
Kinkéliba (Combretum micranthum) Leaf Extract Alleviates Skin Inflammation: In Vitro and In Vivo Study

Abstract
:1. Introduction
2. Results
2.1. Definition of UVA Dosage
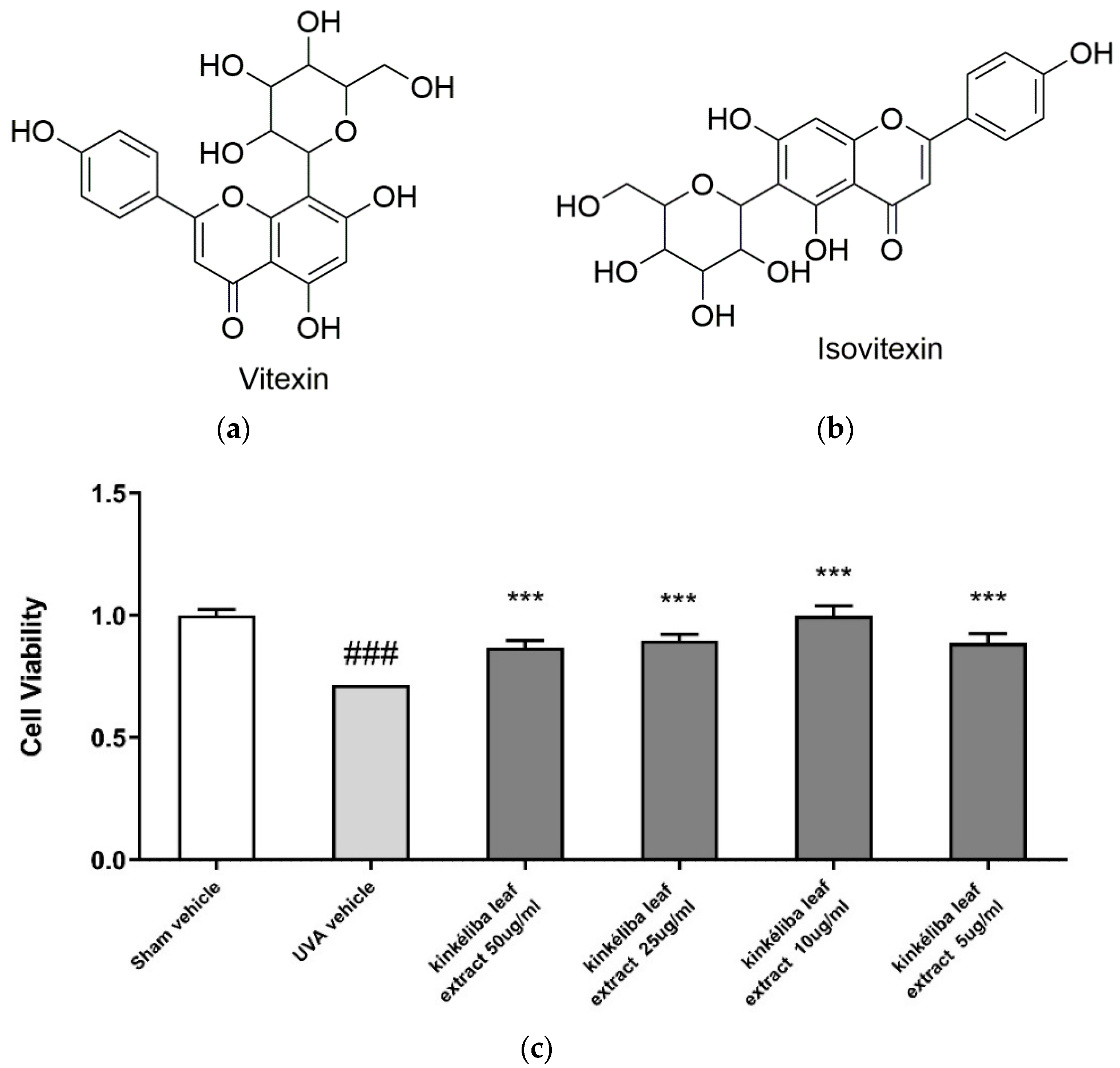
2.2. Kinkéliba Leaf Extract Enhanced Cell Viability after UVA Irradiation
2.3. Kinkéliba Leaf Extract Decreased UVA-Induced Inflammatory Cytokines Production
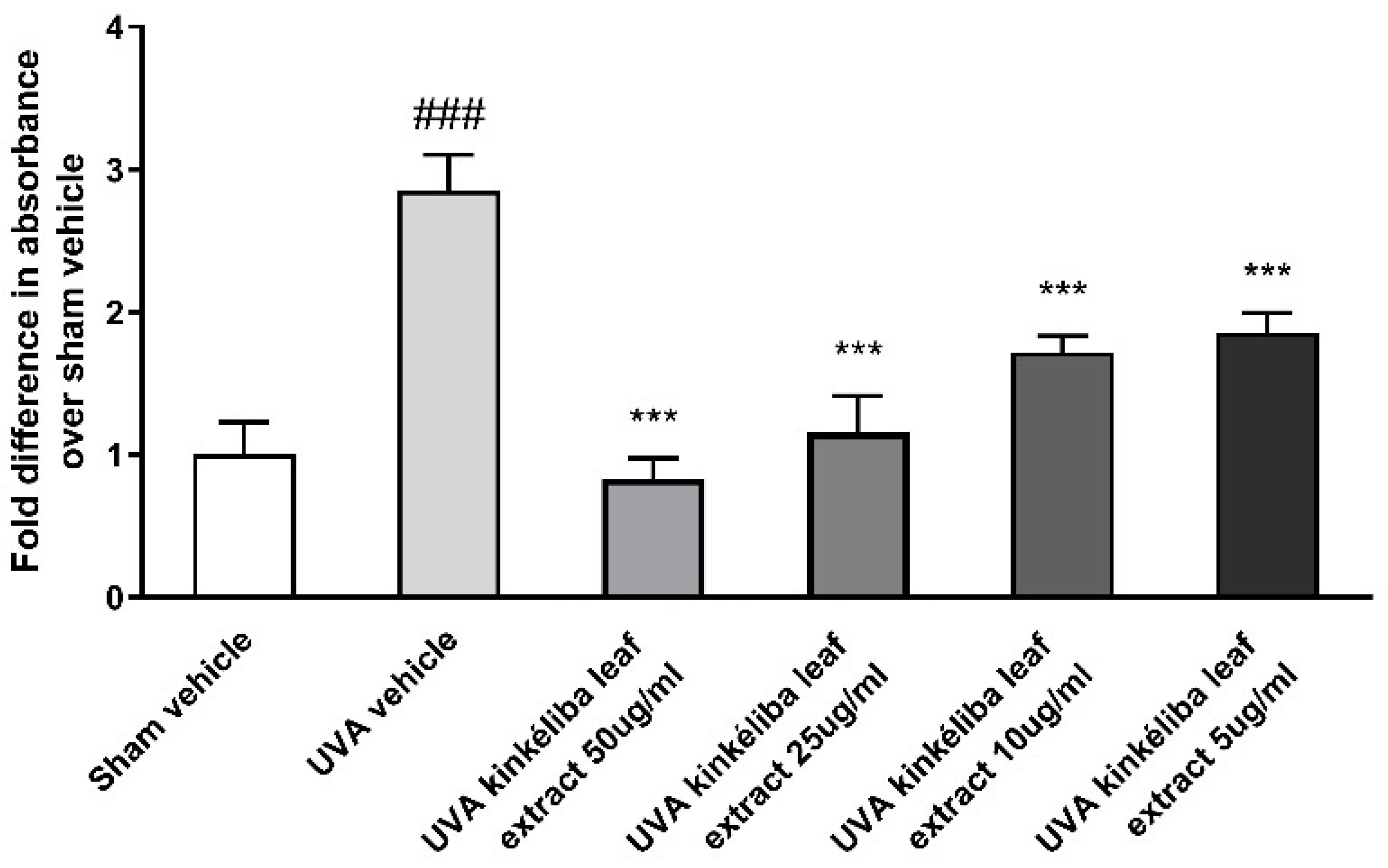
2.4. Kinkéliba Leaf Extract Reduced UVA-Induced ROS Production
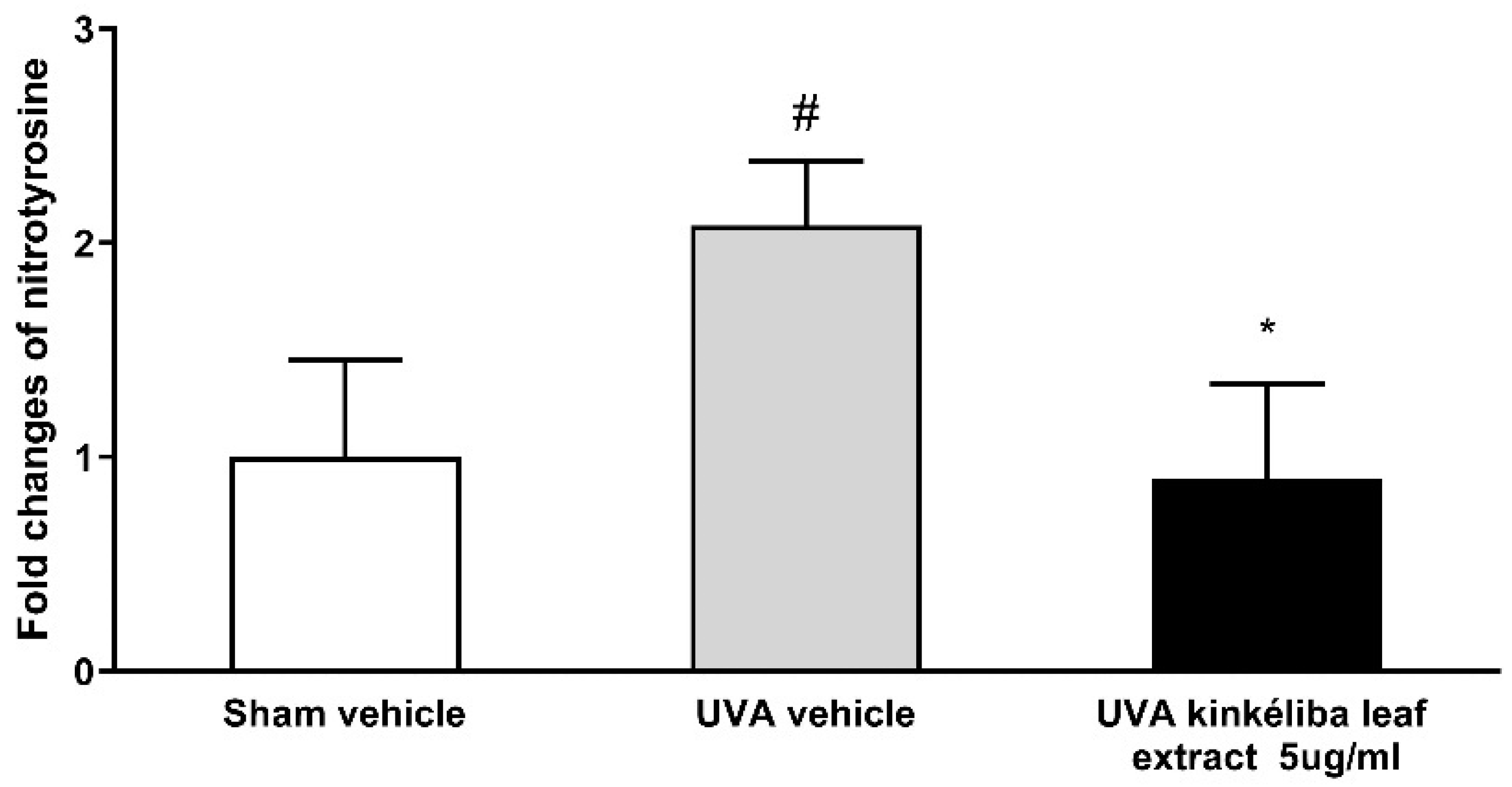
2.5. Kinkéliba Leaf Extract Protected against UVA-Induced Increase in Nitrotyrosine
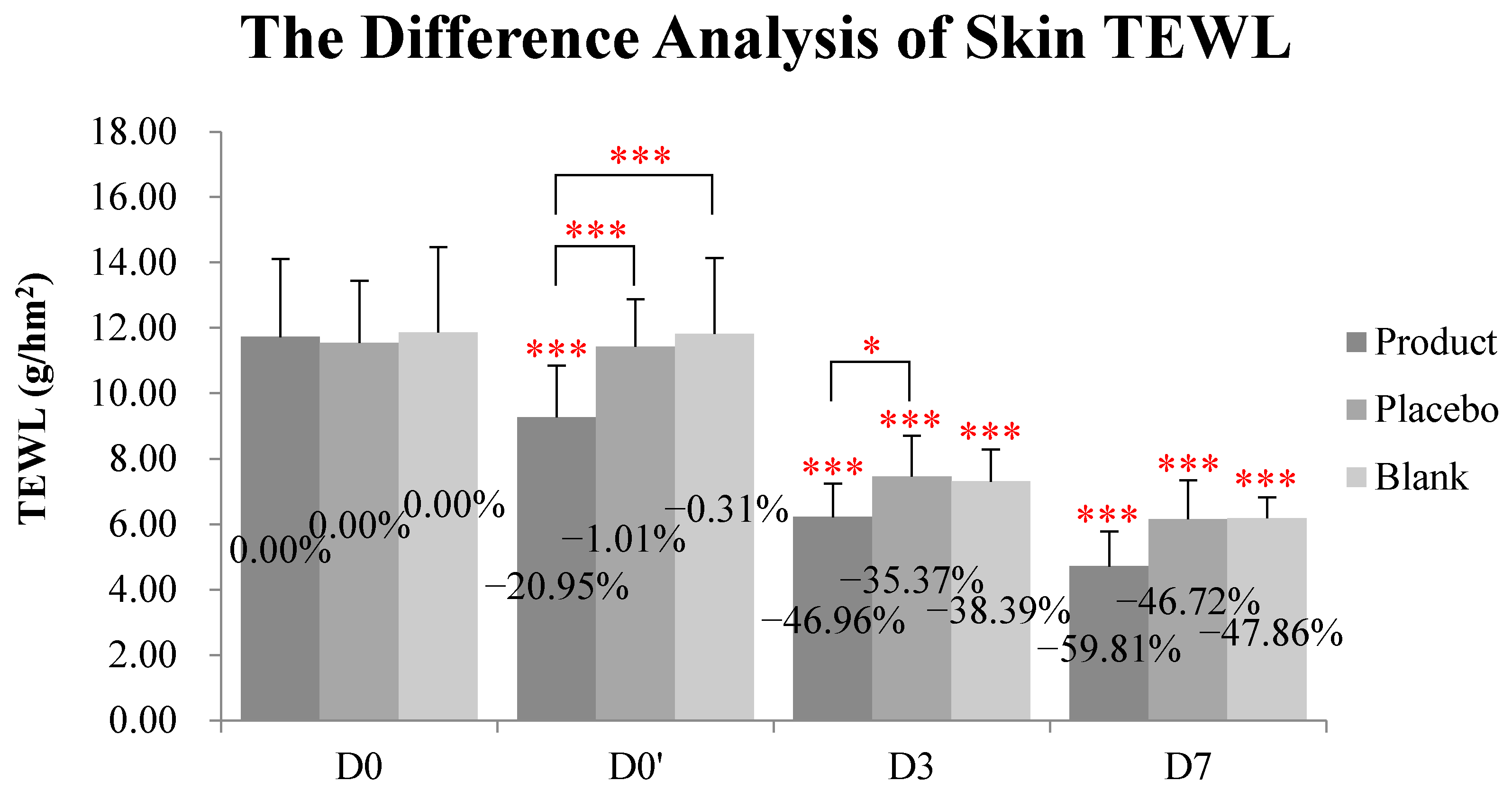
2.6. Kinkéliba Leaf Extract Formula Significantly Reduced Skin TEWL
2.7. Kinkéliba Leaf Extract Formula Reduced SLS-Irritated Erythema
3. Discussion
4. Materials and Methods
4.1. Vitexin and Isovitexin-Rich Kinkéliba Leaf Extract Preparation
4.2. Cell Culture, Kinkéliba Leaf Extract Treatment, and UVA Irradiation
4.3. Cell Viability Measurement
4.4. Measurement of Pro-Inflammatory Cytokines
4.5. Cellular Oxidative Stress (ROS) Measurement
4.6. Measurement of Nitrotyrosine
4.7. In Vivo Study
4.8. Statistical Analysis
5. Conclusions
6. Patents
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Sample Availability
References
- Juliani, H.R.; Koelliker, Y.; Bucuk, M.; Welch, C.; Tepper, B.J.; Jefthas, E.; Simon, J.E. Quality and Consumer Studies in the USA of African Herbal Teas for the Natural Product Industry Development in Sub-Sahara Africa. In African Natural Plant Products: New Discoveries and Challenges in Chemistry and Quality; ACS Publications: Washington, DC, USA, 2009; pp. 403–420. [Google Scholar] [CrossRef]
- Welch, C.R. Chemistry and Pharmacology of Kinkéliba (Combretum micranthum), a West African Medicinal Plant. Ph.D. Thesis, Rutgers, The State University of New Jersey, New Brunswick, NJ, USA, 2010. [Google Scholar]
- Akeem, A.A.; Ejikeme, U.C.; Okarafor, E.U. Antibacterial Potentials of the Ethanolic Extract of the Stem Bark of Combretum micranthum G. Don and Its Fractions. J. Plant Stud. 2012, 1, 75. [Google Scholar] [CrossRef]
- Touré, A.; Xu, X.; Michel, T.; Bangoura, M. In Vitro antioxidant and radical scavenging of Guinean kinkeliba leaf (Combretum micranthum G. Don) extracts. Natural Prod. Res. 2011, 25, 1025–1036. [Google Scholar] [CrossRef] [PubMed]
- Dada, T.; Fall, A.D.; Mbacke, D.S.; Abdou, S.; Lyu, W.; Wu, Q.L.; Simon, J.E.; Bassene, E. Rapid isolation of vitexin from leaves of kinkeliba, Combretum micranthum G. Don. J. Pharmacogn. Phytochem. 2021, 10, 14–16. [Google Scholar]
- Welch, C.; Zhen, J.; Bassène, E.; Raskin, I.; Simon, J.E.; Wu, Q. Bioactive polyphenols in kinkéliba tea (Combretum micranthum) and their glucose-lowering activities. J. Food Drug Anal. 2018, 26, 487–496. [Google Scholar] [CrossRef]
- Zhen, J.; Simon, J.E.; Wu, Q. Total Synthesis of Novel Skeleton Flavan-Alkaloids. Molecules 2020, 25, 4491. [Google Scholar] [CrossRef]
- Wu, Q.L.; Welch, C.; Simon, J.E. Peperidine-Flavan Alkaloid Compounds Derived from African Herb Tea Kinkeliba as Anti-Diabetic Agents. US Patent No. US 8,642,769 B2, 4 February 2014. [Google Scholar]
- Seck, S.M.; Doupa, D.; Dia, D.G.; Diop, E.A.; Ardiet, D.-L.; Nogueira, R.C.; Graz, B.; Diouf, B. Clinical efficacy of African traditional medicines in hypertension: A randomized controlled trial with Combretum micranthum and Hibiscus sabdariffa. J. Hum. Hypertens. 2017, 32, 75–81. [Google Scholar] [CrossRef]
- Kpemissi, M.; Eklu-Gadegbeku, K.; Veerapur, V.P.; Negru, M.; Taulescu, M.; Chandramohan, V.; Hiriyan, J.; Banakar, S.M.; Nv, T.; Suhas, D.S.; et al. Nephroprotective activity of Combretum micranthum G. Don in cisplatin induced nephrotoxicity in rats: In-vitro, in-vivo and in-silico experiments. Biomed. Pharmacother. 2019, 116, 108961. [Google Scholar] [CrossRef]
- Yapo, B.M.; Besson, V.; Beourou, S.; Koffi, K. Optimization of water-extract of phenolic and antioxidant compounds from kinkéliba (Combretum micranthum) leaves. Afr. J. Food Sci. Res. 2014, 2, 37–43. [Google Scholar]
- Zannou, O.; Pashazadeh, H.; Ibrahim, S.A.; Koca, I.; Galanakis, C.M. Green and highly extraction of phenolic compounds and antioxidant capacity from kinkeliba (Combretum micranthum G. Don) by natural deep eutectic solvents (NADESs) using maceration, ultrasound-assisted extraction and homogenate-assisted extraction. Arab. J. Chem. 2022, 15, 103752. [Google Scholar] [CrossRef]
- Kpemissi, M.; Kantati, Y.T.; Veerapur, V.P.; Eklu-Gadegbeku, K.; Hassan, Z. Anti-cholinesterase, anti-inflammatory and antioxidant properties of Combretum micranthum G. Don: Potential implications in neurodegenerative disease. IBRO Neurosci. Rep. 2023, 14, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Kolarsick, P.A.; Kolarsick, M.A.; Goodwin, C. Anatomy and physiology of the skin. J. Dermatol. Nurses Assoc. 2011, 3, 203–213. [Google Scholar] [CrossRef] [Green Version]
- Pilkington, S.M.; Bulfone-Paus, S.; Griffiths, C.E.; Watson, R.E. Inflammaging and the Skin. J. Investig. Dermatol. 2021, 141, 1087–1095. [Google Scholar] [CrossRef] [PubMed]
- Afaq, F.; Katiyar, S.K. Polyphenols: Skin Photoprotection and Inhibition of Photocarcinogenesis. Mini-Rev. Med. Chem. 2011, 11, 1200–1215. [Google Scholar] [CrossRef]
- Farage, M.A.; Miller, K.W.; Elsner, P.; Maibach, H.I. Intrinsic and extrinsic factors in skin ageing: A review. Int. J. Cosmet. Sci. 2008, 30, 87–95. [Google Scholar] [CrossRef]
- Nichols, J.A.; Katiyar, S.K. Skin photoprotection by natural polyphenols: Anti-inflammatory, antioxidant and DNA repair mechanisms. Arch. Dermatol. Res. 2009, 302, 71–83. [Google Scholar] [CrossRef] [PubMed]
- Afaq, F.; Adhami, V.M.; Mukhtar, H. Photochemoprevention of ultraviolet B signaling and photocarcinogenesis. Mutat. Res. Fundam. Mol. Mech. Mutagen. 2005, 571, 153–173. [Google Scholar] [CrossRef]
- Buckman, S.Y.; Gresham, A.; Hale, P.; Hruza, G.; Anast, J.; Masferrer, J.; Pentland, A.P. COX-2 expression is induced by UVB exposure in human skin: Implications for the development of skin cancer. Carcinogenesis 1998, 19, 723–729. [Google Scholar] [CrossRef] [PubMed]
- Furman, D.; Campisi, J.; Verdin, E.; Carrera-Bastos, P.; Targ, S.; Franceschi, C.; Ferrucci, L.; Gilroy, D.W.; Fasano, A.; Miller, G.W.; et al. Chronic inflammation in the etiology of disease across the life span. Nat. Med. 2019, 25, 1822–1832. [Google Scholar] [CrossRef]
- Varani, J.; Perone, P.; Spahlinger, D.M.; Singer, L.M.; Diegel, K.L.; Bobrowski, W.F.; Dunstan, R. Human Skin in Organ Culture and Human Skin Cells (Keratinocytes and Fibroblasts) in Monolayer Culture for Assessment of Chemically Induced Skin Damage. Toxicol. Pathol. 2007, 35, 693–701. [Google Scholar] [CrossRef]
- Baumann, L. Skin ageing and its treatment. J. Pathol. 2007, 211, 241–251. [Google Scholar] [CrossRef]
- Portugal-Cohen, M.; Soroka, Y.; Frušić-Zlotkin, M.; Verkhovsky, L.; Brégégère, F.M.; Neuman, R.; Kohen, R.; Milner, Y. Skin organ culture as a model to study oxidative stress, inflammation and structural alterations associated with UVB-induced photodamage. Exp. Dermatol. 2011, 20, 749–755. [Google Scholar] [CrossRef] [PubMed]
- Beck, L.A.; Cork, M.J.; Amagai, M.; De Benedetto, A.; Kabashima, K.; Hamilton, J.D.; Rossi, A.B. Type 2 Inflammation Contributes to Skin Barrier Dysfunction in Atopic Dermatitis. JID Innov. 2022, 2, 100131. [Google Scholar] [CrossRef] [PubMed]
- Ramos-González, E.; Bitzer-Quintero, O.; Ortiz, G.; Hernández-Cruz, J.; Ramírez-Jirano, L. Relationship between inflammation and oxidative stress and its effect on multiple sclerosis. Neurologia 2021, in press. [Google Scholar] [CrossRef]
- Chatterjee, S. Oxidative stress, inflammation, and disease. In Oxidative Stress and Biomaterials; Elsevier: Amsterdam, The Netherlands, 2016; pp. 35–58. [Google Scholar]
- Bruch-Gerharz, D.; Ruzicka, T.; Kolb-Bachofen, V. Nitric oxide and its implications in skin homeostasis and disease—A review. Arch. Dermatol. Res. 1998, 290, 643–651. [Google Scholar] [CrossRef] [PubMed]
- Brenneisen, P.; Sies, H.; Scharffetter-Kochanek, K. Ultraviolet-B irradiation and matrix metalloproteinases: From induction via signaling to initial events. Ann. N. Y. Acad. Sci. 2002, 973, 31–43. [Google Scholar] [CrossRef]
- Hu, S.; Chen, F.; Wang, M. Photoprotective effects of oxyresveratrol and kuwanon O on DNA damage induced by UVA in human epidermal keratinocytes. Chem. Res. Toxicol. 2015, 28, 541–548. [Google Scholar] [CrossRef]
- National Weather Service. Available online: https://www.cpc.ncep.noaa.gov/products/stratosphere/uv_index/gif_files/lax_17.png (accessed on 1 January 2017).
- Hong Kong Observatory. Average and Range of Daily Maximum UVA Radiation Intensity in Different Months. Available online: https://www.hko.gov.hk/en/wxinfo/uvinfo/uvinfo.html (accessed on 1 January 2010).
- The Bureau of Meteorology. Available online: http://www.bom.gov.au/metadata/catalogue/19115/ANZCW0503900371#distribution-information (accessed on 1 January 2017).
- Meteorological Service Singapore. Available online: http://www.weather.gov.sg/home/ (accessed on 1 January 2022).
- de Jager, T.L.; Cockrell, A.E.; Du Plessis, S.S. Ultraviolet Light Induced Generation of Reactive Oxygen Species. In Ultraviolet Light in Human Health, Diseases and Environment; Springer: Cham, Switzerland, 2017; Volume 996, pp. 15–23. [Google Scholar] [CrossRef]
- Hu, S.; Zhang, X.; Chen, F.; Wang, M. Dietary polyphenols as photoprotective agents against UV radiation. J. Funct. Foods 2017, 30, 108–118. [Google Scholar] [CrossRef]
- Urbanski, A.; Schwarz, T.; Neuner, P.; Krutmann, J.; Kirnbauer, R.; Luger, T.A.; Köck, A. Ultraviolet Light Induces Increased Circulating Interleukin-6 in Humans. J. Investig. Dermatol. 1990, 94, 808–811. [Google Scholar] [CrossRef] [PubMed]
- Sugawara, T.; Gallucci, R.; Simeonova, P.P.; Luster, M.I. Regulation and Role of Interleukin 6 in Wounded Human Epithelial Keratinocytes. Cytokine 2001, 15, 328–336. [Google Scholar] [CrossRef]
- Gutowska-Owsiak, D.; Podobas, E.I.; Eggeling, C.; Ogg, G.S.; de la Serna, J.B. Addressing Differentiation in Live Human Keratinocytes by Assessment of Membrane Packing Order. Front. Cell Dev. Biol. 2020, 8, 573230. [Google Scholar] [CrossRef] [PubMed]
- Bashir, M.; Sharma, M.; Werth, V. TNF-α production in the skin. Arch. Dermatol. Res. 2009, 301, 87–91. [Google Scholar] [CrossRef] [PubMed]
- Han, Y.; Tuan, T.; Wu, H.; Hughes, M.; Garner, W. TNF-alpha stimulates activation of pro-MMP2 in human skin through NF-(kappa)B mediated induction of MT1-MMP. J. Cell Sci. 2001, 114, 131–139. [Google Scholar] [CrossRef]
- Kondo, S.; Kono, T.; Sauder, D.N.; McKenzie, R.C. IL-8 Gene Expression and Production in Human Keratinocytes and Their Modulation by UVB. J. Investig. Dermatol. 1993, 101, 690–694. [Google Scholar] [CrossRef]
- Murata, S.; Kaneko, S.; Morita, E. Interleukin-8 Levels in the Stratum Corneum as a Biomarker for Monitoring Therapeutic Effect in Atopic Dermatitis Patients. Int. Arch. Allergy Immunol. 2021, 182, 592–606. [Google Scholar] [CrossRef] [PubMed]
- Berardesca, E.; Fideli, D.; Borroni, G.; Rabbiosi, G.; Maibach, H. In Vivo hydration and water-retention capacity of stratum corneum in clinically uninvolved skin in atopic and psoriatic patients. Acta Derm.-Venereol. 1990, 70, 400–404. [Google Scholar]
- Orsmond, A.; Bereza-Malcolm, L.; Lynch, T.; March, L.; Xue, M. Skin barrier dysregulation in psoriasis. Int. J. Mol. Sci. 2021, 22, 10841. [Google Scholar] [CrossRef]
- Mittal, M.; Siddiqui, M.R.; Tran, K.; Reddy, S.P.; Malik, A.B. Reactive Oxygen Species in Inflammation and Tissue Injury. Antioxid. Redox Signal. 2014, 20, 1126–1167. [Google Scholar] [CrossRef] [PubMed]
- Martemucci, G.; Costagliola, C.; Mariano, M.; D’Andrea, L.; Napolitano, P.; D’Alessandro, A.G. Free Radical Properties, Source and Targets, Antioxidant Consumption and Health. Oxygen 2022, 2, 48–78. [Google Scholar] [CrossRef]
- Nakai, K.; Tsuruta, D. What are reactive oxygen species, free radicals, and oxidative stress in skin diseases? Int. J. Mol. Sci. 2021, 22, 10799. [Google Scholar] [CrossRef]
- Svobodová, A.; Psotová, J.; Walterová, D. Natural phenolics in the prevention of UV-induced skin damage. A review. Biomed. Pap. 2003, 147, 137–145. [Google Scholar] [CrossRef]
- Martínez, M.C.; Andriantsitohaina, R. Reactive Nitrogen Species: Molecular Mechanisms and Potential Significance in Health and Disease. Antioxid. Redox Signal. 2009, 11, 669–702. [Google Scholar] [CrossRef] [PubMed]
- Daniela, B.-G.; Thomas, R.; Kolb-Bachofen, V. Nitric Oxide in Human Skin: Current Status and Future Prospects. J. Investig. Dermatol. 1998, 110, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, T.; Inukai, M. Effects of Nitrite and Nitrate on DNA Damage Induced by Ultraviolet Light. Chem. Res. Toxicol. 2006, 19, 457–462. [Google Scholar] [CrossRef]
- Aitken, G.R.; Henderson, J.R.; Chang, S.-C.; McNeil, C.J.; Birch-Machin, M.A. Direct monitoring of UV-induced free radical generation in HaCaT keratinocytes. Clin. Exp. Dermatol. 2007, 32, 722–727. [Google Scholar] [CrossRef] [PubMed]
- Garthwaite, J.; Boulton, C.L. Nitric Oxide Signaling in the Central Nervous System. Annu. Rev. Physiol. 1995, 57, 683–706. [Google Scholar] [CrossRef] [PubMed]
- ter Steege, J.C.; Koster-Kamphuis, L.; van Straaten, E.A.; Forget, P.P.; Buurman, W.A. Nitrotyrosine in plasma of celiac disease patients as detected by a new sandwich ELISA. Free. Radic. Biol. Med. 1998, 25, 953–963. [Google Scholar] [CrossRef]
- Ding, W.; Hudson, L.G.; Liu, K.J. Inorganic arsenic compounds cause oxidative damage to DNA and protein by inducing ROS and RNS generation in human keratinocytes. Mol. Cell. Biochem. 2005, 279, 105–112. [Google Scholar] [CrossRef]
- Sequeira, V.B.; Rybchyn, M.S.; Gordon-Thomson, C.; Tongkao-On, W.; Mizwicki, M.T.; Norman, A.W.; Reeve, V.E.; Halliday, G.M.; Mason, R.S. Opening of chloride channels by 1α, 25-dihydroxyvitamin D3 contributes to photoprotection against UVR-induced thymine dimers in keratinocytes. J. Investig. Dermatol. 2013, 133, 776–782. [Google Scholar] [CrossRef]
- De Fine Olivarious, F.; Agner, T.; Menne, T. Skin barrier function and dermal inflammation. An experimental study of transepidermal water loss after dermal tuberculin injection compared with SLS patch testing. Brit. J. Dermatol. 1993, 129, 554–557. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Skin TEWL (g/hm2) | Test Product Group | Placebo Control Group | Blank Control Group | p (Inter-Group) | ||
|---|---|---|---|---|---|---|
| Product vs. Placebo | Product vs. Blank | Placebo vs. Blank | ||||
| D0 baseline | 11.73 ± 2.39 | 11.54 ± 1.90 | 11.86 ± 2.61 | |||
| D0′ | 9.27 ± 1.59 | 11.43 ± 1.46 | 11.82 ± 2.32 | |||
| D3 | 6.22 ± 1.03 | 7.46 ± 1.25 | 7.31 ± 0.98 | |||
| D7 | 4.71 ± 1.07 | 6.15 ± 1.20 | 6.18 ± 0.64 | |||
| p (D0′ vs. D0) | <0.001 | 0.697 | 0.832 | <0.001 | <0.001 | 0.814 |
| p (D3 vs. D0) | <0.001 | <0.001 | <0.001 | 0.042 | 0.294 | 0.550 |
| p (D7 vs. D0) | <0.001 | <0.001 | <0.001 | 0.099 | 0.286 | 0.782 |
| Skin a* Value | Test Product Group | Placebo Control Group | Blank Control Group | p (Inter-Group) | ||
|---|---|---|---|---|---|---|
| Product vs. Placebo | Product vs. Blank | Placebo vs. Blank | ||||
| D0 baseline | 7.11 ± 1.01 | 6.87 ± 0.95 | 6.94 ± 1.12 | |||
| D0′ | 6.81 ± 1.10 | 6.70 ± 0.79 | 7.13 ± 1.00 | |||
| D3 | 6.35 ± 1.14 | 6.19 ± 0.70 | 6.61 ± 0.92 | |||
| D7 | 5.52 ± 1.11 | 5.69 ± 0.88 | 5.98 ± 1.18 | |||
| p (D0′ vs. D0) | 0.006 | 0.039 | 0.129 | 0.243 | 0.003 | 0.016 |
| p (D3 vs. D0) | 0.004 | 0.016 | 0.167 | 0.770 | 0.149 | 0.280 |
| p (D7 vs. D0) | <0.001 | 0.004 | <0.001 | 0.268 | 0.028 | 0.549 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hu, S.; Simon, J.E.; Wang, M.; Wu, Y.; Huang, Y.; Wu, Q. Kinkéliba (Combretum micranthum) Leaf Extract Alleviates Skin Inflammation: In Vitro and In Vivo Study. Molecules 2023, 28, 1791. https://doi.org/10.3390/molecules28041791
Hu S, Simon JE, Wang M, Wu Y, Huang Y, Wu Q. Kinkéliba (Combretum micranthum) Leaf Extract Alleviates Skin Inflammation: In Vitro and In Vivo Study. Molecules. 2023; 28(4):1791. https://doi.org/10.3390/molecules28041791
Chicago/Turabian StyleHu, Shuting, James E. Simon, Mingfu Wang, Yizhen Wu, Yumin Huang, and Qingli Wu. 2023. "Kinkéliba (Combretum micranthum) Leaf Extract Alleviates Skin Inflammation: In Vitro and In Vivo Study" Molecules 28, no. 4: 1791. https://doi.org/10.3390/molecules28041791