Eicosanoid Profiles in the Vitreous Humor of Patients with Proliferative Diabetic Retinopathy

 , , ,
, , ,
Abstract
:1. Introduction
2. Results
3. Discussion
4. Materials and Methods
4.1. Inclusion Criteria
4.2. Exclusion Criteria
4.3. Sample Collection
4.4. LC/MS Eicosanoid Assay
4.5. Data Analysis
4.6. Statistics
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Mohamed, Q.; Gillies, M.C.; Wong, T.Y. Management of diabetic retinopathy: A systematic review. JAMA 2007, 298, 902–916. [Google Scholar] [CrossRef] [Green Version]
- Javitt, J.C.; Aiello, L.P.; Chiang, Y.; Ferris, F.L.; Canner, J.K.; Greenfield, S. Preventive eye care in people with diabetes is cost-saving to the federal government. Implications for health-care reform. Diabetes Care 1994, 17, 909–917. [Google Scholar] [CrossRef]
- Klein, R.; Klein, B.E.; Moss, S.E.; Cruickshanks, K.J. The Wisconsin epidemiologic study of diabetic retinopathy. XV. The long-term incidence of macular edema. Ophthalmology 1995, 102, 7–16. [Google Scholar] [CrossRef]
- Fundus Photographic Risk Factors for Progression of Diabetic Retinopathy: ETDRS Report Number 12. Ophthalmology 1991, 98, 823–833. [CrossRef]
- Kempen, J.H.; O’Colmain, B.J.; Leske, M.C.; Haffner, S.M.; Klein, R.; Moss, S.E.; Taylor, H.R.; Hamman, R.F. The prevalence of diabetic retinopathy among adults in the United States. Arch. Ophthalmol. 1960 2004, 122, 552–563. [Google Scholar] [CrossRef] [Green Version]
- Giuliari, G.P. Diabetic retinopathy: Current and new treatment options. Curr. Diabetes Rev. 2012, 8, 32–41. [Google Scholar] [CrossRef] [PubMed]
- Stefánsson, E. The therapeutic effects of retinal laser treatment and vitrectomy. A theory based on oxygen and vascular physiology. Acta Ophthalmol. Scand. 2001, 79, 435–440. [Google Scholar] [CrossRef] [PubMed]
- Michels, R. Basic and Advanced Vitreous Surgery; Springer: New York, NY, USA, 1986. [Google Scholar]
- Iyer, S.R.; Regan, K.A.; Burnham, J.M.; Chen Ching, J. Surgical management of diabetic tractional retinal detachments. Surv. Ophthalmol. 2019, 64, 780–809. [Google Scholar] [CrossRef] [PubMed]
- Schwartzman, M.L.; Iserovich, P.; Gotlinger, K.; Bellner, L.; Dunn, M.W.; Sartore, M.; Grazia, P.M.; Leonardi, A.; Sathe, S.; Beaton, A.; et al. Profile of lipid and protein autacoids in diabetic vitreous correlates with the progression of diabetic retinopathy. Diabetes 2010, 59, 1780–1788. [Google Scholar] [CrossRef] [Green Version]
- Othman, A.; Ahmad, S.; Megyerdi, S.; Mussell, R.; Choksi, K.; Maddipati, K.R.; Elmarakby, A.; Rizk, N.; Al-Shabrawey, M. 12/15-Lipoxygenase-derived lipid metabolites induce retinal endothelial cell barrier dysfunction: Contribution of NADPH oxidase. PLoS ONE 2013, 8, e57254. [Google Scholar] [CrossRef] [Green Version]
- Diabetic Retinopathy Clinical Research Network; Elman, M.J.; Aiello, L.P.; Beck, R.W.; Bressler, N.M.; Bressler, S.B.; Edwards, A.R.; Ferris, F.L.; Friedman, S.M.; Glassman, A.R.; et al. Randomized trial evaluating ranibizumab plus prompt or deferred laser or triamcinolone plus prompt laser for diabetic macular edema. Ophthalmology 2010, 117, 1064–1077.e35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frank, R.N. On the pathogenesis of diabetic retinopathy. A 1990 update. Ophthalmology 1991, 98, 586–593. [Google Scholar] [CrossRef]
- Van Geest, R.J.; Klaassen, I.; Lesnik-Oberstein, S.Y.; Tan, H.S.; Mura, M.; Goldschmeding, R.; Van Noorden, C.J.; Schlingemann, R.O. Vitreous TIMP-1 levels associate with neovascularization and TGF-β2 levels but not with fibrosis in the clinical course of proliferative diabetic retinopathy. J. Cell Commun. Signal. 2013, 7, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Aiello, L.P.; Avery, R.L.; Arrigg, P.G.; Keyt, B.A.; Jampel, H.D.; Shah, S.T.; Pasquale, L.R.; Thieme, H.; Iwamoto, M.A.; Park, J.E.; et al. Vascular endothelial growth factor in ocular fluid of patients with diabetic retinopathy and other retinal disorders. N. Engl. J. Med. 1994, 331, 1480–1487. [Google Scholar] [CrossRef] [PubMed]
- Adamis, A.P.; Miller, J.W.; Bernal, M.T.; D’Amico, D.J.; Folkman, J.; Yeo, T.K.; Yeo, K.T. Increased vascular endothelial growth factor levels in the vitreous of eyes with proliferative diabetic retinopathy. Am. J. Ophthalmol. 1994, 118, 445–450. [Google Scholar] [CrossRef]
- Al-Shabrawey, M.; Mussell, R.; Kahook, K.; Tawfik, A.; Eladl, M.; Sarthy, V.; Nussbaum, J.; El-Marakby, A.; Park, S.Y.; Gurel, Z.; et al. Increased expression and activity of 12-lipoxygenase in oxygen-induced ischemic retinopathy and proliferative diabetic retinopathy: Implications in retinal neovascularization. Diabetes 2011, 60, 614–624. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stuart, M.J.; Walenga, R.W.; Setty, B.N.; Phelps, D.L. Effects of changes in oxygen tension on lipoxygenase metabolites. Serum 15-HETE is increased in kittens exposed to hyperoxia. Biol. Neonate. 1990, 57, 313–317. [Google Scholar] [CrossRef] [PubMed]
- Bajpai, A.K.; Blaskova, E.; Pakala, S.B.; Zhao, T.; Glasgow, W.C.; Penn, J.S.; Johnson, D.A.; Rao, G.N. 15(S)-HETE production in human retinal microvascular endothelial cells by hypoxia: Novel role for MEK1 in 15(S)-HETE induced angiogenesis. Invest. Ophthalmol. Vis. Sci. 2007, 48, 4930–4938. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bajpai, A.K.; Blaskova, E.; Pakala, S.B.; Zhao, T.; Glasgow, W.C.; Penn, J.S.; Johnson, D.A.; Rao, G.N. Key role of 15-LO/15-HETE in angiogenesis and functional recovery in later stages of post-stroke mice. Sci. Rep. 2017, 7, 46698. [Google Scholar] [CrossRef] [Green Version]
- Soumya, S.J.; Binu, S.; Helen, A.; Anil Kumar, K.; Reddanna, P.; Sudhakaran, P.R. Effect of 15-lipoxygenase metabolites on angiogenesis: 15(S)-HPETE is angiostatic and 15(S)-HETE is angiogenic. Inflamm Res. 2012, 61, 707–718. [Google Scholar] [CrossRef]
- Chen, L.; Zhu, Y.-M.; Li, Y.-N.; Li, P.-Y.; Wang, D.; Liu, Y.; Qu, Y.-Y.; Zhu, D.-L.; Zhu, Y.-L. The 15-LO-1/15-HETE system promotes angiogenesis by upregulating VEGF in ischemic brains. Neurol. Res. 2017, 39, 795–802. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Joseph, G.; Zhang, F.F.; Nguyen, H.; Jiang, H.; Gotlinger, K.H.; Falck, J.R.; Yang, J.; Schwartzman, M.L.; Guo, A.M. 20-HETE contributes to ischemia-induced angiogenesis. Vascul. Pharmacol. 2016, 83, 57–65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, L.; Ackerman, R.; Saleh, M.; Gotlinger, K.H.; Kessler, M.; Mendelowitz, L.G.; Falck, J.R.; Arbab, A.S.; Scicli, A.G.; Schwartzman, M.L.; et al. 20-HETE regulates the angiogenic functions of human endothelial progenitor cells and contributes to angiogenesis in vivo. J. Pharm. Exp. Ther. 2014, 348, 442–451. [Google Scholar] [CrossRef] [PubMed]
- Fan, F.; Sun, C.W.; Maier, K.G.; Williams, J.M.; Pabbidi, M.R.; Didion, S.P.; Falck, J.R.; Zhuo, J.; Roman, R.J. 20-Hydroxyeicosatetraenoic acid contributes to the inhibition of K+ channel activity and vasoconstrictor response to angiotensin II in rat renal microvessels. PLoS ONE 2013, 8, e82482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amaral, S.L.; Maier, K.G.; Schippers, D.N.; Roman, R.J.; Greene, A.S. CYP4A metabolites of arachidonic acid and VEGF are mediators of skeletal muscle angiogenesis. Am. J. Physiol. Heart Circ. Physiol. 2003, 284, H1528–H1535. [Google Scholar] [CrossRef] [PubMed]
- Fang, X.; Faraci, F.M.; Kaduce, T.L.; Harmon, S.; Modrick, M.L.; Hu, S.; Moore, S.A.; Falck, J.R.; Weintraub, N.L.; Spector, A.A. 20-Hydroxyeicosatetraenoic acid is a potent dilator of mouse basilar artery: Role of cyclooxygenase. Am. J. Physiol. Heart Circ. Physiol. 2006, 291, H2301–H2307. [Google Scholar] [CrossRef] [Green Version]
- Fang, X.; Faraci, F.M.; Kaduce, T.L.; Harmon, S.; Modrick, M.L.; Hu, S.; Moore, S.A.; Falck, J.R.; Weintraub, N.L.; Spector, A.A. 20-hydroxyeicosatetraenoic acid (20-HETE) metabolism in coronary endothelial cells. J. Biol. Chem. 2004, 279, 2648–2656. [Google Scholar] [CrossRef] [Green Version]
- Ma, C.; Li, Y.; Ma, J.; Liu, Y.; Li, Q.; Niu, S.; Shen, Z.; Zhang, L.; Pan, Z.; Zhu, D. Key role of 15-lipoxygenase/15-hydroxyeicosatetraenoic acid in pulmonary vascular remodeling and vascular angiogenesis associated with hypoxic pulmonary hypertension. Hypertension Dallas. Tex. 1979 2011, 58, 679–688. [Google Scholar] [CrossRef] [Green Version]
- Ma, C.; Wang, Y.; Shen, T.; Zhang, C.; Ma, J.; Zhang, L.; Liu, F.; Zhu, D. Placenta growth factor mediates angiogenesis in hypoxic pulmonary hypertension. Prostaglandins Leukot. Essent. Fat. Acids 2013, 89, 159–168. [Google Scholar] [CrossRef]
- Augustin, A.J.; Grus, F.H.; Koch, F.; Spitznas, M. Detection of eicosanoids in epiretinal membranes of patients suffering from proliferative vitreoretinal diseases. Br. J. Ophthalmol. 1997, 81, 58–60. [Google Scholar] [CrossRef] [Green Version]
- Ibrahim, A.S.; Elshafey, S.; Sellak, H.; Hussein, K.A.; El-Sherbiny, M.; Abdelsaid, M.; Rizk, N.; Beasley, S.; Tawfik, A.M.; Smith, S.B.; et al. A lipidomic screen of hyperglycemia-treated HRECs links 12/15-Lipoxygenase to microvascular dysfunction during diabetic retinopathy via NADPH oxidase. J. Lipid Res. 2015, 56, 599–611. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Antonipillai, I.; Nadler, J.; Vu, E.J.; Bughi, S.; Natarajan, R.; Horton, R. A 12-lipoxygenase product, 12-hydroxyeicosatetraenoic acid, is increased in diabetics with incipient and early renal disease. J. Clin. Endocrinol. Metab. 1996, 81, 1940–1945. [Google Scholar] [CrossRef] [Green Version]
- Martidis, A.; Duker, J.S.; Greenberg, P.B.; Rogers, A.H.; Puliafito, C.A.; Reichel, E.; Baumal, C. Intravitreal triamcinolone for refractory diabetic macular edema. Ophthalmology 2002, 109, 920–927. [Google Scholar] [CrossRef]
- Guo, A.M.; Arbab, A.S.; Falck, J.R.; Chen, P.; Edwards, P.A.; Roman, R.J.; Scicli, A.G. Activation of vascular endothelial growth factor through reactive oxygen species mediates 20-hydroxyeicosatetraenoic acid-induced endothelial cell proliferation. J. Pharm. Exp. Ther. 2007, 321, 18–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gubitosi-Klug, R.A.; Talahalli, R.; Du, Y.; Nadler, J.L.; Kern, T.S. 5-lipoxygenase, but not 12/15-lipoxygenase, contributes to degeneration of retinal capillaries in a mouse model of diabetic retinopathy. Diabetes 2008, 57, 1387–1393. [Google Scholar] [CrossRef] [Green Version]
- Talahalli, R.; Zarini, S.; Sheibani, N.; Murphy, R.C.; Gubitosi-Klug, R.A. Increased synthesis of leukotrienes in the mouse model of diabetic retinopathy. Investig. Ophthalmol. Vis. Sci. 2010, 51, 1699–1708. [Google Scholar] [CrossRef]
- Orozco, L.D.; Liu, H.; Perkins, E.; Johnson, D.A.; Chen, B.B.; Fan, F.; Baker, R.C.; Roman, R.J. 20-Hydroxyeicosatetraenoic acid inhibition attenuates balloon injury-induced neointima formation and vascular remodeling in rat carotid arteries. J. Pharm. Exp. Ther. 2013, 346, 67–74. [Google Scholar] [CrossRef] [Green Version]
- Arevalo, J.F.; Lasave, A.F.; Kozak, I.; Al Rashaed, S.; Al Kahtani, E.; Maia, M.; Farah, M.E.; Cutolo, C.; Brito, M.; Osorio, C.; et al. Preoperative bevacizumab for tractional retinal detachment in proliferative diabetic retinopathy: A prospective randomized clinical trial. Am. J. Ophthalmol. 2019, 207, 279–287. [Google Scholar] [CrossRef]
- Dreisbach, A.W.; Smith, S.V.; Kyle, P.B.; Ramaiah, M.; Amenuke, M.; Garrett, M.R.; Lirette, S.T.; Griswold, M.E.; Roman, R.J. Urinary CYP eicosanoid excretion correlates with glomerular filtration in African-Americans with chronic kidney disease. Prostaglandins Other Lipid Mediat. 2014, 113, 45–51. [Google Scholar] [CrossRef] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Metabolite | PDR ± SEM (31) | Control ± SEM (13) | p-Value |
|---|---|---|---|
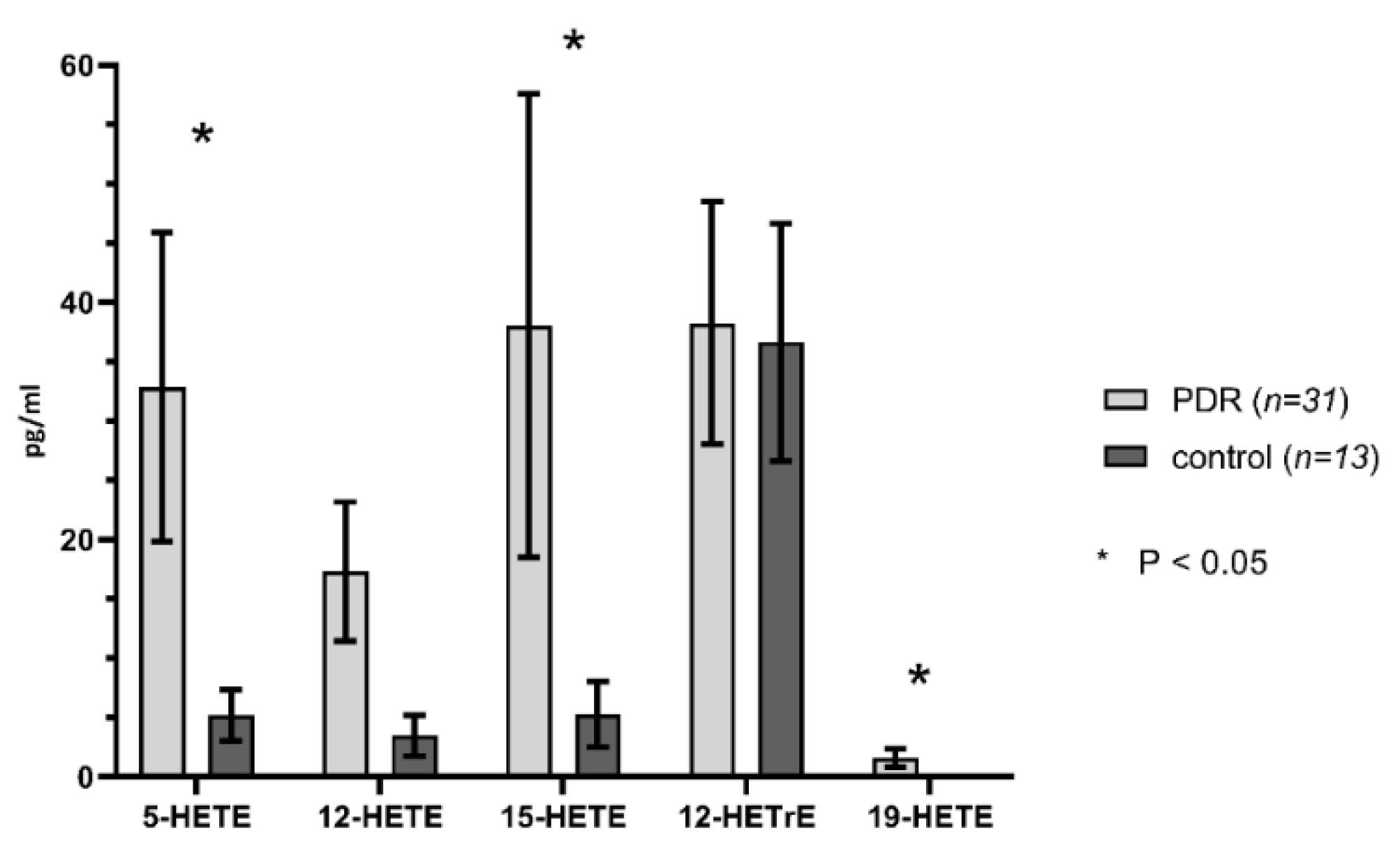
| 5-HETE | 32.85 ± 13.04 | 5.185 ± 2.155 | 0.0444 |
| 12-HETE | 17.32 ± 5.869 | 3.462 ±1.698 | 0.0297 |
| 15-HETE | 38.042 ± 19.526 | 5.269 ± 2.763 | 0.1066 |
| 19-HETE | 1.594 ± 0.7731 | 0 | 0.048 |
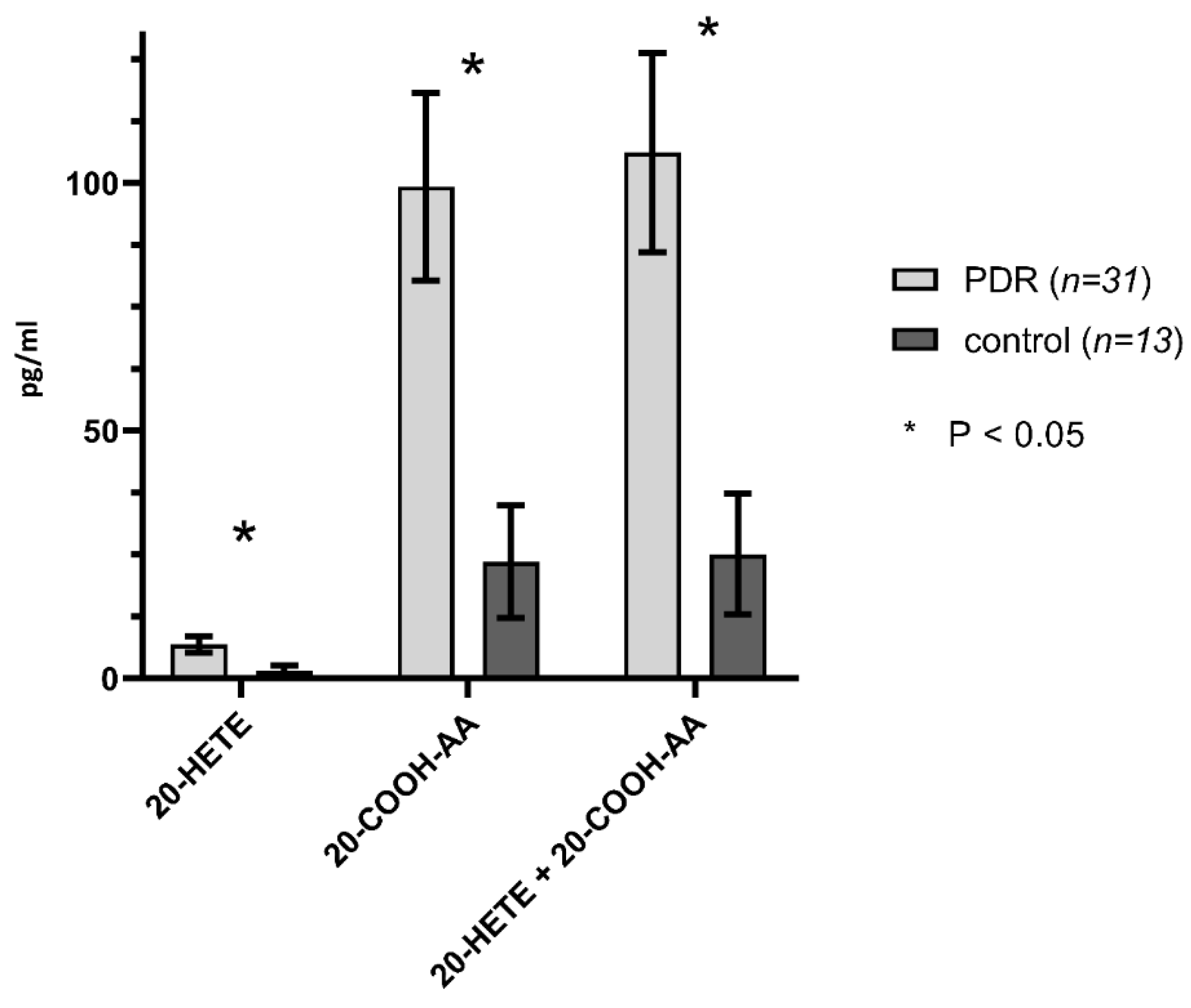
| 20-HETE | 6.884 ± 1.671 | 1.538 ±1.042 | 0.0096 |
| 20-COOH-AA | 99.28 ± 18.919 | 23.56 ±11.302 | 0.0013 |
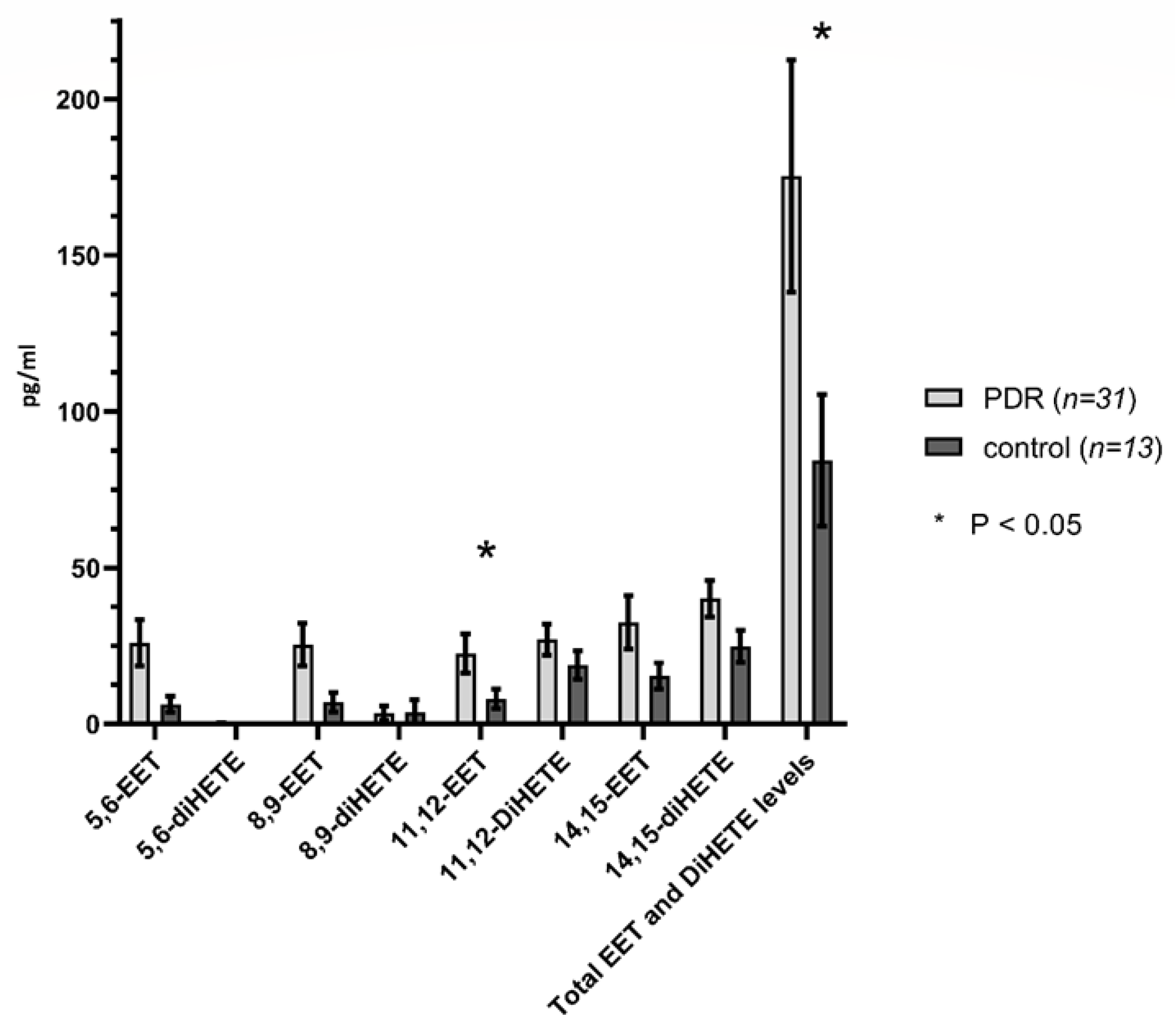
| 11,12-EET | 22.684 ± 6.234 | 8.052 ± 3.070 | 0.0367 |
| 14,15-EET | 32.629 ± 8.507 | 15.408 ± 4.142 | 0.0544 |
| 11,12-DiHETE | 27.037 ± 4.876 | 18.892 ± 4.515 | 0.2283 |
| 14,15-DiHETE | 40.13 ± 5.950 | 24.831 ± 5.150 | 0.0594 |
| 12-HETrE | 38.26 ± 10.23 | 36.646 ±10.018 | 0.9108 |
| Total ꞷ-hydroxylase level | 106.2 ± 20.118 | 25.1 ±12.183 | 0.0013 |
| Total epoxygenase level | 175.403 ± 37.245 | 84.354 ±21.101 | 0.0394 |
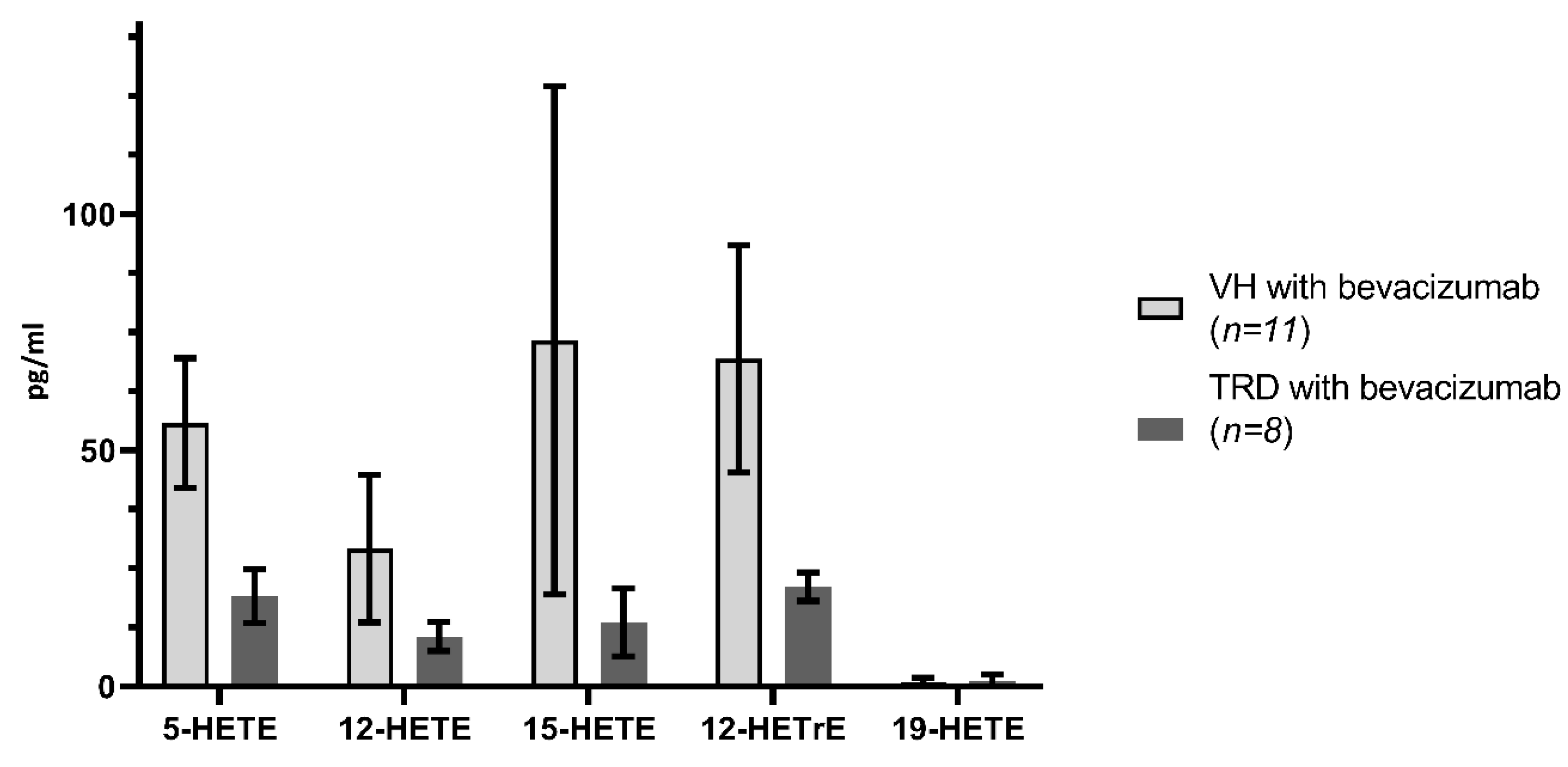
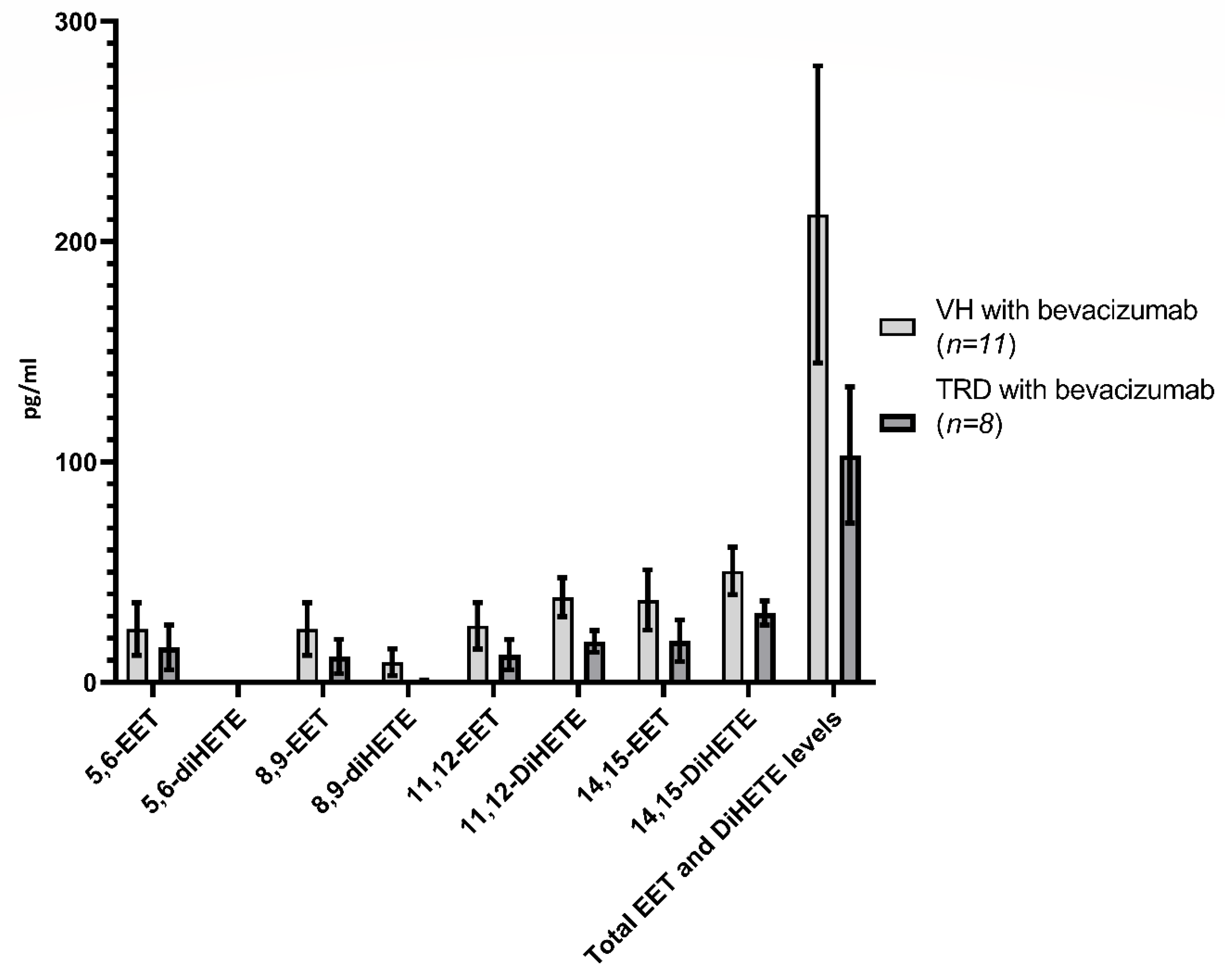
| Metabolite | VH ± SEM (11) | TRD ± SEM (8) | p-Value |
|---|---|---|---|
| 5-HETE | 55.772 ± 36.114 | 19.088 ± 5.708 | 0.3383 |
| 12-HETE | 29.164 ± 15.587 | 10.575 ± 3.046 | 0.2671 |
| 15-HETE | 73.273 +/− 53.75 | 13.575 ± 7.183 | 0.2959 |
| 20-HETE | 7.927 ± 2.169 | 10.213 ± 4.280 | 0.6436 |
| 20-COOH-AA | 119.518 ± 34.719 | 87.338 ± 41.407 | 0.5603 |
| Total ꞷ-hydroxylase level | 127.446 ± 36.211 | 97.550 ± 44.996 | 0.6124 |
| 12-HETrE | 69.355 ± 24.072 | 21.713 ± 10.290 | 0.0913 |
| 11,12-EET | 25.645 ± 10.543 | 12.563 ± 6.829 | 0.313 |
| 14,15-EET | 37.381 ± 13.720 | 18.838 ± 9.437 | 0.2815 |
| 11,12-DiHETE | 38.691 ± 8.852 | 18.829 ± 5.510 | 0.0658 |
| 14,15-DiHETE | 50.582 ± 10.828 | 31.414 ± 5.510 | 0.1366 |
| Total epoxygenase level | 212.363 ± 67.437 | 103.200 ± 30.979 | 0.1638 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, A.L.; Roman, R.J.; Regan, K.A.; Bolch, C.A.; Chen, C.-J.; Iyer, S.S.R. Eicosanoid Profiles in the Vitreous Humor of Patients with Proliferative Diabetic Retinopathy. Int. J. Mol. Sci. 2020, 21, 7451. https://doi.org/10.3390/ijms21207451
Lin AL, Roman RJ, Regan KA, Bolch CA, Chen C-J, Iyer SSR. Eicosanoid Profiles in the Vitreous Humor of Patients with Proliferative Diabetic Retinopathy. International Journal of Molecular Sciences. 2020; 21(20):7451. https://doi.org/10.3390/ijms21207451
Chicago/Turabian StyleLin, Albert L, Richard J Roman, Kathleen A Regan, Charlotte A Bolch, Ching-Jygh Chen, and Siva S.R. Iyer. 2020. "Eicosanoid Profiles in the Vitreous Humor of Patients with Proliferative Diabetic Retinopathy" International Journal of Molecular Sciences 21, no. 20: 7451. https://doi.org/10.3390/ijms21207451