoma with fluorescence probe targeting dipeptidylpeptidase IV. Sci. Rep. 2016, 6, 26399. [Google Scholar] [CrossRef] [PubMed]
- Sinha, N.; Kumar, V.; Puri, V.; Nada, R.; Rastogi, A.; Jha, V.; Puri, S. Urinary exosomes: Potential biomarkers for diabetic nephropathy. Nephrology 2020, 25, 881–887. [Google Scholar] [CrossRef] [Green Version]
- Brondani, L.d.A.; Soares, A.A.; Recamonde-Mendoza, M.; Dall’Agnol, A.; Camargo, J.L.; Monteiro, K.M.; Silveiro, S.P. Urinary peptidomics and bioinformatics for the detection of diabetic kidney disease. Sci. Rep. 2020, 10, 1242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miyata, Y.; Ishizawa, T.; Kamiya, M.; Yamashita, S.; Hasegawa, K.; Ushiku, A.; Shibahara, J.; Fukayama, M.; Urano, Y.; Kokudo, N. Intraoperative imaging of hepatic cancers using γ-glutamyltranspeptidase-specific fluorophore enabling real-time identification and estimation of recurrence. Sci. Rep. 2017, 7, 3542. [Google Scholar] [CrossRef]
- Ueo, H.; Shinden, Y.; Tobo, T.; Gamachi, A.; Udo, M.; Komatsu, H.; Nambara, S.; Saito, T.; Ueda, M.; Hirata, H.; et al. Rapid intraoperative visualization of breast lesions with γ-glutamyl hydroxymethyl rhodamine green. Sci. Rep. 2015, 5, 12080. [Google Scholar] [CrossRef]
- Iyama, T.; Takata, T.; Yamada, K.; Mae, Y.; Taniguchi, S.; Ida, A.; Ogawa, M.; Yamamoto, M.; Hamada, S.; Fukuda, S.; et al. A novel method for assessing the renal biopsy specimens using an activatable fluorescent probe. Sci. Rep. 2020, 10, 12094. [Google Scholar] [CrossRef]
- Marcelino, P.; Tavares, I.; Carvalho, D.; Marques, C.; Silvestre, M.J.; Perdigoto, R.; Barroso, E. Is Urinary γ-Glutamyl Transpeptidase Superior to Urinary Neutrophil Gelatinase–Associated Lipocalin for Early Prediction of Acute Kidney Injury After Liver Transplantation? Transplant. Proc. 2014, 46, 1812–1818. [Google Scholar] [CrossRef] [PubMed]
- Endre, Z.H.; Pickering, J.W.; Walker, R.J.; Devarajan, P.; Edelstein, C.L.; Bonventre, J.V.; Frampton, C.M.; Bennett, M.R.; Ma, Q.; Sabbisetti, V.S.; et al. Improved performance of urinary biomarkers of acute kidney injury in the critically ill by stratification for injury duration and baseline renal function. Kidney Int. 2011, 79, 1119–1130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yilmaz, M.I.; Turgut, F.; Kanbay, M.; Saglam, M.; Sonmez, A.; Yaman, H.; Demirbas, S.; Unal, H.U.; Gok, M.; Karaman, M.; et al. Serum gamma-glutamyltransferase levels are inversely related to endothelial function in chronic kidney disease. Int. Urol. Nephrol. 2013, 45, 1071–1078. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.Y.; Han, K.; Yu, J.H.; Park, S.; Heo, J.-I.; Seo, J.A.; Kim, N.H.; Yoo, H.J.; Kim, S.G.; Kim, S.M.; et al. Gamma-glutamyl transferase variability can predict the development of end-stage of renal disease: A nationwide population-based study. Sci. Rep. 2020, 10, 11668. [Google Scholar] [CrossRef]
- Gupta, S.; Sen, U. More than just an enzyme: Dipeptidyl peptidase-4 (DPP-4) and its association with diabetic kidney remodelling. Pharmacol. Res. 2019, 147, 104391. [Google Scholar] [CrossRef]
- Yang, J.; Campitelli, J.; Hu, G.; Lin, Y.; Luo, J.; Xue, C. Increase in DPP-IV in the intestine, liver and kidney of the rat treated with high fat diet and streptozotocin. Life Sci. 2007, 81, 272–279. [Google Scholar] [CrossRef]
- Nargis, T.; Kumar, K.; Ghosh, A.R.; Sharma, A.; Rudra, D.; Sen, D.; Chakrabarti, S.; Mukhopadhyay, S.; Ganguly, D.; Chakrabarti, P. KLK5 induces shedding of DPP4 from circulatory Th17 cells in type 2 diabetes. Mol. Metab. 2017, 6, 1529–1539. [Google Scholar] [CrossRef]
- Sun, A.L.; Deng, J.T.; Guan, G.J.; Chen, S.H.; Liu, Y.T.; Cheng, J.; Li, Z.W.; Zhuang, X.H.; Sun, F.D.; Deng, H.P. Dipeptidyl peptidase-IV is a potential molecular biomarker in diabetic kidney disease. Diabetes Vasc. Dis. Res. 2012, 9, 301–308. [Google Scholar] [CrossRef] [Green Version]
- Singh, G.; Massak, M.; Czaplicki, M.; Young, E.; Sharma, S.; Chang, A.; Bhanushali, A.; Anand, P. Use of a Smartphone Camera at the Bedside to Assess Adequacy of Kidney Biopsies. J. Am. Soc. Nephrol. 2021, 32, 3024–3026. [Google Scholar] [CrossRef]
- Iyama, T.; Takata, T.; Koda, M.; Fukuda, S.; Hoi, S.; Mae, Y.; Fukui, T.; Munemura, C.; Isomoto, H. Renal shear wave elastography for the assessment of nephron hypertrophy: A cross-sectional study in chronic kidney disease. J. Med. Ultrason. 2018, 45, 571–576. [Google Scholar] [CrossRef] [Green Version]
- Mae, Y.; Takata, T.; Ida, A.; Ogawa, M.; Taniguchi, S.; Yamamoto, M.; Iyama, T.; Fukuda, S.; Isomoto, H. Prognostic Value of Neutrophil-To-Lymphocyte Ratio and Platelet-To-Lymphocyte Ratio for Renal Outcomes in Patients with Rapidly Progressive Glomerulonephritis. J. Clin. Med. 2020, 9, 1128. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All | DM (+) | |
|---|---|---|
| Number | 102 | 25 |
| Sex (male/female) | 59/43 | 19/6 |
| Age, years | 55.3 ± 20.7 | 62.5 ± 13.0 |
| Body mass index, kg/m2 | 23.3 ± 4.2 | 25.8 ± 5.1 |
| Creatinine, mg/dL | 0.93 (0.38–8.71) | 1.10 (0.45–8.71) |
| estimated GFR, mL/min/1.73 m2 | 61.6 ± 32.3 | 47.9 ± 26.8 |
| Urinary protein, g/day | 0.93 (0.05–16.47) | 1.79 (0.20–10.52) |
| Histological diagnosis | ||
| Glomerulonephritis, n | 76 | 9 |
| Nephrosclerosis, n | 17 | 9 |
| Diabetic kidney disease, n | 9 | 7 |
| GGT-HMRG | DPP-HMRG | |||
|---|---|---|---|---|
| r | p-Value | r | p-Value | |
| Age, years | 0.041 | 0.69 | 0.133 | 0.18 |
| Body mass index, kg/m2 | 0.121 | 0.26 | 0.010 | 0.93 |
| eGFR, mL/min/1.73 m2 | 0.030 | 0.77 | −0.086 | 0.39 |
| Urinary protein, g/day | 0.039 | 0.70 | 0.180 | 0.072 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yamada, K.; Takata, T.; Iyama, T.; Hamada, S.; Mae, Y.; Sugihara, T.; Isomoto, H. Fluorescence Imaging Using Enzyme-Activatable Probes for Detecting Diabetic Kidney Disease and Glomerular Diseases. Int. J. Mol. Sci. 2022, 23, 8150. https://doi.org/10.3390/ijms23158150
Yamada K, Takata T, Iyama T, Hamada S, Mae Y, Sugihara T, Isomoto H. Fluorescence Imaging Using Enzyme-Activatable Probes for Detecting Diabetic Kidney Disease and Glomerular Diseases. International Journal of Molecular Sciences. 2022; 23(15):8150. https://doi.org/10.3390/ijms23158150
Chicago/Turabian StyleYamada, Kentaro, Tomoaki Takata, Takuji Iyama, Shintaro Hamada, Yukari Mae, Takaaki Sugihara, and Hajime Isomoto. 2022. "Fluorescence Imaging Using Enzyme-Activatable Probes for Detecting Diabetic Kidney Disease and Glomerular Diseases" International Journal of Molecular Sciences 23, no. 15: 8150. https://doi.org/10.3390/ijms23158150