
Custodiol® Supplemented with Synthetic Human Relaxin Decreases Ischemia-Reperfusion Injury after Porcine Kidney Transplantation

 , , and
, , and
Abstract
:1. Introduction
2. Materials & Methods
2.1. Study Approval
2.2. Animals
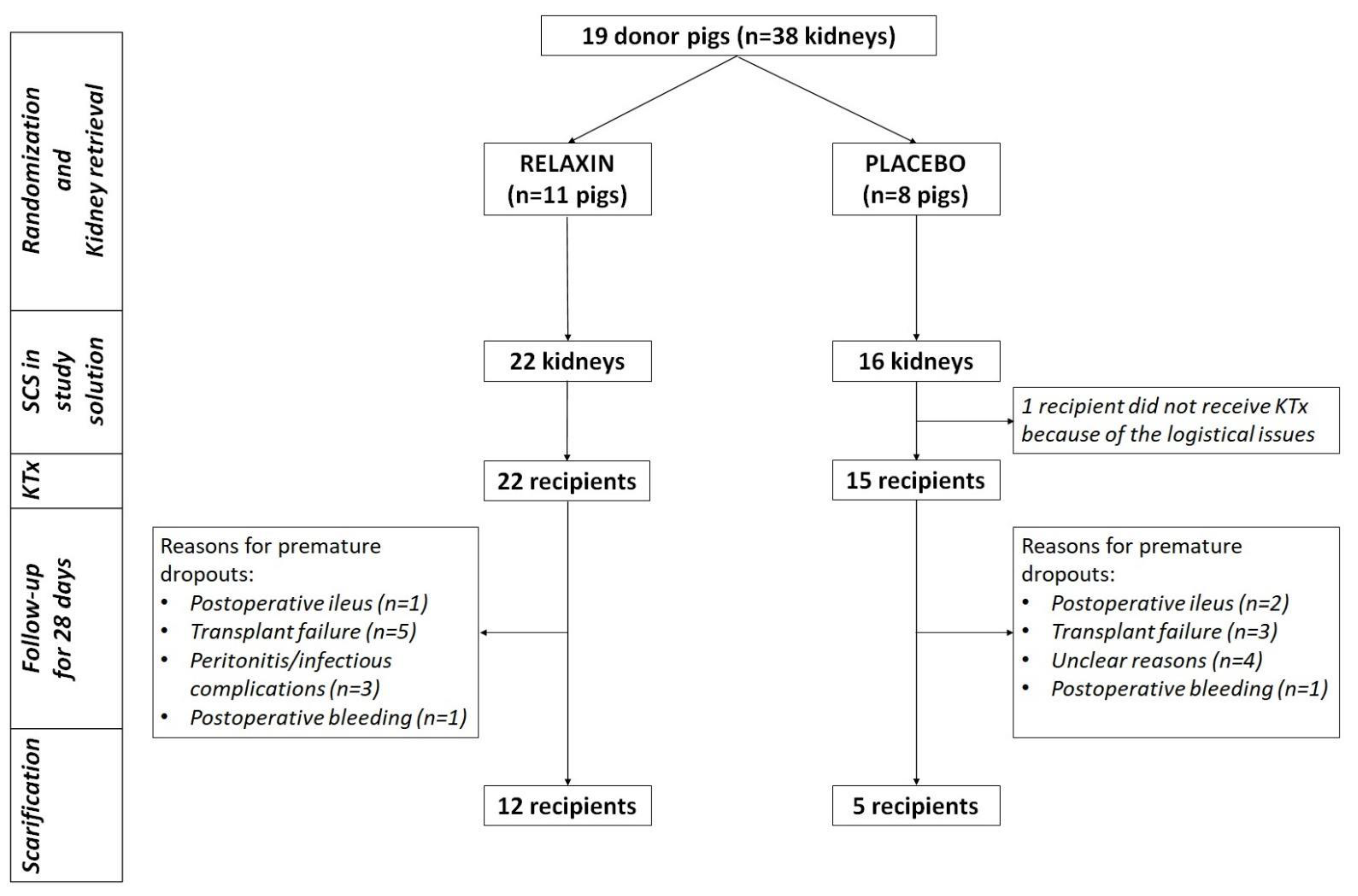
2.3. Experimental Design
2.4. Kidney Perfusion and Retrieval
2.5. Kidney Implantation
2.6. Immunosuppression and Postoperative Care
2.7. Tissue and Blood Sampling
2.8. Whole Blood and Serum Measurements
2.9. Immunohistochemistry
2.10. qPCR
3. Statistical Analysis
4. Results
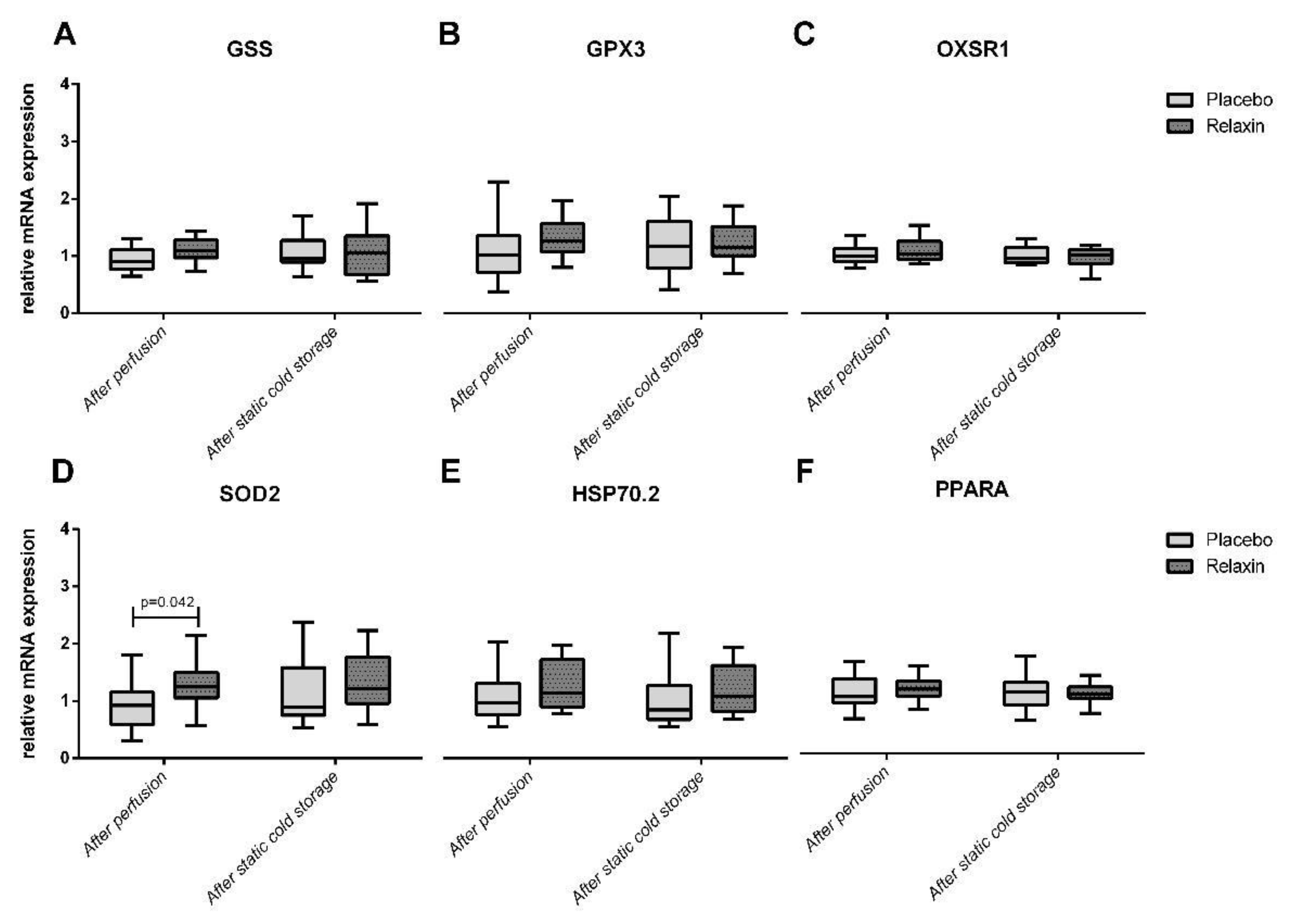
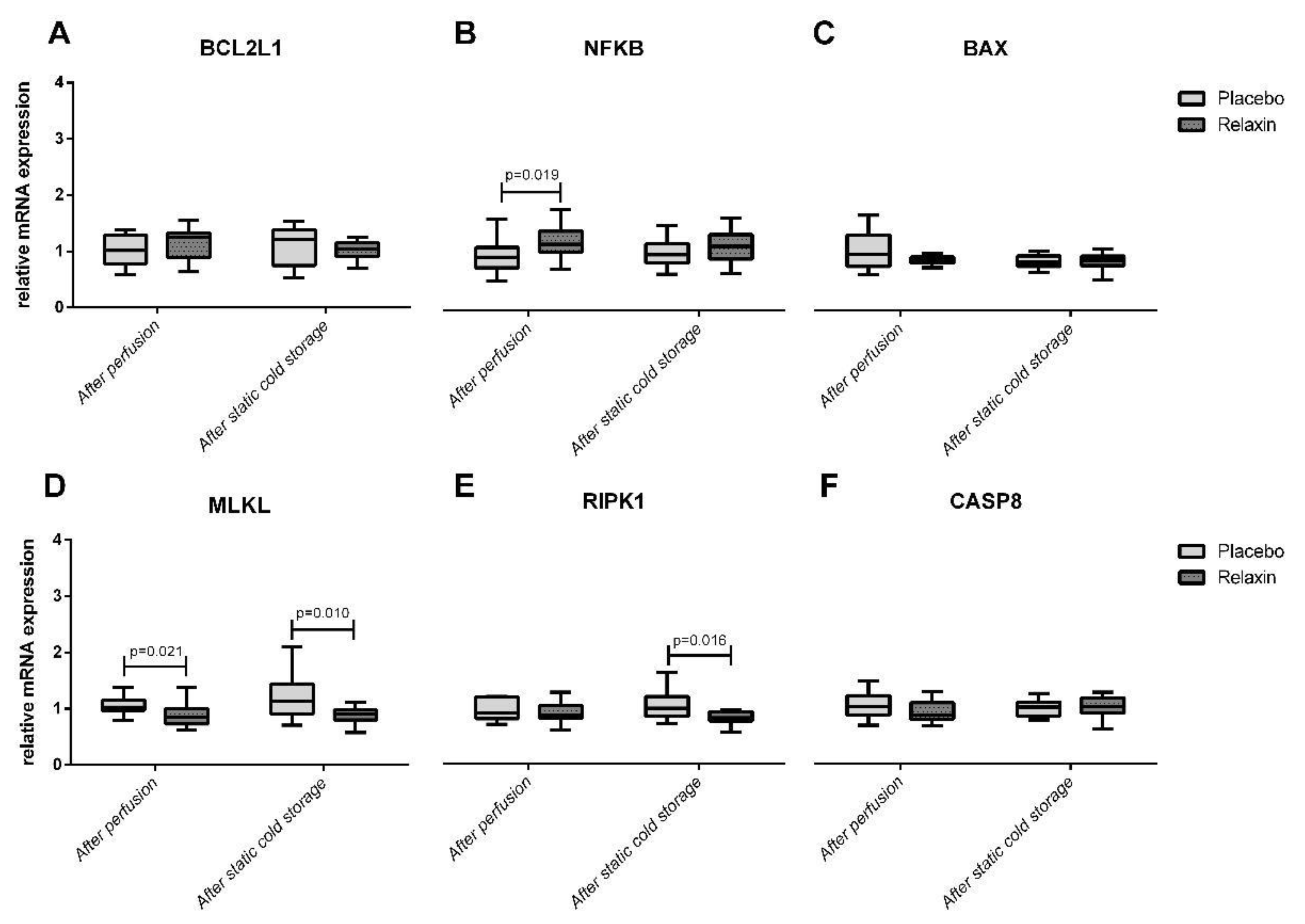
4.1. Apoptosis/Necroptosis Gene Expression after Kidney Perfusion and Static Cold Storage
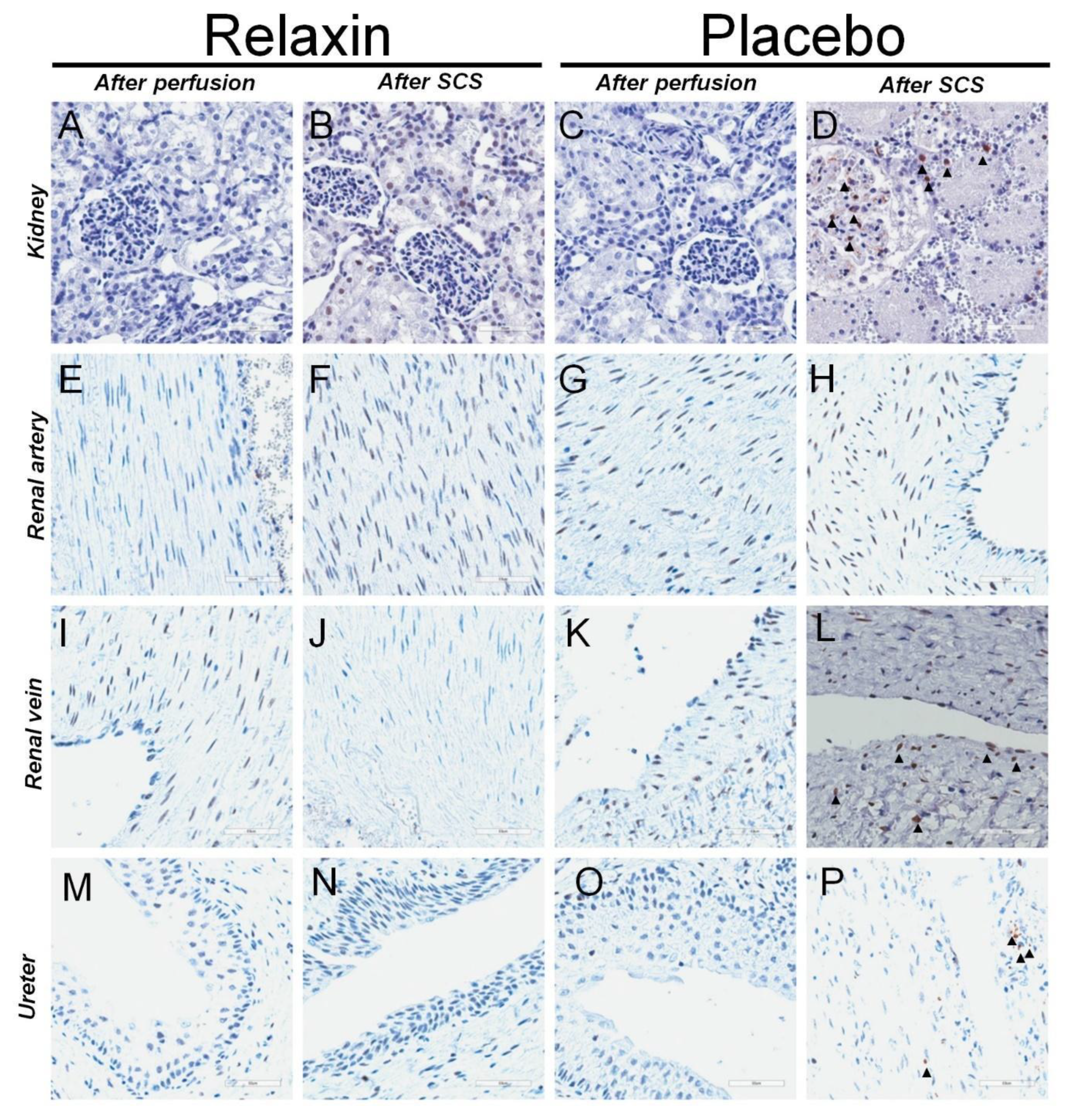
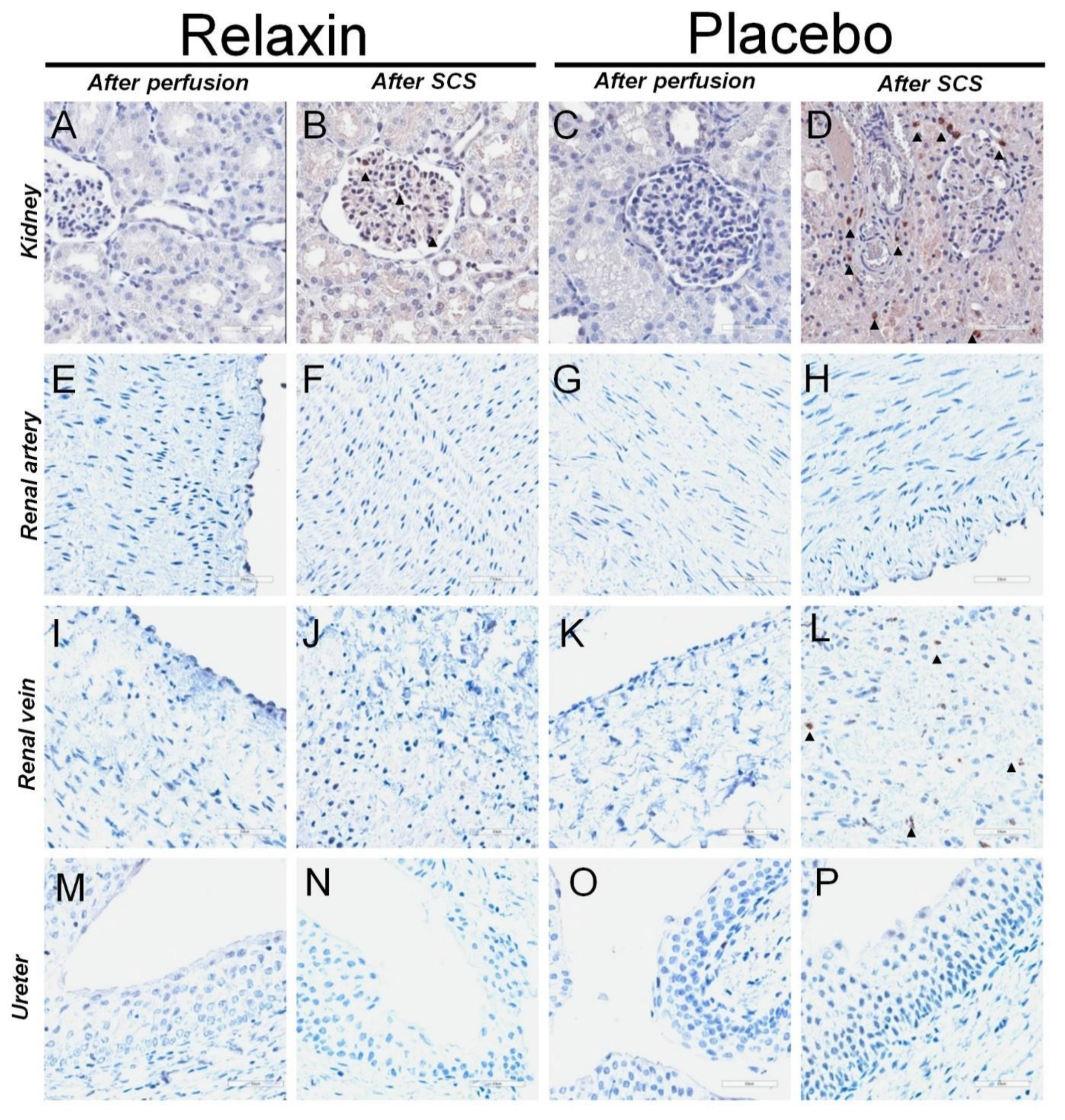
4.2. Immunohistochemistry for Caspase 3 and MPO in after Kidney Perfusion and Static Cold Storage
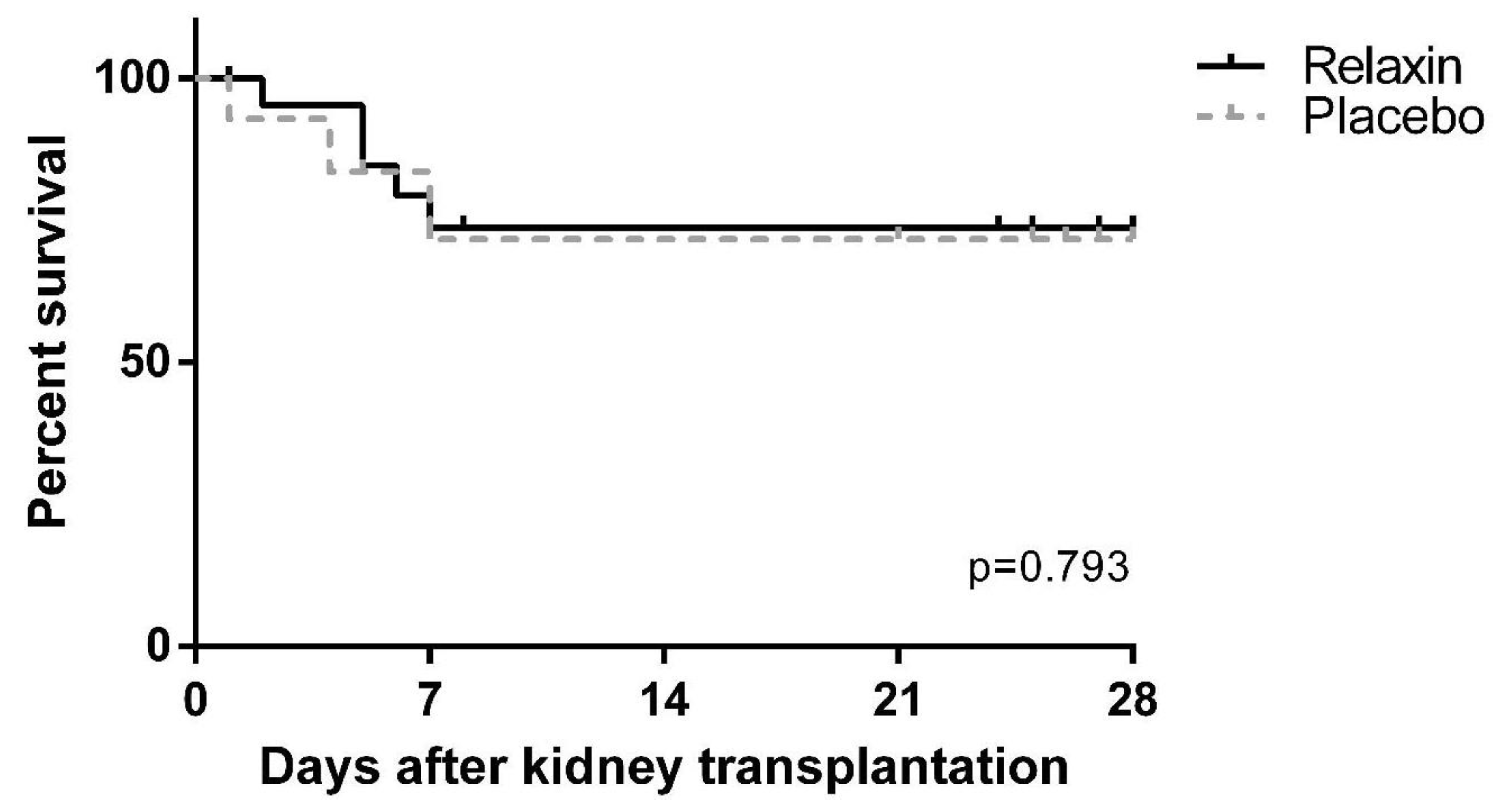
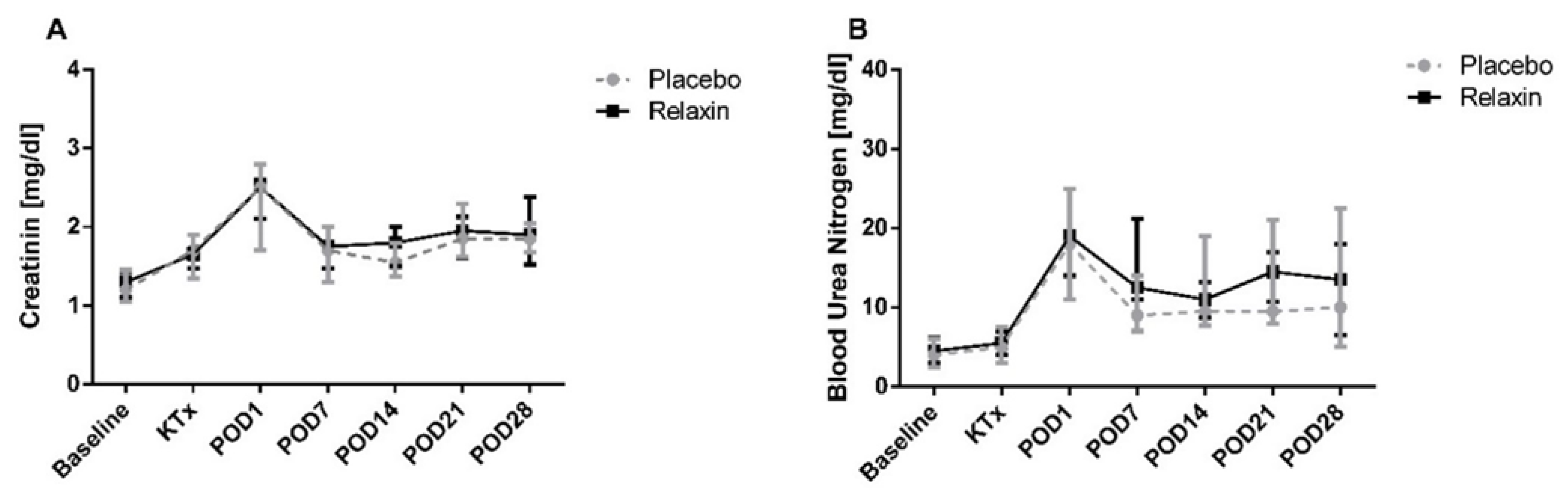
4.3. Kidney Transplantation and Graft Function
4.4. Subgroup Analysis
4.4.1. 24 vs. 48 h of SCS in Placebo and RLX Groups
4.4.2. High vs. Low Concentration of RLX
5. Discussion
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| IRI | Ischemia/reperfusion injury |
| ECD | extended criteria donor |
| SCS | Static cold storage |
| RLX | Relaxin-2 |
| POD | postoperative day |
| PCR | polymerase chain reaction |
| BUN | blood urea nitrogen |
| MPO | myeloperoxidase |
| ACTB | Actin Beta |
| GAPDH | Glyceraldehyde-3-Phosphate Dehydrogenase |
| GSS | Glutathione Synthetase |
| GPX3 | Glutathione Peroxidase 3 |
| OXSR1 | Oxidative Stress Responsive Kinase 1 |
| SOD2 | Superoxide Dismutase |
| HSP70.2 | Heat Shock Protein 70.2 |
| BCL2L1 | BCL2 Like 1 |
| PPARA | Peroxisome Proliferators Activated Receptor Alpha |
| NFKB1 | Nuclear Factor of Kappa Light Polypeptide Gene Enhancer in B-cells |
| MLKL | Mixed-lineage kinase domain-like protein) |
| BAX | BCL2 Associated X Protein |
| RIPK1 | Receptor Interacting Serine/Threonine Kinase 1 |
| CASP8 | Caspase 8 |
References
- Menke, J.; Sollinger, D.; Schamberger, B.; Heemann, U.; Lutz, J. The effect of ischemia/reperfusion on the kidney graft. Curr. Opin. Organ Transplant. 2014, 19, 395–400. [Google Scholar] [CrossRef]
- Nieuwenhuijs-Moeke, G.J.; Pischke, S.E.; Berger, S.P.; Sanders, J.S.F.; Pol, R.A.; Struys, M.M.R.F.; Ploeg, R.J.; Leuvenink, H.G.D. Ischemia and reperfusion injury in kidney transplantation: Relevant mechanisms in injury and repair. J. Clin. Med. 2020, 9, 253. [Google Scholar] [CrossRef] [Green Version]
- De Deken, J.; Rex, S.; Lerut, E.; Martinet, W.; Monbaliu, D.; Pirenne, J.; Jochmans, I. Postconditioning effects of argon or xenon on early graft function in a porcine model of kidney autotransplantation. Br. J. Surg. 2018, 105, 1051–1060. [Google Scholar] [CrossRef] [PubMed]
- Hosgood, S.A.; Mohamed, I.H.; Bagul, A.; Nicholson, M.L. Hypothermic machine perfusion after static cold storage does not improve the preservation condition in an experimental porcine kidney model. BJS 2011, 98, 943–950. [Google Scholar] [CrossRef] [PubMed]
- Jakubauskiene, L.; Jakubauskas, M.; Leber, B.; Strupas, K.; Stiegler, P.; Schemmer, P. Relaxin positively influences ischemia—Reperfusion injury in solid organ transplantation: A comprehensive review. Int. J. Mol. Sci. 2020, 21, 631. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lodhi, R.S.Z.; Nakabayashi, K.; Suzuki, K.; Yamada, A.Y.; Hazama, R.; Ebina, Y.; Yamada, H. Relaxin has anti-apoptotic effects on human trophoblast-derived HTR-8/SV neo cells. Gynecol. Endocrinol. 2013, 29, 1051–1054. [Google Scholar] [CrossRef] [PubMed]
- Lekgabe, E.D.; Kiriazis, H.; Zhao, C.; Xu, Q.; Moore, X.L.; Su, Y.; Bathgate, R.A.; Du, X.J.; Samuel, C.S. Relaxin reverses cardiac and renal fibrosis in spontaneously hypertensive rats. Hypertension 2005, 46, 412–418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teichman, S.L.; Unemori, E.; Teerlink, J.R.; Cotter, G.; Metra, M. Relaxin: Review of biology and potential role in treating heart failure. Curr. Heart Fail Rep. 2010, 7, 75–82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoshida, T.; Kumagai, H.; Kohsaka, T.; Ikegaya, N. Relaxin protects against renal ischemia-reperfusion injury. Am. J. Physiol. Renal. Physiol. 2013, 305, F1169–F1176. [Google Scholar] [CrossRef] [Green Version]
- Collino, M.; Rogazzo, M.; Pini, A.; Benetti, E.; Rosa, A.C.; Chiazza, F.; Fantozzi, R.; Bani, D.; Masini, E. Acute treatment with relaxin protects the kidney against Ischaemia/reperfusion injury. J. Cell Mol. Med. 2013, 17, 1494–1505. [Google Scholar] [CrossRef]
- Walchak, A.C.; Zarow, G.J.; Gamble, C.S.; Conley, S.P.; Hampshire, V. Simple blood typing and cross matching techniques in swine. Lab. Anim. 2016, 45, 366–368. [Google Scholar] [CrossRef] [PubMed]
- Tomsa, A.M.; Alexa, A.L.; Junie, M.L.; Rachisan, A.L.; Ciumarnean, L. Oxidative stress as a potential target in acute kidney injury. PeerJ 2019, 7, e8046. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.; Jang, H.-S.; Park, K.M. Reactive oxygen species generated by renal ischemia and reperfusion trigger protection against subsequent renal ischemia and reperfusion injury in mice. Am. J. Physiol. Ren. Physiol. 2009, 298, F158–F166. [Google Scholar] [CrossRef] [Green Version]
- Tabriziani, H.; Lipkowitz, M.S.; Vuong, N. Chronic kidney disease, kidney transplantation and oxidative stress: A new look to successful kidney transplantation. Clin. Kidney J. 2018, 11, 130–135. [Google Scholar] [CrossRef] [Green Version]
- Stiegler, P.; Sereinigg, M.; Puntschart, A.; Bradatsch, A.; Seifert-Held, T.; Wiederstein-Grasser, I.; Leber, B.; Stadelmeyer, E.; Dandachi, N.; Zelzer, S.; et al. Oxidative stress and apoptosis in a pig model of brain death (BD) and living donation (LD). J. Transl. Med. 2013, 11, 244. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pavlakou, P.; Liakopoulos, V.; Eleftheriadis, T.; Mitsis, M.; Dounousi, E. Oxidative stress and acute kidney injury in critical illness: Pathophysiologic Mechanisms—Biomarkers—Interventions, and future perspectives. Oxidat. Med. Cell. Longev. 2017, 2017, e6193694. [Google Scholar] [CrossRef] [Green Version]
- Kasahara, E.; Lin, L.-R.; Ho, Y.-S.; Reddy, V.N. Manganese superoxide dismutase protects against oxidation-induced apoptosis in mouse retinal pigment epithelium: Implications for age-related macular degeneration. Investig. Ophthalmol. Vis. Sci. 2005, 46, 3426–3434. [Google Scholar] [CrossRef]
- Atalla, S.L.; Toledo-Pereyra, L.H.; MacKenzie, G.H.; Cederna, J.P. Influence of oxygen-derived free radical scavengers on ischemic livers. Transplantation 1985, 40, 584–590. [Google Scholar] [CrossRef]
- Dimmeler, S.; Hermann, C.; Galle, J.; Zeiher, A.M. Upregulation of superoxide dismutase and nitric oxide synthase mediates the apoptosis-suppressive effects of shear stress on endothelial cells. Arterioscler. Thromb. Vasc. Biol. 1999, 19, 656–664. [Google Scholar] [CrossRef] [Green Version]
- Petrache, I.; Medler, T.R.; Richter, A.T.; Kamocki, K.; Chukwueke, U.; Zhen, L.; Gu, Y.; Adamowicz, J.; Schweitzer, K.S.; Hubbard, W.C.; et al. Superoxide dismutase protects against apoptosis and alveolar enlargement induced by ceramide. Am. J. Physiol. Lung Cell Mol. Physiol. 2008, 295, L44–L53. [Google Scholar] [CrossRef] [Green Version]
- Chang, C.; Worley, B.L.; Phaëton, R.; Hempel, N. Extracellular glutathione peroxidase GPx3 and its role in cancer. Cancers 2020, 12, 2197. [Google Scholar] [CrossRef] [PubMed]
- Hendrick, J.P.; Hartl, F.U. Molecular chaperone functions of heat-shock proteins. Annu. Rev. Biochem. 1993, 62, 349–384. [Google Scholar] [CrossRef] [PubMed]
- Marx, N.; Kehrle, B.; Kohlhammer, K.; Grüb, M.; Koenig, W.; Hombach, V.; Libby, P.; Plutzky, J. PPAR activators as antiinflammatory mediators in human T lymphocytes: Implications for atherosclerosis and transplantation-associated arteriosclerosis. Circ. Res. 2002, 90, 703–710. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuwabara, N.; Oyama, T.; Tomioka, D.; Ohashi, M.; Yanagisawa, J.; Shimizu, T.; Miyachi, H. Peroxisome proliferator-activated receptors (PPARs) have multiple binding points that accommodate ligands in various conformations: Phenylpropanoic acid-type PPAR ligands bind to PPAR in different conformations, depending on the subtype. J. Med. Chem. 2012, 55, 893–902. [Google Scholar] [CrossRef] [PubMed]
- Kahl, R.; Kampkötter, A.; Wätjen, W.; Chovolou, Y. Antioxidant enzymes and apoptosis. Drug Metab. Rev. 2004, 36, 747–762. [Google Scholar] [CrossRef]
- Jiang, Z.; Zhang, H.; Böckmann, R.A. Allostery in BAX protein activation. J. Biomol. Struct. Dyn. 2016, 34, 2469–2480. [Google Scholar] [CrossRef]
- Ghaemi, S.; Arefian, E.; Rezazadeh Valojerdi, R.; Soleimani, M.; Moradimotlagh, A.; Jamshidi Adegani, F. Inhibiting the expression of anti-apoptotic genes BCL2L1 and MCL1, and apoptosis induction in glioblastoma cells by microRNA-342. Biomed. Pharmacother. 2020, 121, 109641. [Google Scholar] [CrossRef]
- Sanz, A.B.; Sanchez-Niño, M.D.; Ramos, A.M.; Moreno, J.A.; Santamaria, B.; Ruiz-Ortega, M.; Egido, J.; Ortiz, A. NF-κB in renal inflammation. JASN 2010, 21, 1254–1262. [Google Scholar] [CrossRef] [Green Version]
- He, K.; Chen, X.; Han, C.; Xu, L.; Zhang, J.; Zhang, M.; Xia, Q. Lipopolysaccharide-induced cross-tolerance against renal ischemia–reperfusion injury is mediated by hypoxia-inducible factor-2α-regulated nitric oxide production. Kidney Int. 2014, 85, 276–288. [Google Scholar] [CrossRef] [Green Version]
- Song, N.; Thaiss, F.; Guo, L. NFκB and kidney injury. Front. Immunol. 2019, 10, 815. [Google Scholar] [CrossRef]
- Zhang, X.; Dowling, J.P.; Zhang, J. RIPK1 can mediate apoptosis in addition to necroptosis during embryonic development. Cell Death Dis. 2019, 10, 1–11. [Google Scholar] [CrossRef]
- Yoon, S.; Kovalenko, A.; Bogdanov, K.; Wallach, D. MLKL, the protein that mediates necroptosis, also regulates endosomal trafficking and extracellular vesicle generation. Immunity 2017, 47, 51–65. [Google Scholar] [CrossRef] [Green Version]
- Cao, W.-X.; Li, T.; Tang, Z.-H.; Zhang, L.L.; Wang, Z.Y.; Guo, X.; Su, M.X.; Chen, X.; Lu, J.J. MLKL mediates apoptosis via a mutual regulation with PERK/eIF2α pathway in response to reactive oxygen species generation. Apoptosis 2018, 23, 521–531. [Google Scholar] [CrossRef]
- Baidya, R.; Gautheron, J.; Crawford, D.H.G.; Wang, H.; Bridle, K.R. Inhibition of MLKL attenuates necroptotic cell death in a murine cell model of Ischaemia injury. J. Clin. Med. 2021, 10, 212. [Google Scholar] [CrossRef]
- Lau, A.; Wang, S.; Jiang, J.; Haig, A.; Pavlosky, A.; Linkermann, A.; Zhang, Z.X.; Jevnikar, A.M. RIPK3-mediated necroptosis promotes donor kidney inflammatory injury and reduces allograft survival. Am. J. Transplant. 2013, 13, 2805–2818. [Google Scholar] [CrossRef] [PubMed]
- Linkermann, A.; Bräsen, J.H.; Himmerkus, N.; Liu, S.; Huber, T.B.; Kunzendorf, U.; Krautwald, S. Rip1 (receptor-interacting protein kinase 1) mediates necroptosis and contributes to renal ischemia/reperfusion injury. Kidney Int. 2012, 81, 751–761. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, H.; Zamel, R.; Bai, X.-H.; Lu, C.; Keshavjee, S.; Keshavjee, S.; Liu, M. Ischemia-reperfusion induces death receptor-independent necroptosis via calpain-STAT3 activation in a lung transplant setting. Am. J. Physiol. Lung Cell Mol. Physiol. 2018, 315, L595–L608. [Google Scholar] [CrossRef] [PubMed]
- Matthijsen, R.A.; Huugen, D.; Hoebers, N.T.; de Vries, B.; Peutz-Kootstra, C.J.; Aratani, Y.; Daha, M.R.; Tervaert, J.W.; Buurman, W.A.; Heeringa, P. Myeloperoxidase is critically involved in the induction of organ damage after renal Ischemia reperfusion. Am. J. Pathol. 2007, 171, 1743–1752. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gurel, A.; Armutcu, F.; Sahin, S.; Sogut, S.; Ozyurt, H.; Gulec, M.; Kutlu, N.O.; Akyol, O. Protective role of α-tocopherol and caffeic acid phenethyl ester on ischemia–reperfusion injury via nitric oxide and myeloperoxidase in rat kidneys. Clin. Chim. Acta 2004, 339, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Kageyama, S.; Nakamura, K.; Ke, B.; Busuttil, R.W.; Kupiec-Weglinski, J.W. Serelaxin induces Notch1 signaling and alleviates hepatocellular damage in orthotopic liver transplantation. Am. J. Transplant. 2018, 18, 1755–1763. [Google Scholar] [CrossRef] [Green Version]
- Kageyama, S.; Nakamura, K.; Fujii, T.; Ke, B.; Sosa, R.A.; Reed, E.F.; Datta, N.; Zarrinpar, A.; Busuttil, R.W.; Kupiec-Weglinski, J.W. Recombinant relaxin protects liver transplants from ischemia damage via hepatocyte glucocorticoid receptor: From bench-to-bedside. Hepatology 2018, 68, 258–273. [Google Scholar] [CrossRef]
- Zonta, S.; Alessiani, M.; Abbiati, F.; Fayer, F.; Zitelli, E.; Bardone, M.C.; Cobianchi, I.; Lovisetto, F.; Piccioni, P.F.; Burroni, B.; et al. Experimental kidney transplantation: A comparison between different models. Minerva Chirurgica 2003, 58, 755–767. [Google Scholar]
- He, B.; Musk, G.C.; Mou, L.; Waneck, G.L.; Delriviere, L. Laparoscopic kidney orthotopic transplant: Preclinical study in the pig model. Transplant. Proc. 2013, 45, 1776–1779. [Google Scholar] [CrossRef]
- Boehnert, M.U.; Hilbig, H.; Armbruster, F.P. Relaxin as an additional protective substance in preserving and reperfusion solution for liver transplantation, shown in a model of isolated perfused rat liver. Ann. N. Y. Acad. Sci. 2005, 1041, 434–440. [Google Scholar] [CrossRef]
- Boehnert, M.U.; Armbruster, F.P.; Hilbig, H. Relaxin as a protective substance in the preserving solution for liver transplantation: Spectrophotometric in vivo imaging of local oxygen supply in an isolated perfused rat liver model. Ann. N. Y. Acad. Sci. 2009, 1160, 320–321. [Google Scholar] [CrossRef] [PubMed]
- Boehnert, M.U.; Armbruster, F.P.; Hilbig, H. Relaxin as a protective substance in preservation solutions for organ transplantation, as shown in an isolated perfused rat liver model. Transplant. Proc. 2008, 40, 978–980. [Google Scholar] [CrossRef]
- Alexiou, K.; Matschke, K.; Westphal, A.; Stangl, K.; Dschietzig, T. Relaxin is a candidate drug for lung preservation: Relaxin-induced protection of rat lungs from ischemia-reperfusion injury. J. Heart Lung Transplant. 2010, 29, 454–460. [Google Scholar] [CrossRef] [PubMed]
- Masini, E.; Bani, D.; Sardi, I.; Baronti, R.; Bani-Sacchi, T.; Bigazzi, M.; Mannaioni, P.F. Dual role of nitric oxide in myocardial ischemia-reperfusion. Inflamm Res. 2000, 49 (Suppl. 1), S78–S79. [Google Scholar] [CrossRef]
- Valle Raleigh, J.; Mauro, A.G.; Devarakonda, T.; Marchetti, C.; He, J.; Kim, E.; Filippone, S.; Das, A.; Toldo, S.; Abbate, A.; et al. Reperfusion therapy with recombinant human relaxin-2 (Serelaxin) attenuates myocardial infarct size and NLRP3 inflammasome following ischemia/reperfusion injury via eNOS-dependent mechanism. Cardiovasc. Res. 2017, 113, 609–619. [Google Scholar] [CrossRef] [Green Version]
- Giraud, S.; Favreau, F.; Chatauret, N.; Thuillier, R.; Maiga, S.; Hauet, T. Contribution of large pig for renal ischemia-reperfusion and transplantation studies: The preclinical model. J. Biomed. Biotechnol. 2011, 2011, e532127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dehoux, J.-P.; Gianello, P. The importance of large animal models in transplantation. Front. Biosci. 2007, 12, 4864–4880. [Google Scholar] [CrossRef] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Accession Number | Forward (5′- > 3′) | Reverse (5′- > 3′) | Product Length |
|---|---|---|---|
| ACTB (Actin Beta) | |||
| XM_021086047.1 XM_003124280.5 | CTCCAGAGCGCAAGTACTCC | ACTCCTGCTTGCTGATCCAC | 90 bp |
| GAPDH (Glyceraldehyde-3-Phosphate Dehydrogenase) | |||
| NM_001206359.1 | CCGTGTGTTCCGTGCATTG | GCCAAATCCGTTCACTCCGA | 71 bp |
| GSS (Glutathione Synthetase) [15] | |||
| NM_001244625.1 | AAGAAGCTGCCAAGATCCTC | ATTCTCTATGGCACGCTGGT | 155 bp |
| GPX3 (Glutathione Peroxidase 3) [15] | |||
| NM_001115155.1 | GAGACAACTCGGAGATTCTG | GGAACGTGTAGAACTTCTGC | 126 bp |
| OXSR1 (Oxidative Stress Responsive Kinase 1) [15] | |||
| NM_214342.1 | CCGAAGTTATGGAACAGGTC | GATCATTCTGCAGTGTCAGC | 147 bp |
| SOD2 (Superoxide Dismutase 2) [15] | |||
| NM_214127 | CCTACGTGAACAACCTGAAC | GATACAGCGGTCAACTTCTC | 247 bp |
| HSP70.2 (Heat Shock Protein 70.2) [15] | |||
| NM_213766.1 | AGGTGCAGGTGAGCTACAAG | CTGCGAGTCGTTGAAGTAGG | 158 bp |
| PPARA (Peroxisome Proliferators Activated Receptor Alpha) [15] | |||
| NM_001044526.1 | TGAAGTTCAATGCGCTGGAG | TTGAGCACATGCACGATACC | 139 bp |
| BCL2 L1 (BCL2 Like 1) [15] | |||
| NM_214285.1 | TGAGTCGGATCGCAACTTGG | ATCGGTTGAAGCGTTCCTGG | 150 bp |
| NFKB1 (Nuclear Factor of Kappa Light Polypeptide Gene Enhancer in B-cells) [15] | |||
| NM_001048232.1 | GAGGTGCATCTGACGTATTC | CACATCTCCTGTCACTGCAT | 138 bp |
| BAX (BCL2 Associated X Protein) [15] | |||
| XM_003127290 | GCTGACGGCAACTTCAACTG | CCGATCTCGAAGGAAGTCCA | 141 bp |
| MLKL (Mixed-lineage kinase domain-like protein) | |||
| XM_003481791.4 | TTGGAAAACACCACGAGGGA | CCCTTCTTGGGTTTGTGTGC | 77 bp |
| RIPK1 (Receptor Interacting Serine/Threonine Kinase 1) | |||
| XM_005665536 | CACTCGGAGAAATCAAGGCAG | CTGCGCCCTGATGGTTACAAAA | 86 bp |
| CASP8 (Caspase 8) | |||
| NM_001031779.2 | CCAGGATTTGCCTCCGGTTA | TCACTGTCCAAATGTTCCCCA | 99 bp |
| Caspase 3 | Myeloperoxidase | ||||||
|---|---|---|---|---|---|---|---|
| RLX | Placebo | p Value | RLX | Placebo | p Value | ||
| Kidney | After perfusion | 0 (0; 0) | 0 (0; 0) | 0.999 | 0 (0; 0) | 0 (0; 0) | 0.999 |
| After SCS | 0 (0; 0.5) | 1 (0; 1.6) | 0.005 | 0 (0; 0.5) | 1 (0; 1.3) | 0.017 | |
| Renal artery | After perfusion | 0 (0; 0) | 0 (0; 0) | 0.999 | 0 (0; 0) | 0 (0; 0) | 0.999 |
| After SCS | 0 (0; 0) | 0 (0; 0.2) | 0.650 | 0 (0; 0) | 0 (0; 0) | 0.660 | |
| Renal vein | After perfusion | 0 (0; 0) | 0 (0; 0) | 0.811 | 0 (0; 0) | 0 (0; 0) | 0.999 |
| After SCS | 0 (0; 0) | 0.8 (0; 1) | 0.027 | 0 (0; 0) | 0 (0; 1) | 0.066 | |
| Ureter | After perfusion | 0 (0; 0) | 0 (0; 0) | 0.999 | 0 (0; 0) | 0 (0; 0) | 0.999 |
| After SCS | 0 (0; 0) | 0.6 (0; 1) | 0.019 | 0 (0; 0) | 0 (0; 0) | 0.839 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bausys, A.; Maneikyte, J.; Leber, B.; Weber, J.; Feldbacher, N.; Strupas, K.; Dschietzig, T.B.; Schemmer, P.; Stiegler, P. Custodiol® Supplemented with Synthetic Human Relaxin Decreases Ischemia-Reperfusion Injury after Porcine Kidney Transplantation. Int. J. Mol. Sci. 2021, 22, 11417. https://doi.org/10.3390/ijms222111417
Bausys A, Maneikyte J, Leber B, Weber J, Feldbacher N, Strupas K, Dschietzig TB, Schemmer P, Stiegler P. Custodiol® Supplemented with Synthetic Human Relaxin Decreases Ischemia-Reperfusion Injury after Porcine Kidney Transplantation. International Journal of Molecular Sciences. 2021; 22(21):11417. https://doi.org/10.3390/ijms222111417
Chicago/Turabian StyleBausys, Augustinas, Juste Maneikyte, Bettina Leber, Jennifer Weber, Nicole Feldbacher, Kestutis Strupas, Thomas Bernd Dschietzig, Peter Schemmer, and Philipp Stiegler. 2021. "Custodiol® Supplemented with Synthetic Human Relaxin Decreases Ischemia-Reperfusion Injury after Porcine Kidney Transplantation" International Journal of Molecular Sciences 22, no. 21: 11417. https://doi.org/10.3390/ijms222111417