NECTIN4 Expression in Extramammary Paget’s Disease: Implication of a New Therapeutic Target


Abstract
:1. Introduction
2. Results
2.1. Characteristics of the Study Cohort
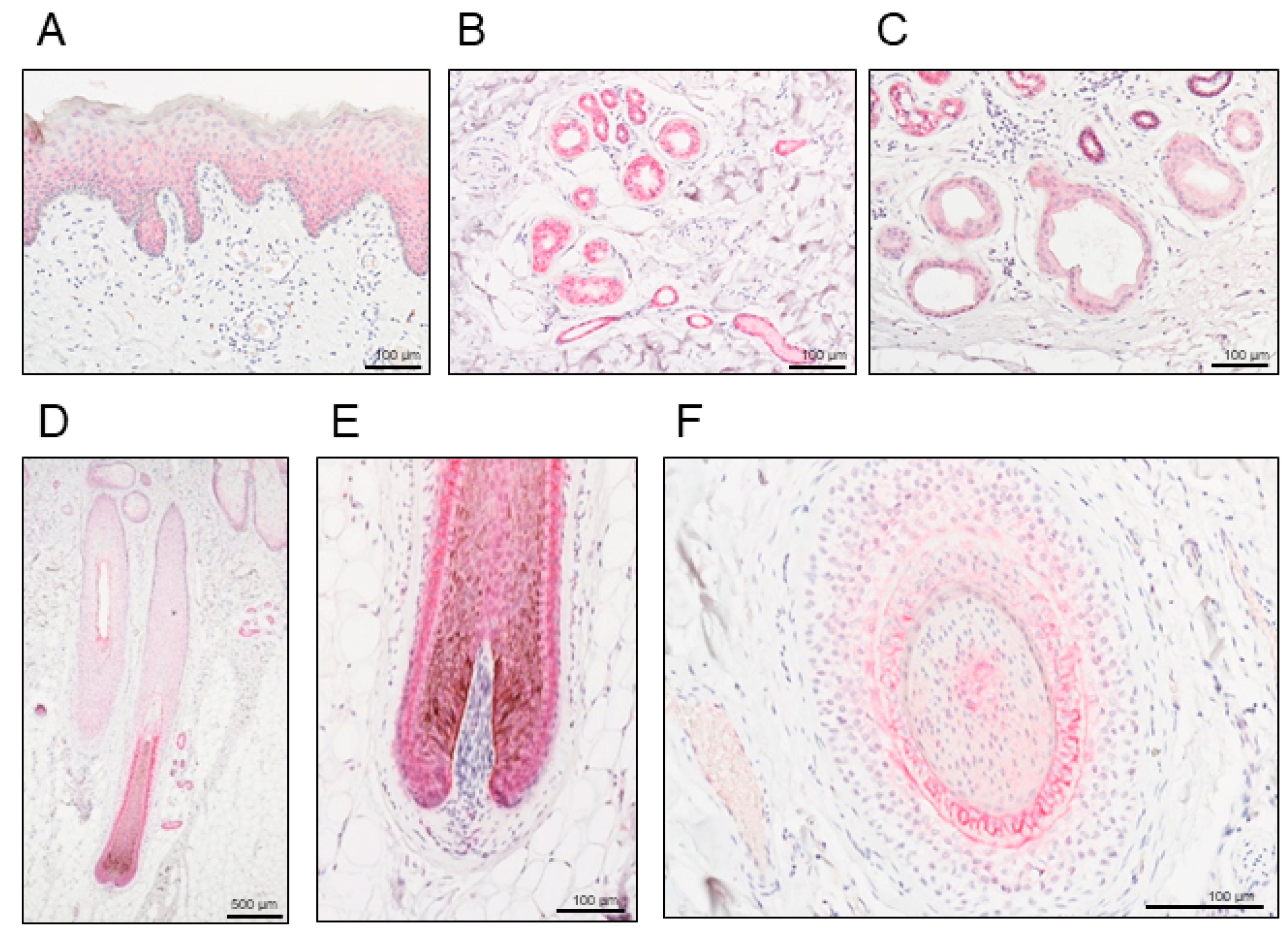
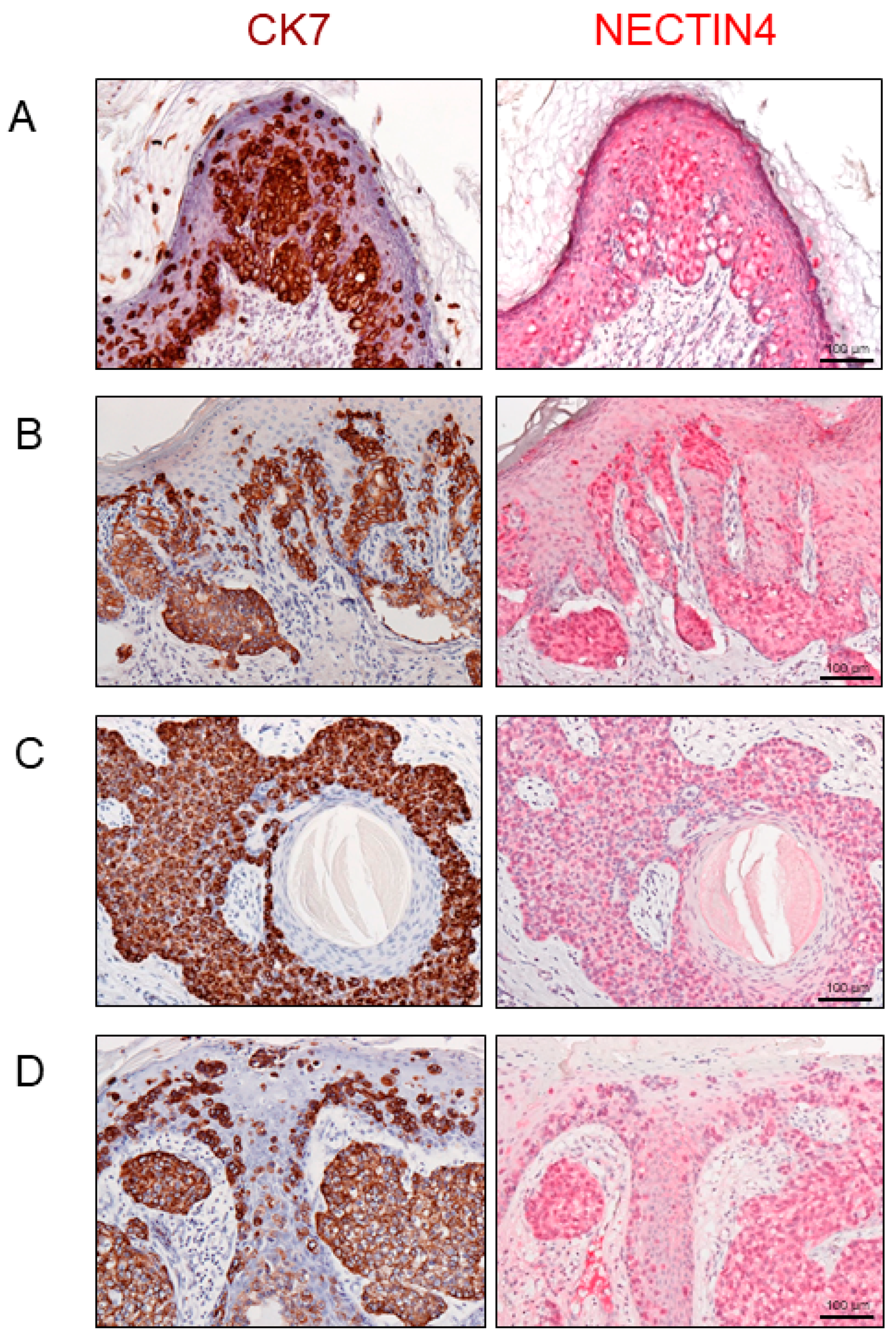
2.2. NECTIN4 Expression in Normal Skin and Extramammary Paget’s Disease (EMPD)
2.3. Association between NECTIN4 and Clinicopathological Factors in EMPD
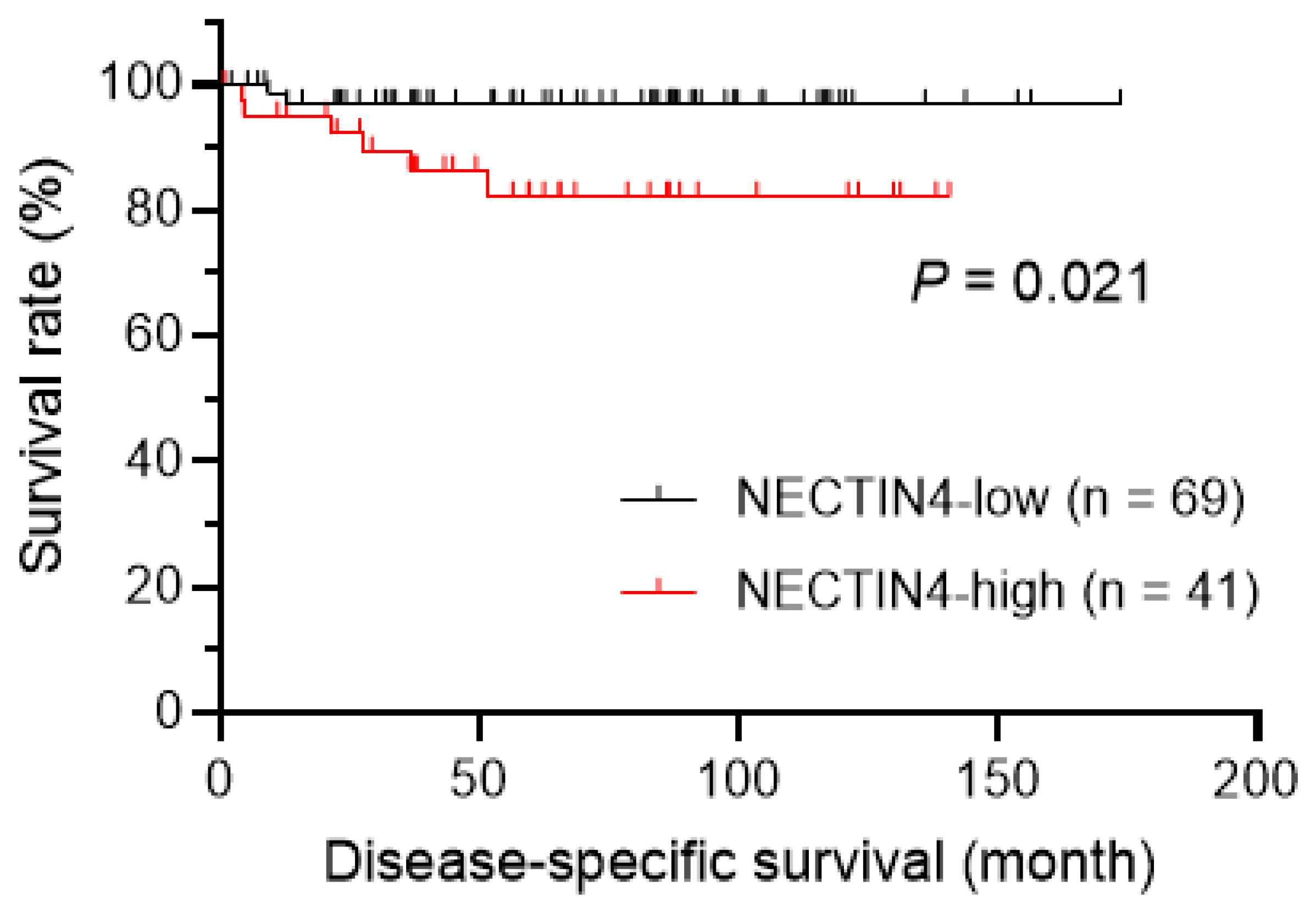
2.4. Prognostic Impact of NECTIN4 Expression
3. Discussion
4. Materials and Methods
4.1. Patients
4.2. Immunohistochemistry
4.3. Evaluation of NECTIN4 Immunohistochemical Staining
4.4. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| EMPD | extramammary Paget’s disease |
| NECTIN4 | nectin cell adhesion molecule 4 |
| CK7 | cytokeratin 7 |
| DSS | disease-specific survival |
| TT | tumor thickness |
| 95% CI | 95% confidence interval |
References
- Kanitakis, J. Mammary and extramammary Paget’s disease. J. Eur. Acad. Dermatol. Venereol. 2007, 21, 581–590. [Google Scholar] [CrossRef]
- Shepherd, V.; Davidson, E.J.; Davies-Humphreys, J. Extramammary Paget’s disease. BJOG 2005, 112, 273–279. [Google Scholar] [CrossRef]
- Simonds, R.M.; Segal, R.J.; Sharma, A. Extramammary Paget’s disease: A review of the literature. Int. J. Dermatol. 2019, 58, 871–879. [Google Scholar] [CrossRef]
- Ito, T.; Kaku-Ito, Y.; Furue, M. The diagnosis and management of extramammary Paget’s disease. Expert Rev. Anticancer Ther. 2018, 18, 543–553. [Google Scholar] [CrossRef]
- Funaro, D.; Krasny, M.; Lam, C.; Desy, D.; Sauthier, P.; Bouffard, D. Extramammary Paget disease: Epidemiology and association to cancer in a Quebec-based population. J. Low. Genit. Tract Dis. 2013, 17, 167–174. [Google Scholar] [CrossRef]
- Nasioudis, D.; Bhadra, M.; Ko, E.M. Extramammary Paget disease of the vulva: Management and prognosis. Gynecol. Oncol. 2019, 157, 146–150. [Google Scholar] [CrossRef] [PubMed]
- Ohara, K.; Fujisawa, Y.; Yoshino, K.; Kiyohara, Y.; Kadono, T.; Murata, Y.; Uhara, H.; Hatta, N.; Uchi, H.; Matsushita, S.; et al. A proposal for a TNM staging system for extramammary Paget disease: Retrospective analysis of 301 patients with invasive primary tumors. J. Dermatol. Sci. 2016, 83, 234–239. [Google Scholar] [CrossRef] [PubMed]
- Murata, Y.; Kumano, K. Extramammary Paget’s disease of the genitalia with clinically clear margins can be adequately resected with 1 cm margin. Eur. J. Dermatol. 2005, 15, 168–170. [Google Scholar] [PubMed]
- Hatta, N.; Yamada, M.; Hirano, T.; Fujimoto, A.; Morita, R. Extramammary Paget’s disease: Treatment, prognostic factors and outcome in 76 patients. Br. J. Dermatol. 2008, 158, 313–318. [Google Scholar] [CrossRef] [PubMed]
- Hendi, A.; Brodland, D.G.; Zitelli, J.A. Extramammary Paget’s disease: Surgical treatment with Mohs micrographic surgery. J. Am. Acad. Dermatol. 2004, 51, 767–773. [Google Scholar] [CrossRef] [PubMed]
- Kaku-Ito, Y.; Ito, T.; Tsuji, G.; Nakahara, T.; Hagihara, A.; Furue, M.; Uchi, H. Evaluation of mapping biopsies for extramammary Paget disease: A retrospective study. J. Am. Acad Dermatol. 2018, 78, 1171–1177. [Google Scholar] [CrossRef] [PubMed]
- Kato, J.; Hida, T.; Yamashita, T.; Kamiya, S.; Horimoto, K.; Sato, S.; Takahashi, H.; Sawada, M.; Yamada, M.; Uhara, H. Successful TS-1 monotherapy as the second-line treatment for advanced extramammary Paget’s disease: A report of two cases. J. Dermatol. 2018, 45, 80–82. [Google Scholar] [CrossRef] [PubMed]
- Fukuda, K.; Funakoshi, T. Metastatic extramammary Paget’s disease: Pathogenesis and novel therapeutic approach. Front. Oncol. 2018, 8, 38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mauzo, S.H.; Tetzlaff, M.T.; Milton, D.R.; Siroy, A.E.; Nagarajan, P.; Torres-Cabala, C.A.; Ivan, D.; Curry, J.L.; Hudgens, C.W.; Wargo, J.A.; et al. Expression of PD-1 and PD-L1 in Extramammary Paget Disease: Implications for Immune-Targeted Therapy. Cancers 2019, 11, 754. [Google Scholar] [CrossRef] [Green Version]
- Rosenberg, J.E.; O’Donnell, P.H.; Balar, A.V.; McGregor, B.A.; Heath, E.I.; Yu, E.Y.; Galsky, M.D.; Hahn, N.M.; Gartner, E.M.; Pinelli, J.M.; et al. Pivotal Trial of Enfortumab Vedotin in Urothelial Carcinoma after Platinum and Anti-Programmed Death 1/Programmed Death Ligand 1 Therapy. J. Clin. Oncol. 2019, 37, 2592–2600. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, S.; Uemura, M.; Kimura, T.; Kawasaki, Y.; Takamoto, A.; Yamaguchi, A.; Melhem-Bertrandt, A.; Gartner, E.M.; Inoue, T.; Akazawa, R.; et al. A phase I study of enfortumab vedotin in Japanese patients with locally advanced or metastatic urothelial carcinoma. Invest. New Drugs 2019. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Zhang, J.; Shen, Q.; Yin, W.; Huang, H.; Liu, Y.; Ni, Q. High expression of Nectin-4 is associated with unfavorable prognosis in gastric cancer. Oncol. Lett. 2018, 15, 8789–8795. [Google Scholar] [CrossRef]
- Hao, R.T.; Zheng, C.; Wu, C.Y.; Xia, E.J.; Zhou, X.F.; Quan, R.D.; Zhang, X.H. NECTIN4 promotes papillary thyroid cancer cell proliferation, migration, and invasion and triggers EMT by activating AKT. Cancer Manag. Res. 2019, 11, 2565–2578. [Google Scholar] [CrossRef] [Green Version]
- Zeindler, J.; Soysal, S.D.; Piscuoglio, S.; Ng, C.K.Y.; Mechera, R.; Isaak, A.; Weber, W.P.; Muenst, S.; Kurzeder, C. Nectin-4 expression is an independent prognostic biomarker and associated with better survival in triple-negative breast cancer. Front. Med. 2019, 6, 200. [Google Scholar] [CrossRef] [Green Version]
- Deng, H.; Shi, H.; Chen, L.; Zhou, Y.; Jiang, J. Over-expression of Nectin-4 promotes progression of esophageal cancer and correlates with poor prognosis of the patients. Cancer Cell Int. 2019, 19, 106. [Google Scholar] [CrossRef] [Green Version]
- Bekos, C.; Muqaku, B.; Dekan, S.; Horvat, R.; Polterauer, S.; Gerner, C.; Aust, S.; Pils, D. NECTIN4 (PVRL4) as putative therapeutic target for a specific subtype of high grade serous ovarian cancer-an integrative multi-omics approach. Cancers 2019, 11, 698. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Challita-Eid, P.M.; Satpayev, D.; Yang, P.; An, Z.; Morrison, K.; Shostak, Y.; Raitano, A.; Nadell, R.; Liu, W.; Lortie, D.R.; et al. Enfortumab vedotin antibody-drug conjugate targeting Nectin-4 is a highly potent therapeutic agent in multiple preclinical cancer models. Cancer Res. 2016, 76, 3003–3013. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pavlova, N.N.; Pallasch, C.; Elia, A.E.; Braun, C.J.; Westbrook, T.F.; Hemann, M.; Elledge, S.J. A role for PVRL4-driven cell-cell interactions in tumorigenesis. Elife 2013, 2, e00358. [Google Scholar] [CrossRef] [PubMed]
- Noyce, R.S.; Bondre, D.G.; Ha, M.N.; Lin, L.T.; Sisson, G.; Tsao, M.S.; Richardson, C.D. Tumor cell marker PVRL4 (nectin 4) is an epithelial cell receptor for measles virus. PLoS Pathog. 2011, 7, e1002240. [Google Scholar] [CrossRef]
- Mühlebach, M.D.; Mateo, M.; Sinn, P.L.; Prüfer, S.; Uhlig, K.M.; Leonard, V.H.; Navaratnarajah, C.K.; Frenzke, M.; Wong, X.X.; Sawatsky, B.; et al. Adherens junction protein nectin-4 is the epithelial receptor for measles virus. Nature 2011, 480, 530–533. [Google Scholar] [CrossRef] [Green Version]
- Kedashiro, S.; Sugiura, A.; Mizutani, K.; Takai, Y. Nectin-4 cis-interacts with ErbB2 and its trastuzumab-resistant splice variants, enhancing their activation and DNA synthesis. Sci. Rep. 2019, 9, 1–15. [Google Scholar] [CrossRef] [Green Version]
- McClelland, R.A.; Finlay, P.; Walker, K.J.; Nicholson, D.; Robertson, J.F.; Blamey, R.W.; Nicholson, R.I. Automated quantitation of immunocytochemically localized estrogen receptors in human breast cancer. Cancer Res. 1990, 50, 3545–3550. [Google Scholar]
- Ito, T.; Kaku, Y.; Nagae, K.; Nakano-Nakamura, M.; Nakahara, T.; Oda, Y.; Hagihara, A.; Furue, M.; Uchi, H. Tumor thickness as a prognostic factor in extramammary Paget’s disease. J. Dermatol. 2015, 42, 269–275. [Google Scholar] [CrossRef]
- M-Rabet, M.; Cabaud, O.; Josselin, E.; Finetti, P.; Castellano, R.; Farina, A.; Agavnian-Couquiaud, E.; Saviane, G.; Collette, Y.; Viens, P.; et al. Nectin-4: A new prognostic biomarker for efficient therapeutic targeting of primary and metastatic triple-negative breast cancer. Ann. Oncol. 2017, 28, 769–776. [Google Scholar] [CrossRef]
- Rosenberg, J.; Sridhar, S.S.; Zhang, J.; Smith, D.; Ruether, D.; Flaig, T.W.; Baranda, J.; Lang, J.; Plimack, E.R.; Sangha, R.; et al. EV-101: A phase I study of single-agent enfortumab vedotin in patients with Nectin-4-positive solid tumors, including metastatic urothelial carcinoma. J. Clin. Oncol. 2020, 38, 1041–1049. [Google Scholar] [CrossRef]
- Burki, T.K. Enfortumab vedotin shows promise in solid tumours. Lancet Oncol. 2020, 21, e133. [Google Scholar] [CrossRef]
- Murata, M.; Ito, T.; Tanaka, Y.; Yamamura, K.; Furue, K.; Furue, M. OVOL2-mediated ZEB1 downregulation may prevent promotion of actinic keratosis to cutaneous squamous cell carcinoma. J. Clin. Med. 2020, 9, 618. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ito, T.; Kaku-Ito, Y.; Murata, M.; Ichiki, T.; Kuma, Y.; Tanaka, Y.; Ide, T.; Ohno, F.; Wada-Ohno, M.; Yamada, Y.; et al. Intra- and inter-tumor BRAF heterogeneity in acral melanoma: An immunohistochemical analysis. Int. J. Mol. Sci. 2019, 20, 6191. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Parameters | |
|---|---|
| Age, years | |
| Average | 73.7 |
| Median | 73.0 |
| Range | 47–91 |
| Sex | |
| Male | 69 (62.7%) |
| Female | 41 (37.3%) |
| Tumor site | |
| Anogenital area | 104 (94.5%) |
| Others | 6 (5.5%) |
| TNM stage | |
| I–II | 94 (85.5%) |
| III–IV | 16 (14.5%) |
| Tumor thickness (TT) | |
| TT ≤ 1 mm | 76 (69.1%) |
| 1 < TT ≤ 2 mm | 10 (9.1%) |
| 2 < TT ≤ 4 mm | 5 (4.5%) |
| TT > 4 mm | 7 (6.4%) |
| Unknown | 12 (10.9%) |
| NECTIN4 Expression | |||
|---|---|---|---|
| Parameters | Low | High | p-Value |
| Age (years) | |||
| <70 | 19 (17.3%) | 17 (15.5%) | 0.15 |
| ≥70 | 50 (45.5%) | 24 (21.8%) | |
| Sex | |||
| Male | 37 (33.6%) | 32 (29.1%) | 0.014 |
| Female | 32 (29.1%) | 9 (8.2%) | |
| Tumor site | |||
| Anogenital area | 63 (57.3%) | 41 (37.3%) | 0.082 |
| Others | 6 (5.5%) | 0 (0%) | |
| TNM stage | |||
| I–II | 62 (56.4%) | 29 (26.4%) | 0.017 |
| III–IV | 7 (6.4%) | 12 (10.9%) | |
| Tumor thickness | |||
| ≤1 mm | 57 (51.8%) | 19 (17.3%) | 0.017 |
| >1 mm | 10 (9.1%) | 12 (10.9%) | |
| Unknown | 2 (1.8%) | 10 (9.1%) | |
| Total | 69 (62.7%) | 41 (37.3%) | |
| Variable | Hazard Ratio | 95% CI | p-Value |
|---|---|---|---|
| Age, years | 0.80 | 0.58–0.96 | 0.061 |
| Sex, male | 0.47 | 0.075–2.94 | 0.42 |
| TNM stage, III or IV | 3.01 × 1012 | 0 | 0.99 |
| TT, >1 mm | 7.02 | 0.24–200.58 | 0.25 |
| NECTIN4 expression, high | 0.07 | 0.0018–2.39 | 0.14 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Murata, M.; Ito, T.; Tanaka, Y.; Kaku-Ito, Y.; Furue, M. NECTIN4 Expression in Extramammary Paget’s Disease: Implication of a New Therapeutic Target. Int. J. Mol. Sci. 2020, 21, 5891. https://doi.org/10.3390/ijms21165891
Murata M, Ito T, Tanaka Y, Kaku-Ito Y, Furue M. NECTIN4 Expression in Extramammary Paget’s Disease: Implication of a New Therapeutic Target. International Journal of Molecular Sciences. 2020; 21(16):5891. https://doi.org/10.3390/ijms21165891
Chicago/Turabian StyleMurata, Maho, Takamichi Ito, Yuka Tanaka, Yumiko Kaku-Ito, and Masutaka Furue. 2020. "NECTIN4 Expression in Extramammary Paget’s Disease: Implication of a New Therapeutic Target" International Journal of Molecular Sciences 21, no. 16: 5891. https://doi.org/10.3390/ijms21165891