1. Introduction
The clinical application of bone substitute materials (BSM) has become an integral part of daily routine in various parts of medicine and dentistry. The gold standard is still autogenous bone won from different intraoral or extraoral donor sites due to its osteoinductive, osteogenic, and osteoconductive properties [
1,
2,
3]. However, its application is associated with different complications such as donor site morbidity, nerve lesions, and in general the need of a second surgical site with a second pain situation and inflammation risks [
4,
5]. It has been revealed that BSM perform equally to autologous bone transplants, superseding their application in many indications [
6,
7,
8]. In particular, animal derived xenografts are the most widely used BSM due to both their natural chemical composition and the structure that represents the trabecular framework, including the macro- and microporosity as well as the ultrastructure or nanotopography of the hydroxyapatite-based bone matrix [
9,
10]. A variety of preclinical and clinical studies have already shown that the application of xenogeneic BSMs lead to predictable bone formation due to their excellent osteoconductive properties [
11,
12,
13]. In this context, it has been revealed that xenogeneic BSMs are beneficial for oral and maxillofacial surgery in indications such as sinus augmentation procedures, providing a long-term scaffold for successful subsequent insertion of dental implants [
14,
15].
Due to the different indications in oral surgery, a broad variety of xenogeneic BSM is available in various delivery forms, ranging from bone blocks over granules to bone pastes [
16]. Moldable BSMs have already been shown to be advantageous in indications such as socket preservation, sinus augmentation, and treatment of bone cysts [
17,
18]. Their viscous properties allow for an optimal filling of irregularly shaped bone defects up to the defect borders [
19]. Not least, their viscosity enables an improved handling that helps clinicians to overcome implantation failures such as over- or under-packing of defect sites [
19,
20].
The currently available bone pastes are two-component biomaterials combining synthetic calcium phosphate (CaP)-based BSM granules with a hydrogel composed of polymers such as collagen or hyaluronic acid (HY) due to their high-water binding capacity [
19,
21]. It is generally assumed that the added extracellular matrix proteins also enable an enhancement of bone healing by triggering molecular processes such as cell adhesion, proliferation, and migration of osteoblast and other related cascades [
22,
23]. Furthermore, it has been shown that cell types such as endothelial cells as well as the implantation bed vascularization can be increased by such molecules via an increased cell migration or angiogenesis [
24]. Thereby, it has revealed that the application of BSM with a paste-like consistency seem to induce a special integration pattern in accordance with the process of Guided Bone Regeneration (GBR), guiding a cell and vessel ingrowth from the periphery towards the implant core [
25]. Finally, different study results revealed that an addition of collagen or HY increased osseous healing [
26,
27,
28].
In addition, the biomaterial-associated immune response has received increasing attention in recent years, as a primarily anti-inflammatory approach can improve the healing of (bone) tissue defects [
29,
30]. In this context, it has been reported that even high molecular weight HY (HMWHY) triggered the polarity of macrophages towards an M2-phenotype, which is supposed to contribute to the overall anti-inflammatory alignment of the material-related foreign body reaction and to improve bone tissue regeneration [
31]. In contrast, it was presented in another in vivo experiment that the addition of two different amounts of HMWHY, combined with a synthetic biphasic BSM, to an injectable BSM did not affect the inflammatory response, while only improving the material handling properties [
32]. In this context, it is known that the unstabilized HY molecule has a relatively short half-life in the body of between 17 hours and 1.5 days [
33,
34]. Thus, it can be concluded that the HY molecules integrated in injectable BSM are most often degraded within a short time span after implantation into the bony defects before having any effect on the tissue or healing response. Altogether, these results lead to the question of the biological and regenerative activity of HY for bone tissue regeneration. Even in view of the development of a new class of immunoregulating biomaterials such as BSM, this question needs to be clarified.
Thus, the present in vivo study was conducted, analyzing the (inflammatory) tissue reaction in combination with the bone healing capacities of a newly developed bone grafting material based on a well-researched xenogeneic BSM combined with HMWHY. Previously established methods were applied after implantation of the injectable BSM using the calvaria model in Wistar rats [
35,
36,
37].
3. Discussion
Bone grafts of paste-like consistency are more and more used in hard tissue regeneration, not only in the dental field but also in orthopedics or traumatology. It has been shown that their applicability ranges from sinus augmentation procedures over bone cyst fillings to jawbone regeneration procedure [
38]. Thereby, they allow for more precise application, even into deeply enclosed defects and for the repair of irregularly shaped lesions [
39].
Mainly, bone graft pastes based on calcium phosphate (CaP) granules combined with water-binding molecules such as collagen, cellulose, or hyaluronate (HY) are used in dentistry [
39]. All of them are based on synthetic CaP granules composed of pure CaP phases such as hydroxyapatite (HA) or β-tricalcium phosphate (β-TCP) or mixtures of both compounds called biphasic BSM [
38]. In this context, it has been shown that these BSM have their own indication area in which their application leads to the desired regenerative outcome [
18,
40]. Thereby, its regenerative properties are mainly depending on the integrated CaP granules. Especially in the case of synthetic BSM, it has been shown that they undergo degradation via (a) dissolution to calcium and phosphate ions in the organism and (b) cellular degradation or phagocytosis mediated by macrophages and multinucleated giant cells (MNGCs) [
41]. Their degradation pattern depends on the phase composition, and a degradation pattern that is correlating with simultaneous bone ingrowth has mainly appeared in the case of biphasic BSM [
42]. Thus, it can be concluded that the application of such BSM are mainly indicated in regenerative procedures that do not need a permanent maintenance of an osteoconductive basis such as jawbone reconstructions in the case of extraction sockets, after bone cysts, furcation defects, or other (intra-) osseus defects [
43]. However, indications that require permanent bone maintenance or volume stability, such as sinus augmentation procedures or jawbone regeneration even in the case of larger defects or bone resorption locations in the case of (long-term) edentulous patients—particularly if this condition might be strengthened by comorbidities such as osteoporosis or bone cancer —need the application of BSM with a prolonged degradation behavior. Xenogeneic BSMs such as Bio-Oss
® or cerabone
® have been shown to provide this resorption profile as they have been found within their implantation beds several years after their implantation. Interestingly, the molecular basis of their biodegradation pattern has already been revealed in different studies, showing that this material type does induce a low grade of material-associated inflammation and especially of low numbers of multinucleated giant cells. Thereby, a broad variety of clinical studies revealed their good bone regeneration capacities [
14,
44].
Xenogeneic BSMs are mainly applied in the form of granules, and also in the form of blocks [
45]. However, there is not yet a BSM available combining xenogeneic bone substitute granules with hyaluronic acid. The base principle of this two-component material class is to mix BSM granules with a hydrogel composed of minimally one water-binding polymer to increase the clinical handling [
39]. In particular, the extracellular matrix protein hyaluronic acid (HY)—and even high molecular weight HY (HMWHY)—has gained importance as a component of actual BSM [
46]. Besides its water-binding properties, it is believed to trigger the bone regeneration process by influencing underlying molecular processes such as osteoblast differentiation, proliferation, and migration [
47]. Additionally, it has been revealed that HY can increase implant bed vascularization based on its influence on endothelial cells and angiogenesis [
48]. Not least, the HY addition is believed to have an influence on macrophage polarity towards an M2-phenotype, contributing to an overall anti-inflammatory alignment of the material-related foreign body reaction and an improved bone tissue regeneration [
31]. Finally, it has been reported that its addition might allow for a special integration pattern in accordance with the process of Guided Bone Regeneration (GBR) [
28,
49].
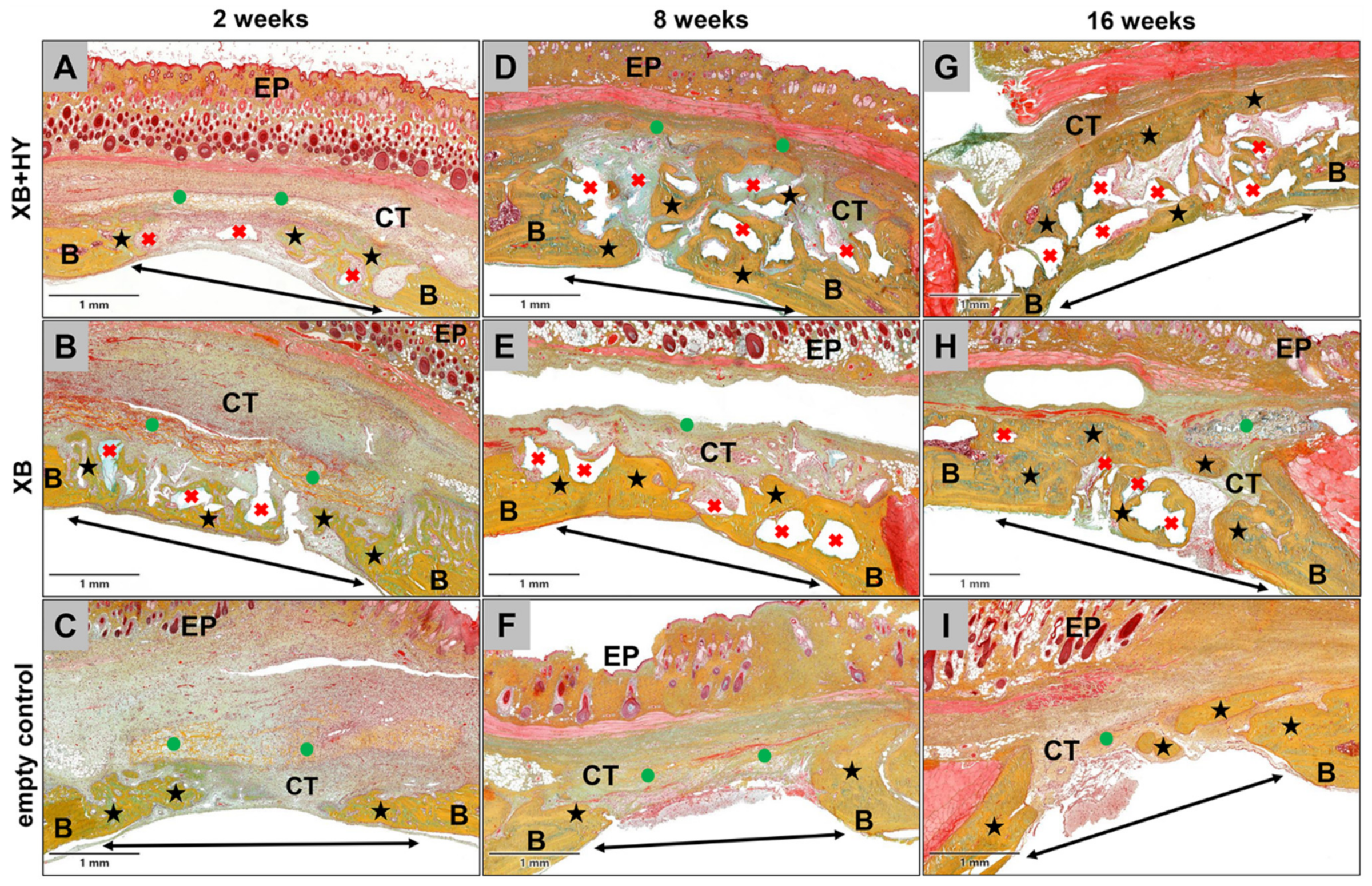
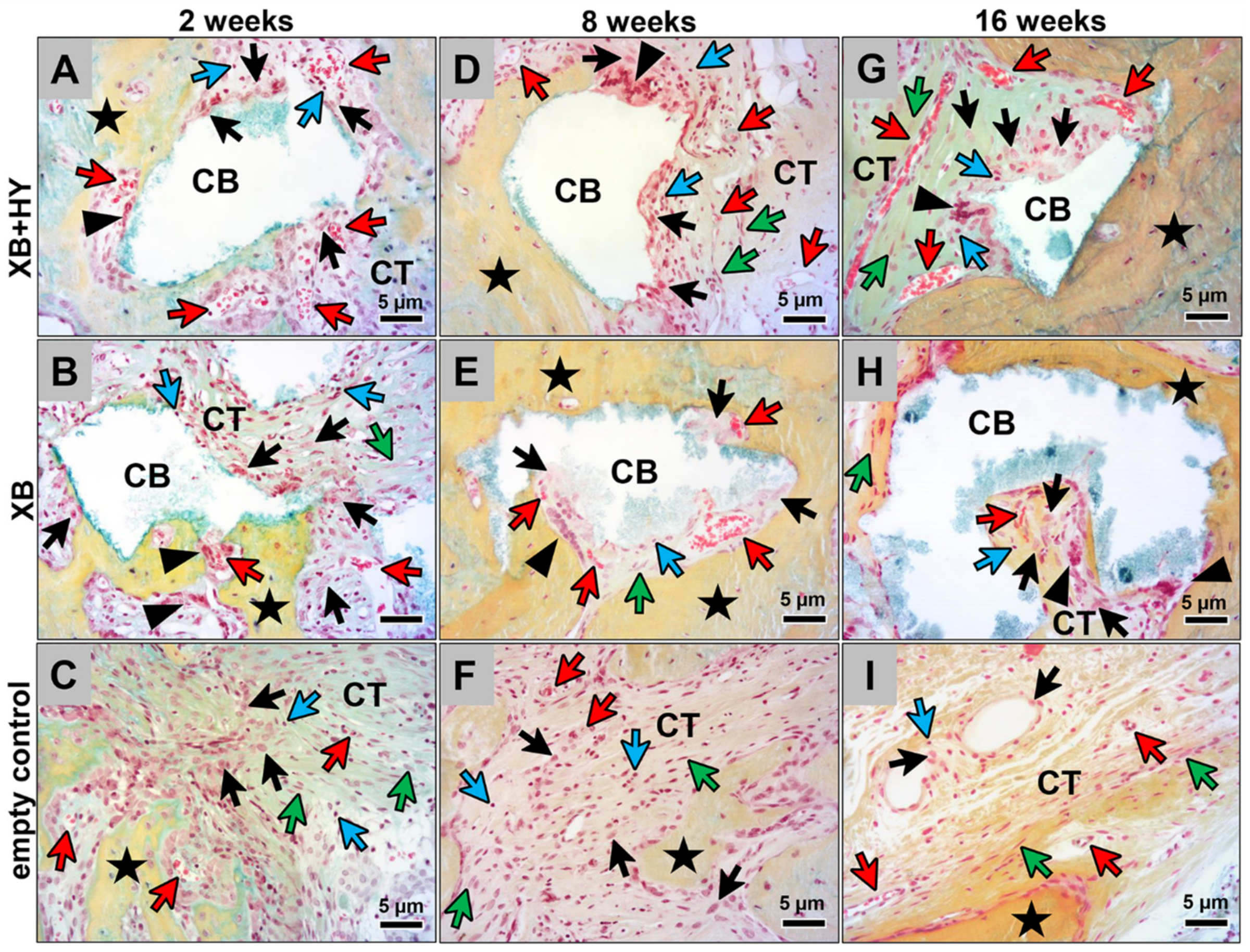
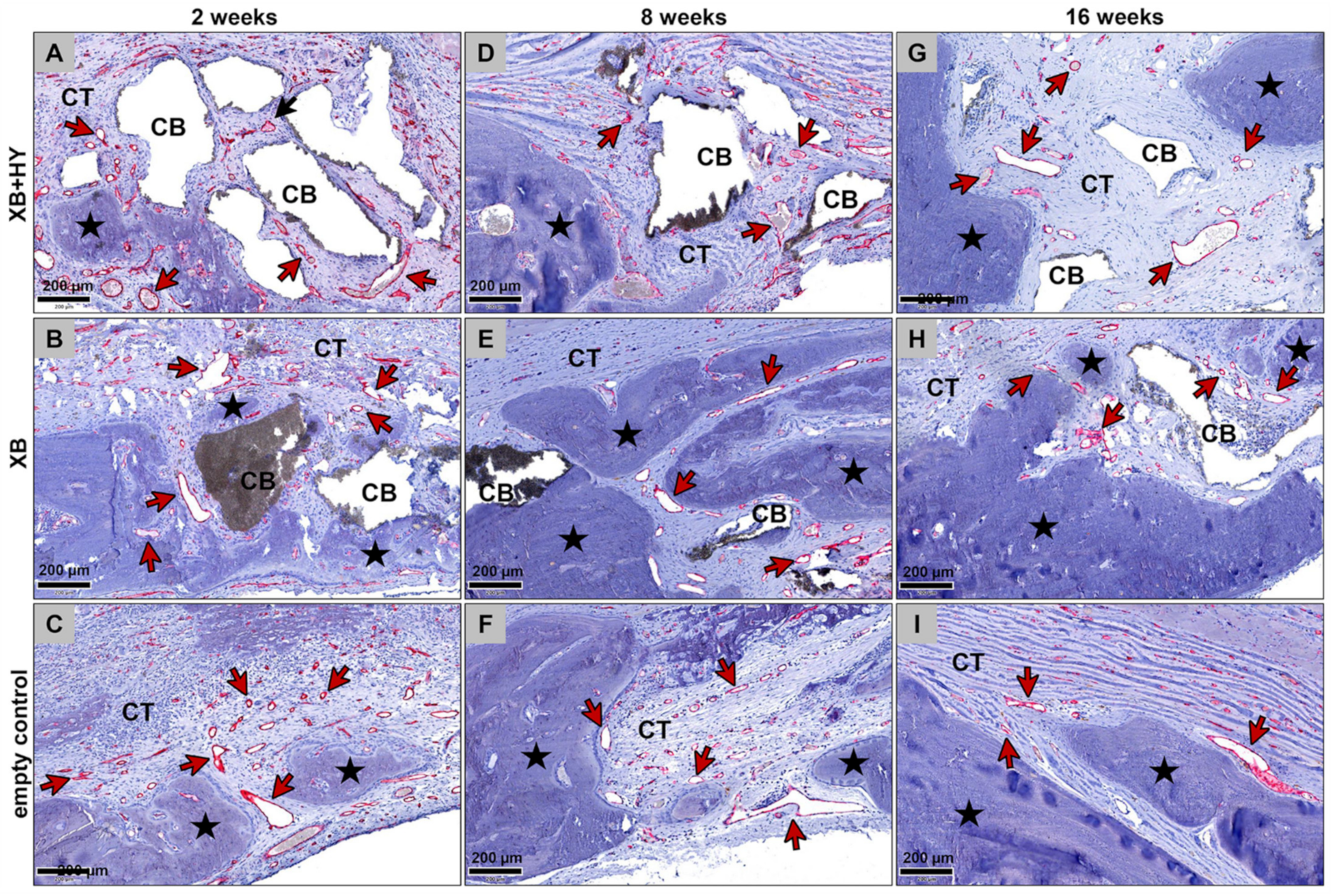
The present in vivo study was conducted by analyzing the (inflammatory) tissue reaction in combination with the bone healing capacities of a newly developed BSM based on an xenogeneic BSM combined with HMWHY. Established in vivo methods including specialized histological workup processes, (immuno-) histological staining procedures, and both histopathological and histomorphometrical analysis protocols according to the DIN EN ISO 10993-6 were applied after implantation of the hyaluronate containing BSM using the calvaria model in Wistar rats. Implantations of the xenogeneic BSM not containing HMWHY and sham operations were used as control groups.
Altogether, the results of the present study show that the HY allows for an optimal material-associated bone tissue healing comparable to the control xenogeneic BSM. The added HY seems to be degraded within a very short time period of less than 2 weeks so that the remaining BSM granules allow for a gradual osteoconductive bone regeneration. Additionally, no differences between the inflammatory tissue reactions in both material groups and the sham operation group were found.
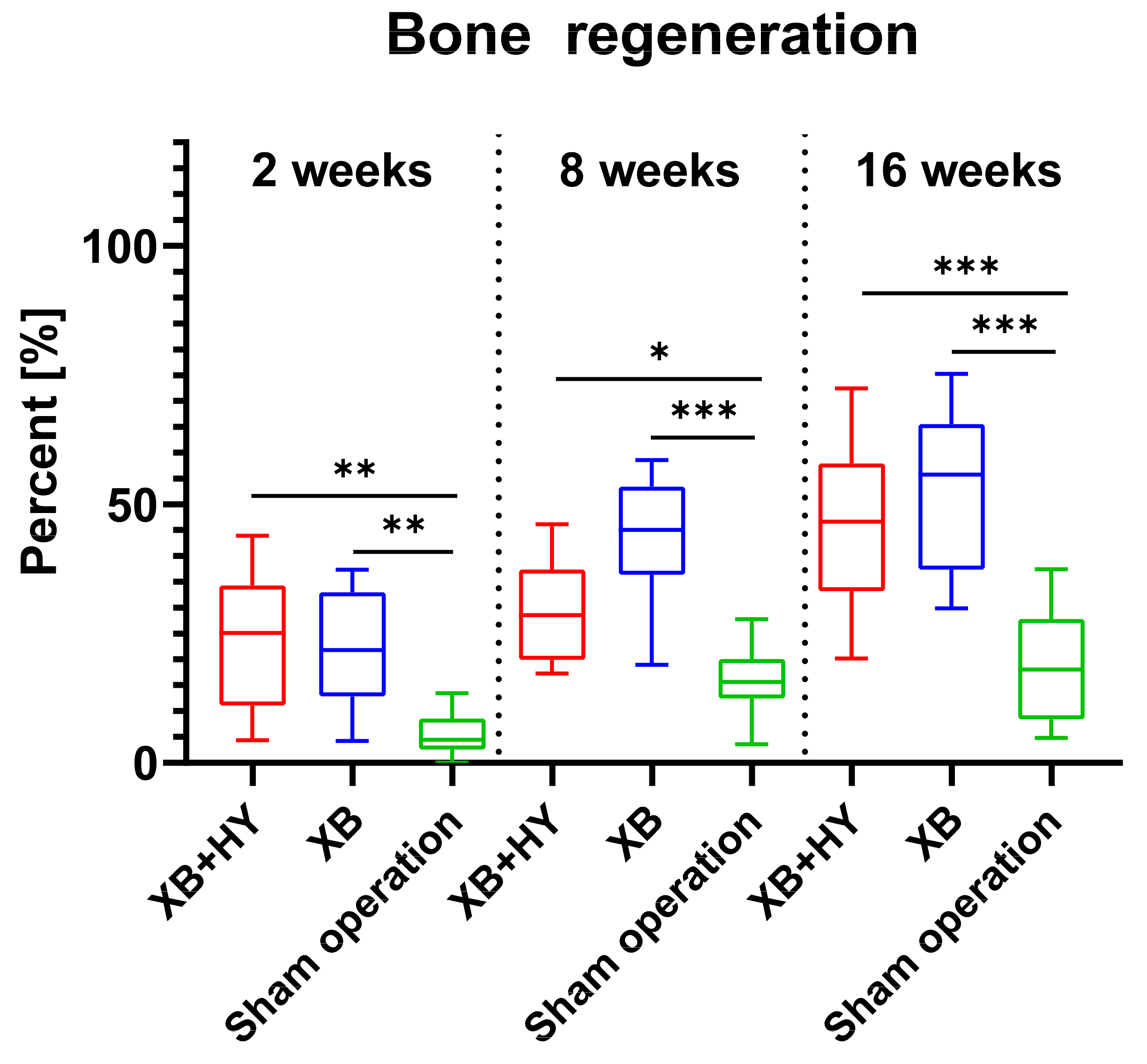
The results of the study, including not only the histological observations but also the histomorphometrical measurements, initially showed that comparable bone regeneration values were found in the analyzed xenogeneic BSM group and the group of the control xenogeneic BSM. This result shows that the initially implanted HMWHY seemed not to influence the bone growth process. Thus, it is conceivable that the HMWHY served as a hydrogel component during the implantation but was degraded prior to having a molecular influence on the bone regeneration or associated processes. In this context, Snetkov et al. described the degradation pattern of HY—although only poor knowledge is available about the degradation times [
50]. Within tissues, HY is generally degraded via enzymatic hydrolysis of hyaluronidases (HYALs), and even HYAL1 and HYAL2 are considered major HA-degrading enzymes [
51]. Moreover, it was reported in different studies that HMWHY was finally degraded within 24–48 h [
50]. Thus, it is conceivable that the HMWHY present in the analyzed BSM did not have any effect on the material-associated tissue reactions. Furthermore, it was shown in another study series, including in vitro, in vivo, and clinical study parts that combinatorically analyzed the tissue reactions and the (bony) integration behavior of a bone paste based on β-TCP granules with a hydrogel combining HY and methylcellulose, showed that this material underwent continuous degradation from the periphery towards the core [
24]. Additionally, the combination of the three biocompatible materials into one material enabled modification of the tissue reaction to the implant and resulted in a longer in vivo lifetime than that of β-TCP granules alone. In addition, this combination increased the vascularization of the implantation bed. While these study results attributed the observed reaction pattern to the added HY, the results of the present study led to the conclusion that it might rather be traced to the methylcellulose. This assumption cannot completely be confirmed as the aforementioned study series did not include a respective control group without methylcellulose. Another in vivo study by Sieger et al. analyzed the tissue reactions and the bone regeneration to a synthetic biphasic BSM combined with two different amounts of HMWHY [
32]. Again, no differences in the bone healing, even compared to the control group (without HY), were detected, which underlines the present results.
The results of the present study showed that, in all study groups, an increasing bone volume was detected over the study period, which was expectable. Moreover, significantly higher bone regeneration was found in both material groups, substantiating the good osteoconductive properties and the good biocompatibility of the xenogeneic BSM, which has already been examined and confirmed in different other studies [
24,
32,
52,
53]. Additionally, the analysis showed that the values of newly formed bone tissue in the sham operation group were significantly lower compared to both material groups, which underlines the idea that the calvaria implantation site reached a critical size. Thus, bone regeneration cannot take place to the same extent as in the groups containing the osteoconductive BSM. This result substantiates the regenerative capacity of the xenogeneic bone substitute.
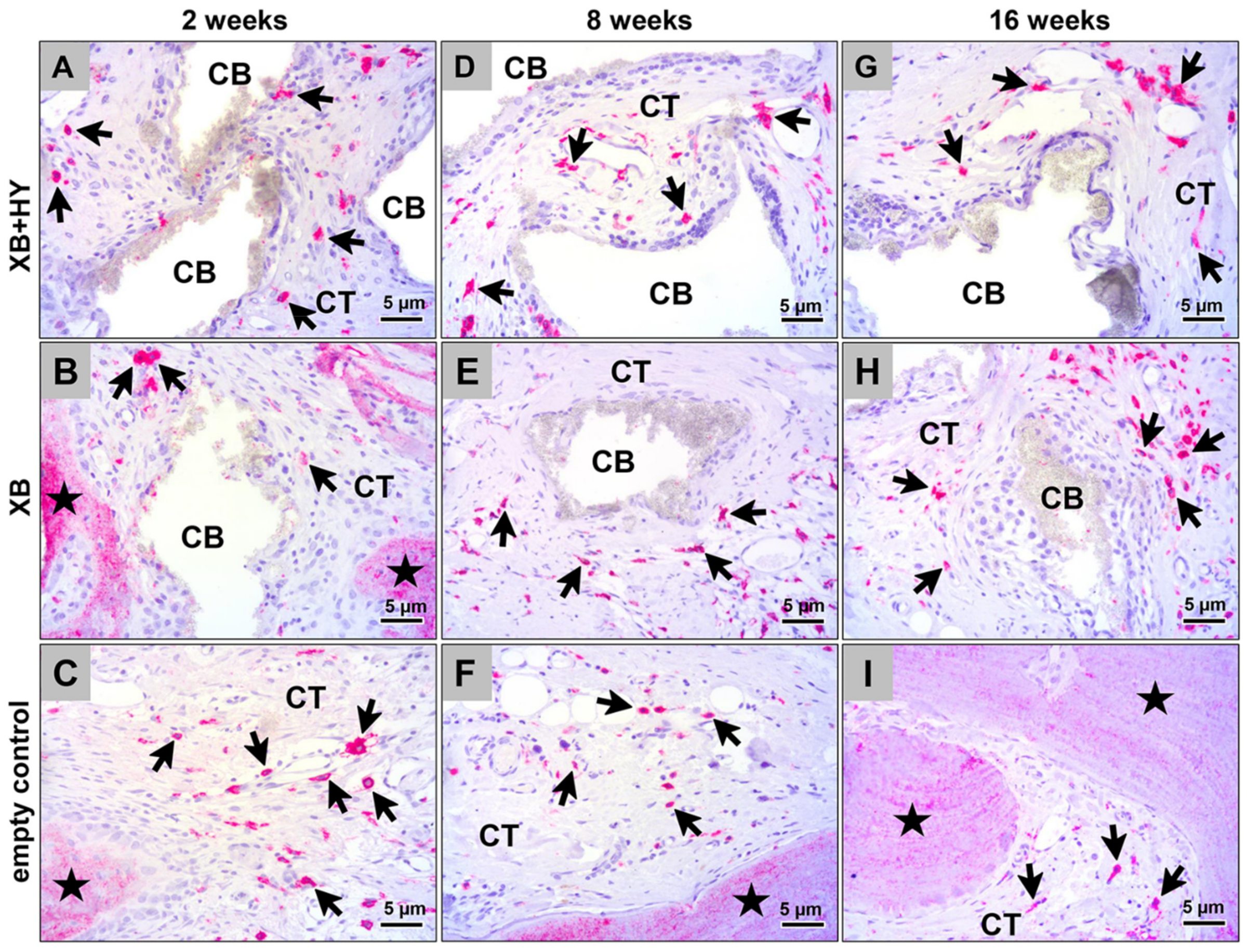
The results of (a) the histopathological analysis, (b) the scoring, and (c) the histomorphometrical analysis of the immune response via detection of M1- and M2-macrophages combinatorically showed that the added HMWHY did not have an effect on the cellular or inflammatory reactions to the xenogeneic BSM. This result also supports the aforementioned assumption of the fast degradation of the added HMWHY. Interestingly, the analysis of the M1- and M2-macrophage induction additionally showed that none of the materials, i.e., the hyaluronate containing BSM and the control BSM, induced significant differences in view of the macrophage subtypes found in the sham operation group. Moreover, no differences in cell numbers were found while conducting the histopathological scoring. Even in view of the heavily discussed topic of potential immune responses to natural biomaterial, such as the analyzed xenogeneic BSM, the presented results show that the xenogeneic BSM did not seem to evoke an immune response contrary to the sham operation group [
54,
55,
56]. In this context, Kačarević et al. stated in a review article that the xenogeneic BSM analyzed in the present study is treated with temperatures above 1200 °C, which has been reported to safely reduce the risk of pathogen transmission and eliminates cell or protein content. Thus, the present data substantiate the previous results that are also proved in a new study by Barbeck et al. analyzing the systemic and local immune response to 15 commercially available BSMs and allogeneic bone grafts after subcutaneous implantation for up to 90 days [
57] (manuscript submitted). These data reveal that none of the materials induced increased levels of 14 measured cytokines from the peripheral blood, while only slight local effects onto macrophage responses were found.
Interestingly, the results of these study parts clearly showed that, in all study groups, more M2-macrophages compared to their M1-subtype were found. In combination with data from bone growth measurements, it can be concluded that both analyzed biomaterials provide an excellent biocompatibility, creating a microenvironment optimally suitable for bone tissue healing [
58]. However, it must be mentioned that the analysis of the local effects of biomaterials, such as the analyzed BSM, which are only based on the macrophage counting, may only provide limited data. In combination with the histopathological scoring data, more information is provided, but it still shows some limitations. This is because the scoring that is based on the ISO-norm 10993 does not include relevant cell types such as T- or B-lymphocytes or even mast cells. Thus, a revision of the ISO-norm including more cell types and also a differentiation of different cell subtypes may be necessary. This approach may not only help to introduce safer materials into the market but also help to develop a next generation of BSM that modulate the immune response to improve (bone) tissue regeneration. However, it must be mentioned that most of the studies analyzing tissue reactions to biomaterials such as the analyzed BSM include less information than presented in the actual study.
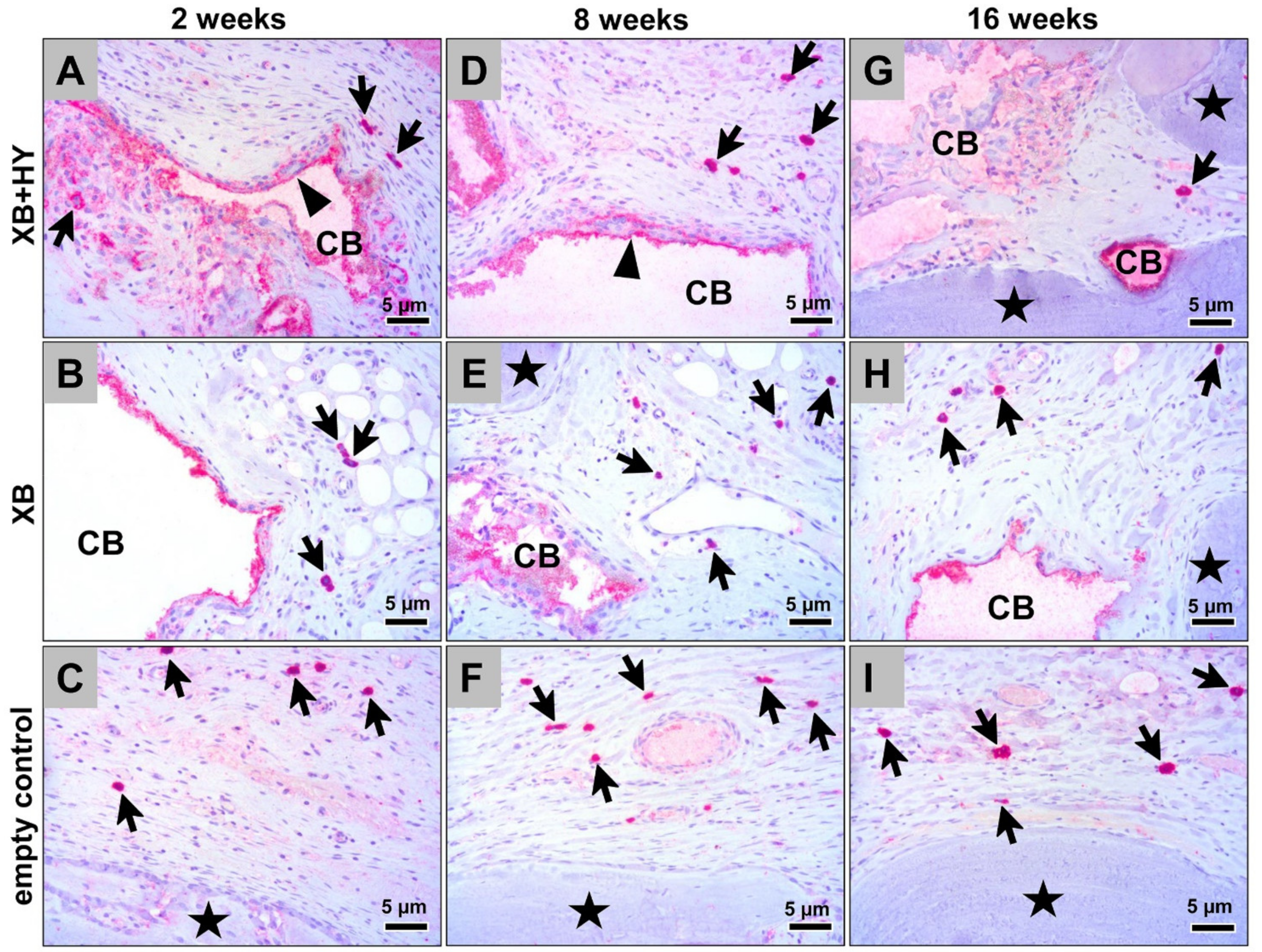
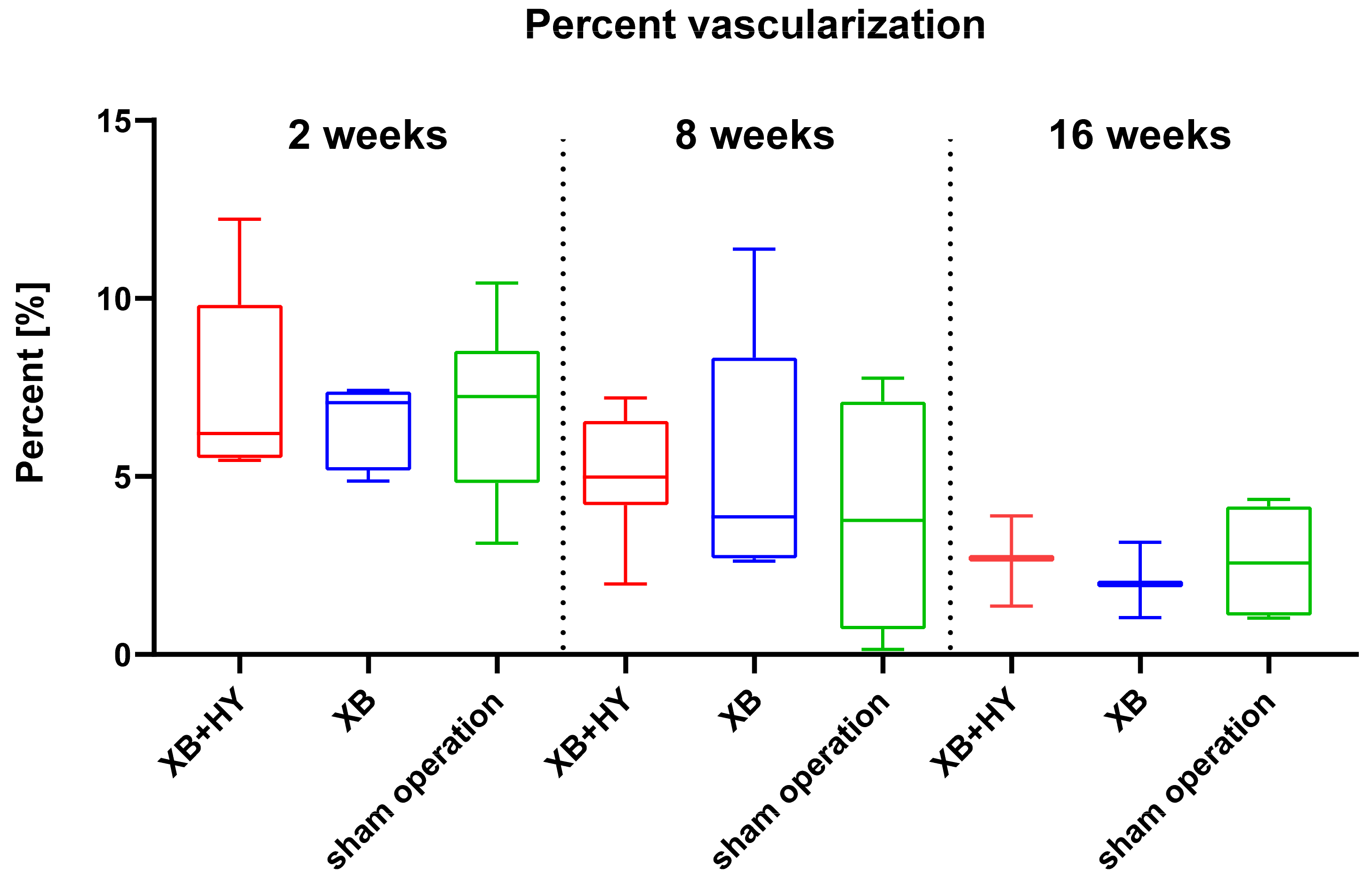
Finally, the measurements of the implant bed vascularization showed a consistently comparable vessel density in all study groups, while only a significant decrease up to 16 weeks post implantationem was found in the sham operation group. The analysis of the percent vascularization did not show any significant differences between or within the different groups over the study period, while in all groups a decreasing tendency was detectable up to the end of the study period. These data additionally lead to the conclusion that neither the analyzed hyaluronate containing BSM nor the control xenogeneic BSM evoked pronounced inflammatory tissue reactions, as already shown by the other study parts. This assumption is based on the fact that it has been shown that both macrophages and multinucleated giant cells (MNGCs) are expressing pro-angiogenic molecules such as the vascular endothelial growth factor (VEGF) that has a major influence on the implantation bed vascularization, even in the case of biomaterials inducing strong tissue reactions [
59]. Different studies have revealed that both vascularization parameters are especially dependent on the numbers of MNGCs induced by a biomaterial such as synthetic BSM [
24,
37,
47,
59,
60,
61]. The results of the present study showed in conformity with other preclinical studies analyzing the tissue reactions to the same xenogeneic material implanted within the subcutaneous tissue and also after its clinical application for sinus augmentation that both BSMs induced a low tissue reaction pattern, including low numbers of MNGCs [
12,
36]. Thus, a correlating low vascularization pattern was expectable and has been shown in the present study. Interestingly, both the vessel density and the percentage of vascularization differed from that detected in the previous study using the subcutaneous implantation model that measured a significant implant bed vascularization [
12]. This data reflects the reported differences of the tissue reactions using different implantation models [
62]. In this context, it has already been assumed that the different micromilieus lead to differences in measurement data such as the observed vascularization pattern. Thus, data gained via the subcutaneous implantation model—especially in the case of BSM—may not represent the physiological conditions existing within the “bone tissue compartment”. However, data gained by this preclinical implantation model can initially give basic insights into the tissue reaction pattern to biomaterials such in vitro cytocompatibility analyses that are also proposed by the ISO guidelines. Thus, further studies have to prove the comparability of data won by different implantation models—even with regard to different biomaterials for different clinical applications.
In summary, the results of the present study show that the newly developed bone grafting material composed of xenogeneic BSM granules combined with HMWHY provides an excellent biocompatibility and good osteoconductive properties that are fully comparable to the pure BSM granules whose performance has already been tested in a broad variety of preclinical and clinical studies [
14,
44,
63]. Moreover, the scoring, in combination with the molecular biological analyses, showed that this hyaluronate containing BSM induced a similar tissue reaction pattern comparable to the control BSM. Moreover, similar M1- and M2-macrophage numbers were also found in the sham operation group. These data show that the added HMWHY did not induce effects on the bone healing process or on the inflammatory tissue reaction or on the implantation bed vascularization. It also shows that both BSM did not evoke pronounced inflammatory tissue reactions substantiating their purity and tissue compatibility.
4. Material and Methods
4.1. Biomaterials
All biomaterials analyzed in the present study were kindly provided by botiss biomaterials GmbH (Zossen, Germany).
4.1.1. Cerabone®
The xenogeneic BSM cerabone
® (XB, botiss biomaterials GmbH, Zossen, Germany) is obtained from the femoral heads of cattle from registered slaughterhouses in New Zealand and Germany. The potentially immunogenic components are removed in a multi-step-process to ensure its safe application [
11]. Thereby, the bovine bone raw material undergoes a sophisticated three-step heating, which is free of chemical additives and includes a final high temperature treatment at more than 1200 °C. After the purification processes the bone substitute material is packed and sterilized. For the present in vivo study cerabone
® granules with a particle size of 0.5–1 mm were used.
4.1.2. Cerabone® plus
Cerabone® plus (XB+HY, botiss biomaterials GmbH, Zossen, Germany) is a combination of cerabone® granules and high molecular weight sodium hyaluronate. The bone substitute material is provided dry and has to be hydrated before use. Upon hydration with saline or blood, it forms a malleable bone grafting material, which facilitates the application and reduces particle distribution in the augmentation area. For the present study, cerabone® plus with cerabone® granules in the size of 0.5–1 mm were used.
4.2. In Vivo Study Design, Implantation and Explantation Procedure
The study included 42 male 10–12-week-old Wistar rats with an approximate weight of 220–240 g, which were randomly allocated in three different study groups. Thus, each group consisted of 21 animals with 7 animals per study time point (
n = 7) (
Table 9). Explantation was timed at 2, 8, and 16 weeks (
Table 9). Prior to the study, the in vivo experiments were authorized by the local Ethical Committee of the Faculty of Medicine (University of Niš, Serbia). Approval of the Local Ethical Committee (Faculty of Medicine, University of Niš, Niš, Serbia) was based on decision number 323-07-00073/2017-05/7 of the Veterinary Directorate of the Ministry of Agriculture, Forestry and Water Management of the Republic of Serbia (date of approval: 22/02/2017). Animal welfare included animal housing and standard operative care in compliance with standardized guideline for animal experiments (e.g., water ad libitum, artificial light-dark cycle of 12 h each, controlled temperature and humidity, regular rat pellets). The animal welfare was conducted and ensured by appropriately qualified and trained staff at the Faculty of Medicine (University of Niš, Serbia). Standard veterinary medical care was provided in this study, and only healthy animals were selected for implantation.
To evaluate the tissue response to the newly developed BSM after implantation, three groups were set (
Table 9).
Calvaria Implantation
After an acclimation period of 1 week, the surgical interventions for implantation of the biomaterials according to the study plan were conducted as previously described. Prior to the implantation, intraperitoneal anesthesia with 10 mL ketamine (50 mg/mL) with 1.6 mL Xylazine (2%), was performed, and animals were shaved and disinfected. Bilateral cranial defects (8 mm diameter) were created using a trephine bur (GC, Tokyo, Japan). Left-sided defects were filled with equal amounts of the BSM, while the right-sided defects served as controls without biomaterial insertion (control group). Both defects were covered via a collagen membrane (Jason® membrane, botiss biomaterials GmbH, Zossen, Germany) and sutured. After the predefined healing periods (2, 8, and 16 weeks), the animals were euthanized by means of euthasol (400 mg/mL), followed by the extraction of the implantation area and subsequent histological workup. The explanted tissues were initially fixed using 4% formalin solution for 48 h and were then stored in phosphate-buffered saline (PBS) at 4 °C until further histological preparation.
4.3. Sample Preparation and Staining Procedures
By means of a diamond-bandsaw (Diamond-bandsaw Makro, EXAKT Advanced Technologies GmbH, Norderstedt, Germany) the calvarial explants were cut into segments that contained both bone defects, i.e., the left and the right defect. For further histological processing, the explants were placed in embedding cassettes (Histosette®, VWR, Darmstadt, Deutschland). Automatic dehydration was performed in a series of increasing alcohol concentrations (80%, 96%, 100%) to prepare the tissue for following plastic embedding in Technovit 9100 (Technovit 9100, Kulzer GmbH, Hanau, Germany) After dehydration, stepwise immersion at 4 °C with Technovit 9100 medium using different infiltration solutions (pre-infiltration, infiltration I + II with same composition) was conducted. Afterwards, the polymerization solution was prepared according to the operation instructions. The explants were orientated on the saw-edges and placed on the bottom of rolled rim bottles (rolled rim bottles with snap-on lid (VWR, Darmstadt, Germany), subsequently followed by pouring with the polymerization mixture. To avoid exposition of oxygen and therefore occurrence of irregular polymerization, the bottles were sealed hermetically and immediately stored at −20 °C until the liquid Technovit 9100 was completely polymerized and hardened. Subsequently, the tissue blocks were trimmed into shape by means of a grinding machine (EcoMet 30, Buehler, Esslingen, Germany). Sections with a thickness of 4–6 µm were prepared using a rotation microtome (CUT4060E, microTec GmbH, Walldorf, Germany). Histochemical and immunohistochemical staining was performed using specialized methods, as previously published. Four sections of every tissue explant were used for hematoxylin and eosin (H&E), Masson–Goldner, Movat’s Penatchrome, and Heidenhain’s Azan trichrome stainings. Two additional sections were used for immunohistochemical staining. Briefly, antibodies for detection of pro- and anti-inflammatory macrophage subtypes, i.e., integrin alpha x (CD11c) (abx231412, Abbexa Ltd, Milton, United Kingdom) and hemoglobin scavenger receptor (CD163) (ab182422, abcam, Cambridge, UK), were used to assess the immunological tissue response. Initially, the slides were treated with TRIS-EDTA pH 9 for 20 min in a steamer at 96 °C, followed by equilibration using cold wash buffer. Before the incubation with the respective first antibody for 60 min at room temperature, a blocking step with protein blocking solution for 10 min was conducted. Final detection of the antigen was caused by incubation with the biotinylated secondary antibody for 15 min, subsequently followed by application of the streptavidin–alkaline–phosphatase conjugate and the permanent alkaline phosphatase (AP)-red chromogen. Finally, counterstaining was performed using Mayer’s hemalum solution (Merck KGaA, Darmstadt, Germany). Unless otherwise stated, all solutions and reagents were purchased from Zytomed Systems (Berlin, Germany).
4.4. Histopathological & Histomorphometrical Analysis
To evaluate the inflammatory tissue response and osseointegration, the groups were compared histologically and based on histopathological scoring system according to the respective DIN ISO norm 10993-6 [
64]. Thereby, XB+HY (group 1) was compared with XB (control group) to evaluate the effect of the addition of sodium hyaluronate.
The histology sections were evaluated for a number of parameters, evaluating safety and efficacy. The sections were analyzed and graded according to cell type and responses. Safety was evaluated following the irritancy/reactivity grading scheme adapted from the ISO 10993-6 Annex E (
Table 10).
Afterwards, irritancy/reactivity scores based on ISO 10993-6 derived from the parameters listed in
Table 10 were calculated as follows for each defect (
Table 11):
The irritancy score for each test or control treatment was then calculated by averaging the irritancy scores of all test or control defect sites for each treatment, respectively. Each irritancy/reactivity score was calculated as follows:
Test Article Irritancy Score—Control Article Irritancy Score = Irritancy/Reactivity score;
If the result was a negative number, the Irritancy/Reactivity Score was considered to be 0.0.
Additionally, the macrophage numbers, the bone growth, and the implantation bed vascularization were examined histomorphometrically using specialized digital methods, as previously described [
64]. For the histomorphometrical analysis, the regions of interest, including newly formed bone, remaining BSM, and soft-tissue cavities, were digitized with a specialized scanning microscope (M8, precipoint, Munich, Germany). For comparative measurements of the tissue distribution, the respective areas of newly built bone, remaining BSM, and connective tissue within the implantation area were measured by manually marking the different tissue parts using the open-source software ImageJ. The tissue fractions were calculated by calculating the respective percentage of the fraction area in relation to the total implant area. The occurrence of pro- and anti-inflammatory macrophages within the implant beds was also determined with the ImageJ software using a specially developed plugin, as already described by Lindner et al. [
64]. For this measurement step, the workflow-plugin allowed us to calculate the respective cell densities via relation to the total implant area (cells/mm
2). For analysis of the implantation bed vascularization, the vessels were marked based on a newly developed plugin for ImageJ [Linder et al., manuscript in preparation] and related to the total implant area as vessel density (vessels/mm
2) and as percent vascularization (total vessel area in relation to the total implant area, in %).
4.5. Statistical Analysis
An analysis of variance (ANOVA) was used via the GraphPad Prism 8.0 software (GraphPad Software Inc., La Jolla, CA, USA), followed by an LSD post-hoc test for statistical analysis of the qualitative data won via histomorphometry. Both inter- (*) and intra-individual (●) significances were calculated and designated as significant if the p-values were less than 0.05 (*/● p ≤ 0.05), and highly significant if the p-values were less than 0.01 (**/●● p ≤ 0.01) or less than 0.001 (***/●●● p ≤ 0.001). Finally, the data were shown as mean and standard deviations.


 ,
, 









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}