
Prognostic Role of Tumoral PD-L1 and IDO1 Expression, and Intratumoral CD8+ and FoxP3+ Lymphocyte Infiltrates in 132 Primary Cutaneous Merkel Cell Carcinomas

 , , ,
, , ,
Abstract
:1. Introduction
2. Results
2.1. Positive MCPyV Status Correlated with Tumoral PD-L1 Expression and High Intratumoral CD8+ Cell Count
2.2. Tumoral PD-L1 Expression Correlated with Intratumoral CD8+ and FoxP3+ Lymphocytes, Which Is Supportive of an Adaptive Immune Response
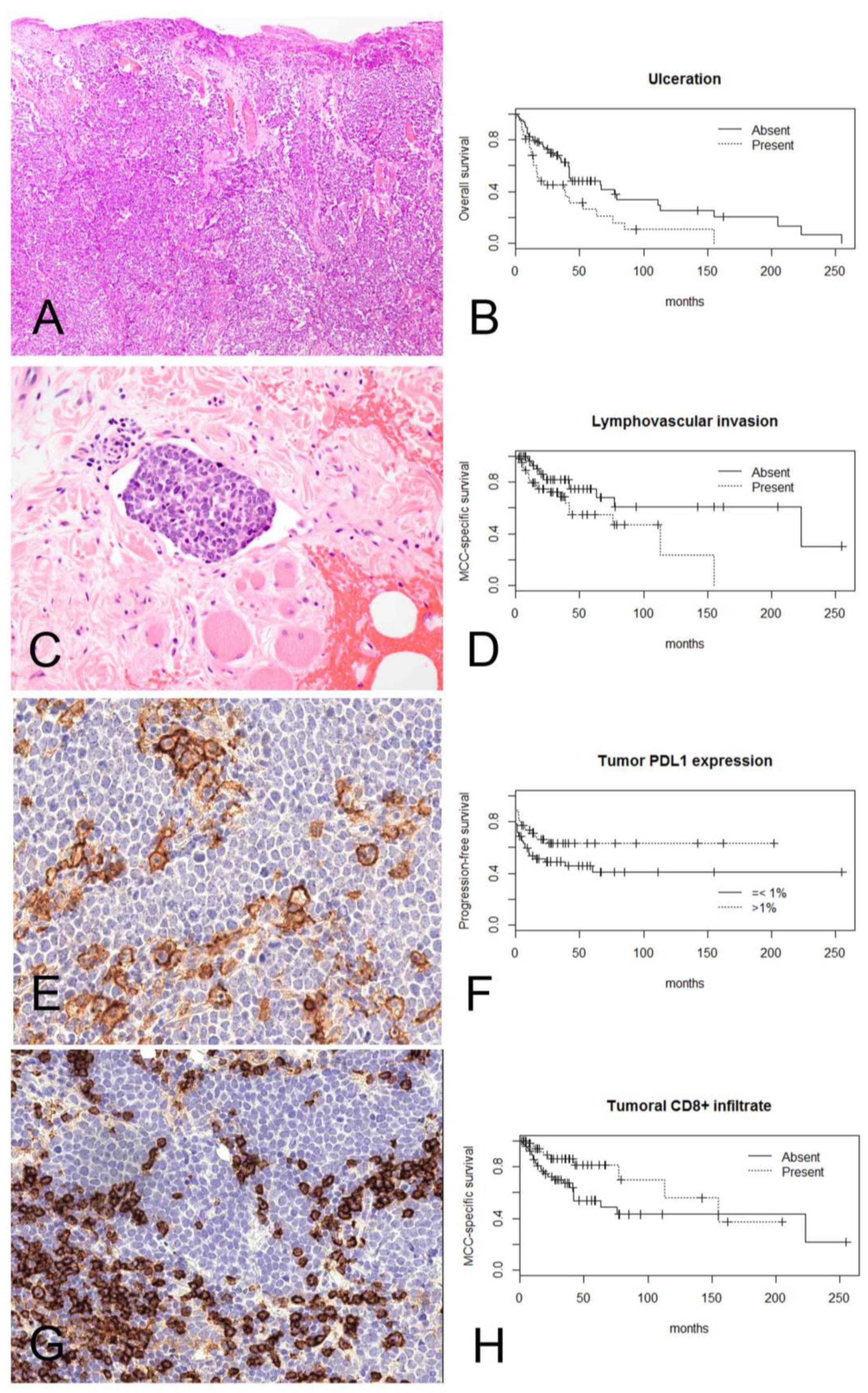
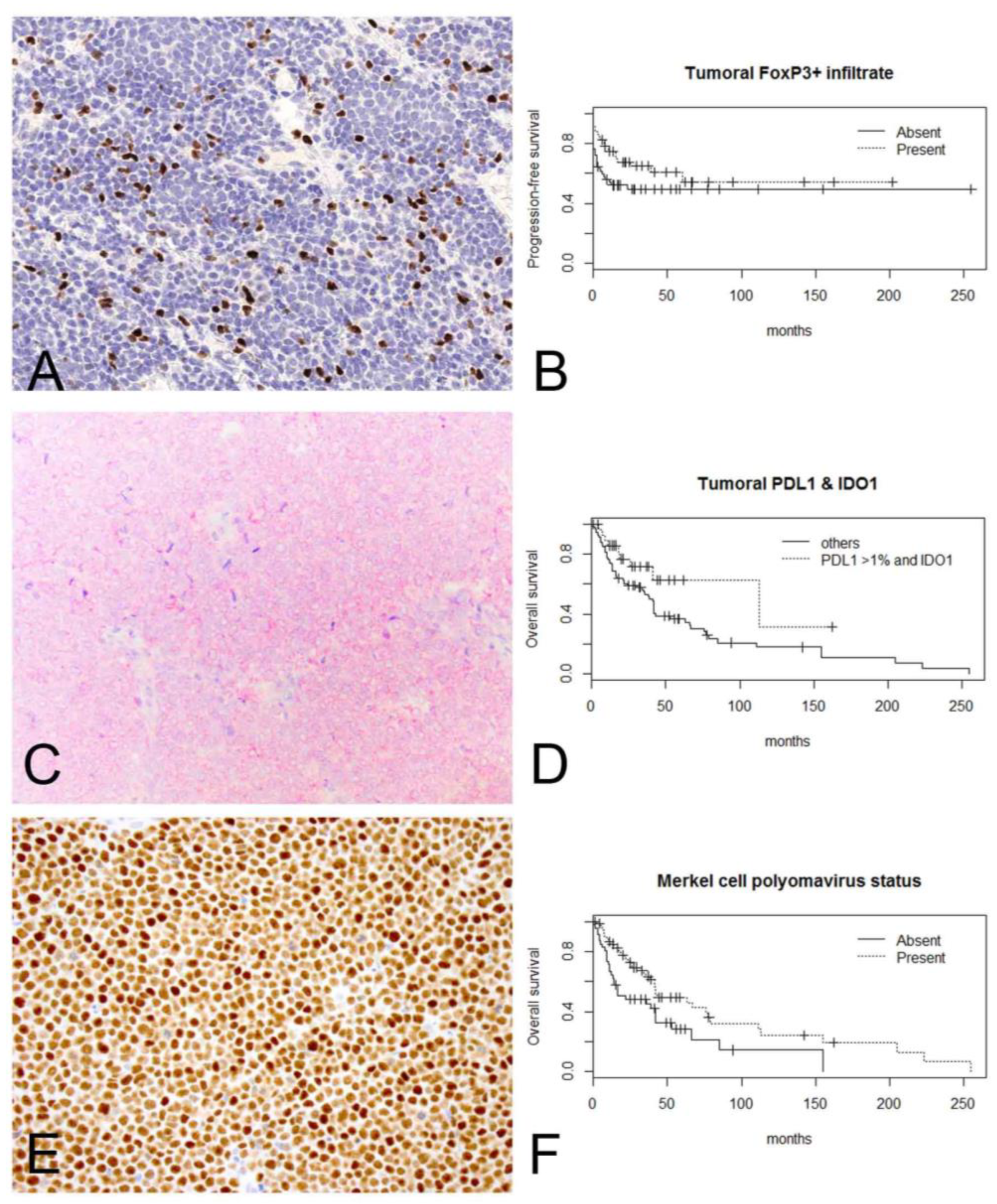
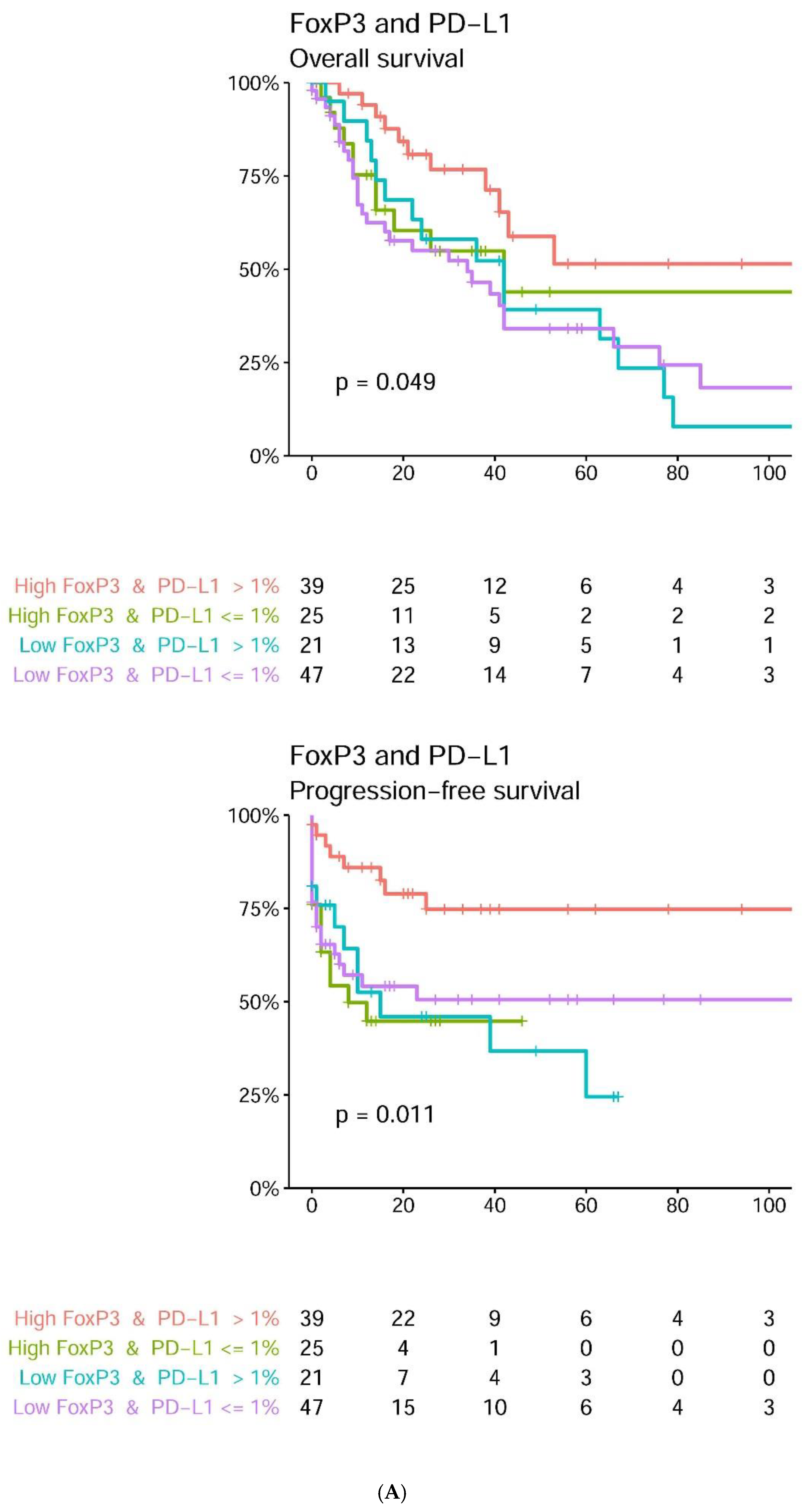
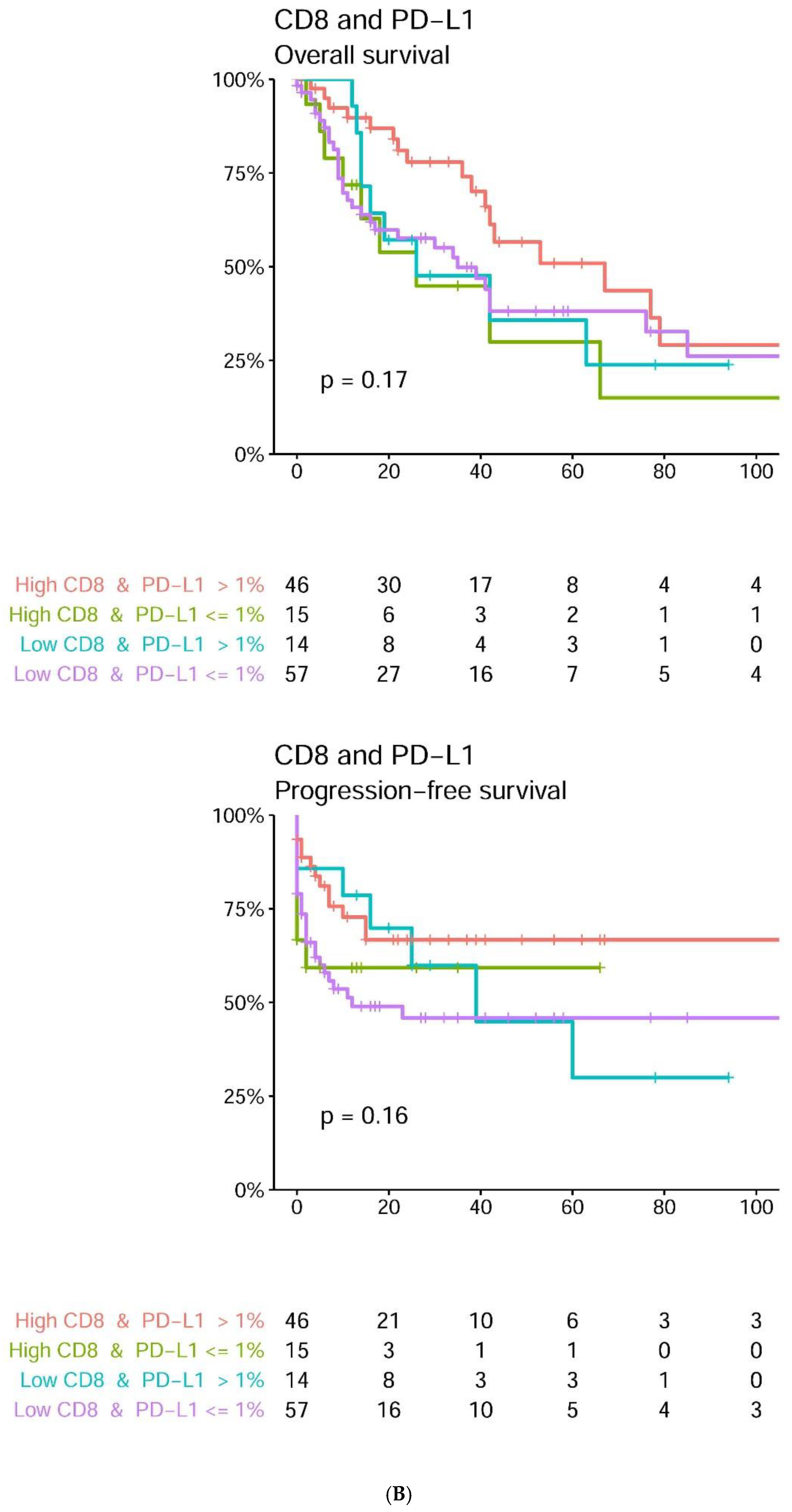
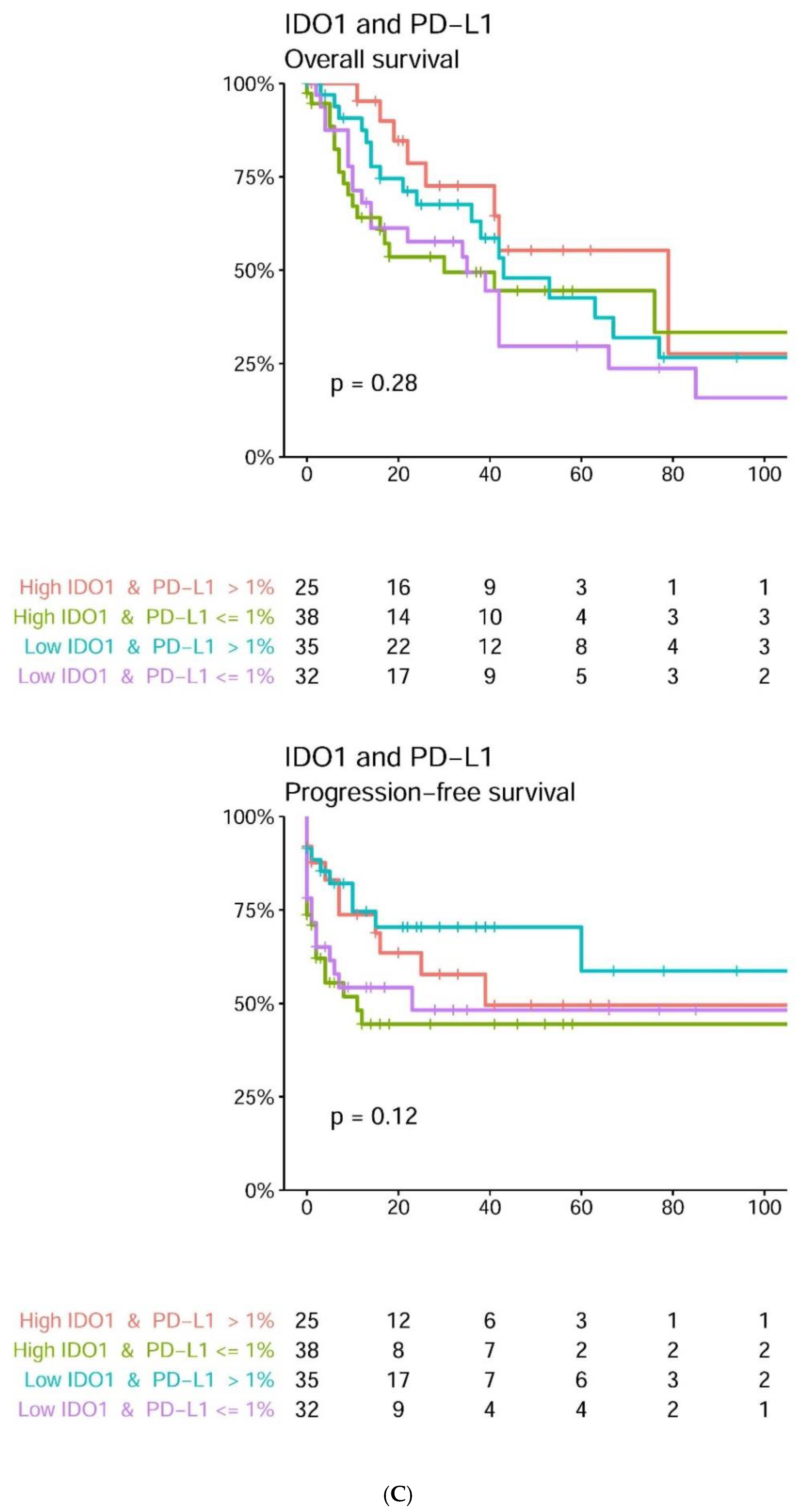
2.3. Tumoral PD-L1 Expression and Increased Density of Intratumoral CD8+ Lymphocytes and FoxP3+ Lymphocytes May Positively Impact Survival in a Subset of MCCs
2.4. By Multivariate Analyses, Ulceration and Age Are Independent Predictors of Worse OS; and Gender and Stage Are Independent Predictors of Shorter PFS
3. Discussion
4. Materials and Methods
4.1. Clinical Findings and Histologic Features
4.2. Immunohistochemistry
4.3. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Coggshall, K.; Tello, T.L.; North, J.P.; Yu, S.S. Merkel cell carcinoma: An update and review: Pathogenesis, diagnosis, and staging. J. Am. Acad. Dermatol. 2018, 78, 433–442. [Google Scholar] [CrossRef] [Green Version]
- Von der Grün, J.; Winkelmann, R.; Meissner, M.; Wieland, U.; Silling, S.; Martin, D.; Fokas, E.; Rödel, C.; Rödel, F.; Balermpas, P. Merkel Cell Polyoma viral load and intratumoral CD8+ lymphocyte infiltration predict overall survival in patients with Merkel cell carcinoma. Front. Oncol. 2019, 9, 20. [Google Scholar] [CrossRef] [Green Version]
- Sihto, H.; Böhling, T.; Kavola, H.; Koljonen, V.; Salmi, M.; Jalkanen, S.; Joensuu, H. Tumor infiltrating immune cells and outcome of Merkel cell carcinoma: A population-based study. Clin. Cancer Res. 2012, 18, 2872–2881. [Google Scholar] [CrossRef] [Green Version]
- Paulson, K.G.; Iyer, J.G.; Tegeder, A.R.; Thibodeau, R.; Schelter, J.; Koba, S.; Schrama, D.; Simonson, W.T.; Lemos, B.D.; Byrd, D.R.; et al. Transcriptome-wide studies of Merkel cell carcinoma and validation of intratumoral CD8+ lymphocyte invasion as an independent predictor of survival. J. Clin. Oncol. 2011, 29, 1539–1546. [Google Scholar] [CrossRef] [Green Version]
- Bilir, C.; Sarisozen, C. Indoleamine 2,3-dioxygenase (IDO): Only an enzyme or a checkpoint controller? J. Oncol. Sci. 2017, 3, 52–56. [Google Scholar] [CrossRef]
- Munn, D.H.; Mellor, A.L. Indoleamine 2,3-dioxygenase and tumor-induced tolerance. J. Clin. Investig. 2007, 117, 1147–1154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brochez, L.; Chevolet, I.; Kruse, V. The rationale of indoleamine 2,3-dioxygenase inhibition for cancer therapy. Eur. J. Cancer 2017, 76, 167–182. [Google Scholar] [CrossRef] [PubMed]
- Jacquemier, J.; Bertucci, F.; Finetti, P.; Esterni, B.; Charafe-Jauffret, E.; Thibult, M.L.; Houvenaeghel, G.; Van den Eynde, B.; Birnbaum, D.; Olive, D.; et al. High expression of indoleamine 2,3-dioxygenase in the tumour is associated with medullary features and favourable outcome in basal-like breast carcinoma. Int. J. Cancer 2012, 130, 96–104. [Google Scholar] [CrossRef] [PubMed]
- Wardhani, L.O.; Matsushita, M.; Iwasaki, T.; Kuwamoto, S.; Nonaka, D.; Nagata, K.; Kato, M.; Kitamura, Y.; Hayashi, K. Expression of the IDO1/TDO2-AhR pathway in tumor cells or the tumor microenvironment is associated with Merkel cell polyomavirus status and prognosis in Merkel cell carcinoma. Hum. Pathol. 2019, 84, 52–61. [Google Scholar] [CrossRef] [Green Version]
- Barkdull, S.; Brownell, I. PDL1 blockade with avelumab: A new paradigm for treating Merkel cell carcinoma. Cancer Biol. Ther. 2017, 18, 937–939. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nghiem, P.T.; Bhatia, S.; Lipson, E.J.; Kudchadkar, R.R.; Miller, N.J.; Annamalai, L.; Berry, S.; Chartash, E.K.; Daud, A.; Fling, S.P.; et al. PD1 blockade with Pembrolizumab in advanced Merkel cell carcinoma. N. Engl. J. Med. 2016, 374, 2542–2552. [Google Scholar] [CrossRef] [PubMed]
- Lipson, E.J.; Vincent, J.G.; Loyo, M.; Kagohara, L.T.; Luber, B.S.; Wang, H.; Xu, H.; Nayar, S.K.; Wang, T.S.; Sidransky, D.; et al. PD-L1 expression in the Merkel cell carcinoma microenvironment: Association with inflammation, Merkel cell polyomavirus and overall survival. Cancer Immunol. Res. 2013, 1, 54–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feldmeyer, L.; Hudgens, C.W.; Ray-Lyons, G.; Nagarajan, P.; Aung, P.P.; Curry, J.L.; Torres-Cabala, C.A.; Mino, B.; Rodriguez-Canales, J.; Reuben, A.; et al. Density, distribution, and composition of immune infiltrates correlate with survival in Merkel cell carcinoma. Clin. Cancer Res. 2016, 22, 5553–5563. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wehkamp, U.; Stern, S.; Krüger, S.; Weichenthal, M.; Hauschild, A.; Röcken, C.; Egberts, F. Co-expression of NGF and PD-L1 on tumor-associated immune cells in the microenvironment of Merkel cell carcinoma. J. Cancer Res. Clin. Oncol. 2018, 144, 1301–1308. [Google Scholar] [CrossRef] [PubMed]
- Micevic, G.; Thakral, D.; McGeary, M.; Bosenberg, M.W. PD-L1 methylation regulates PD-L1 expression and is associated with melanoma survival. Pigment Cell Melanoma Res. 2019, 32, 435–440. [Google Scholar] [CrossRef]
- Ozaki, Y.; Edelstein, M.P.; Duch, D.S. Induction of indoleamine 2,3-dioxygenaseda mechanism of the antitumor-activity of interferon-gamma. Proc. Natl. Acad. Sci. USA 1988, 85, 1242–1246. [Google Scholar] [CrossRef] [Green Version]
- Takikawa, O.; Kuroiwa, T.; Yamazaki, F.; Kido, R. Mechanism of interferon-gamma action and characterization of indoleamine 2,3- dioxygenase in cultured human-cells induced by interferon gamma and evaluation of the enzyme-mediated tryptophan degradation in its anticellular activity. J. Biol. Chem. 1988, 263, 2041–2048. [Google Scholar] [CrossRef]
- Schalper, K.A.; Carvajal-Hausdorf, D.; McLaughlin, J.; Altan, M.; Velcheti, V.; Gaule, P.; Sanmamed, M.F.; Chen, L.; Herbst, R.S.; Rimm, D.L. Differential expression and significance of PD-L1, IDO-1, and B7-H4 in human lung cancer. Clin. Cancer Res. 2017, 23, 370–378. [Google Scholar] [CrossRef] [Green Version]
- Prendergast, G.C.; Malachowski, W.P.; DuHadaway, J.B.; Muller, A.J. Discovery of IDO1 inhibitors: From bench to bedside. Cancer Res. 2017, 77, 6795–6811. [Google Scholar] [CrossRef] [Green Version]
- Mitchell, T.C.; Hamid, O.; Smith, D.C.; Bauer, T.M.; Wasser, J.S.; Olszanski, A.J.; Luke, J.J.; Balmanoukian, A.S.; Schmidt, E.V.; Zhao, Y.; et al. Epacadostat plus pembrolizumab in patients with advanced solid tumors: Phase I results from a multicenter, open-label phase I/II trial (ECHO-202/KEYNOTE-037). J. Clin. Oncol. 2018, 36, 3223–3230. [Google Scholar] [CrossRef]
- Walsh, N.M.; Fleming, K.E.; Hanly, J.G.; Dakin Hache, K.; Doucette, S.; Ferrara, G.; Cerroni, L. A morphological and immunophenotypic map of the immune response in Merkel cell carcinoma. Hum. Pathol. 2016, 52, 190–196. [Google Scholar] [CrossRef] [PubMed]
- Wheat, R.; Roberts, C.; Waterboer, T.; Steele, J.; Marsden, J.; Steven, N.M.; Blackbourn, D.J. Inflammatory cell distribution in primary Merkel cell carcinomas. Cancers 2014, 6, 1047–1064. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dowlatshahi, M.; Huang, V.; Gehad, A.E.; Jiang, Y.; Calarese, A.; Teague, J.E.; Dorosario, A.A.; Cheng, J.; Nghiem, P.; Schanbacher, C.F.; et al. Tumor-specific T cells in human Merkel cell carcinomas: A possible role for Tregs and T-cell exhaustion in reducing T-cell responses. J. Investig. Dermatol. 2013, 133, 1879–1889. [Google Scholar] [CrossRef] [Green Version]
- Jin, H.T.; Ahmed, R.; Okazaki, T. Role of PD-1 in regulating T-cell immunity. Curr. Top. Microbiol. Immunol. 2011, 350, 17–37. [Google Scholar] [PubMed]
- Mitteldorf, C.; Berisha, A.; Tronnier, M.; Pfaltz, M.C.; Kempf, W. PD-1 and PD-L1 in neoplastic cells and the tumor microenvironment of Merkel cell carcinoma. J. Cutan. Pathol. 2017, 44, 740–746. [Google Scholar] [CrossRef] [PubMed]
- Afanasiev, O.K.; Yelistratova, L.; Miller, N.; Nagase, K.; Paulson, K.; Iyer, J.G.; Ibrani, D.; Koelle, D.M.; Nghiem, P. Merkel polyomavirus-specific T cells fluctuate with Merkel cell carcinoma burden and express therapeutically targetable PD-1 and Tim-3 exhaustion markers. Clin. Cancer Res. 2013, 19, 5351–5360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taube, J.M.; Anders, R.A.; Young, G.D.; Xu, H.; Sharma, R.; McMiller, T.L.; Chen, S.; Klein, A.P.; Pardoll, D.M.; Chen, L. Colocalization of inflammatory response with B7-h1 expression in human melanocytic lesions supports an adaptive resistance mechanism of immune escape. Sci. Transl. Med. 2012, 4, 127ra37. [Google Scholar] [CrossRef] [Green Version]
- Miller, N.J.; Church, C.D.; Dong, L.; Crispin, D.; Fitzgibbon, M.P.; Lachance, K.; Jing, L.; Shinohara, M.; Gavvovidis, I.; Willimsky, G.; et al. Tumor-infiltrating Merkel cell polyomavirus-specific T cells are diverse and associated with improved patient survival. Cancer Immunol. Res. 2017, 5, 137–147. [Google Scholar] [CrossRef] [Green Version]
- Harms, P.W.; Patel, R.M.; Verhaegen, M.E.; Giordano, T.J.; Nash, K.T.; Johnson, C.N.; Daignault, S.; Thomas, D.G.; Gudjonsson, J.E.; Elder, J.T.; et al. Distinct gene expression profiles of viral- and nonviral-associated Merkel cell carcinoma revealed by transcriptome analysis. J. Investig. Dermatol. 2013, 133, 936–945. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- R Development Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2019; ISBN 3-900051-07-0. Available online: http://www.R-project.org/ (accessed on 29 October 2019).






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PD-L1 n = 132 | CD8 n = 132 | FoxP3 n = 132 | IDO1 n = 130 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| High | Low | p-Value | High | Low | p-Value | High | Low | p-Value | High | Low | p-Value | |
| Age | ||||||||||||
| >77 years | 27 | 38 | 0.48 | 32 | 32 | 0.65 | 29 | 36 | 0.86 | 33 | 30 | 0.65 |
| <=77 years | 37 | 30 | 29 | 39 | 31 | 36 | 30 | 37 | ||||
| Gender | ||||||||||||
| Male | 37 | 36 | 0.72 | 31 | 42 | 0.72 | 29 | 44 | 0.64 | 34 | 39 | 0.72 |
| Female | 27 | 32 | 30 | 29 | 31 | 28 | 29 | 28 | ||||
| Site | ||||||||||||
| Head and neck | 32 | 30 | 0.73 | 30 | 32 | 0.73 | 33 | 31 | 0.56 | 27 | 35 | 0.56 |
| Other sites | 32 | 38 | 31 | 39 | 27 | 41 | 36 | 32 | ||||
| Size | ||||||||||||
| >20 mm | 36 | 23 | 0.07 | 27 | 32 | 1 | 26 | 34 | 1 | 32 | 27 | 0.48 |
| <=20 mm | 28 | 45 | 34 | 39 | 33 | 39 | 31 | 40 | ||||
| Thickness | ||||||||||||
| >10 mm | 39 | 23 | 0.019 * | 30 | 34 | 1 | 26 | 37 | 0.64 | 34 | 29 | 0.58 |
| <=10 mm | 25 | 43 | 30 | 36 | 32 | 35 | 28 | 37 | ||||
| Ulceration | ||||||||||||
| Present | 20 | 24 | 0.71 | 13 | 31 | 0.037 * | 15 | 29 | 0.14 | 24 | 20 | 0.48 |
| Absent | 44 | 44 | 48 | 40 | 45 | 43 | 39 | 47 | ||||
| Mitoses | ||||||||||||
| >40/mm2 | 31 | 33 | 1 | 25 | 40 | 0.32 | 25 | 40 | 0.32 | 30 | 34 | 1 |
| <=40/mm2 | 33 | 34 | 35 | 31 | 34 | 32 | 32 | 33 | ||||
| Growth pattern | ||||||||||||
| Nodular | 34 | 26 | 0.44 | 26 | 34 | 0.73 | 31 | 29 | 0.44 | 28 | 32 | 0.73 |
| Nodular and infiltrative, infiltrative | 30 | 42 | 35 | 37 | 29 | 43 | 35 | 35 | ||||
| Necrosis | ||||||||||||
| Present | 22 | 21 | 0.71 | 17 | 27 | 0.48 | 17 | 26 | 0.48 | 25 | 18 | 0.48 |
| Absent | 42 | 47 | 44 | 44 | 43 | 46 | 38 | 49 | ||||
| Lymphovascular invasion | ||||||||||||
| Present | 33 | 31 | 0.60 | 28 | 36 | 0.60 | 25 | 39 | 0.34 | 36 | 26 | 0.21 |
| Absent | 31 | 37 | 33 | 35 | 35 | 33 | 27 | 41 | ||||
| Perineural invasion | ||||||||||||
| Present | 6 | 6 | 1 | 4 | 8 | 1 | 4 | 8 | 1 | 6 | 6 | 1 |
| Absent | 58 | 62 | 57 | 63 | 56 | 64 | 57 | 61 | ||||
| MCPyV | ||||||||||||
| Present | 48 | 37 | 0.036 * | 46 | 39 | 0.036 * | 42 | 43 | 0.27 | 45 | 38 | 0.15 |
| Absent | 16 | 31 | 15 | 32 | 18 | 29 | 18 | 29 | ||||
| Overall Survival | Merkel Cell Carcinoma-Specific Survival | Progression-Free Survival | |||||
|---|---|---|---|---|---|---|---|
| N | Hazard Ratio | p-Value | Hazard Ratio | p-Value | Hazard Ratio | p-Value | |
| PD-L1 >1% | 132 | 0.55 | 0.016 * | 0.41 | 0.019 * | 0.56 | 0.043 * |
| CD8-high | 132 | 0.76 | 0.25 | 0.45 | 0.036 * | 0.62 | 0.098 |
| FoxP3-high | 132 | 0.66 | 0.092 | 0.62 | 0.17 | 0.57 | 0.047 * |
| IDO1-high | 130 | 0.93 | 0.75 | 1.15 | 0.69 | 1.29 | 0.36 |
| CD8-high FoxP3-high | 132 | 0.66 | 0.13 | 0.41 | 0.046 * | 0.58 | 0.091 |
| PD-L1 >1% FoxP3-high | 132 | 0.43 | 0.0072 * | 0.28 | 0.017 * | 0.35 | 0.004 * |
| PD-L1 >1% CD8-high | 132 | 0.57 | 0.053 | 0.28 | 0.018 * | 0.45 | 0.024 * |
| PD-L1 >1% IDO1-high | 130 | 0.50 | 0.057 | 0.87 | 0.74 | 1.14 | 0.66 |
| Size (>20 mm) | 132 | 1.03 | 0.91 | 1.31 | 0.44 | 1.20 | 0.50 |
| Thickness (>10 mm) | 132 | 1.04 | 0.89 | 1.14 | 0.71 | 1.06 | 0.84 |
| Growth pattern (nodular versus infiltrative/mixed) | 132 | 0.69 | 0.12 | 0.58 | 0.12 | 0.57 | 0.051 |
| Ulceration | 132 | 2.01 | 0.0046 * | 2.51 | 0.008 * | 1.67 | 0.067 |
| Mitoses (>40/mm2) | 132 | 0.97 | 0.89 | 1.28 | 0.47 | 1.17 | 0.58 |
| Necrosis | 132 | 1.30 | 0.32 | 1.19 | 0.66 | 1.45 | 0.19 |
| Lymphovascular invasion | 132 | 1.50 | 0.095 | 2.29 | 0.02 * | 1.51 | 0.14 |
| MCPyV large T-antigen | 132 | 0.52 | 0.0076 * | 0.49 | 0.04 * | 0.71 | 0.22 |
| Age (>versus ≤77 years) | 132 | 2.35 | 0.00067 * | 1.33 | 0.41 | 0.9 | 0.7 |
| Gender (male versus female) | 132 | 1.29 | 0.28 | 2.23 | 0.029 * | 2.29 | 0.006 * |
| Site (other versus head & neck) | 132 | 1.32 | 0.26 | 0.76 | 0.44 | 0.48 | 0.012 * |
| Stage (3–4 versus 1–2) | 132 | 1.27 | 0.62 | 2.75 | 0.038 * | 27.2 | <0.0001 * |
| Immunosuppression | 132 | 1.18 | 0.63 | 1.2 | 0.71 | 1.02 | 0.97 |
| Treatment (adjuvant therapy versus surgery | 132 | 1.13 | 0.63 | 1.82 | 0.094 | 1.52 | 0.13 |
| Overall Survival | Merkel Cell Carcinoma-Specific Survival | Progression-Free Survival | |||||
|---|---|---|---|---|---|---|---|
| N | Hazard Ratio | p-Value | Hazard Ratio | p-Value | Hazard Ratio | p-Value | |
| PD-L1 >1% | 132 | 0.92 | 0.78 | 0.84 | 0.76 | 1.48 | 0.37 |
| Ulceration | 132 | 1.79 | 0.03 * | 1.73 | 0.18 | - | - |
| MCPyV T-antigen expression | 132 | 0.73 | 0.24 | 0.72 | 0.41 | - | - |
| PD-L1 >1% FoxP3-high | 132 | 0.54 | 0.13 | 0.99 | 0.99 | 0.32 | 0.058 |
| PD-L1 >1% CD8-high | 132 | - | - | 0.27 | 0.15 | 0.70 | 0.48 |
| CD8-high FoxP3-high | 132 | - | - | 0.44 | 0.26 | - | - |
| Lymphovascular invasion | 132 | - | - | 1.94 | 0.1 | - | - |
| CD8 | 132 | - | - | 2.4 | 0.24 | - | - |
| FoxP3 | 132 | - | - | - | - | 1.35 | 0.41 |
| Age | 132 | 2.13 | 0.0031 * | - | - | - | - |
| Gender | 132 | - | - | 1.78 | 0.19 | 2.08 | 0.018 * |
| Site (other versus head & neck) | 132 | - | - | - | - | 0.56 | 0.064 |
| Stage (3–4 versus 1–2) | 132 | - | - | 2.37 | 0.12 | 20.57 | <0.0001 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Donizy, P.; Wu, C.-L.; Kopczynski, J.; Pieniazek, M.; Biecek, P.; Ryś, J.; Hoang, M.P. Prognostic Role of Tumoral PD-L1 and IDO1 Expression, and Intratumoral CD8+ and FoxP3+ Lymphocyte Infiltrates in 132 Primary Cutaneous Merkel Cell Carcinomas. Int. J. Mol. Sci. 2021, 22, 5489. https://doi.org/10.3390/ijms22115489
Donizy P, Wu C-L, Kopczynski J, Pieniazek M, Biecek P, Ryś J, Hoang MP. Prognostic Role of Tumoral PD-L1 and IDO1 Expression, and Intratumoral CD8+ and FoxP3+ Lymphocyte Infiltrates in 132 Primary Cutaneous Merkel Cell Carcinomas. International Journal of Molecular Sciences. 2021; 22(11):5489. https://doi.org/10.3390/ijms22115489
Chicago/Turabian StyleDonizy, Piotr, Cheng-Lin Wu, Janusz Kopczynski, Malgorzata Pieniazek, Przemyslaw Biecek, Janusz Ryś, and Mai P. Hoang. 2021. "Prognostic Role of Tumoral PD-L1 and IDO1 Expression, and Intratumoral CD8+ and FoxP3+ Lymphocyte Infiltrates in 132 Primary Cutaneous Merkel Cell Carcinomas" International Journal of Molecular Sciences 22, no. 11: 5489. https://doi.org/10.3390/ijms22115489