
Specific Local Predictors That Reflect the Tropism of Endometriosis—A Multiple Immunohistochemistry Technique

 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
1.1. Clinical Characteristics and Risk Factors Related to Endometriosis
1.2. Morphopathological Features of Endometriosis
2. Objectives
3. Results
3.1. Associated Symptomatology Analysis: Pain and Infertility
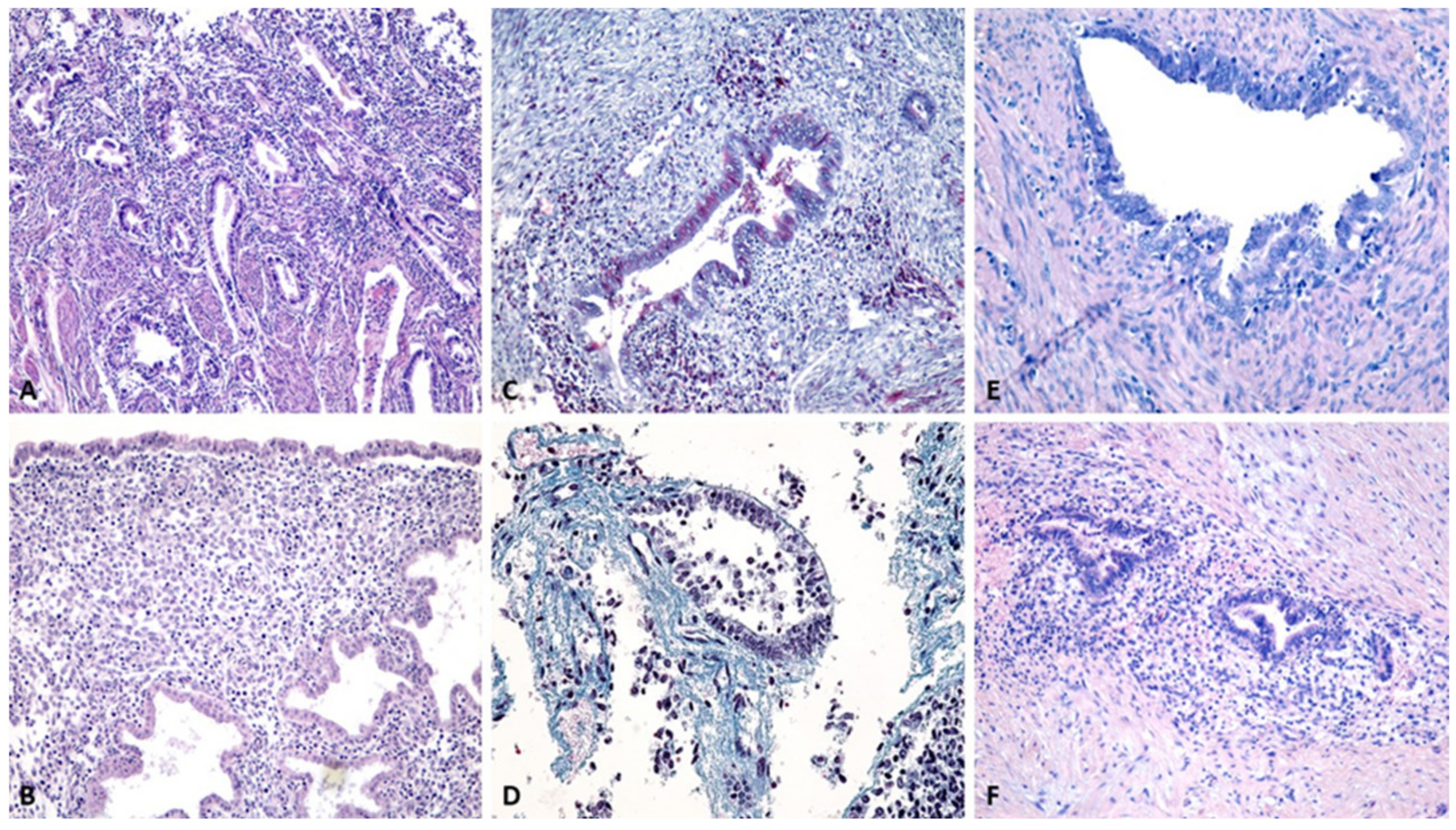
3.2. Evaluation by Classical Histopathological Staining Methods
3.3. Histopathological Characterization by Single Immunohistochemistry
3.3.1. Cytokeratin Reactivity Analysis
3.3.2. Hormone Receptor Reactivity Analysis
3.4. Stromal Vascularization Analysis
3.5. Analysis of Cell Proliferation and Involvement of Tumor Proteins
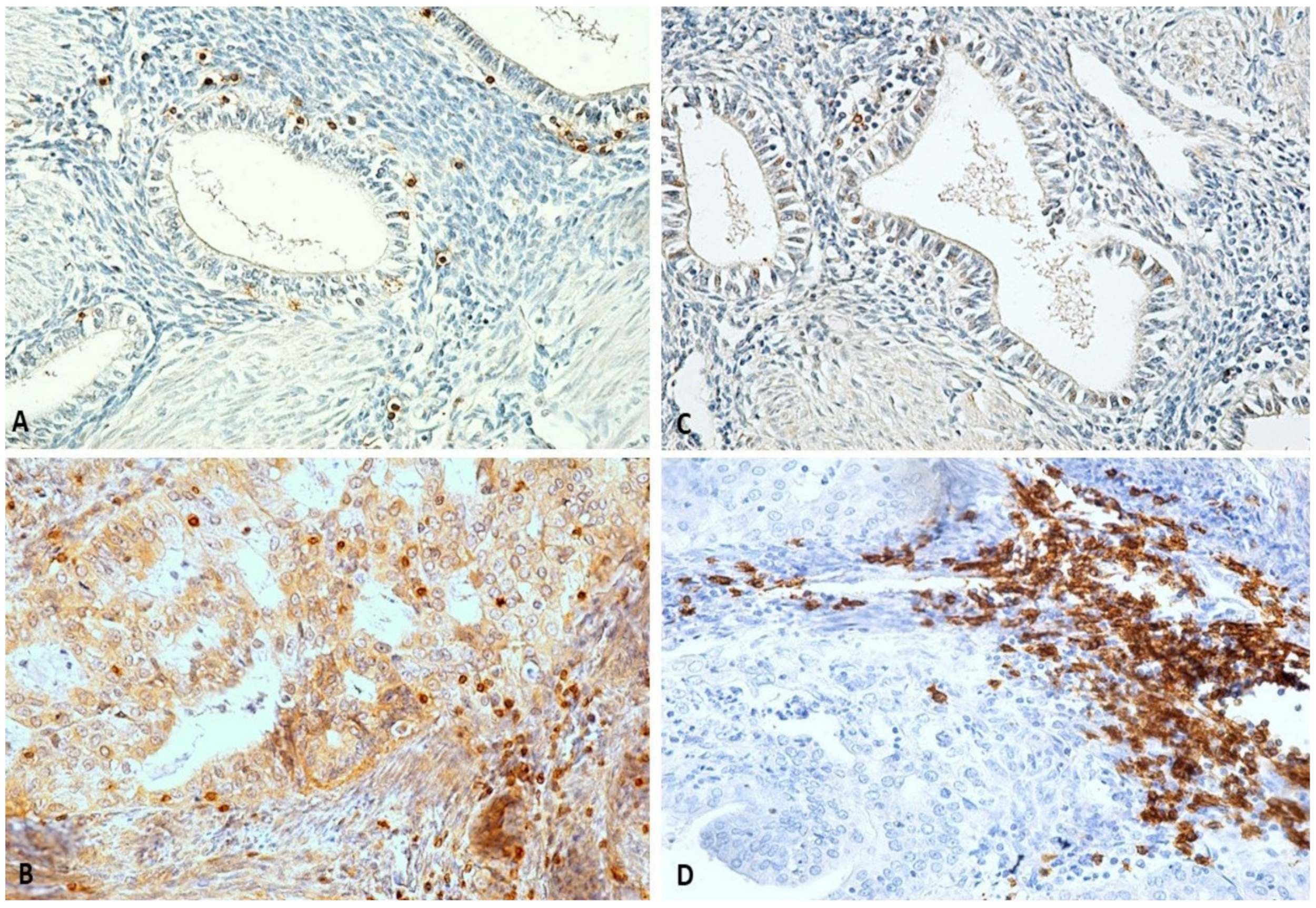
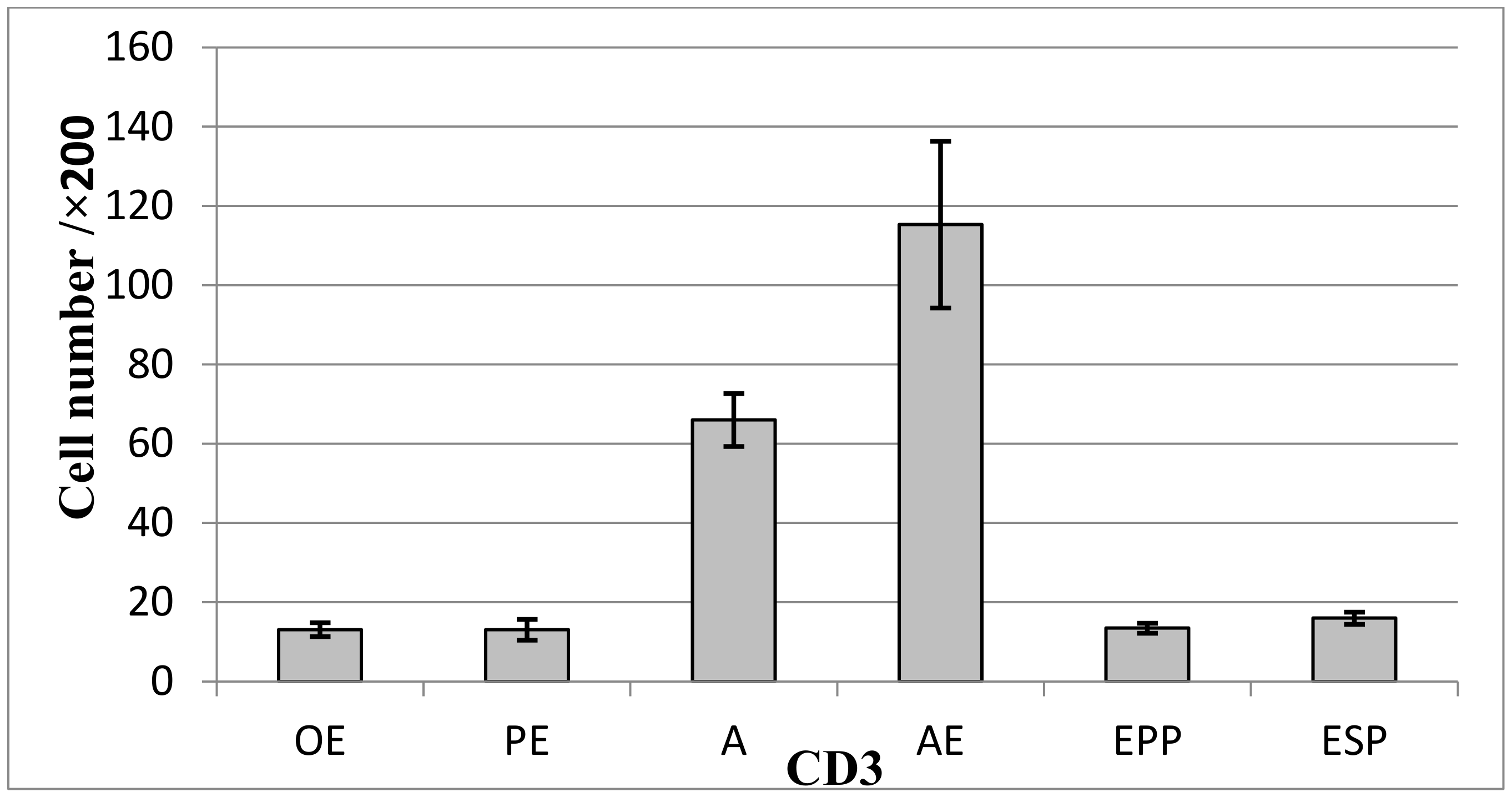
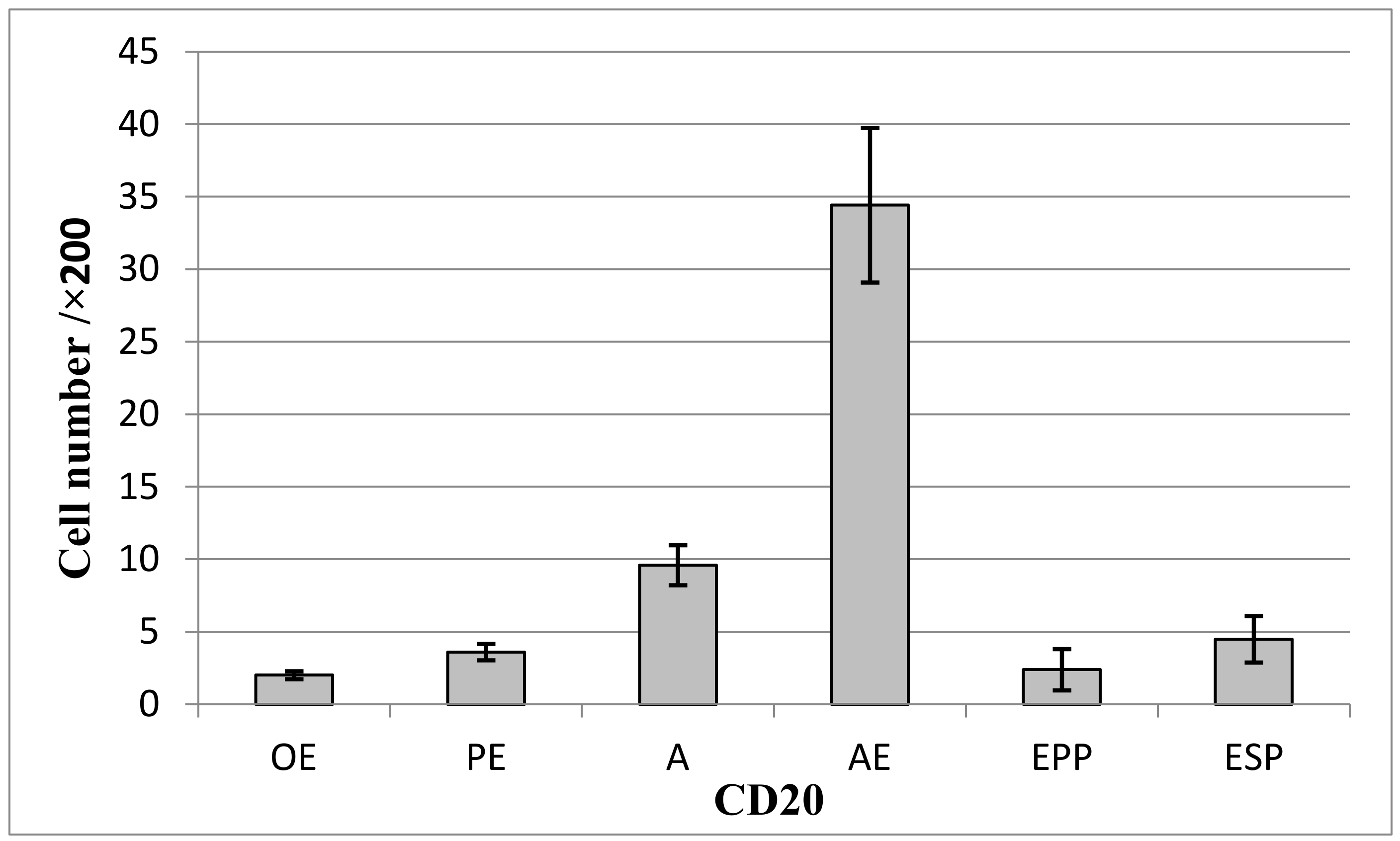
3.6. Analysis of Perilesional Stromal Inflammatory Changes
3.7. Histopathological Characterization by a Novel, Multiple Immunohistochemical Labeling Technique
4. Discussion
4.1. Evolution Predictors for Endometriosis/Adenomyosis Foci
The Role of Cytokeratin
4.2. The Role of Hormone Receptors
4.3. The Role of Perilesional Vascularization
4.4. The Role of Cell Proliferation and the Presence of Tumor Proteins
4.5. The Implications of Perilesional Inflammation
4.6. The Role of Stromal Factors in Symptomatology: Pain and Infertility
4.7. The Role of the Novel Technique of Multiple Immunolabeling
5. Materials and Methods
5.1. Assessment of Patient Symptoms and Infertility
5.2. Histopathological Preparation
5.3. Novel Technique for Multiple Immunohistochemical Labeling
5.4. Analysis Methods
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Genazzani, A.R.; Nisolle, M.; Petraglia, F.; Taylor, R.N. (Eds.) Endometriosis Pathogenesis, Clinical Impact and Management: Volume 9: Frontiers in Gynecological Endocrinology; ISGE Series; Springer International Publishing: Cham, Switzerland, 2021; ISBN 978-3-030-57865-7. [Google Scholar]
- Overton, C.; Davis, C.; McMillan, L.; Shaw, R.W.; Koh, C. (Eds.) An Atlas of ENDOMETRIOSIS, 3rd ed.; CRC Press: London, UK, 2013; ISBN 978-0-429-13050-2. [Google Scholar]
- Macer, M.L.; Taylor, H.S. Endometriosis and Infertility: A Review of the Pathogenesis and Treatment of Endometriosis-Associated Infertility. Obstet. Gynecol. Clin. N. Am. 2012, 39, 535–549. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gruenwald, P. Origin of endometriosis from the mesenchyme of the celomic walls. Am. J. Obstet. Gynecol. 1942, 44, 470–474. [Google Scholar] [CrossRef]
- Burney, R.O.; Giudice, L.C. Pathogenesis and pathophysiology of endometriosis. Fertil. Steril. 2012, 98, 511–519. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gupta, S.; Harlev, A.; Agarwal, A.; Pandithurai, E. Predisposing and Protective Factors of Endometriosis. In Endometriosis: A Comprehensive Update; Springer Briefs in Reproductive Biology; Gupta, S., Harlev, A., Agarwal, A., Eds.; Springer International Publishing: Cham, Switzerland, 2015; pp. 7–15. ISBN 978-3-319-18308-4. [Google Scholar]
- Alkatout, İ.; Meinhold-Heerlein, I.; Keckstein, J.; Mettler, L. Endometriosis: A Concise Practical Guide to Current Diagnosis and Treatment. J. Turk. Ger. Gynecol. Assoc. 2018, 19, 173–175. [Google Scholar] [CrossRef]
- Berceanu, C.; Istrate-Ofiţeru, A.M.; Voicu, N.L.; Capitanescu, R.; Berceanu, S. Endometrioza; Ed Medicală Universitară: Craiova, Romania, 2018; pp. 237–262. [Google Scholar]
- Brătilă, E.; Ionescu, O.M.; Badiu, D.C.; Berceanu, C.; Vlădăreanu, S.; Pop, D.M.; MehedinŢu, C. Umbilical Hernia Masking Primary Umbilical Endometriosis-a Case Report. Rom. J. Morphol. Embryol. 2016, 57, 825–829. [Google Scholar]
- Brătilă, E.; Comandaşu, D.E.; Coroleucă, C.; Cîrstoiu, M.M.; Berceanu, C.; Mehedintu, C.; Bratila, P.; Vladareanu, S. Diagnosis of Endometriotic Lesions by Sonovaginography with Ultrasound Gel. Med. Ultrason. 2016, 18, 469–474. [Google Scholar] [CrossRef] [Green Version]
- Istrate-Ofiţeru, A.M.; Pirici, D.; Niculescu, M.; Berceanu, C.; Berceanu, S.; Voicu, N.L.; Piringă, G.D.; Roşu, G.C.; Iovan, L.; Căpitănescu, R.G.; et al. Clinical, Morphological and Immunohistochemical Survey in Different Types of Endometriosis. Rom. J. Morphol. Embryol. 2018, 59, 1133–1153. [Google Scholar]
- Rolly, F. Ueber einen Fall von Adenomyoma uteri mit Uebergang in Carcinom und Metastasenbildung. Arch. Pathol. Anat. Physiol. Klin. Med. Vol. 1897, 150, 555–582. [Google Scholar] [CrossRef]
- Endometriosis of the Abdominal Wall-Clinical, Histopathological and Immunohistochemical Aspects | Request PDF. Available online: https://www.researchgate.net/publication/338993187_Endometriosis_of_the_Abdominal_Wall_-_Clinical_Histopathological_and_Immunohistochemical_Aspects (accessed on 2 March 2022).
- Koike, N.; Tsunemi, T.; Uekuri, C.; Akasaka, J.; Ito, F.; Shigemitsu, A.; Kobayashi, H. Pathogenesis and Malignant Transformation of Adenomyosis (Review). Oncol. Rep. 2013, 29, 861–867. [Google Scholar] [CrossRef] [Green Version]
- Rosenberg, M.; Fuchs, E.; Le Beau, M.M.; Eddy, R.L.; Shows, T.B. Three Epidermal and One Simple Epithelial Type II Keratin Genes Map to Human Chromosome 12. Cytogenet. Cell Genet. 1991, 57, 33–38. [Google Scholar] [CrossRef]
- Schweizer, J.; Bowden, P.E.; Coulombe, P.A.; Langbein, L.; Lane, E.B.; Magin, T.M.; Maltais, L.; Omary, M.B.; Parry, D.A.D.; Rogers, M.A.; et al. New Consensus Nomenclature for Mammalian Keratins. J. Cell Biol. 2006, 174, 169–174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leong, A.S.-Y.; Cooper, K.; Leong, F.J.W.-M. Manual of Diagnostic Antibodies for Immunohistology; Cambridge University Press: Cambridge, UK, 2003; ISBN 978-1-84110-100-2. [Google Scholar]
- Walter, P.; Green, S.; Greene, G.; Krust, A.; Bornert, J.M.; Jeltsch, J.M.; Staub, A.; Jensen, E.; Scrace, G.; Waterfield, M. Cloning of the Human Estrogen Receptor CDNA. Proc. Natl. Acad. Sci. USA 1985, 82, 7889–7893. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greene, G.L.; Gilna, P.; Waterfield, M.; Baker, A.; Hort, Y.; Shine, J. Sequence and Expression of Human Estrogen Receptor Complementary DNA. Science 1986, 231, 1150–1154. [Google Scholar] [CrossRef]
- Paterni, I.; Granchi, C.; Katzenellenbogen, J.A.; Minutolo, F. Estrogen Receptors Alpha (ERα) and Beta (ERβ): Subtype-Selective Ligands and Clinical Potential. Steroids 2014, 90, 13–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hammond, C.B.; Rock, J.A.; Parker, R.T. Conservative Treatment of Endometriosis: The Effects of Limited Surgery and Hormonal Pseudopregnancy. Fertil. Steril. 1976, 27, 756–766. [Google Scholar] [CrossRef]
- Satterthwaite, A.B.; Burn, T.C.; Le Beau, M.M.; Tenen, D.G. Structure of the Gene Encoding CD34, a Human Hematopoietic Stem Cell Antigen. Genomics 1992, 12, 788–794. [Google Scholar] [CrossRef]
- Civin, C.I.; Strauss, L.C.; Brovall, C.; Fackler, M.J.; Schwartz, J.F.; Shaper, J.H. Antigenic Analysis of Hematopoiesis. III. A Hematopoietic Progenitor Cell Surface Antigen Defined by a Monoclonal Antibody Raised against KG-1a Cells. J. Immunol. 1984, 133, 157–165. [Google Scholar]
- Taylor, G.M. Leucocyte Typing III: White Cell Differentiation Antigens. J. Med. Genet. 1988, 25, 573. [Google Scholar] [CrossRef] [Green Version]
- Berg, E.L.; Mullowney, A.T.; Andrew, D.P.; Goldberg, J.E.; Butcher, E.C. Complexity and Differential Expression of Carbohydrate Epitopes Associated with L-Selectin Recognition of High Endothelial Venules. Am. J. Pathol. 1998, 152, 469–477. [Google Scholar]
- Suzawa, K.; Kobayashi, M.; Sakai, Y.; Hoshino, H.; Watanabe, M.; Harada, O.; Ohtani, H.; Fukuda, M.; Nakayama, J. Preferential Induction of Peripheral Lymph Node Addressin on High Endothelial Venule-like Vessels in the Active Phase of Ulcerative Colitis. Am. J. Gastroenterol. 2007, 102, 1499–1509. [Google Scholar] [CrossRef]
- Drew, E.; Merzaban, J.S.; Seo, W.; Ziltener, H.J.; McNagny, K.M. CD34 and CD43 Inhibit Mast Cell Adhesion and Are Required for Optimal Mast Cell Reconstitution. Immunity 2005, 22, 43–57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strilić, B.; Kucera, T.; Eglinger, J.; Hughes, M.R.; McNagny, K.M.; Tsukita, S.; Dejana, E.; Ferrara, N.; Lammert, E. The Molecular Basis of Vascular Lumen Formation in the Developing Mouse Aorta. Dev. Cell 2009, 17, 505–515. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bullwinkel, J.; Baron-Lühr, B.; Lüdemann, A.; Wohlenberg, C.; Gerdes, J.; Scholzen, T. Ki-67 Protein Is Associated with Ribosomal RNA Transcription in Quiescent and Proliferating Cells. J. Cell Physiol. 2006, 206, 624–635. [Google Scholar] [CrossRef] [PubMed]
- Scholzen, T.; Gerdes, J. The Ki-67 Protein: From the Known and the Unknown. J. Cell Physiol. 2000, 182, 311–322. [Google Scholar] [CrossRef]
- Brătilă, E.; Brătilă, C.P.; Comandaşu, D.-E.; Bauşic, V.; Vlădescu, C.T.; Mehedinţu, C.; Berceanu, C.; Cîrstoiu, M.M.; Mitroi, G.; Stănculescu, R. The Assessment of Immunohistochemical Profile of Endometriosis Implants, a Practical Method to Appreciate the Aggressiveness and Recurrence Risk of Endometriosis. Rom. J. Morphol. Embryol. 2015, 56, 1301–1307. [Google Scholar] [PubMed]
- Surget, S.; Khoury, M.P.; Bourdon, J.-C. Uncovering the Role of P53 Splice Variants in Human Malignancy: A Clinical Perspective. Onco Targets Ther. 2013, 7, 57–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suvarna, V.; Singh, V.; Murahari, M. Current Overview on the Clinical Update of Bcl-2 Anti-Apoptotic Inhibitors for Cancer Therapy. Eur. J. Pharmacol. 2019, 862, 172655. [Google Scholar] [CrossRef]
- Wu, M.-Y.; Ho, H.-N. The Role of Cytokines in Endometriosis. Am. J. Reprod. Immunol. 2003, 49, 285–296. [Google Scholar] [CrossRef]
- Chu, E.C.; Tarnawski, A.S. PTEN Regulatory Functions in Tumor Suppression and Cell Biology. Med. Sci. Monit. 2004, 10, RA235–RA241. [Google Scholar]
- Fang, D.; Nguyen, T.K.; Leishear, K.; Finko, R.; Kulp, A.N.; Hotz, S.; Van Belle, P.A.; Xu, X.; Elder, D.E.; Herlyn, M. A Tumorigenic Subpopulation with Stem Cell Properties in Melanomas. Cancer Res. 2005, 65, 9328–9337. [Google Scholar] [CrossRef] [Green Version]
- Pavlasova, G.; Borsky, M.; Seda, V.; Cerna, K.; Osickova, J.; Doubek, M.; Mayer, J.; Calogero, R.; Trbusek, M.; Pospisilova, S.; et al. Ibrutinib Inhibits CD20 Upregulation on CLL B Cells Mediated by the CXCR4/SDF-1 Axis. Blood 2016, 128, 1609–1613. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lebovic, D.I.; Mueller, M.D.; Taylor, R.N. Immunobiology of Endometriosis. Fertil. Steril. 2001, 75, 1–10. [Google Scholar] [CrossRef]
- Taylor, R.N.; Lebovic, D.I.; Mueller, M.D. Angiogenic Factors in Endometriosis. Ann. N. Y. Acad. Sci. 2002, 955, 89–100. [Google Scholar] [CrossRef] [PubMed]
- Kyama, C.M.; Debrock, S.; Mwenda, J.M.; D’Hooghe, T.M. Potential Involvement of the Immune System in the Development of Endometriosis. Reprod. Biol. Endocrinol. 2003, 1, 123. [Google Scholar] [CrossRef] [Green Version]
- Salamonsen, L.A.; Lathbury, L.J. Endometrial Leukocytes and Menstruation. Hum. Reprod. Update 2000, 6, 16–27. [Google Scholar] [CrossRef] [Green Version]
- Ibrahim, M.G.; Sillem, M.; Plendl, J.; Chiantera, V.; Sehouli, J.; Mechsner, S. Myofibroblasts Are Evidence of Chronic Tissue Microtrauma at the Endometrial-Myometrial Junctional Zone in Uteri With Adenomyosis. Reprod. Sci. 2017, 24, 1410–1418. [Google Scholar] [CrossRef] [PubMed]
- Harvima, I.T.; Schechter, N.M.; Harvima, R.J.; Fräki, J.E. Human Skin Tryptase: Purification, Partial Characterization and Comparison with Human Lung Tryptase. Biochim. Biophys. Acta (BBA)-Protein Struct. Mol. Enzymol. 1988, 957, 71–80. [Google Scholar] [CrossRef]
- Iwabe, T.; Harada, T.; Tsudo, T.; Nagano, Y.; Yoshida, S.; Tanikawa, M.; Terakawa, N. Tumor Necrosis Factor-α Promotes Proliferation of Endometriotic Stromal Cells by Inducing Interleukin-8 Gene and Protein Expression. J. Clin. Endocrinol. Metab. 2000, 85, 824–829. [Google Scholar] [CrossRef] [Green Version]
- Arici, A.; Matalliotakis, I.; Goumenou, A.; Koumantakis, G.; Vassiliadis, S.; Mahutte, N.G. Altered Expression of Interleukin-18 in the Peritoneal Fluid of Women with Endometriosis. Fertil. Steril. 2003, 80, 889–894. [Google Scholar] [CrossRef]
- Schindl, M.; Birner, P.; Obermair, A.; Kiesel, L.; Wenzl, R. Increased Microvessel Density in Adenomyosis Uteri. Fertil. Steril. 2001, 75, 131–135. [Google Scholar] [CrossRef]
- Khan, K.N.; Masuzaki, H.; Fujishita, A.; Kitajima, M.; Sekine, I.; Ishimaru, T. Differential Macrophage Infiltration in Early and Advanced Endometriosis and Adjacent Peritoneum. Fertil. Steril. 2004, 81, 652–661. [Google Scholar] [CrossRef]
- Zhihong, N.; Yun, F.; Pinggui, Z.; Sulian, Z.; Zhang, A. Cytokine Profiling in the Eutopic Endometrium of Adenomyosis During the Implantation Window After Ovarian Stimulation. Reprod. Sci. 2016, 23, 124–133. [Google Scholar] [CrossRef] [PubMed]
- Cornillie, F.J.; Oosterlynck, D.; Lauweryns, J.M.; Koninckx, P.R. Deeply infiltrating pelvic endometriosis: Histology and clinical significance. Fertil. Steril. 1990, 53, 978–983. [Google Scholar] [CrossRef]
- Istrate-Ofiţeru, A.M.; Pîrvan, I.C.; Pirici, D.; Roşu, G.C.; Niculescu, M.; Berceanu, S.; Manolea, M.M.; Comănescu, M.V.; Voicu, N.L.; Iovan, L.; et al. Triple Immunohistochemistry for Assessing the Inflammatory, Vascular and Progression of Adenomyosis. Rom. J. Morphol. Embryol. 2019, 60, 419–428. [Google Scholar] [PubMed]
- Verkauf, B.S. Incidence, Symptoms, and Signs of Endometriosis in Fertile and Infertile Women. J. Fla. Med. Assoc. 1987, 74, 671–675. [Google Scholar]
- Schenken, R.S.; Asch, R.H.; Williams, R.F.; Hodgen, G.D. Etiology of Infertility in Monkeys with Endometriosis: Luteinized Unruptured Follicles, Luteal Phase Defects, Pelvic Adhesions, and Spontaneous Abortions. Fertil. Steril. 1984, 41, 122–130. [Google Scholar] [CrossRef]
- Downie, W.W.; Leatham, P.A.; Rhind, V.M.; Wright, V.; Branco, J.A.; Anderson, J.A. Studies with Pain Rating Scales. Ann. Rheum. Dis. 1978, 37, 378–381. [Google Scholar] [CrossRef] [Green Version]
- Pirici, D.; Mogoanta, L.; Kumar-Singh, S.; Pirici, I.; Margaritescu, C.; Simionescu, C.; Stanescu, R. Antibody Elution Method for Multiple Immunohistochemistry on Primary Antibodies Raised in the Same Species and of the Same Subtype. J. Histochem. Cytochem. 2009, 57, 567–575. [Google Scholar] [CrossRef] [Green Version]
- Mogoanta, L.; Popescu, C.F.; Georgescu, C.V. Cap. II-II:Tehnici de Histologie –Preparatul Histologic, Colorații Nucleare, Colorații Pentru Țesuturile Conjuctive. In Ghid de Tehnici de Histologie, Citologie şi Imunohistochimie; Medicală Universitară: Craiova, Romania, 2007; pp. 21–80. [Google Scholar]

















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Antibody | Company | Clone | Antigenic Retrieval | Dilution | Target |
|---|---|---|---|---|---|
| Anti-CK7 | Dako, Glostrup, Denmark | OV-TL 12/30 | Citrate, pH 6 | 1:50 | Glandular epithelium |
| Anti-CK20 | Dako | Ks20.8 | Citrate, pH 6 | 1:25 | Cellular proteins present in enterocytes and goblet cells |
| Anti-ERα | Dako | 1D5 | EDTA, pH 9 | 1:50 | Estrogen receptors α |
| Anti-PR | Dako | PgR 636 | EDTA, pH 9 | 1:50 | Progesterone receptors |
| Anti-CD34 | Dako | QBE nd 10 | Citrate, pH 6 | 1:50 | Capillary endothelial cells |
| Anti-Ki67 | Dako | MIB-1 | EDTA, pH 9 | 1:50 | Cells dividing in G1, S, G2 and M phase |
| Anti-p53 | Dako | DO-7 | EDTA, pH 9 | 1:50 | Nuclear marker |
| Anti-BCL2 | Dako | 124 | EDTA, pH 9 | 1:50 | B-cell lymphoma 2 |
| Anti-PTEN | Abcam | ab31392 | Citrate, pH 6 | 1:50 | Tumor suppressor gene |
| Anti- CD3 | Dako | - | Citrate, pH 6 | 1:50 | T lymphocytes |
| Anti-CD20 | Dako | L26 | Citrate, pH 6 | 1:50 | B lymphocytes |
| Anti-CD68 | Dako | KP1 | Citrate, pH 6 | 1:100 | Macrophages |
| Anti-Tryptase | Dako | AA1 | Citrate, pH 6 | 1:500 | Mast-cells |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Istrate-Ofiţeru, A.-M.; Berbecaru, E.-I.-A.; Zorilă, G.-L.; Roşu, G.-C.; Dîră, L.M.; Comănescu, C.M.; Drăguşin, R.C.; Ruican, D.; Nagy, R.D.; Iliescu, D.G.; et al. Specific Local Predictors That Reflect the Tropism of Endometriosis—A Multiple Immunohistochemistry Technique. Int. J. Mol. Sci. 2022, 23, 5614. https://doi.org/10.3390/ijms23105614
Istrate-Ofiţeru A-M, Berbecaru E-I-A, Zorilă G-L, Roşu G-C, Dîră LM, Comănescu CM, Drăguşin RC, Ruican D, Nagy RD, Iliescu DG, et al. Specific Local Predictors That Reflect the Tropism of Endometriosis—A Multiple Immunohistochemistry Technique. International Journal of Molecular Sciences. 2022; 23(10):5614. https://doi.org/10.3390/ijms23105614
Chicago/Turabian StyleIstrate-Ofiţeru, Anca-Maria, Elena-Iuliana-Anamaria Berbecaru, George-Lucian Zorilă, Gabriela-Camelia Roşu, Laurențiu Mihai Dîră, Cristina Maria Comănescu, Roxana Cristina Drăguşin, Dan Ruican, Rodica Daniela Nagy, Dominic Gabriel Iliescu, and et al. 2022. "Specific Local Predictors That Reflect the Tropism of Endometriosis—A Multiple Immunohistochemistry Technique" International Journal of Molecular Sciences 23, no. 10: 5614. https://doi.org/10.3390/ijms23105614