Melatonin and Sirtuins in Buccal Epithelium: Potential Biomarkers of Aging and Age-Related Pathologies

 , , , and
, , , and
Abstract
:1. Introduction
2. Results
2.1. Expression of SIRT1, SIRT3, and SIRT6 mRNA in BE of Subjects of Different Ages with and without AH
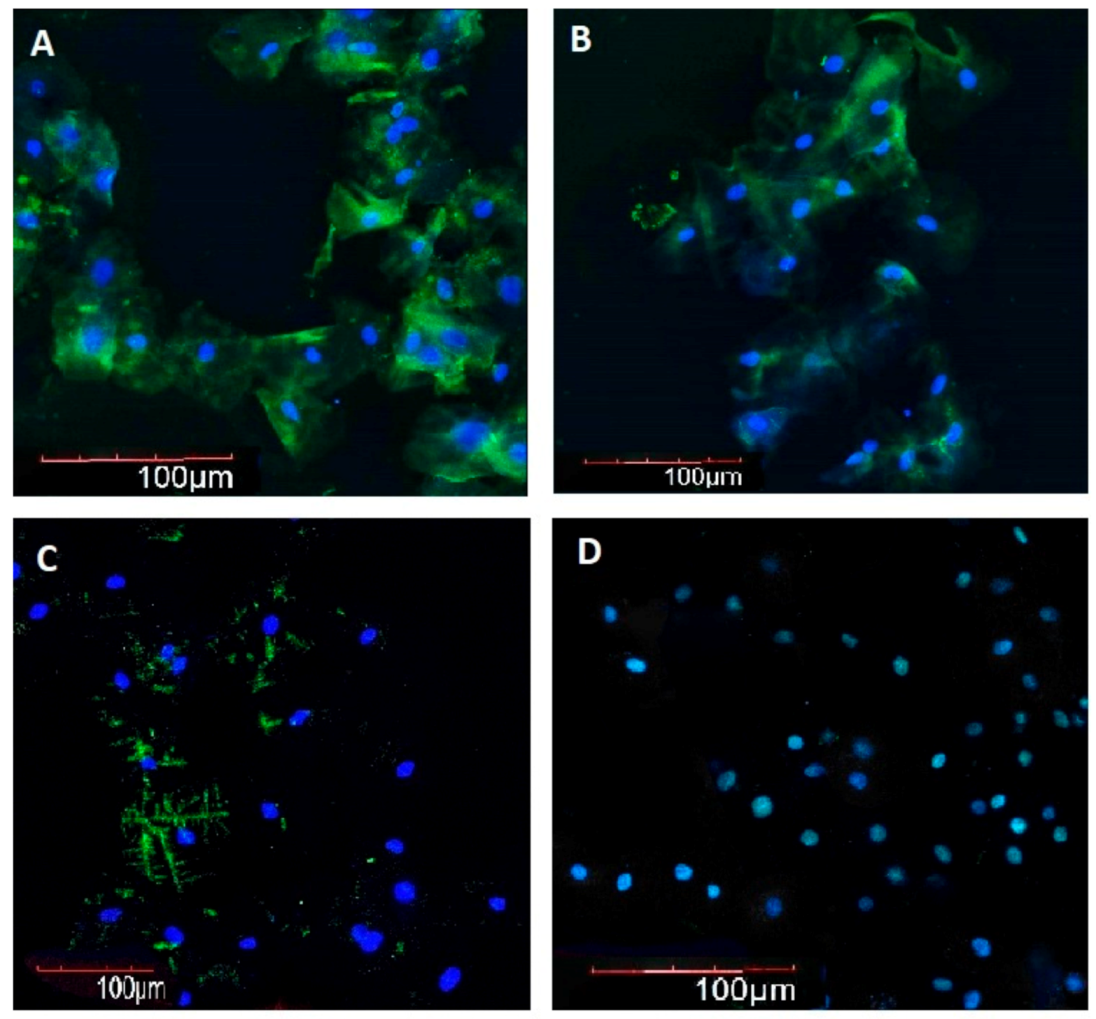
2.2. Melatonin, SIRT1, SIRT3, and SIRT6 Immunofluorescence Intensity in BE in Subjects of Different Ages with and without AH
3. Discussion
- ∙
- BE sampling is a non-invasive procedure, yielding highly informative material for evaluating the expression of genes and proteins as well as the synthesis of molecules.
- ∙
- No data are so far available on the role of BE sampling to assess the expression of the geroprotective molecules MT and SIRTs as biomarkers of aging and age-related diseases.
- ∙
- Gauging the expression of MT and SIRTs in BE of subjects of different ages with and without AH using RT-PCR, immunocytochemistry, and immunofluorescence microscopy yields reliable results.
- ∙
- It can be proposed that MT and SIRTs levels evaluation in BE samples might provide valuable markers of the aging process and age-related pathologies.
4. Materials and Methods
4.1. Buccal Epithelium Samples Collection
4.2. Real-Time Polymerase Chain Reaction (RT-PCR)
4.3. Immunofluorescence Analysis by Confocal Microscopy
4.4. Statistical Analysis
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Raikhlin, N.T.; Kvetnoy, I.M. Melatonin and enterochromaffine cells. Acta Histochem. 1976, 1, 19–24. [Google Scholar] [CrossRef]
- Kvetnoy, I.M. Extrapineal melatonin: Location and role within diffuse neuroendocrine system. Histochem. J. 1999, 1, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Kvetnoy, I. Extrapineal melatonin in pathology: New perspectives for diagnosis, prognosis and treatment of illness. Neuroendocrinol. Lett. 2002, 1, 92–96. [Google Scholar]
- Reiter, R.J.; Ma, Q.; Sharma, R. Melatonin in Mitochondria: Mitigating Clear and Present Dangers. Physiology 2020, 2, 86–95. [Google Scholar] [CrossRef] [PubMed]
- Polyakova, V.O.; Kvetnoy, I.M.; Anderson, G.; Rosati, J.; Mazzoccoli, G.; Linkova, N.S. Reciprocal Interactions of Mitochondria and the Neuroimmunoendocrine System in Neurodegenerative Disorders: An Important Role for Melatonin Regulation. Front. Physiol. 2018, 9, 1–13. [Google Scholar] [CrossRef]
- Paltsev, M.A.; Polyakova, V.O.; Kvetnoy, I.M.; Anderson, G.; Kvetnaia, T.V.; Linkova, N.S.; Paltseva, E.M.; Rubino, R.; De Cosmo, S.; De Cata, A.; et al. Morphofunctional and signaling molecules overlap of pineal gland and thymus: Role and significance in aging. Oncotarget 2016, 7, 11972–11983. [Google Scholar] [CrossRef]
- Petrova, A.; Kondratiuk, V.; Karpenko, O.; Ostashevska, T.; Krasiuk, E. The effectiveness of melatonin in the complex treatment of hypertension in patients with stage 5 chronic kidney disease. Georgian Med. News 2020, 299, 87–93. [Google Scholar]
- Baltatu, O.C.; Amaral, F.G.; Campos, L.A.; Cipolla-Neto, J. Melatonin, mitochondria and hypertension. Cell. Mol. Life Sci. 2017, 21, 3955–3964. [Google Scholar] [CrossRef]
- Hardeland, R. Aging, Melatonin, and the Pro- and Anti-Inflammatory Networks. Int. J. Mol. Sci. 2019, 5, 1223. [Google Scholar] [CrossRef] [Green Version]
- Kaeberlein, M.; McVey, M.; Guarente, L. The SIR2/3/4 complex and SIR2 alone promote longevity in Saccharomyces cerevisiae by two different mechanisms. Genes Dev. 1999, 13, 2570–2580. [Google Scholar] [CrossRef] [Green Version]
- Chen, B.; Zang, W.; Wang, J.; Huangm, Y.; He, Y.; Yan, L.; Liu, J.; Zheng, W. The chemical biology of Sirtuins. Chem. Soc. Rev. 2015, 44, 5246–5264. [Google Scholar] [CrossRef] [PubMed]
- Singh, C.K.; Chhabra, G.; Ndiaye, M.A.; Garcia-Peterson, L.M.; Mack, N.J.; Ahmad, N. The Role of Sirtuins in Antioxidant and Redox Signaling. Antioxid. Redox Signal. 2018, 8, 643–661. [Google Scholar] [CrossRef]
- Xu, S.; Bai, P.; Jin, Z.G. Sirtuins in Cardiovascular Health and Diseases. Trends Endocrinol. Metab. 2016, 10, 677–678. [Google Scholar] [CrossRef] [PubMed]
- Yuan, Y.; Cruzat, V.F.; Newsholme, P.; Cheng, J.; Chen, Y.; Lu, Y. Regulation of SIRT1 in aging: Roles in mitochondrial function and biogenesis. Mech. Ageing Dev. 2016, 155, 10–21. [Google Scholar] [CrossRef] [PubMed]
- D’Onofrio, N.; Servillo, L.; Balestrieri, M.L. SIRT1 and SIRT6 Signaling Pathways in Cardiovascular Disease Protection. Antioxid. Redox Signal. 2018, 8, 711–732. [Google Scholar] [CrossRef] [PubMed]
- Kida, Y.; Goligorsky, M.S. Sirtuins, Cell Senescence, and Vascular Aging. Can. J. Cardiol. 2016, 5, 634–641. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, S.; Yin, M.; Koroleva, M.; Mastrangelo, M.A.; Zhang, W.; Bai, P.; Little, P.J.; Jin, Z.G. SIRT6 protects against endothelial dysfunction and atherosclerosis in mice. Aging 2016, 5, 1064–1082. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McDonnell, E.; Peterson, B.S.; Bomze, H.M.; Hirschey, M.D. SIRT3 regulates progression and development of diseases of aging. Trends Endocrinol. Metab. 2015, 9, 486–492. [Google Scholar] [CrossRef] [Green Version]
- Miller, F.J., Jr. Hypertension and Mitochondrial Oxidative Stress Revisited: Sirtuin 3, the Improved “Antioxidant”. Circ. Res. 2020, 4, 453–455. [Google Scholar] [CrossRef]
- Guo, J.; Wang, Z.; Wu, J.; Liu, M.; Li, M.; Sun, Y.; Huang, W.; Li, Y.; Zhang, Y.; Tang, W.; et al. Endothelial SIRT6 Is Vital to Prevent Hypertension and Associated Cardiorenal Injury Through Targeting Nkx3.2-GATA5 Signaling. Circ. Res. 2019, 10, 1448–1461. [Google Scholar] [CrossRef]
- Nanzadsuren, T.; Myatav, T.; Dorjkhuu, A.; Byamba, K. Association between serum melatonin and skin aging in an urban population of Mongolia. J. Cosmet. Dermatol. 2020, 19, 1501–1507. [Google Scholar] [CrossRef] [PubMed]
- Zuev, V.A.; Trifonov, N.I.; Linkova, N.S.; Kvetnaia, T.V. Melatonin as a molecular marker of age-related pathologies. Adv. Gerontol. 2017, 1, 62–69. [Google Scholar]
- Lee, F.Y.; Sun, C.K.; Sung, P.H.; Chen, K.H.; Chua, S.; Sheu, J.J.; Chung, S.Y.; Chai, H.T.; Chen, Y.L.; Huang, T.H.; et al. Daily melatonin protects the endothelial lineage and functional integrity against the aging process, oxidative stress, and toxic environment and restores blood flow in critical limb ischemia area in mice. J. Pineal Res. 2018, 2, 1–20. [Google Scholar] [CrossRef]
- Anisimov, V.N.; Popovich, I.G.; Zabezhinski, M.A.; Anisimov, S.V.; Vesnushkin, G.M.; Vinogradova, I.A. Melatonin as antioxidant, geroprotector and anticarcinogen. Biochim. Biophys. Acta 2006, 1757, 573–589. [Google Scholar] [CrossRef] [Green Version]
- Gu, H.; Shen, Q.; Mei, D.; Yang, Y.; Wei, R.; Ni, M. Melatonin Inhibits TE-1 Esophageal Cancer Cells Metastasis by Suppressing the NF-κB Signaling Pathway and Decreasing MMP-9. Ann. Clin. Lab. Sci. 2020, 1, 65–72. [Google Scholar]
- Kozina, L.S.; Arutjunyan, A.V.; Khavinson, V.K. Antioxidant properties of geroprotective peptides of the pineal gland. Arch. Gerontol. Geriatr. 2007, 44, 213–216. [Google Scholar] [CrossRef]
- Ebersole, J.L.; Orraca, L.; Novak, M.J.; Kirakodu, S.; Gonzalez-Martinez, J.; Gonzalez, O.A. Comparative Analysis of Gene Expression Patterns for Oral Epithelium-Related Functions with Aging. Adv. Exp. Med. Biol. 2019, 1197, 143–163. [Google Scholar]
- Zuev, V.A.; Dyatlova, A.S.; Lin’kova, N.S.; Kvetnaya, T.V. Expression of Aβ42, τ-Protein, p16, p53 in Buccal Epithelium: Prospects for Use in the Diagnostics of Alzheimer’s Disease and Rate of Aging. Bull. Exp. Biol. Med. 2019, 5, 676–679. [Google Scholar] [CrossRef]
- Elias, W.Y. Age-Dependent Differential Expression of Apoptotic Markers in Rat Oral Mucosa. Asian Pac. J. Cancer Prev. 2018, 11, 3245–3250. [Google Scholar] [CrossRef] [Green Version]
- López-Cuervo, J.E.; Beltran, E.M.; Castillo, A.A.; Sanchez, T.N. Preliminary study of a new, fully automated system for liquid-based cytology: The NovaPrep® processor system. Acta Cytol. 2011, 55, 281–286. [Google Scholar] [CrossRef]
- Barber, R.D.; Harmer, D.W.; Coleman, R.A.; Clark, B.J. GAPDH as a housekeeping gene: Analysis of GAPDH mRNA expression in a panel of 72 human tissues. Physiol. Genom. 2005, 21, 389–395. [Google Scholar] [CrossRef] [Green Version]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age Group | SIRT1 | SIRT3 | SIRT6 | |||
|---|---|---|---|---|---|---|
| Control | AH | Control | AH | Control | AH | |
| 25–59 years old | 1.12 ± 0.24 | 0.67 ± 0.11 * | 1.55 ± 0.27 | 0.50 ± 0.07 * | 2.04 ± 0.30 | 0.90 ± 0.11 * |
| 60–89 years old | 0.90 ± 0.20 | 0.50 ± 0.10 * | 0.81 ± 0.19 ** | 0.63 ± 0.10 * | 1.01 ± 0.17 ** | 0.31 ± 0.06 *,† |
| ≥90 years old | 0.87 ± 0.18 | 0.52 ± 0.12 * | 0.86 ± 0.20 ** | 0.65 ± 0.11 * | 0.96 ± 0.15 ** | 0.35 ± 0.07 *,† |
| Group | Age (Years) | Gender (n) (% of Female Subjects) | Height (cm) | Weight (kg) | Systolic Blood Pressure (mmHg) | Diastolic Blood Pressure (mmHg) |
|---|---|---|---|---|---|---|
| Subjects without arterial hypertension (n = 50) (50%) | ||||||
| 25–59 years old | 43.6 ± 5.5 | 10 males, 11 females (52.3% females) | 178.7 ± 5.5 | 83.4 ± 13.3 | 110.1 ± 5.3 | 76.0 ± 2.2 |
| 60–89 years old | 70.9 ± 7.3 | 10 males, 8 females (44.4% females) | 172.2 ± 5.1 | 86.5 ± 10.1 | 107.2 ± 2.6 | 78.1 ± 2.5 |
| ≥90 years old | 89.9 ± 1.2 | 2 males, 9 females (81.8% females) | 174.0 ± 6.5 | 87.1 ± 10.4 | 113.4 ± 4.6 | 74.2 ± 3.6 |
| Subjects with arterial hypertension (n = 50) (50%) | ||||||
| 25–59 years old | 47.0 ± 6.1 | 8 males, 13 females (61.9% females) | 176.3 ± 9.06 | 89.6 ± 7.8 | 142.3 ± 3.1 * | 89.4 ± 4.0 * |
| 60–89 years old | 66.4 ± 4.1 | 6 males, 12 females (66.7% females) | 170.1 ± 5.3 | 94.1 ± 3.7 | 150.0 ± 3.04 * | 92.0 ± 3.8 * |
| ≥90 years old | 95.1 ± 1.76 | 3 males, 8 females (72.7% females) | 172.09 ± 7.9 | 95.2 ± 5.1 | 163.0 ± 2.5 * | 96.0 ± 2.02 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carbone, A.; Linkova, N.; Polyakova, V.; Mironova, E.; Hashimova, U.; Gadzhiev, A.; Safikhanova, K.; Kvetnaia, T.; Krylova, J.; Tarquini, R.; et al. Melatonin and Sirtuins in Buccal Epithelium: Potential Biomarkers of Aging and Age-Related Pathologies. Int. J. Mol. Sci. 2020, 21, 8134. https://doi.org/10.3390/ijms21218134
Carbone A, Linkova N, Polyakova V, Mironova E, Hashimova U, Gadzhiev A, Safikhanova K, Kvetnaia T, Krylova J, Tarquini R, et al. Melatonin and Sirtuins in Buccal Epithelium: Potential Biomarkers of Aging and Age-Related Pathologies. International Journal of Molecular Sciences. 2020; 21(21):8134. https://doi.org/10.3390/ijms21218134
Chicago/Turabian StyleCarbone, Annalucia, Natalia Linkova, Victoria Polyakova, Ekaterina Mironova, Ulduz Hashimova, Ahmed Gadzhiev, Khatira Safikhanova, Tatiana Kvetnaia, Julia Krylova, Roberto Tarquini, and et al. 2020. "Melatonin and Sirtuins in Buccal Epithelium: Potential Biomarkers of Aging and Age-Related Pathologies" International Journal of Molecular Sciences 21, no. 21: 8134. https://doi.org/10.3390/ijms21218134