Routes of Clonal Evolution into Complex Karyotypes in Myelodysplastic Syndrome Patients with 5q Deletion

Abstract
:1. Introduction
2. Results
3. Discussion
4. Material and Methods
4.1. Patient Characteristics
4.2. Fluorescence R-Banding and Analysis of Karyotypes
4.3. FISH
4.4. mFISH
4.5. Statistical Analysis
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| AML | Acute myeloid leukemia |
| del(5q) | Deletion of 5q |
| CyDAS | Cytogenetic Data Analysis System |
| FISH | Fluorescence in situ hybridization |
| MDS | Myelodysplastic syndrome |
| m | Multicolor |
| WHO | World Health Organization |
References
- Arber, D.A.; Orazi, A.; Hasserjian, R.; Thiele, J.; Borowitz, M.J.; Le Beau, M.M.; Bloomfield, C.D.; Cazzola, M.; Vardiman, J.W. The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia. Blood 2016, 127, 2391–2405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greenberg, P.L.; Tuechler, H.; Schanz, J.; Sanz, G.; Garcia-Manero, G.; Sole, F.; Bennett, J.M.; Bowen, D.; Fenaux, P.; Dreyfus, F.; et al. Revised international prognostic scoring system for myelodysplastic syndromes. Blood 2012, 120, 2454–2465. [Google Scholar] [CrossRef] [PubMed]
- Haase, D.; Germing, U.; Schanz, J.; Pfeilstöcker, M.; Nösslinger, T.; Hildebrandt, B.; Kundgen, A.; Lübbert, M.; Kunzmann, R.; Giagounidis, A.A.N.; et al. New insights into the prognostic impact of the karyotype in MDS and correlation with subtypes: Evidence from a core dataset of 2124 patients. Blood 2007, 110, 4385–4395. [Google Scholar] [CrossRef] [PubMed]
- Ding, L.; Ley, T.J.; Larson, D.E.; Miller, C.A.; Koboldt, D.C.; Welch, J.S.; Ritchey, J.K.; Young, M.A.; Lamprecht, T.; McLellan, M.D.; et al. Clonal evolution in relapsed acute myeloid leukaemia revealed by whole-genome sequencing. Nature 2012, 481, 506–510. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schanz, J.; Tüchler, H.; Solé, F.; Mallo, M.; Luño, E.; Cervera, J.; Granada, I.; Hildebrandt, B.; Slovak, M.L.; Ohyashiki, K.; et al. New comprehensive cytogenetic scoring system for primary myelodysplastic syndromes (MDS) and oligoblastic acute myeloid leukemia after MDS derived from an international database merge. J. Clin. Oncol. 2012, 30, 820–829. [Google Scholar] [CrossRef] [PubMed]
- Schanz, J.; Cevik, N.; Fonatsch, C.; Braulke, F.; Shirneshan, K.; Bacher, U.; Haase, D. Detailed analysis of clonal evolution and cytogenetic evolution patterns in patients with myelodysplastic syndromes (MDS) and related myeloid disorders. Blood Cancer J. 2018, 8, 28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strupp, C.; Nachtkamp, K.; Hildebrandt, B.; Giagounidis, A.; Haas, R.; Gattermann, N.; Bennett, J.M.; Aul, C.; Germing, U. New proposals of the WHO working group (2016) for the diagnosis of myelodysplastic syndromes (MDS): Characteristics of refined MDS types. Leuk. Res. 2017, 57, 78–84. [Google Scholar] [CrossRef] [PubMed]
- Kaivers, J.; Lauseker, M.; Hildebrandt, B.; Fenaux, P.; Pfeilstocker, M.; Valent, P.; Platzbecker, U.; Latagliata, R.; Oliva, E.N.; Xicoy, B.; et al. The IPSS-R has prognostic impact in untreated patients with MDS del(5q). Leuk. Res. 2018, 72, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Göhring, G.; Lange, K.; Hofmann, W.; Nielsen, K.V.; Hellström-Lindberg, E.; Roy, L.; Morgan, M.; Kreipe, H.; Büsche, G.; Giagounidis, A.; et al. Telomere shortening, clonal evolution and disease progression in myelodysplastic syndrome patients with 5q deletion treated with lenalidomide. Leukemia 2012, 26, 356–358. [Google Scholar] [CrossRef] [PubMed]
- Göhring, G.; Giagounidis, A.; Büsche, G.; Kreipe, H.H.; Zimmermann, M.; Hellström-Lindberg, E.; Aul, C.; Schlegelberger, B. Patients with del(5q) MDS who fail to achieve sustained erythroid or cytogenetic remission after treatment with lenalidomide have an increased risk for clonal evolution and AML progression. Ann. Hematol. 2010, 89, 365–374. [Google Scholar] [CrossRef] [PubMed]
- Jädersten, M.; Saft, L.; Smith, A.; Kulasekararaj, A.; Pomplun, S.; Göhring, G.; Hedlund, A.; Hast, R.; Schlegelberger, B.; Porwit, A.; et al. TP53 mutations in low-risk myelodysplastic syndromes with del(5q) predict disease progression. J. Clin. Oncol. 2011, 29, 1971–1979. [Google Scholar] [CrossRef] [PubMed]
- Welch, J.S.; Ley, T.J.; Link, D.C.; Miller, C.A.; Larson, D.E.; Koboldt, D.C.; Wartman, L.D.; Lamprecht, T.L.; Liu, F.; Xia, J.; et al. The origin and evolution of mutations in acute myeloid leukemia. Cell 2012, 150, 264–278. [Google Scholar] [CrossRef] [PubMed]
- Tehranchi, R.; Woll, P.S.; Anderson, K.; Buza-Vidas, N.; Mizukami, T.; Mead, A.J.; Astrand-Grundström, I.; Strömbeck, B.; Horvat, A.; Ferry, H.; et al. Persistent malignant stem cells in del(5q) myelodysplasia in remission. N. Engl. J. Med. 2010, 363, 1025–1037. [Google Scholar] [CrossRef] [PubMed]
- Greaves, M.; Maley, C.C. Clonal evolution in cancer. Nature 2012, 481, 306–313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walter, M.J.; Shen, D.; Ding, L.; Shao, J.; Koboldt, D.C.; Chen, K.; Larson, D.E.; McLellan, M.D.; Dooling, D.; Abbott, R.; et al. Clonal architecture of secondary acute myeloid leukemia. N. Engl. J. Med. 2012, 366, 1090–1098. [Google Scholar] [CrossRef] [PubMed]
- Fearon, E.R.; Vogelstein, B. A genetic model for colorectal tumorigenesis. Cell 1990, 61, 759–767. [Google Scholar] [CrossRef]
- Abaigar, M.; Robledo, C.; Benito, R.; Ramos, F.; Diez-Campelo, M.; Hermosin, L.; Sanchez-Del-Real, J.; Alonso, J.M.; Cuello, R.; Megido, M.; et al. Chromothripsis Is a Recurrent Genomic Abnormality in High-Risk Myelodysplastic Syndromes. PLoS ONE 2016, 11, e0164370. [Google Scholar] [CrossRef] [PubMed]
- Akagi, T.; Ogawa, S.; Dugas, M.; Kawamata, N.; Yamamoto, G.; Nannya, Y.; Sanada, M.; Miller, C.W.; Yung, A.; Schnittger, S.; et al. Frequent genomic abnormalities in acute myeloid leukemia/myelodysplastic syndrome with normal karyotype. Haematologica 2009, 94, 213–223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stephens, P.J.; Greenman, C.D.; Fu, B.; Yang, F.; Bignell, G.R.; Mudie, L.J.; Pleasance, E.D.; Lau, K.W.; Beare, D.; Stebbings, L.A; et al. Massive genomic rearrangement acquired in a single catastrophic event during cancer development. Cell 2011, 144, 27–40. [Google Scholar] [CrossRef] [PubMed]
- Hiller, B.; Bradtke, J.; Balz, H.; Rieder, H. CyDAS: A cytogenetic data analysis system. Bioinformatics 2005, 21, 1282–1283. [Google Scholar] [CrossRef] [PubMed]
- Gurney, M.; Patnaik, M.M.; Hanson, C.A.; Litzow, M.R.; Al-Kali, A.; Ketterling, R.P.; Tefferi, A.; Gangat, N. The 2016 revised World Health Organization definition of “myelodysplastic syndrome with isolated del(5q)”; prognostic implications of single versus double cytogenetic abnormalities. Br. J. Haematol. 2017, 178, 57–60. [Google Scholar] [CrossRef] [PubMed]
- Rausch, T.; Jones, D.T.W.; Zapatka, M.; Stütz, A.M.; Zichner, T.; Weischenfeldt, J.; Jäger, N.; Remke, M.; Shih, D.; Northcott, P.A.; et al. Genome sequencing of pediatric medulloblastoma links catastrophic DNA rearrangements with TP53 mutations. Cell 2012, 148, 59–71. [Google Scholar] [CrossRef] [PubMed]
- Kulasekararaj, A.G.; Smith, A.E.; Mian, S.A.; Mohamedali, A.M.; Krishnamurthy, P.; Lea, N.C.; Gäken, J.; Pennaneach, C.; Ireland, R.; Czepulkowski, B.; et al. TP53 mutations in myelodysplastic syndrome are strongly correlated with aberrations of chromosome 5, and correlate with adverse prognosis. Br. J. Haematol. 2013, 160, 660–672. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schlegelberger, B.; Metzke, S.; Harder, S.; Zühlke-Jenisch, R.; Zhang, Y.; Siebert, R. Classical and molecular Cytogenetics of tumor cells. Diagnostic Cytogenetics; Springer: Berlin/Heidelberg, Germany, 1999; pp. 151–185. [Google Scholar]
- Göhring, G.; Karow, A.; Steinemann, D.; Wilkens, L.; Lichter, P.; Zeidler, C.; Niemeyer, C.; Welte, K.; Schlegelberger, B. Chromosomal aberrations in congenital bone marrow failure disorders--an early indicator for leukemogenesis? Ann. Hematol. 2007, 86, 733–739. [Google Scholar] [CrossRef] [PubMed]
- Lange, K.; Gadzicki, D.; Schlegelberger, B.; Göhring, G. Recurrent involvement of heterochromatic regions in multiple myeloma-a multicolor FISH study. Leuk. Res. 2010, 34, 1002–1006. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Total Cohort | ||
| Patients with del(5q) | 1684 | |
| Patients with acquired additional aberrations at the time of diagnosis/during follow-up | 161 | |
| Patients with clonal evolution within the del(5q) clone | 134 | |
| Patients with independent clones | 27 | |
| Subcategories | ||
| Isolated Del(5q) | Number | Example |
| Initial cytogenetic status at first time point | 112/134 | 46,XX,del(5)(q14q34)[14]/46,XX[6] |
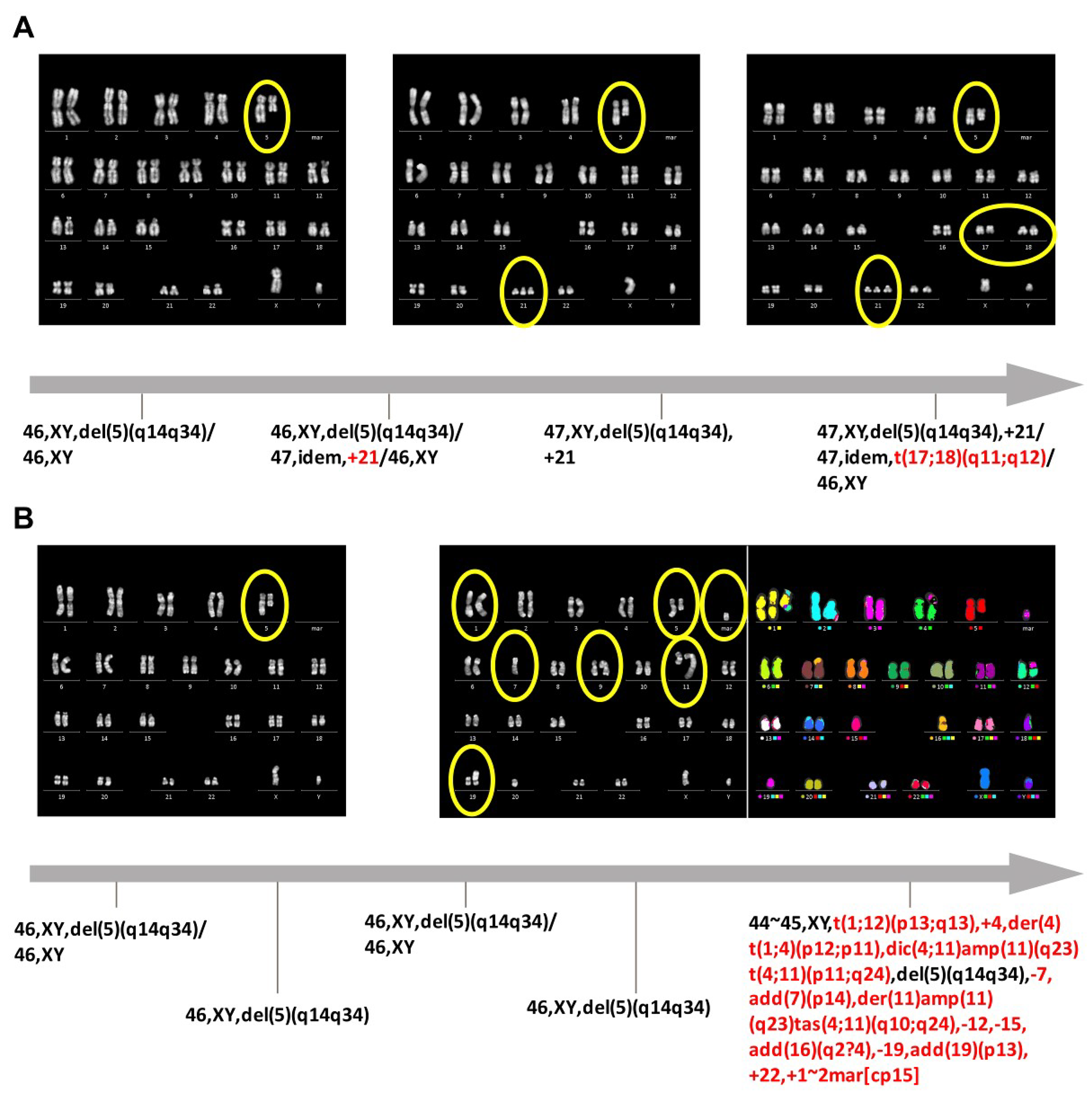
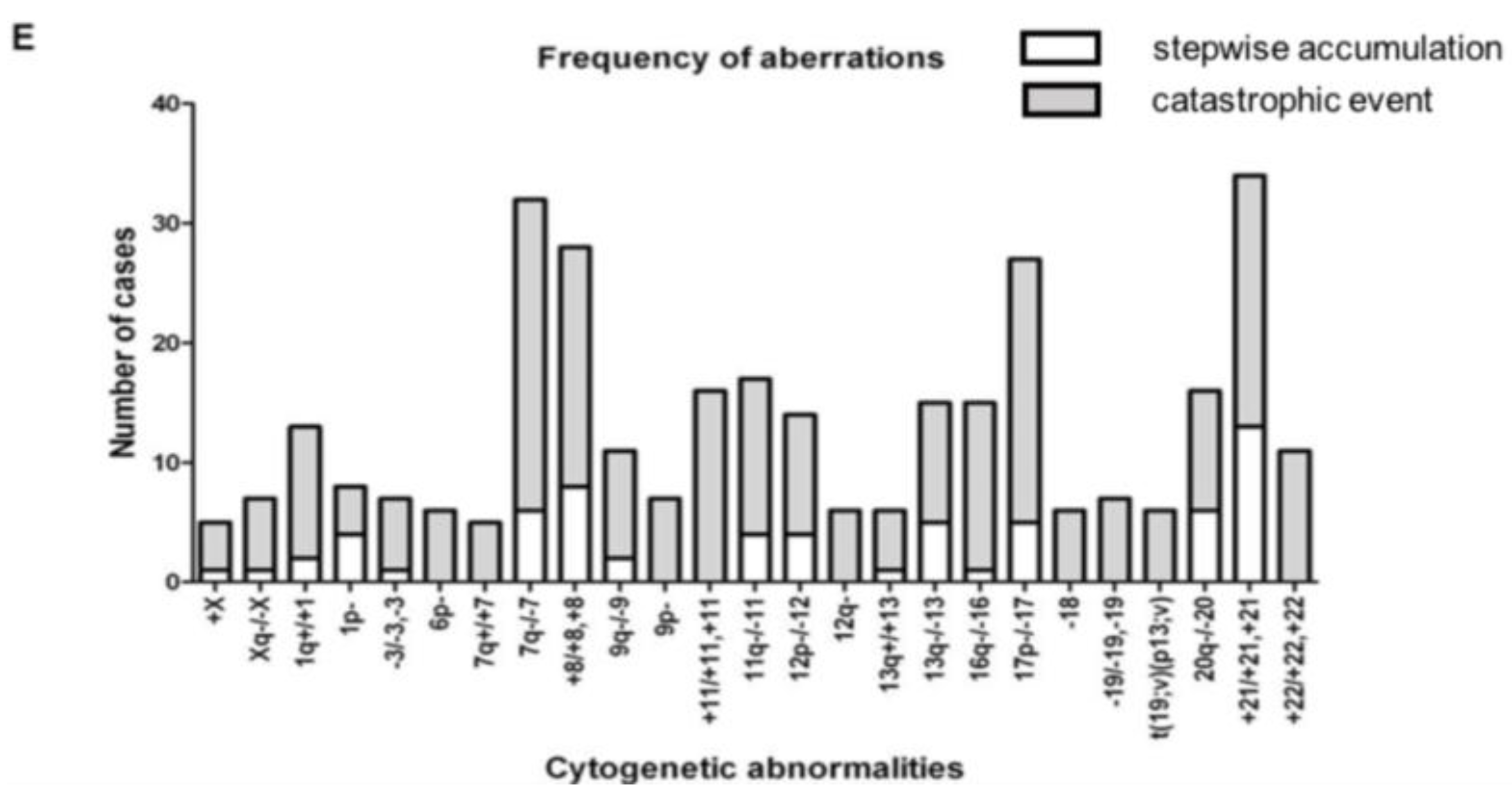
| Stepwise accumulation of cytogenetic events | 70 | |
| -Not resulting in complex karyotypes | 58 | 46,XX,del(5)(q14q34)[3]/47,idem,+21[17] |
| -Resulting in complex karyotypes | 12 | 46,XX,del(5)(q14q34)[3]/47,idem,+21[10]/47,idem,del(12)(p12p13),+21[7] |
| Catastrophic event * | 42 | 46,XX,del(5)(q14q34)[3]/44,idem,-7,dic(8;17)(p11;p11),del(12)(p12p13),-18[17] |
| Del(5q) and One Additional Aberration | Number | Example |
| Initial cytogenetic status at first time point | 22/134 | 46,XX,del(5)(q14q34),del(20)(q12q13)[11]/46,XX[9] |
| Stepwise accumulation of cytogenetic events | 12 | |
| -Not resulting in complex karyotypes | 0 | |
| -Resulting in complex karyotypes | 12 | 46,XX,del(5)(q14q34),del(20)(q12q13)[4]/46,idem,del(11)(q14) [16] |
| Catastrophic event * | 10 | 46,XX,del(5)(q14q34),del(20)(q12q13)[5]/46,idem,t(4;16)(q32;q12),del(7)(q21q31),+8,-17,add(22)(q12) [15] |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Feurstein, S.; Thomay, K.; Hofmann, W.; Buesche, G.; Kreipe, H.; Thol, F.; Heuser, M.; Ganser, A.; Schlegelberger, B.; Göhring, G. Routes of Clonal Evolution into Complex Karyotypes in Myelodysplastic Syndrome Patients with 5q Deletion. Int. J. Mol. Sci. 2018, 19, 3269. https://doi.org/10.3390/ijms19103269
Feurstein S, Thomay K, Hofmann W, Buesche G, Kreipe H, Thol F, Heuser M, Ganser A, Schlegelberger B, Göhring G. Routes of Clonal Evolution into Complex Karyotypes in Myelodysplastic Syndrome Patients with 5q Deletion. International Journal of Molecular Sciences. 2018; 19(10):3269. https://doi.org/10.3390/ijms19103269
Chicago/Turabian StyleFeurstein, Simone, Kathrin Thomay, Winfried Hofmann, Guntram Buesche, Hans Kreipe, Felicitas Thol, Michael Heuser, Arnold Ganser, Brigitte Schlegelberger, and Gudrun Göhring. 2018. "Routes of Clonal Evolution into Complex Karyotypes in Myelodysplastic Syndrome Patients with 5q Deletion" International Journal of Molecular Sciences 19, no. 10: 3269. https://doi.org/10.3390/ijms19103269