A Chronic Ocular-Hypertensive Rat Model induced by Injection of the Sclerosant Agent Polidocanol in the Aqueous Humor Outflow Pathway

 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Animal Handling and Ethics Statement
2.2. Experimental Design
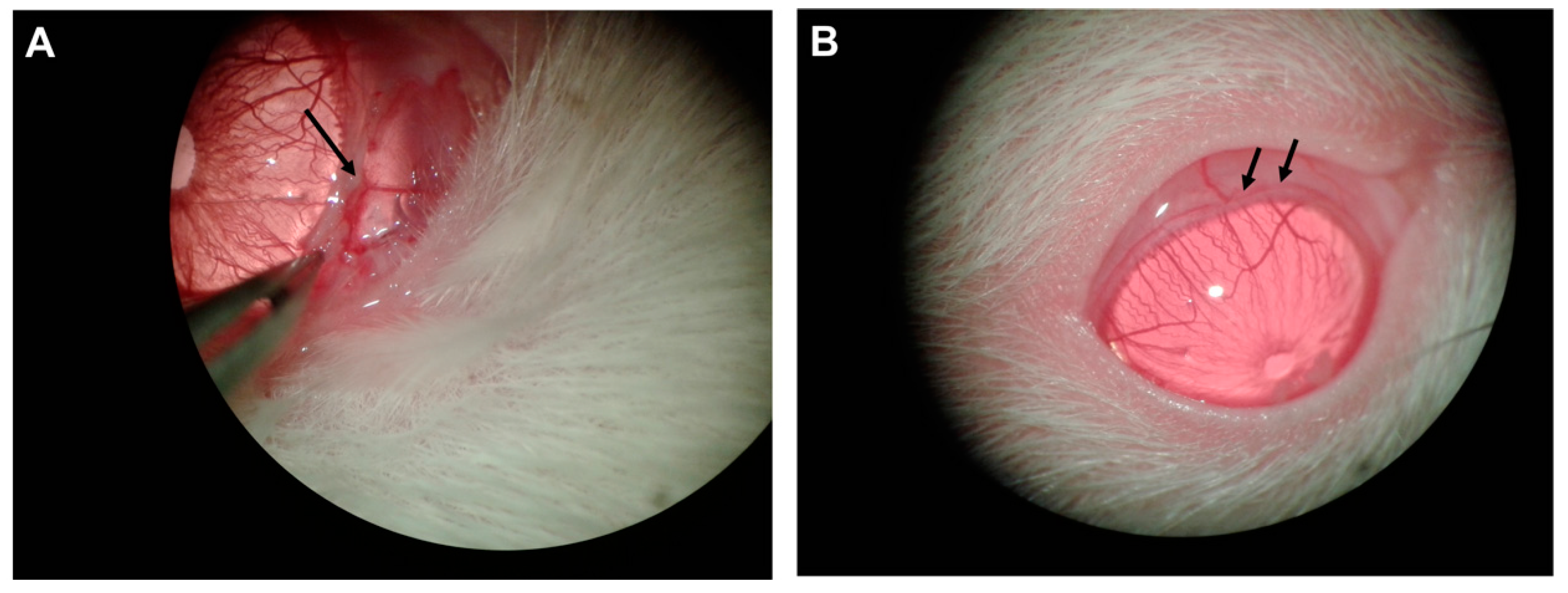
2.3. Surgical Technique
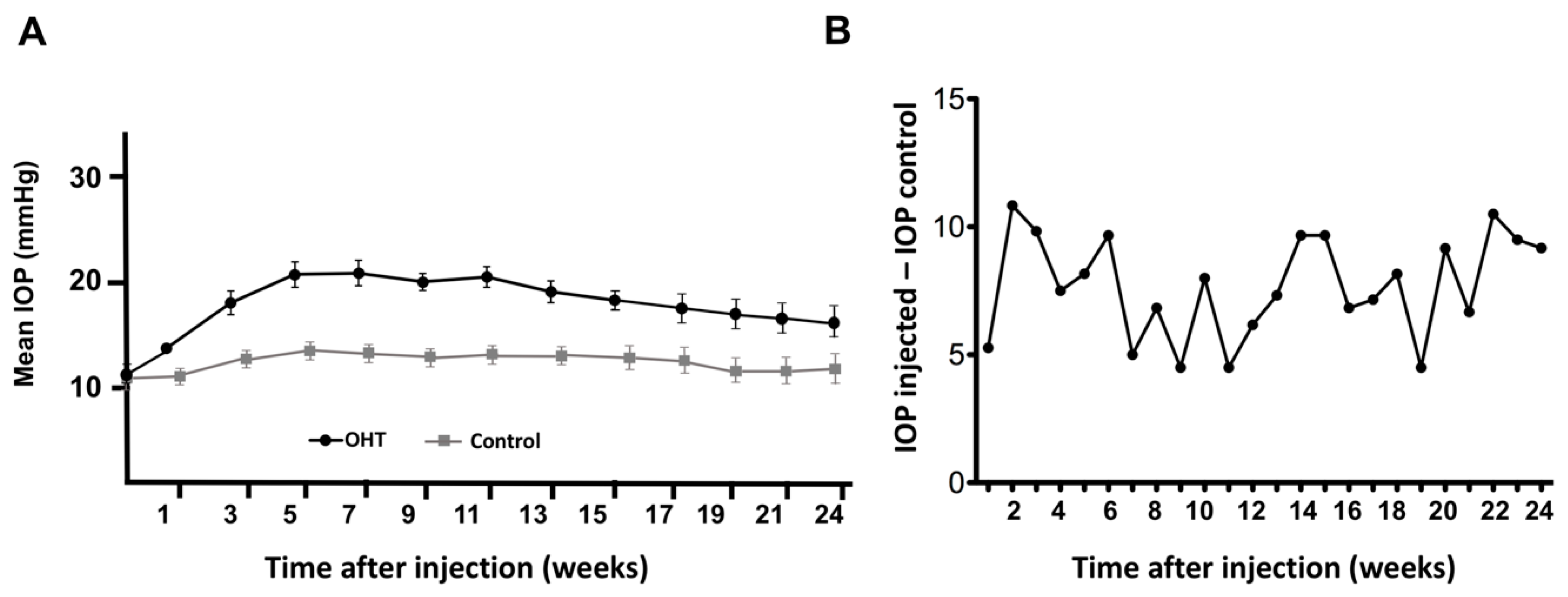
2.4. Intraocular Pressure Measurements
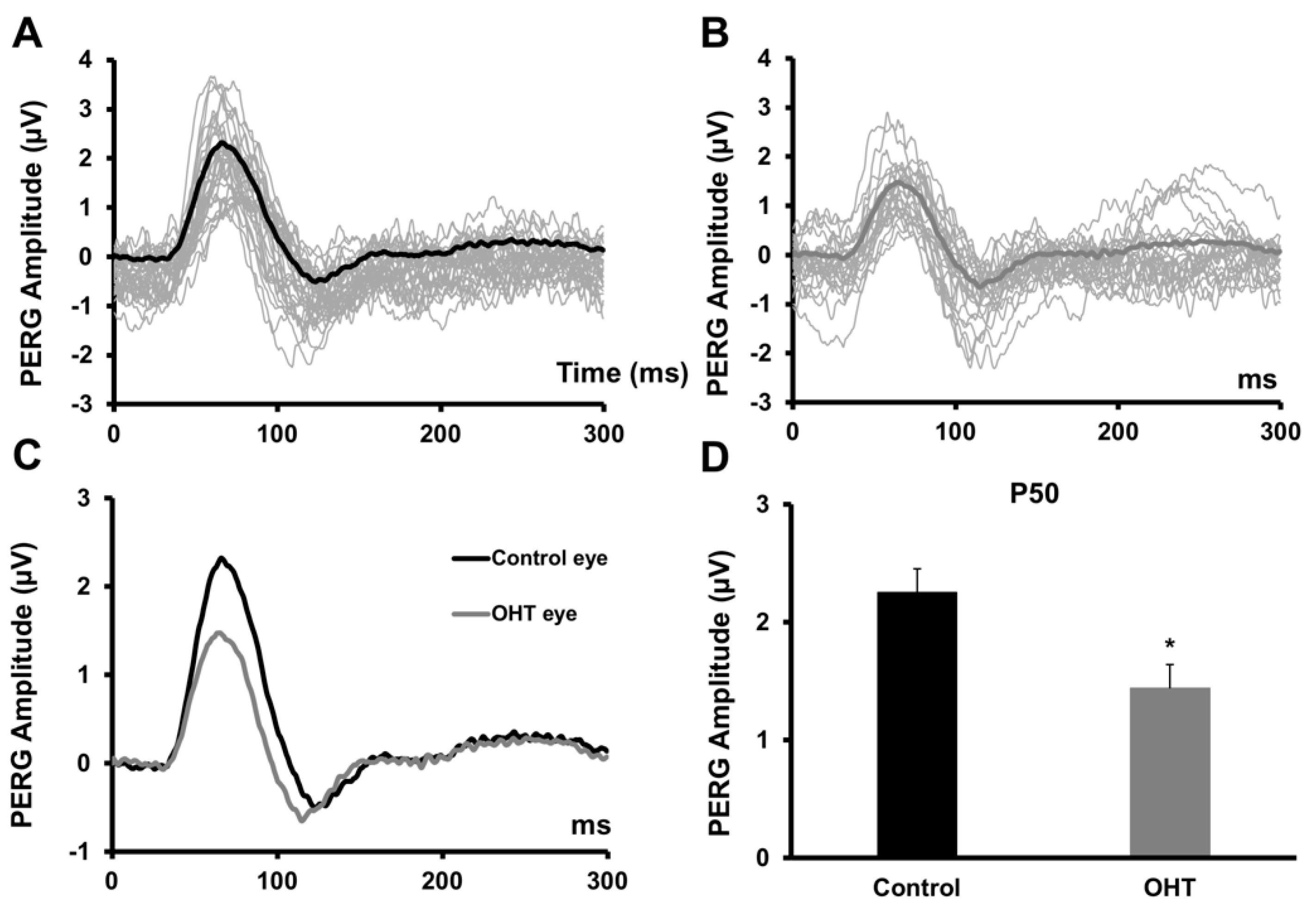
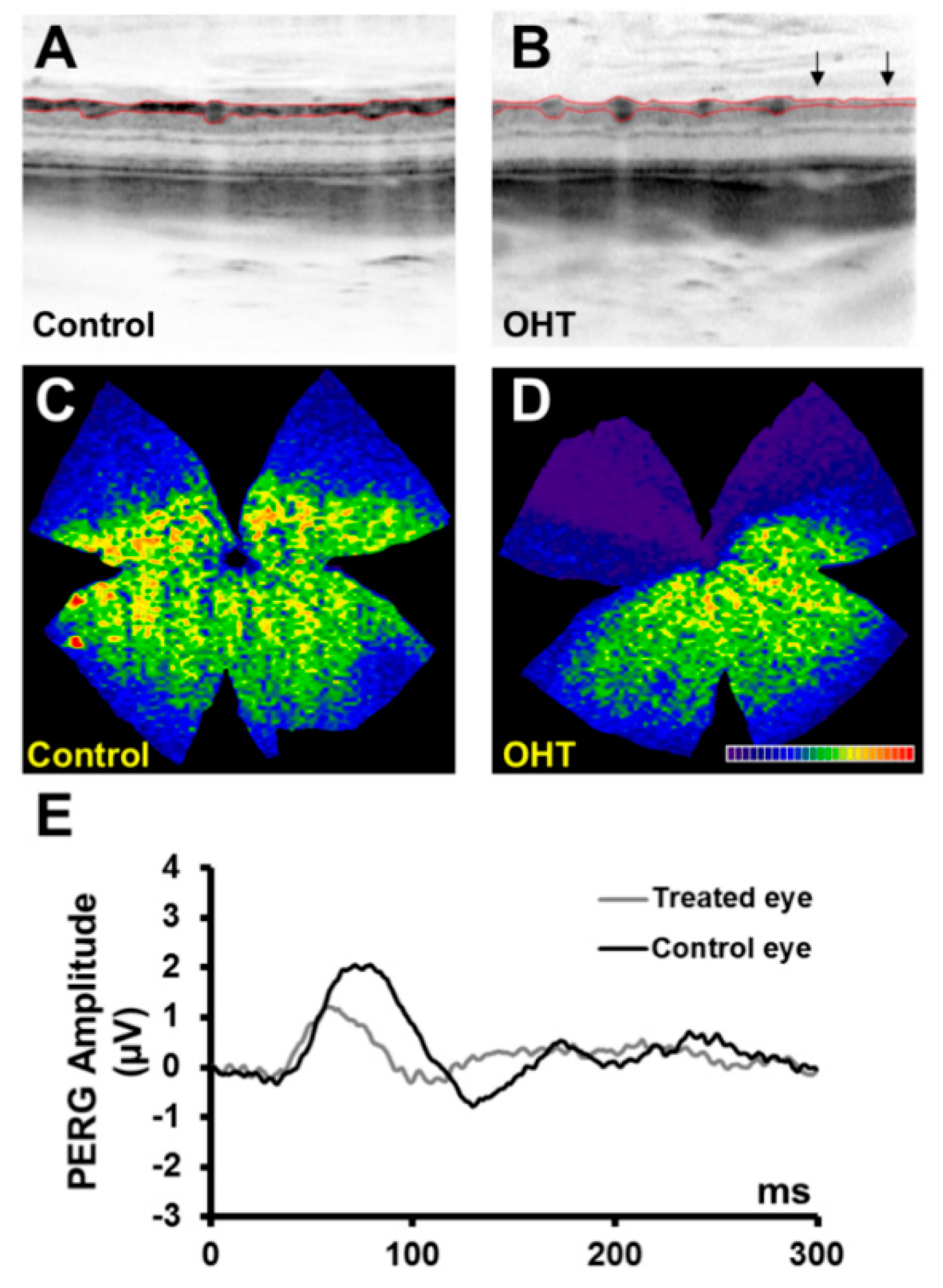
2.5. Pattern Electroretinogram (PERG)
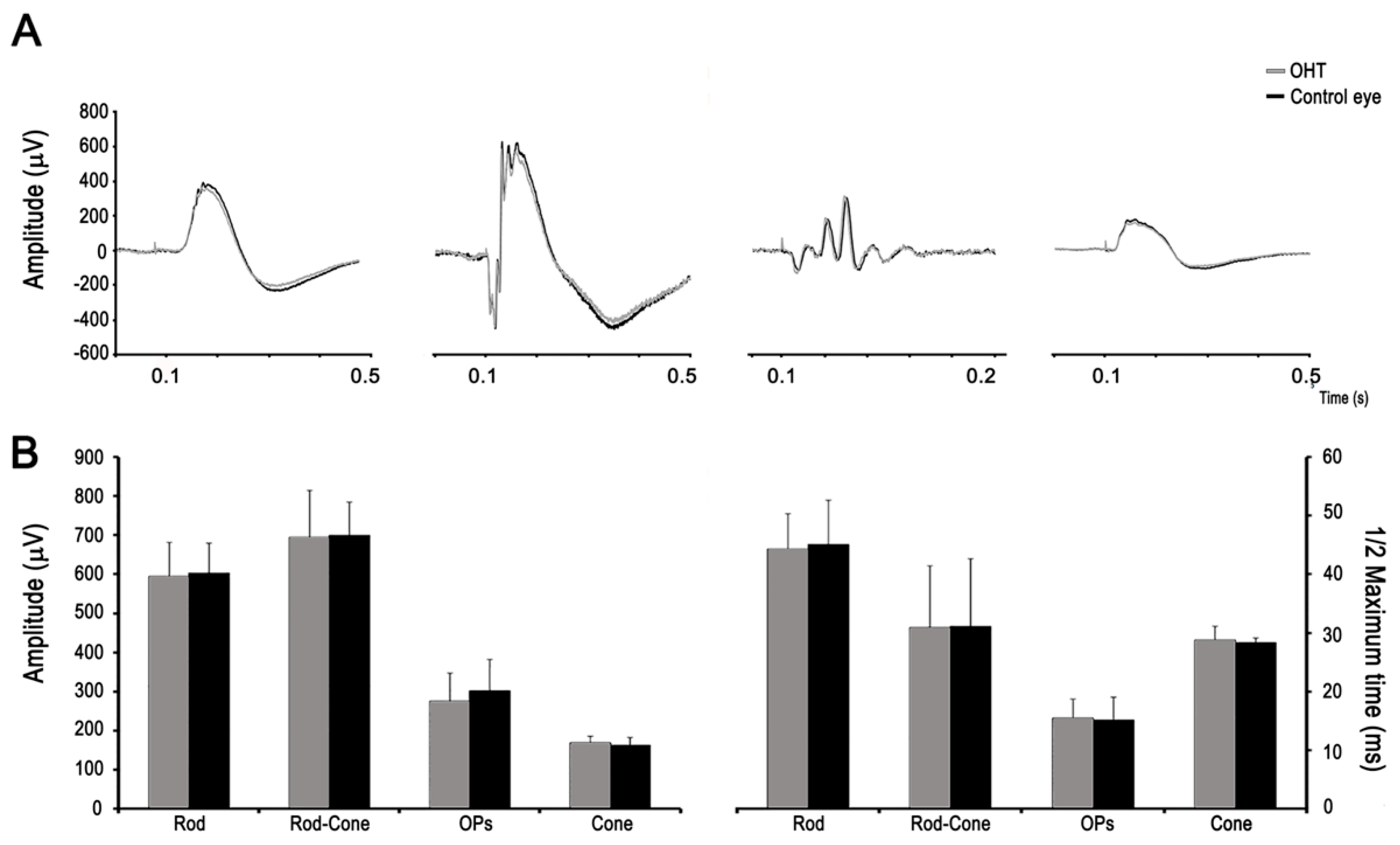
2.6. Full-Field Electroretinogram (ERG)
2.7. Spectral-Domain Optical Coherence Tomography (OCT)
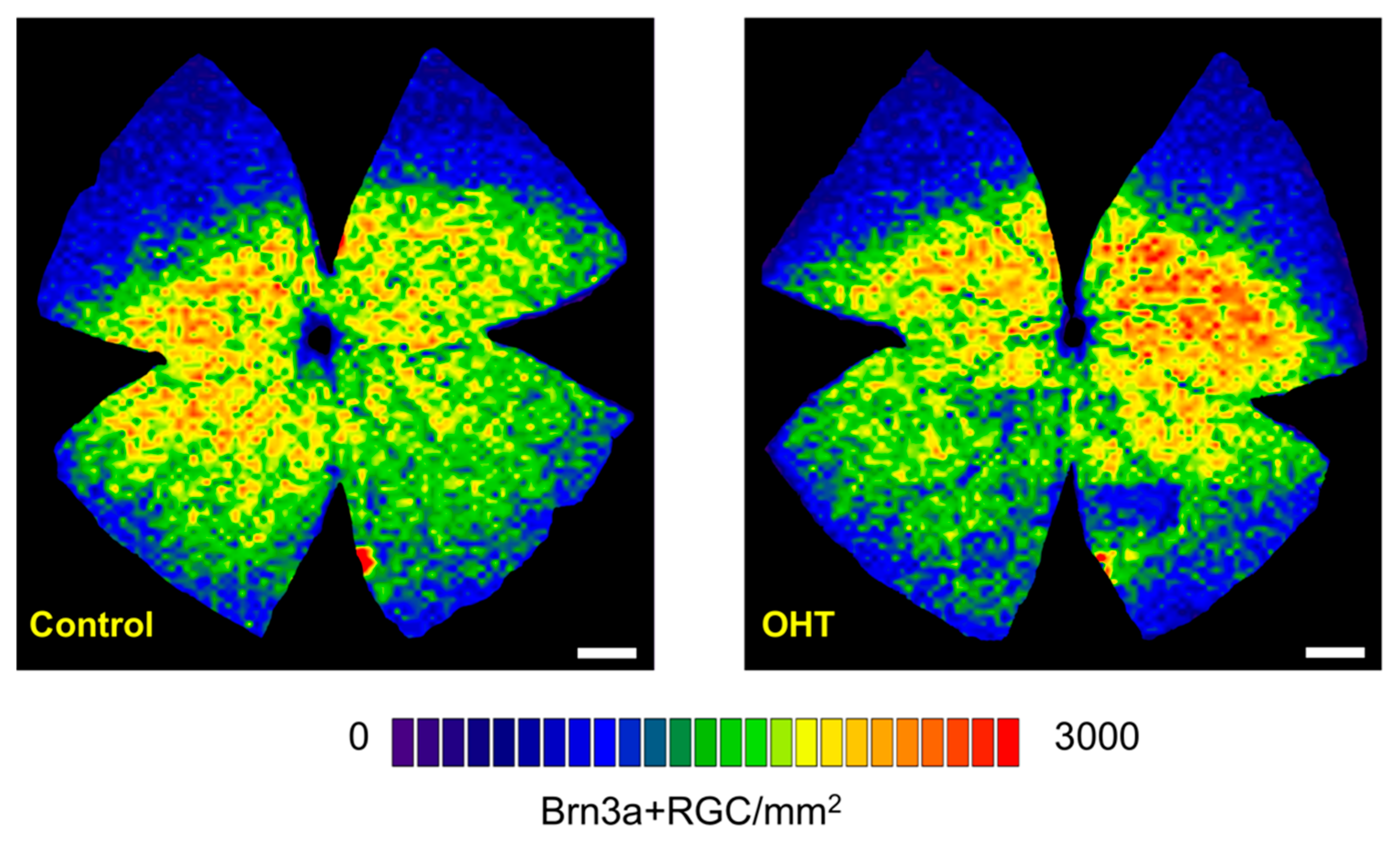
2.8. Brn3a Immunohistochemistry
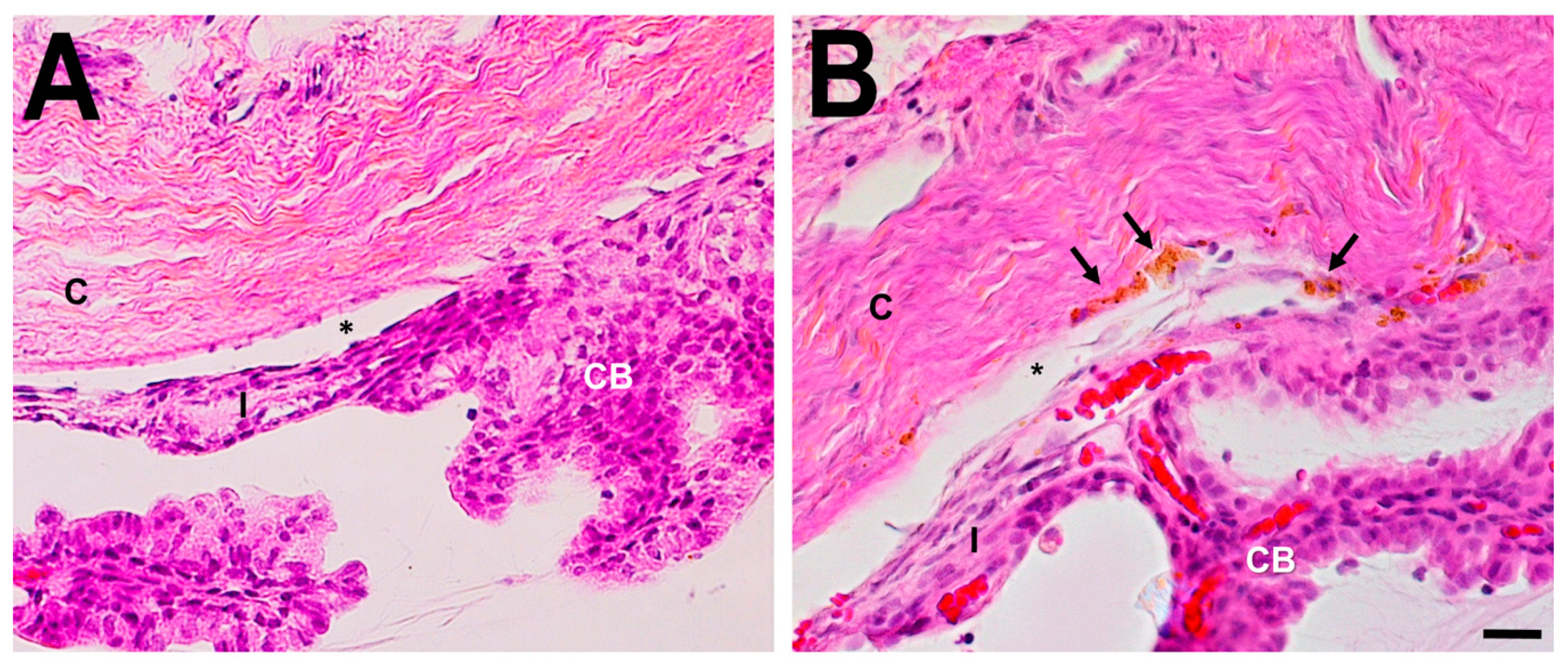
2.9. Histological Examination of the Anterior Segment
2.10. Data Analysis
3. Results
4. Discussion
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| OHT | Chronic ocular hypertension |
| IOP | Intraocular pressure |
| RGC | Retinal ganglion cells |
| PERG | Pattern electroretinogram |
| ERG | Full-field electroretinogram |
| RNFL | Retinal nerve fiber layer |
| OCT | Optical coherence tomography |
References
- Tham, Y.C.; Li, X.; Wong, T.Y.; Quigley, H.A.; Aung, T.; Cheng, C.Y. Global prevalence of glaucoma and projections of glaucoma burden through 2040: A systematic review and meta-analysis. Ophthalmology 2014, 121, 2081–2090. [Google Scholar] [CrossRef]
- Vidal-Sanz, M.; Valiente-Soriano, F.J.; Ortín-Martínez, A.; Nadal-Nicolás, F.M.; Jiménez-López, M.; Salinas-Navarro, M.; Alarcón-Martínez, L.; García-Ayuso, D.; Avilés-Trigueros, M.; Agudo-Barriuso, M.; et al. Retinal neurodegeneration in experimental glaucoma. Prog. Brain Res. 2015, 220, 1–35. [Google Scholar]
- Johnson, T.V.; Tomarev, S.I. Rodent models of glaucoma. Brain Res. Bull. 2010, 81, 349–358. [Google Scholar] [CrossRef]
- WoldeMussie, E.; Ruiz, G.; Wijono, M.; Wheeler, L.A. Neuroprotection of retinal ganglion cells by brimonidine in rats with laser-induced chronic ocular hypertension. Invest. Ophthalmol. Vis. Sci. 2001, 42, 2849–2855. [Google Scholar]
- Levkovitch-Verbin, H.; Quigley, H.A.; Martin, K.R.; Valenta, D.; Baumrind, L.A.; Pease, M.E. Translimbal laser photocoagulation to the trabecular meshworkas a model of glaucoma in rats. Invest. Ophthalmol. Vis. Sci. 2002, 43, 402–410. [Google Scholar]
- Morrison, J.C.; Moore, C.G.; Deppmeier, L.M.; Gold, B.G.; Meshul, C.K.; Johnson, E.C. A rat model of chronic pressure-induced optic nerve damage. Exp. Eye Res. 1997, 64, 85–96. [Google Scholar] [CrossRef]
- Bierman, J.; van Oterendorp, C.; Stoykow, C.; Volz, C.; Jehle, T.; Boehringer, D.; Lagrèze, W.A. Evaluation of intraocular pressure elevation in a modified laser-induced glaucoma model. Exp. Eye Res. 2012, 104, 7–14. [Google Scholar] [CrossRef]
- Shareef, S.R.; Garcia-Valenzuela, E.; Salierno, A.; Walsh, J.; Sharma, S.C. Chronic ocular hypertension following episcleral venous occlusion in rats. Exp. Eye Res. 1995, 61, 379–382. [Google Scholar] [CrossRef]
- Nastasa, V.; Samaras, K.; Ampatzidis Ch Karapantsios, T.D.; Trelles, M.A.; Moreno-Moraga, J.; Pascu, M.L. Properties of polidocanol foam in view of its use in sclerotherapy. Int. J. Pharm. 2015, 478, 588–596. [Google Scholar] [CrossRef]
- Rabe, E.; Breu, F.X.; Cavezzi, A.; Coleridge Smith, P.; Frullini, A.; Gillet, J.L.; Guex, J.J.; Hamel-Desnos, C.; Kern, P.; Partsch, B.; et al. European guidelines for sclerotherapy in chronic venous disorders. Phlebology 2013, 29, 338–354. [Google Scholar] [CrossRef]
- Ventura, L.M.; Porciatti, V.; Ishida, K.; Feuer, W.J.; Parrish, R.K., II. Pattern electroretinogram abnormality and glaucoma. Ophthalmology 2005, 112, 10–19. [Google Scholar] [CrossRef] [Green Version]
- Viswanathan, S.; Frishman, L.J.; Robson, J.G. The uniform field and pattern ERG in macaques with experimental glaucoma: Removal of spiking activity. Invest. Ophthalmol. Vis. Sci. 2000, 41, 2797–2810. [Google Scholar]
- Falsini, B.; Marangoni, D.; Salgarello, T.; Stifano, G.; Montrone, L.; Campagna, F.; Aliberti, S.; Balestrazzi, E.; Colotto, A. Structure-function relationship in ocular hypertension and glaucoma: Interindividual and interocular analysis by OCT and pattern ERG. Graefes Arch. Clin. Exp. Ophthalmol. 2008, 246, 1153–1162. [Google Scholar] [CrossRef]
- Valiente-Soriano, F.J.; Salinas-Navarro, M.A.; Bernal-Garro, J.M.; Agudo-Barriuso, M.; Vidal-Sanz, M.; Nadal-Nicolás, F.M.; Jiménez-López, M.; Villegas-Pérez, M.P. BDNF rescues RGCs but not intrinsically photosensitive RGCs in ocular hypertensive albino rat retinas. Invest. Ophthalmol. Vis. Sci. 2015, 56, 1924–1936. [Google Scholar] [CrossRef]
- Krishna, R.; Mermoud, A.; Baerveldt, G.; Minckler, D.S. Circadian rhythm of intraocular pressure: A rat model. Ophthalmic Res 1995, 27, 163–167. [Google Scholar] [CrossRef]
- Moore, C.G.; Johnson, E.C.; Morrison, J.C. Circadian rhythm of intraocular pressure in the rat. Curr. Eye Res. 1996, 15, 185–191. [Google Scholar] [CrossRef]
- Jia, L.; Cepurna, W.O.; Johnson, E.C.; Morrison, J.C. Effect of general anesthetics on IOP in rats with experimental aqueous outflow obstruction. Invest. Ophthalmol. Vis. Sci. 2000, 41, 3415–3419. [Google Scholar]
- Aihara, M.; Lindsey, J.D.; Weinreb, R.N. Twenty-four-hour pattern of mouse intraocular pressure. Exp. Eye Res. 2003, 77, 681–686. [Google Scholar] [CrossRef]
- Drouyer, E.; Dkhissi-Benyahya, O.; Chiquet, C.; WoldeMussie, E.; Ruiz, G.; Wheeler, L.A.; Denis, P.; Cooper, H.M. Glaucoma alters the circadian timing system. PLoS ONE 2008, 3, 3931. [Google Scholar] [CrossRef]
- Hughes, A. The refractive state of the rat eye. Vision Res 1977, 17, 927–939. [Google Scholar] [CrossRef]
- Ben-Shlomo, G.; Bakalash, S.; Lambrou, G.N.; Latour, E.; Dawson, W.W.; Schwartz, M.; Ofri, R. Pattern electroretinography in a rat model of ocular hypertension: Functional evidence for early detection of inner retinal damage. Exp. Eye Res. 2005, 81, 340–349. [Google Scholar] [CrossRef]
- Porciatti, V.; Pizzorusso, T.; Cenni, M.C.; Maffei, L. The visual response of retinal ganglion cells is not altered by optic nerve transaction in transgenic mice overexpressing Bcl-2. Proc. Natl. Acad. Sci. USA 1996, 93, 14955–14959. [Google Scholar] [CrossRef]
- Alarcón-Martínez, L.; de la Villa, P.; Avilés-Trigueros, M.; Blanco, R.; Villegas-Pérez, M.P.; Vidal-Sanz, M. Short and long term axotomy-induced ERG changes in albino and pigmented rats. Mol. Vis. 2009, 15, 2373–2383. [Google Scholar]
- Cuenca, N.; Pinilla, I.; Fernández-Sánchez, L.; Salinas-Navarro, M.; Alarcón-Martínez, L.; Avilés-Trigueros, M.; De La Villa, P.; De Imperial, J.M.; Villegas-Pérez, M.P.; Vidal-Sanz, M. Changes in the inner and outer retinal layers after acute increase of the intraocular pressure in adult albino Swiss mice. Exp. Eye Res. 2010, 91, 273–285. [Google Scholar] [CrossRef]
- McCulloch, D.L.; Marmor, M.F.; Brigell, M.G.; Hamilton, R.; Holder, G.E.; Tzekov, R.; Bach, M. ISCEV Standard for full-field clinical electroretinography. Doc. Ophthalmol. 2015, 130, 1–12. [Google Scholar] [CrossRef]
- Nagata, A.; Higashide, T.; Ohkubo, S.; Takeda, H.; Sugiyama, K. In vivo quantitative evaluation of the rat retinal nerve fiber layer with optical coherence tomography. Invest. Ophthalmol. Vis. Sci. 2009, 50, 2809–2815. [Google Scholar] [CrossRef]
- Rovere, G.; Nadal-Nicolás, F.M.; Agudo-Barriuso, M.; Sobrado-Calvo, P.; Nieto-López, L.; Nucci, C.; Villegas-Pérez, M.P.; Vidal-Sanz, M. Principio del formulario. Comparison of retinal nerve fiber layer thinning and retinal ganglion cell loss after optic nerve transection in adult albino rats. Invest. Ophthalmol. Vis. Sci. 2015, 56, 4487–4498. [Google Scholar] [CrossRef]
- Salinas-Navarro, M.; Alarcón-Martínez, L.; Valiente-Soriano, F.J.; Jiménez-López, M.; Mayor-Torroglosa, S.; Avilés-Trigueros, M.; Villegas-Pérez, M.P.; Vidal-Sanz, M. Ocular hypertension impairs optic nerve axonal transport leading to progressive retinal ganglion cell degeneration. Exp. Eye Res. 2010, 90, 168–183. [Google Scholar] [CrossRef]
- Ortin-Martinez, A.; Salinas-Navarro, M.; Vidal-Sanz, M.; Agudo-Barriuso, M.; Jiménez-López, M.; Nadal-Nicolás, F.M.; Alarcón-Martínez, L.; Sauvé, Y.; Villegas-Pérez, M.P. Automated quantification and topographical distribution of the whole population of S- and L-cones in adult albino and pigmented rats. Invest. Ophthalmol. Vis. Sci. 2010, 51, 3171–3183. [Google Scholar] [CrossRef]
- Morrison, J.C.; Johnson, E.; Cepurna, W.O. Rat models for glaucoma research. Prog. Brain Res. 2008, 173, 285–301. [Google Scholar]
- Fortune, B.; Bui, B.V.; Morrison, J.C.; Johnson, E.C.; Dong, J.; Cepurna, W.O.; Jia, L.; Barber, S.; Cioffi, G.A. Selective ganglion cell functional loss in rats with experimental glaucoma. Invest. Ophthalmol. Vis. Sci. 2004, 45, 1854–1862. [Google Scholar] [CrossRef]
- Liu, H.H.; Bui, B.V.; Nguyen, C.T.; Kezic, J.M.; Vingrys, A.J.; He, Z. Chronic ocular hypertension induced by circumlimbal suture in rats. Invest. Ophthalmol. Vis. Sci. 2015, 56, 2811–2820. [Google Scholar] [CrossRef]
- Pang, J.J.; Frankfort, B.J.; Gross, R.L.; Wu, S.M. Elevated intraocular pressure decreases response sensitivity of inner retinal neurons in experimental glaucoma mice. Proc. Natl. Acad. Sci. USA 2015, 112, 2593–2598. [Google Scholar] [CrossRef] [Green Version]
- Weber, A.J.; Kaufman, P.L.; Hubbard, W.C. Morphology of single ganglion cells in the glaucomatous primate retina. Invest. Ophthalmol. Vis. Sci. 1998, 39, 2304–2320. [Google Scholar]
- Kass, M.A.; Heuer, D.K.; Higginbotham, E.J.; AJohnson, C.; Keltner, J.L.; Miller, J.P.; Parrish, R.K.; Wilson, M.R.; Gordon, M.O. The Ocular Hypertension Treatment Study: A randomized trial determines that topical ocular hypotensive medication delays or prevents the onset of primary open-angle glaucoma. Arch. Ophthalmol. 2002, 120, 701–713. [Google Scholar] [CrossRef]
- Feghali, J.G.; Jin, J.C.; Odom, J.V. Effect of short-term intraocular pressure elevation on the rabbit electroretinogram. Invest. Ophthalmol. Vis. Sci. 1991, 32, 2184–2189. [Google Scholar]
- Bach, M.; Unsoeld, A.S.; Philippin, H.; Staubach, F.; Maier, P.; Walter, H.S.; Bomer, T.G.; Funk, J. Pattern ERG as an early glaucoma indicator in ocular hypertension: A long-term, prospective study. Invest. Ophthalmol. Vis. Sci. 2006, 47, 4881–4887. [Google Scholar] [CrossRef]
- Hood, D.C.; Xu, L.; Thienprasiddhi, P.; Greenstein, V.C.; Odel, J.G.; Grippo, T.M.; Liebmann, J.M.; Ritch, R. The pattern electroretinogram in glaucoma patients with confirmed visual field deficits. Invest. Ophthalmol. Vis. Sci. 2005, 46, 2411–2418. [Google Scholar] [CrossRef]
- Korth, M.; Horn, F.; Stork, B.; Jonas, J. The pattern evoked electroretinogram: Age-related alterations and changes in glaucoma. Graefes Arch. Clin. Exp. Ophthalmol. 1989, 227, 123–131. [Google Scholar] [CrossRef]
- Porciatti, V.; Falsini, B.; Brunori, S.; Colotto, A.; Moretti, G. Pattern electroretinogram as a function of spatial frequency in ocular hypertension and early glaucoma. Doc. Ophthalmol. 1987, 65, 349–355. [Google Scholar] [CrossRef]
- Salgarello, T.; Colotto, A.; Falsini, B.; Buzzonetti, L.; Cesari, L.; Iarossi, G.; Scullica, L. Correlation of pattern electroretinogram with optic disc cup shape in ocular hypertension. Invest. Ophthalmol. Vis. Sci. 1999, 40, 1989–1997. [Google Scholar]
- Ventura, L.M.; Sorokac, N.; De Los Santos, R.; Feuer, W.J.; Porciatti, V. The relationship between retinal ganglion cell function and retinal nerve fiber thickness in early glaucoma. Invest. Ophthalmol. Vis. Sci. 2006, 47, 3904–3911. [Google Scholar] [CrossRef]
- Bowd, C.; Weinreb, R.N.; Williams, J.M.; Zangwill, L.M. The retinal nerve fiber layer thickness in ocular hypertensive, normal, and glaucomatous eyes with optical coherence tomography. Arch. Ophthalmol. 2000, 118, 22–26. [Google Scholar] [CrossRef]
- Wollstein, G.; Schuman, J.S.; Price, L.L.; Aydin, A.; Stark, P.C.; Hertzmark, E.; Lai, E.; Ishikawa, H.; Mattox, C.; Fujimoto, J.G.; et al. Optical coherence tomography longitudinal evaluation of retinal nerve fiber layer thickness in glaucoma. Arch. Ophthalmol. 2005, 123, 464–470. [Google Scholar] [CrossRef]
- Joos, K.M.; Li, C.; Sappington, R.M. Morphometric changes in the rat optic nerve following short-term intermittent elevations in intraocular pressure. Invest. Ophthalmol. Vis. Sci. 2010, 51, 6431–6440. [Google Scholar] [CrossRef]
- Bayer, A.; Danias, J.; Brodie, S.; Maag, K.-P.; Chen, B.; Shen, F.; Podos, S.; Mittag, T. Electroretinographic abnormalities in a rat glaucoma model with chronic elevated intraocular pressure. Exp. Eye Res. 2001, 72, 667–677. [Google Scholar] [CrossRef]
- Aldebasi, Y.H.; Drasdo, N.; Morgan, J.E.; North, R.V. S-cone, L + M-cone, and pattern, electroretinograms in ocular hypertension and glaucoma. Vis. Res. 2004, 44, 2749–2756. [Google Scholar] [CrossRef]
- Porciatti, V. Electrophysiological assessment of retinal ganglion cell function. Exp. Eye Res. 2015, 141, 164–170. [Google Scholar] [CrossRef] [Green Version]
- Mittag, T.W.; Danias, J.; Pohorenec, G.; Yuan, H.M.; Burakgazi, E.; Chalmers-Redman, R.; Podos, S.M.; Tatton, W.G. Retinal damage after 3 to 4 months of elevated intraocular pressure in a rat glaucoma model. Invest. Ophthalmol. Vis. Sci. 2000, 41, 3451–3459. [Google Scholar]
- Grozdanic, S.D.; Kwon, Y.H.; Sakaguchi, D.S.; Kardon, R.H.; Sonea, I.M. Functional evaluation of retina and optic nerve in the rat model of chronic ocular hypertension. Exp. Eye Res. 2004, 79, 75–83. [Google Scholar] [CrossRef]
- Ortin-Martinez, A.; Salinas-Navarro, M.; Nadal-Nicolás, F.M.; Jiménez-López, M.; Valiente-Soriano, F.J.; García-Ayuso, D.; Bernal-Garro, J.M.; Avilés-Trigueros, M.; Agudo-Barriuso, M.; Villegas-Pérez, M.P.; et al. Laser -induced ocular hypertension in adult rats does not affect non-RGC neurons in the ganglion cell layer but results in protracted severe loss of cone-photoreceptors. Exp. Eye Res. 2015, 132, 17–33. [Google Scholar] [CrossRef]







© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Blanco, R.; Martinez-Navarrete, G.; Pérez-Rico, C.; Valiente-Soriano, F.J.; Avilés-Trigueros, M.; Vicente, J.; Fernandez, E.; Vidal-Sanz, M.; de la Villa, P. A Chronic Ocular-Hypertensive Rat Model induced by Injection of the Sclerosant Agent Polidocanol in the Aqueous Humor Outflow Pathway. Int. J. Mol. Sci. 2019, 20, 3209. https://doi.org/10.3390/ijms20133209
Blanco R, Martinez-Navarrete G, Pérez-Rico C, Valiente-Soriano FJ, Avilés-Trigueros M, Vicente J, Fernandez E, Vidal-Sanz M, de la Villa P. A Chronic Ocular-Hypertensive Rat Model induced by Injection of the Sclerosant Agent Polidocanol in the Aqueous Humor Outflow Pathway. International Journal of Molecular Sciences. 2019; 20(13):3209. https://doi.org/10.3390/ijms20133209
Chicago/Turabian StyleBlanco, Román, Gema Martinez-Navarrete, Consuelo Pérez-Rico, Francisco J. Valiente-Soriano, Marcelino Avilés-Trigueros, Javier Vicente, Eduardo Fernandez, Manuel Vidal-Sanz, and Pedro de la Villa. 2019. "A Chronic Ocular-Hypertensive Rat Model induced by Injection of the Sclerosant Agent Polidocanol in the Aqueous Humor Outflow Pathway" International Journal of Molecular Sciences 20, no. 13: 3209. https://doi.org/10.3390/ijms20133209