
Local Delivery of Azithromycin Nanoformulation Attenuated Acute Lung Injury in Mice

 , and
, and 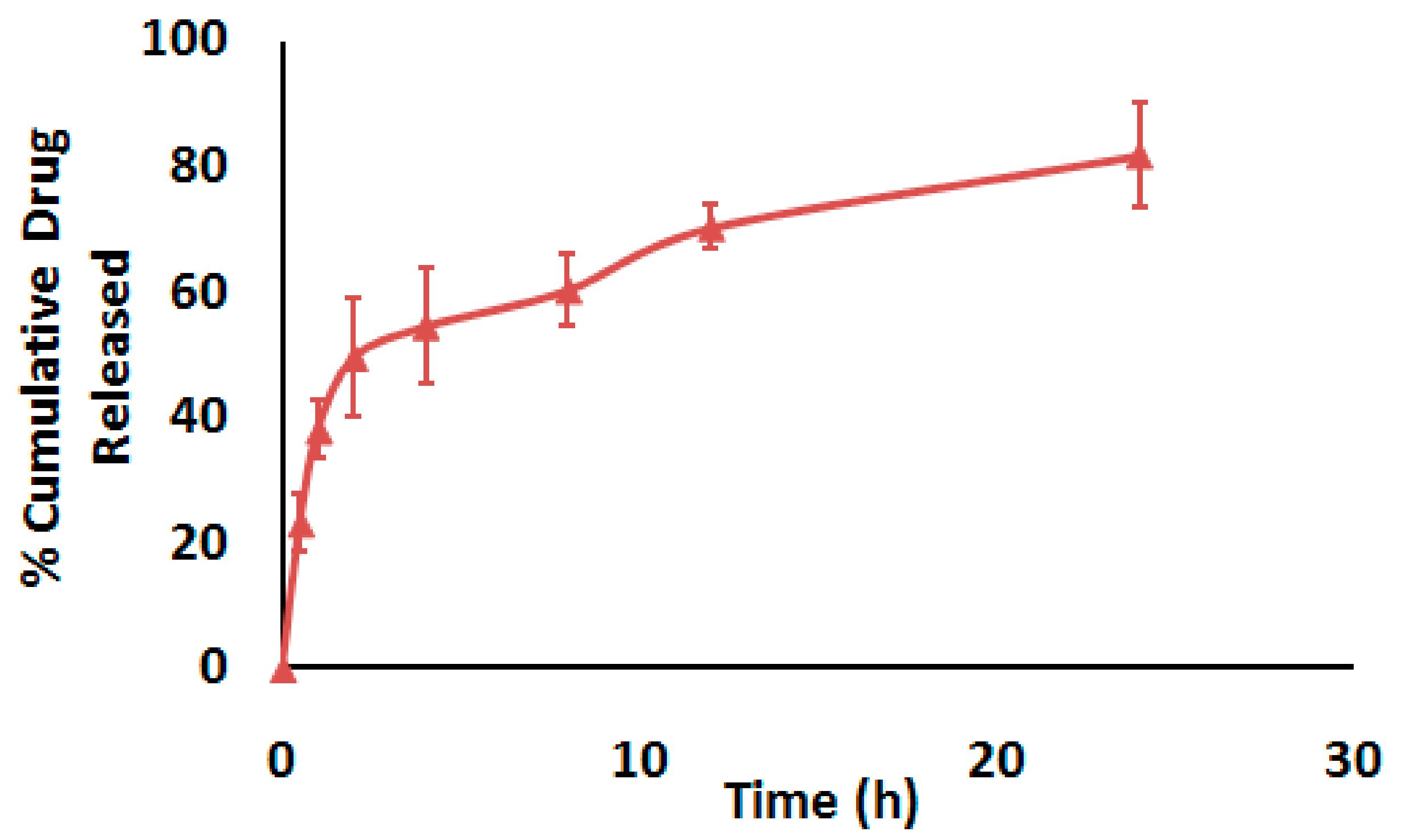{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Results
2.1. In Vitro Characterization of AZ-NLC
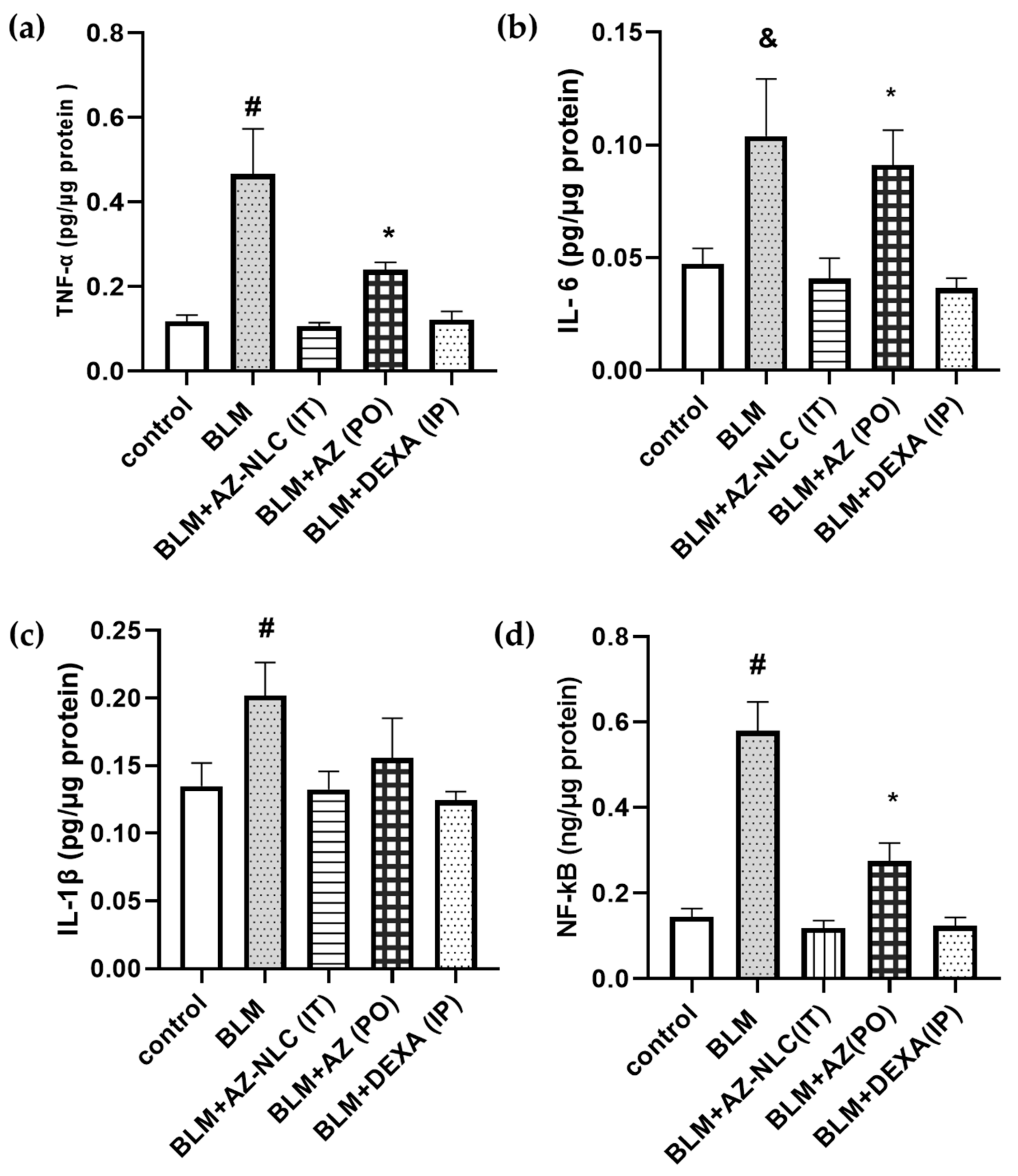
2.2. In Vivo Pro-Inflammatory Markers Evaluation
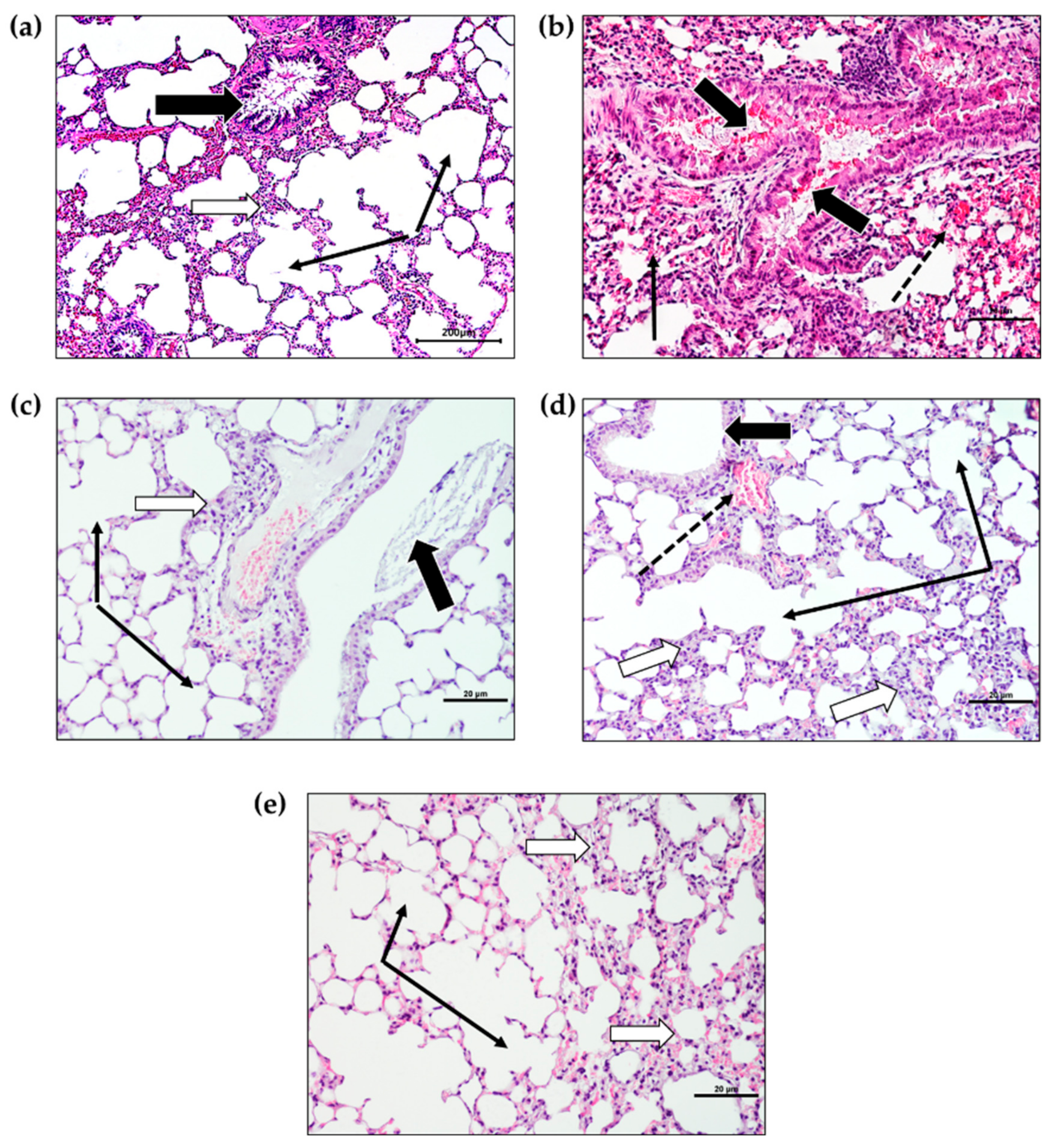
2.3. Histopathological Changes
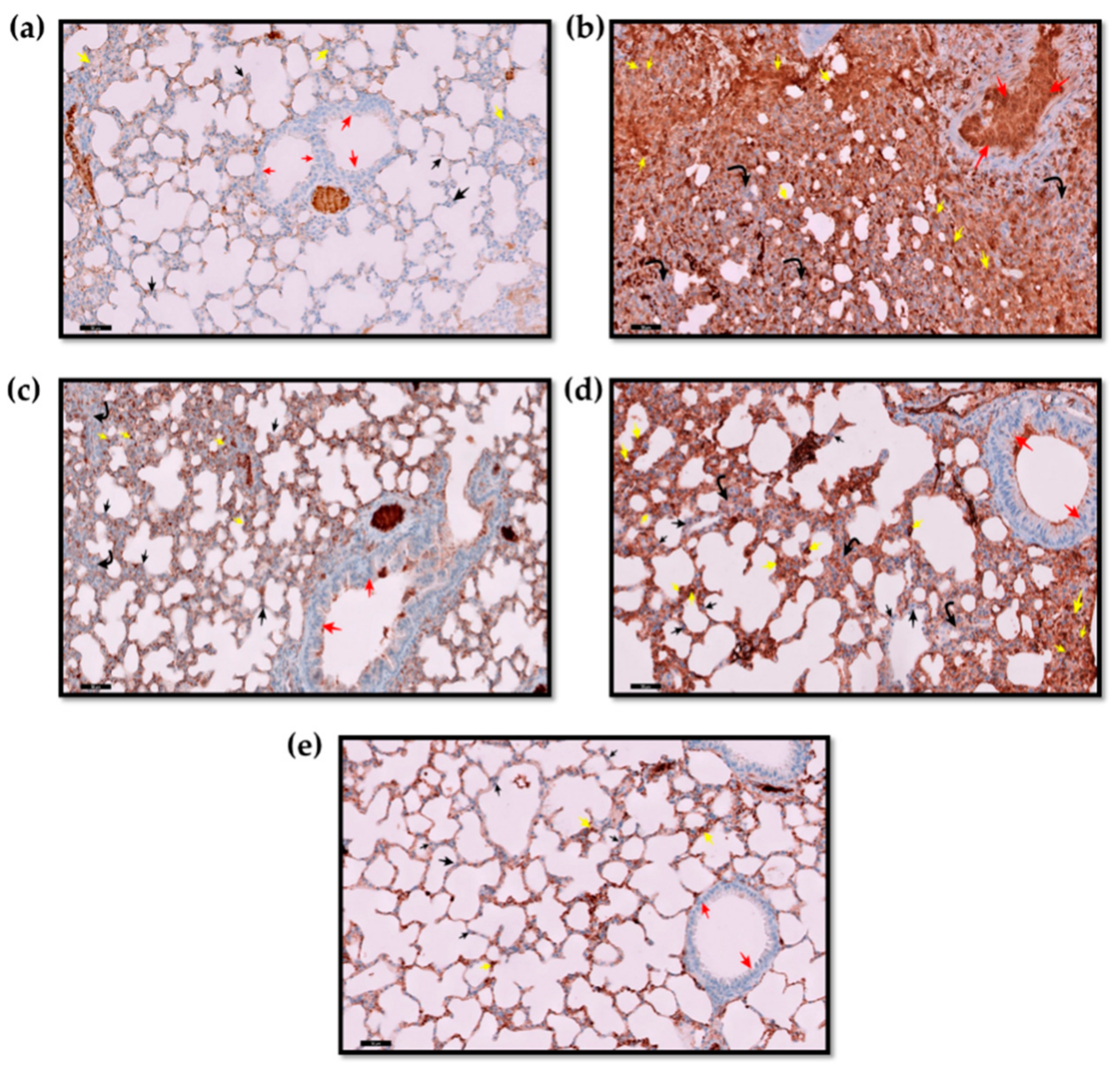
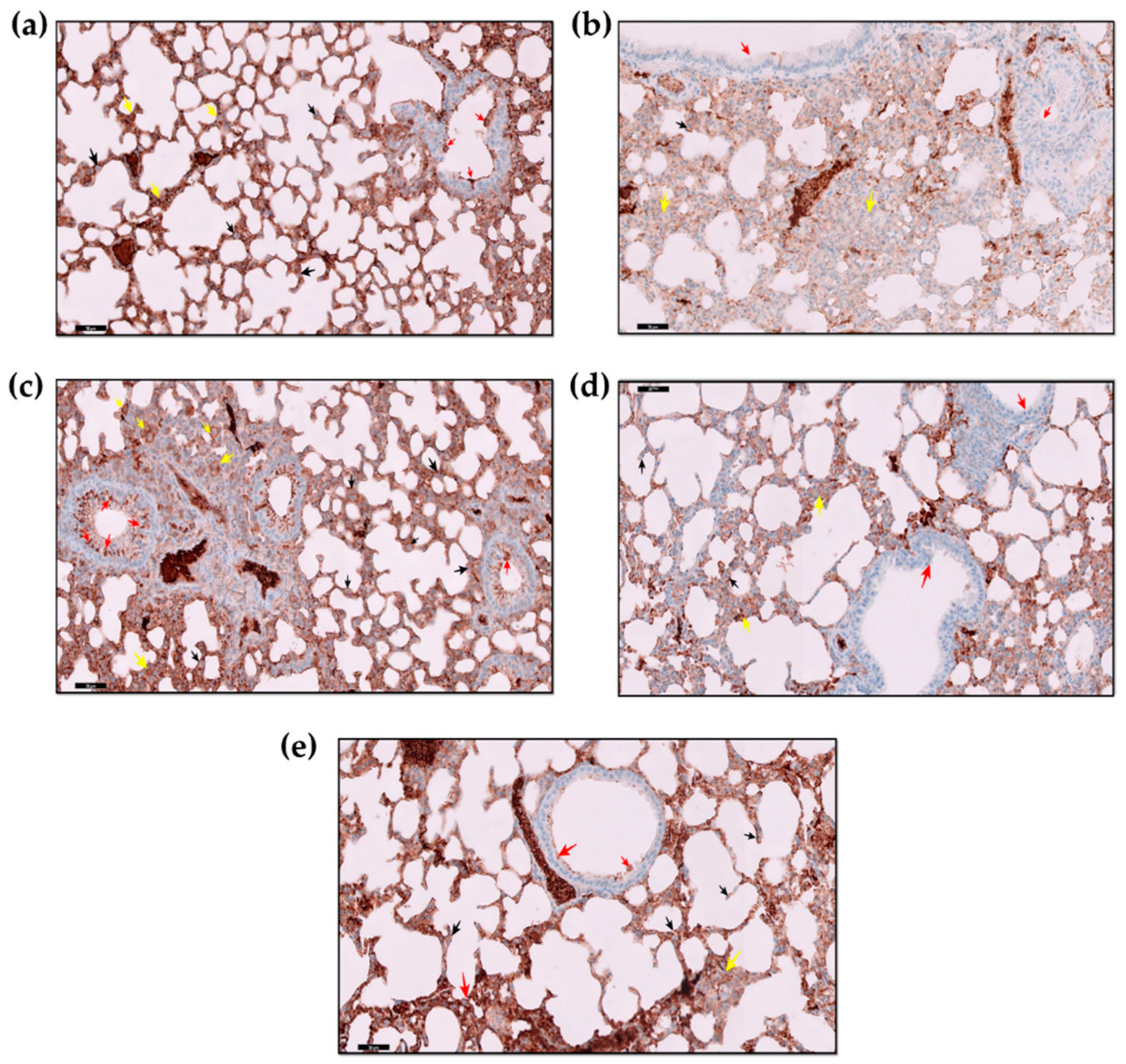
2.4. Immunohistochemistry Findings
3. Discussion
4. Materials and Methods
4.1. Materials
4.2. Preparation of AZ-NLC
4.3. Characterization of AZ-NLC
4.3.1. Particle Size, PDI, and Zeta Potential
4.3.2. In Vitro Drug Release Evaluation
4.4. In Vivo Experiments
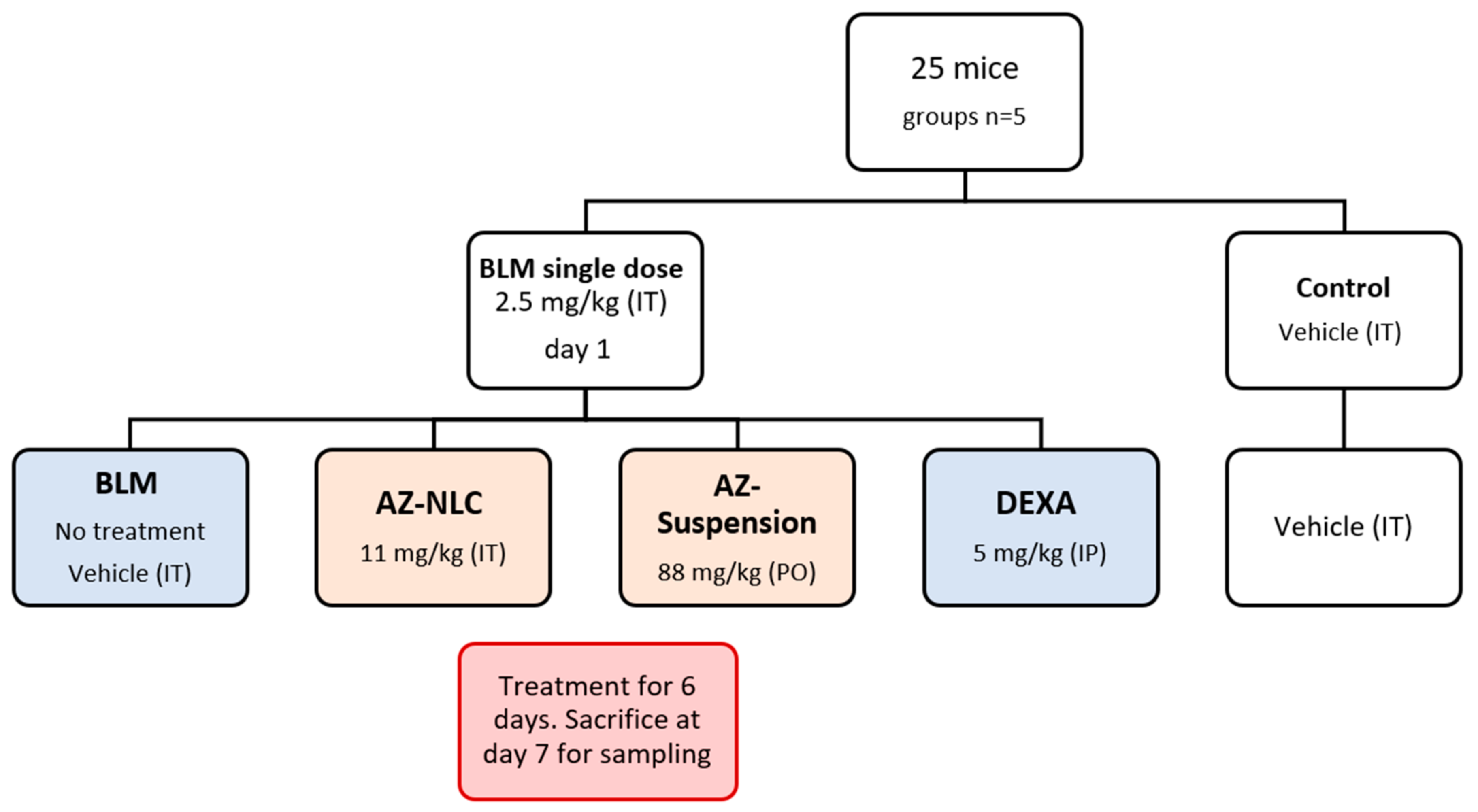
4.4.1. Animals and the Experimental Study Design
4.4.2. Pro-Inflammatory Markers Analysis
4.4.3. Preparation of Tissue Homogenate
4.4.4. Histopathological Evaluation
4.4.5. Immunohistochemical Evaluation
4.5. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mathieu, E.; Ritchie, H.; Rodés-Guirao, L.; Appel, C.; Giattino, C.; Ortiz-Ospina, E.; Hasell, J.; Macdonald, B.; Beltekian, D.; Roser, M. Coronavirus Pandemic (COVID-19). Our World in Data. 2020. Available online: https://ourworldindata.org/coronavirus (accessed on 20 October 2022).
- Nalbandian, A.; Sehgal, K.; Gupta, A.; Madhavan, M.V.; McGroder, C.; Stevens, J.S.; Cook, J.R.; Nordvig, A.S.; Shalev, D.; Sehrawat, T.S. Post-acute COVID-19 syndrome. Nat. Med. 2021, 27, 601–615. [Google Scholar] [CrossRef] [PubMed]
- Yüce, M.; Filiztekin, E.; Özkaya, K.G. COVID-19 diagnosis—A review of current methods. Biosens. Bioelectron. 2021, 172, 112752. [Google Scholar] [CrossRef] [PubMed]
- WHO Coronavirus. Dashboard| WHO Coronavirus (COVID-19) Dashboard with Vaccination Datahttps, COVID19. Who. Int. Available online: https://covid19.who.int/ (accessed on 16 November 2022).
- Gbinigie, K.; Frie, K. Should azithromycin be used to treat COVID-19? A rapid review. BJGP Open 2020, 4, bjgpopen20X101094. [Google Scholar] [CrossRef] [PubMed]
- Touret, F.; Gilles, M.; Barral, K.; Nougairède, A.; van Helden, J.; Decroly, E.; de Lamballerie, X.; Coutard, B. In vitro screening of an FDA-approved chemical library reveals potential inhibitors of SARS-CoV-2 replication. Sci. Rep. 2020, 10, 13093. [Google Scholar] [CrossRef] [PubMed]
- Kamel, A.M.; Monem, M.S.; Sharaf, N.A.; Magdy, N.; Farid, S.F. Efficacy and safety of azithromycin in COVID-19 patients: A systematic review and meta-analysis of randomized clinical trials. Rev. Med. Virol. 2022, 32, e2258. [Google Scholar] [CrossRef] [PubMed]
- Mangkuliguna, G.; Pramono, L.A. Efficacy and Safety of Azithromycin for the Treatment of COVID-19: A Systematic Review and Meta-analysis. Tuberc. Respir. Dis. 2021, 84, 299. [Google Scholar] [CrossRef]
- Damle, B.; Vourvahis, M.; Wang, E.; Leaney, J.; Corrigan, B. Clinical Pharmacology Perspectives on the Antiviral Activity of Azithromycin and Use in COVID-19. Clin. Pharmacol. Ther. 2020, 108, 201–211. [Google Scholar] [CrossRef] [PubMed]
- Southern, K.W.; Barker, P.M.; Solis-Moya, A.; Patel, L. Macrolide antibiotics for cystic fibrosis. Cochrane Database Syst. Rev. 2012. [Google Scholar] [CrossRef] [PubMed]
- Hahn, D.L. Azithromycin for prevention of exacerbations of COPD. N. Engl. J. Med. 2011, 365, 2236, author reply 2236–2237. [Google Scholar] [PubMed]
- Vos, R.; Vanaudenaerde, B.M.; Verleden, S.E.; De Vleeschauwer, S.I.; Willems-Widyastuti, A.; Van Raemdonck, D.E.; Schoonis, A.; Nawrot, T.S.; Dupont, L.J.; Verleden, G.M. A randomized controlled trial of azithromycin to prevent chronic rejection after lung transplantation. Eur. Respir. J. 2011, 37, 164. [Google Scholar] [CrossRef] [PubMed]
- Nunes, C.R.; Procianoy, R.S.; Corso, A.L.; Silveira, R.C. Use of Azithromycin for the Prevention of Lung Injury in Mechanically Ventilated Preterm Neonates: A Randomized Controlled Trial. Neonatology 2020, 117, 522–528. [Google Scholar] [CrossRef]
- Bleyzac, N.; Goutelle, S.; Bourguignon, L.; Tod, M. Azithromycin for COVID-19: More than just an antimicrobial? Clin. Drug Investig. 2020, 40, 683–686. [Google Scholar] [CrossRef] [PubMed]
- Hughes, J.H.; Sweeney, K.; Ahadieh, S.; Ouellet, D. Predictions of Systemic, Intracellular, and Lung Concentrations of Azithromycin with Different Dosing Regimens used in COVID-19 Clinical Trials. CPT Pharm. Syst. Pharmacol. 2020, 9, 435–443. [Google Scholar] [CrossRef]
- Echeverría-Esnal, D.; Martin-Ontiyuelo, C.; Navarrete-Rouco, M.E.; De-Antonio Cusco, M.; Ferrández, O.; Horcajada, J.P.; Grau, S. Azithromycin in the treatment of COVID-19: A review. Expert Rev. Anti-Infect. Ther. 2021, 19, 147–163. [Google Scholar] [CrossRef] [PubMed]
- Indari, O.; Jakhmola, S.; Manivannan, E.; Jha, H.C. An update on antiviral therapy against SARS-CoV-2: How far have we come? Front. Pharmacol. 2021, 12, 133. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Wang, X.; Lin, X.; Liu, X.; Tian, B.; Tang, X. High azithromycin loading powders for inhalation and their in vivo evaluation in rats. Int. J. Pharm. 2010, 395, 205–214. [Google Scholar] [CrossRef] [PubMed]
- Mangal, S.; Nie, H.; Xu, R.; Guo, R.; Cavallaro, A.; Zemlyanov, D.; Zhou, Q.T. Physico-chemical properties, aerosolization and dissolution of co-spray dried azithromycin particles with l-leucine for inhalation. Pharm. Res. 2018, 35, 28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, X.; Vogt, F.G.; Hayes, D., Jr.; Mansour, H.M. Physicochemical characterization and aerosol dispersion performance of organic solution advanced spray-dried microparticulate/nanoparticulate antibiotic dry powders of tobramycin and azithromycin for pulmonary inhalation aerosol delivery. Eur. J. Pharm. Sci. 2014, 52, 191–205. [Google Scholar] [CrossRef]
- Siekmeier, R.; Hofmann, T.; Scheuch, G. Inhalation of macrolides: A novel approach to treatment of pulmonary infections. In Inflammatory Disorders; Springer: Zurich, Switzerland, 2014; pp. 13–24. [Google Scholar]
- Ali, M. Pulmonary drug delivery. In Handbook of Non-Invasive Drug Delivery Systems; Elsevier: Amsterdam, The Netherlands, 2010; pp. 209–246. [Google Scholar]
- Campos, E.V.; Pereira, A.E.; De Oliveira, J.L.; Carvalho, L.B.; Guilger-Casagrande, M.; De Lima, R.; Fraceto, L.F. How can nanotechnology help to combat COVID-19? Opportunities and urgent need. J. Nanobiotechnol. 2020, 18, 125. [Google Scholar] [CrossRef] [PubMed]
- Bhutta, Z.A.; Kanwal, A.; Ali, M.; Kulyar, M.F.-E.-A.; Yao, W.; Shoaib, M.; Ashar, A.; Mahfooz, A.; Ijaz, M.; Ijaz, N. Emerging nanotechnology role in the development of innovative solutions against COVID-19 pandemic. Nanotechnology 2021, 32, 482001. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, A.P.A.; Conte-Junior, C.A. Recent advances on nanomaterials to COVID-19 management: A systematic review on antiviral/virucidal agents and mechanisms of SARS-CoV-2 inhibition/inactivation. Glob. Chall. 2021, 5, 2000115. [Google Scholar] [CrossRef] [PubMed]
- Singh, L.; Kruger, H.G.; Maguire, G.E.; Govender, T.; Parboosing, R. The role of nanotechnology in the treatment of viral infections. Ther. Adv. Infect. Dis. 2017, 4, 105–131. [Google Scholar] [CrossRef] [PubMed]
- Ghasemiyeh, P.; Mohammadi-Samani, S. Solid lipid nanoparticles and nanostructured lipid carriers as novel drug delivery systems: Applications, advantages and disadvantages. Res. Pharm. Sci. 2018, 13, 288. [Google Scholar] [PubMed]
- Ali, A.S.; ASattar, M.A.; Karim, S.; Kutbi, D.; Aljohani, H.; Bakhshwin, D.; Alsieni, M.; Alkreathy, H.M. Pharmacological basis for the potential role of Azithromycin and Doxycycline in management of COVID-19. Arab. J. Chem. 2021, 14, 102983. [Google Scholar] [CrossRef] [PubMed]
- Alipoor, S.D.; Jamaati, H.; Tabarsi, P.; Mortaz, E. Immunopathogenesis of Pneumonia in COVID-19. Tanaffos 2020, 19, 79–82. [Google Scholar] [PubMed]
- Parvathaneni, V.; Kulkarni, N.S.; Muth, A.; Kunda, N.K.; Gupta, V. Therapeutic potential of inhalable medications to combat coronavirus disease-2019. Ther. Deliv. 2021, 12, 105–110. [Google Scholar] [CrossRef] [PubMed]
- Alrashedi, M.G.; Alrashedi, A.G.; Ali, A.S.; Ibrahim, I.M. Lung Delivery Systems to Optimize Pharmacotherapy of COVID-19: A Concise Review. Lung 2021, 33, 268–277. [Google Scholar] [CrossRef]
- Patil, T.S.; Deshpande, A.S. Nanostructured lipid carriers-based drug delivery for treating various lung diseases: A state-of-the-art review. Int. J. Pharm. 2018, 547, 209–225. [Google Scholar] [CrossRef] [PubMed]
- Fahmy, U.A.; Ahmed, O.A.; Badr-Eldin, S.M.; Aldawsari, H.M.; Okbazghi, S.Z.; Awan, Z.A.; Bakhrebah, M.A.; Alomary, M.N.; Abdulaal, W.H.; Medina, C. Optimized nanostructured lipid carriers integrated into in situ nasal gel for enhancing brain delivery of flibanserin. Int. J. Nanomed. 2020, 15, 5253. [Google Scholar] [CrossRef]
- Pinto, F.; de Barros, D.P.; Fonseca, L.P. Design of multifunctional nanostructured lipid carriers enriched with α-tocopherol using vegetable oils. Ind. Crops Prod. 2018, 118, 149–159. [Google Scholar] [CrossRef]
- Bashiri, S.; Ghanbarzadeh, B.; Ayaseh, A.; Dehghannya, J.; Ehsani, A.; Ozyurt, H. Essential oil-loaded nanostructured lipid carriers: The effects of liquid lipid type on the physicochemical properties in beverage models. Food Biosci. 2020, 35, 100526. [Google Scholar] [CrossRef]
- Zardini, A.A.; Mohebbi, M.; Farhoosh, R.; Bolurian, S. Production and characterization of nanostructured lipid carriers and solid lipid nanoparticles containing lycopene for food fortification. J. Food Sci. Technol. 2018, 55, 287–298. [Google Scholar] [CrossRef]
- Prabha, S.; Arya, G.; Chandra, R.; Ahmed, B.; Nimesh, S. Effect of size on biological properties of nanoparticles employed in gene delivery. Artif. Cells Nanomed. Biotechnol. 2016, 44, 83–91. [Google Scholar] [CrossRef]
- Caputo, F.; Clogston, J.; Calzolai, L.; Rösslein, M.; Prina-Mello, A. Measuring particle size distribution of nanoparticle enabled medicinal products, the joint view of EUNCL and NCI-NCL. A step by step approach combining orthogonal measurements with increasing complexity. J. Control Release 2019, 299, 31–43. [Google Scholar] [CrossRef] [PubMed]
- Clogston, J.D.; Patri, A.K. Zeta potential measurement. In Characterization of Nanoparticles Intended for Drug Delivery; Springer: Berlin/Heidelberg, Germany, 2011; pp. 63–70. [Google Scholar]
- Salopek, B.; Krasic, D.; Filipovic, S. Measurement and application of zeta-potential. Rud.-Geol.-Naft. Zb. 1992, 4, 147. [Google Scholar]
- Putri, D.C.A.; Dwiastuti, R.; Marchaban, M.; Nugroho, A.K. Optimization of mixing temperature and sonication duration in liposome preparation. J. Pharm. Sci. Commun. 2017, 14, 79–85. [Google Scholar] [CrossRef] [Green Version]
- Danaei, M.; Dehghankhold, M.; Ataei, S.; Hasanzadeh Davarani, F.; Javanmard, R.; Dokhani, A.; Khorasani, S.; Mozafari, M. Impact of particle size and polydispersity index on the clinical applications of lipidic nanocarrier systems. Pharmaceutics 2018, 10, 57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gordillo-Galeano, A.; Mora-Huertas, C.E. Solid lipid nanoparticles and nanostructured lipid carriers: A review emphasizing on particle structure and drug release. Eur. J. Pharm. Biopharm. 2018, 133, 285–308. [Google Scholar] [CrossRef] [PubMed]
- Zheng, J.; Zhang, Y.; Zhang, S. Sustained release of azithromycin from lipid liquid-crystalline nanoparticles laden in situ gel for the treatment of periodontitis: In vitro and efficacy study. J. Biomater. Appl. 2022, 3, 08853282221095395. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, R.G.; Moore, B.B.; Chambers, R.C.; Eickelberg, O.; Königshoff, M.; Kolb, M.; Laurent, G.J.; Nanthakumar, C.B.; Olman, M.A.; Pardo, A. An official American Thoracic Society workshop report: Use of animal models for the preclinical assessment of potential therapies for pulmonary fibrosis. Am. J. Respir. Cell Mol. Biol. 2017, 56, 667–679. [Google Scholar] [CrossRef] [Green Version]
- Jackson, M.R.; Stevenson, K.; Chahal, S.K.; Curley, E.; Finney, G.; Gutierrez-Quintana, R.; Onwubiko, E.; Rupp, A.F.; Strathdee, K.; MacLeod, M.K. Low-dose lung radiotherapy for COVID-19 lung disease: A pre-clinical efficacy study in a bleomycin model of pneumonitis. bioRxiv 2021. [Google Scholar]
- Bordag, N.; Biasin, V.; Schnoegl, D.; Valzano, F.; Jandl, K.; Nagy, B.M.; Sharma, N.; Wygrecka, M.; Kwapiszewska, G.; Marsh, L.M. Machine Learning Analysis of the Bleomycin Mouse Model Reveals the Compartmental and Temporal Inflammatory Pulmonary Fingerprint. Science 2020, 23, 101819. [Google Scholar] [CrossRef] [PubMed]
- Su, X.; Liu, K.; Xie, Y.; Zhang, M.; Wang, Y.; Zhao, M.; Guo, Y.; Zhang, Y.; Wang, J. Protective effect of a polyphenols-rich extract from Inonotus Sanghuang on bleomycin-induced acute lung injury in mice. Life Sci. 2019, 230, 208–217. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.-L.; Wang, J. Dioscin attenuates Bleomycin-Induced acute lung injury via inhibiting the inflammatory response in mice. Exp. Lung Res. 2019, 45, 236–244. [Google Scholar] [CrossRef] [PubMed]
- Moore, B.B.; Hogaboam, C.M. Murine models of pulmonary fibrosis. Am. J. Physiol.-Lung Cell. Mol. Physiol. 2008, 294, L152–L160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Apostolova, E.; Lukova, P.; Baldzhieva, A.; Katsarov, P.; Nikolova, M.; Iliev, I.; Peychev, L.; Trica, B.; Oancea, F.; Delattre, C. Immunomodulatory and anti-inflammatory effects of fucoidan: A review. Polymers 2020, 12, 2338. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Liu, Y.; Peng, X.; Liu, W.; Zhao, F.; Feng, D.; Han, J.; Huang, Y.; Luo, S.; Li, L. NMDA receptor antagonist attenuates bleomycin-induced acute lung injury. PLoS ONE 2015, 10, e0125873. [Google Scholar] [CrossRef] [Green Version]
- Gille, T.; Didier, M.; Rotenberg, C.; Delbrel, E.; Marchant, D.; Sutton, A.; Dard, N.; Haine, L.; Voituron, N.; Bernaudin, J.-F. Intermittent hypoxia increases the severity of bleomycin-induced lung injury in mice. Oxid. Med. Cell. Longev. 2018, 2018, 1240192. [Google Scholar] [CrossRef]
- Strieter, R.M.; Kunkel, S.L.; Bone, R.C. Role of tumor necrosis factor-alpha in disease states and inflammation. Crit. Care Med. 1993, 21, S447–S463. [Google Scholar] [CrossRef]
- Gao, M.; Xie, B.; Gu, C.; Li, H.; Zhang, F.; Yu, Y. Targeting the proinflammatory cytokine tumor necrosis factor-α to alleviate cardiopulmonary bypass-induced lung injury. Mol. Med. Rep. 2015, 11, 2373–2378. [Google Scholar] [CrossRef] [Green Version]
- Yull, F. Manipulation of NF-κB Activity in the Macrophage Lineage as a Novel Therapeutic Approach; Vanderbilt University Medical Center: Nashville, TN, USA, 2008. [Google Scholar]
- Pan, W.; Du, J.; Zhang, L.; Ma, J. The roles of NF-kB in the development of lung injury after one-lung ventilation. Eur. Rev. Med. Pharmacol. Sci. 2018, 22, 7414–7422. [Google Scholar]
- Saito, F.; Tasaka, S.; Inoue, K.-i.; Miyamoto, K.; Nakano, Y.; Ogawa, Y.; Yamada, W.; Shiraishi, Y.; Hasegawa, N.; Fujishima, S. Role of interleukin-6 in bleomycin-induced lung inflammatory changes in mice. Am. J. Respir. Cell Mol. Biol. 2008, 38, 566–571. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, T.; Narazaki, M.; Kishimoto, T. IL-6 in inflammation, immunity, and disease. Cold Spring Harb. Perspect. Biol. 2014, 6, a016295. [Google Scholar] [CrossRef]
- Ratzinger, F.; Haslacher, H.; Poeppl, W.; Hoermann, G.; Kovarik, J.; Jutz, S.; Steinberger, P.; Burgmann, H.; Pickl, W.; Schmetterer, K. Azithromycin suppresses CD4+ T-cell activation by direct modulation of mTOR activity. Sci. Rep. 2014, 4, 7438. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wuyts, W.; Willems, S.; Vos, R.; Vanaudenaerde, B.; De Vleeschauwer, S.; Rinaldi, M.; Vanhooren, H.; Geudens, N.; Verleden, S.; Demedts, M. Azithromycin reduces pulmonary fibrosis in a bleomycin mouse model. Exp. Lung Res. 2010, 36, 602–614. [Google Scholar] [CrossRef]
- Banjanac, M.; Kos, V.M.; Nujić, K.; Vrančić, M.; Belamarić, D.; Crnković, S.; Hlevnjak, M.; Haber, V.E. Anti-inflammatory mechanism of action of azithromycin in LPS-stimulated J774A. 1 cells. Pharmacol. Res. 2012, 66, 357–362. [Google Scholar] [CrossRef]
- Venditto, V.J.; Haydar, D.; Abdel-Latif, A.; Gensel, J.; Anstead, M.I.; Pitts, M.G.; Creameans, J.W.; Kopper, T.J.; Peng, C.; Feola, D.J. Immunomodulatory effects of azithromycin revisited: Potential applications to COVID-19. Front. Immunol. 2021, 12, 285. [Google Scholar] [CrossRef] [PubMed]
- Jang, C.-H.; Choi, J.-H.; Byun, M.-S.; Jue, D.-M. Chloroquine inhibits production of TNF-α, IL-1β and IL-6 from lipopolysaccharide-stimulated human monocytes/macrophages by different modes. Rheumatology 2006, 45, 703–710. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, B.; Li, C.; Chen, P.; Zhou, N.; Wang, L.; Li, J.; Jiang, H.; Wang, D.W. Hydroxychloroquine application is associated with a decreased mortality in critically ill patients with COVID-19. medRxiv 2020. [Google Scholar] [CrossRef]
- Oliver, M.E.; Hinks, T.S. Azithromycin in viral infections. Rev. Med. Virol. 2021, 31, e2163. [Google Scholar] [CrossRef]
- Ornstein, M.H.; Sperber, K. The antiinflammatory and antiviral effects of hydroxychloroquine in two patients with acquired immunodeficiency syndrome and active inflammatory arthritis. Arthritis Rheum. Off. J. Am. Coll. Rheumatol. 1996, 39, 157–161. [Google Scholar] [CrossRef]
- Liu, L.; Ren, J.; He, Z.; Men, K.; Mao, Y.; Ye, T.; Chen, H.; Li, L.; Xu, B.; Wei, Y. Cholesterol-modified hydroxychloroquine-loaded nanocarriers in bleomycin-induced pulmonary fibrosis. Sci. Rep. 2017, 7, 10737. [Google Scholar] [CrossRef] [Green Version]
- Rhee, C.K.; Lee, S.H.; Yoon, H.K.; Kim, S.C.; Lee, S.Y.; Kwon, S.S.; Kim, Y.K.; Kim, K.H.; Kim, T.J.; Kim, J.W. Effect of nilotinib on bleomycin-induced acute lung injury and pulmonary fibrosis in mice. Respiration 2011, 82, 273–287. [Google Scholar] [CrossRef] [PubMed]
- Shen, H.; Wu, N.; Wang, Y.; Zhao, H.; Zhang, L.; Li, T.; Zhao, M. Chloroquine attenuates paraquat-induced lung injury in mice by altering inflammation, oxidative stress and fibrosis. Int. Immunopharmacol. 2017, 46, 16–22. [Google Scholar] [CrossRef] [PubMed]
- Ruan, H.; Gao, S.; Li, S.; Luan, J.; Jiang, Q.; Li, X.; Yin, H.; Zhou, H.; Yang, C. Deglycosylated Azithromycin Attenuates Bleomycin-Induced Pulmonary Fibrosis via the TGF-β1 Signaling Pathway. Molecules 2021, 26, 2820. [Google Scholar] [CrossRef]
- Elmore, S. Apoptosis: A review of programmed cell death. Toxicol. Pathol. 2007, 35, 495–516. [Google Scholar] [CrossRef] [PubMed]
- Wu, Q.; Zhang, K.-J.; Jiang, S.-M.; Fu, L.; Shi, Y.; Tan, R.-B.; Cui, J.; Zhou, Y. p53: A Key Protein That Regulates Pulmonary Fibrosis. Oxid. Med. Cell. Longev. 2020, 2020, 6635794. [Google Scholar] [CrossRef] [PubMed]
- Lok, S.; Stewart, J.; Kelly, B.; Hasleton, P.; Egan, J. Epstein–Barr virus and wild p53 in idiopathic pulmonary fibrosis. Respir. Med. 2001, 95, 787–791. [Google Scholar] [CrossRef] [Green Version]
- Nagaraja, M.; Tiwari, N.; Shetty, S.K.; Marudamuthu, A.S.; Fan, L.; Ostrom, R.S.; Fu, J.; Gopu, V.; Radhakrishnan, V.; Idell, S. p53 expression in lung fibroblasts is linked to mitigation of fibrotic lung remodeling. Am. J. Pathol. 2018, 188, 2207–2222. [Google Scholar] [CrossRef] [Green Version]
- Zaafan, M.A.; Haridy, A.R.; Abdelhamid, A.M. Amitriptyline attenuates bleomycin-induced pulmonary fibrosis: Modulation of the expression of NF-κβ, iNOS, and Nrf2. Naunyn-Schmiedeberg’s Arch. Pharmacol. 2019, 392, 279–286. [Google Scholar] [CrossRef]
- Zhou, J.; Li, G.; Wang, Z.-H.; Wang, L.-P.; Dong, P.-J. Effects of low-dose hydroxychloroquine on expression of phosphorylated Akt and p53 proteins and cardiomyocyte apoptosis in peri-infarct myocardium in rats. Exp. Clin. Cardiol. 2013, 18, e95. [Google Scholar]
- Zhang, Y.-P.; Cui, Q.-Y.; Zhang, T.-M.; Yi, Y.; Nie, J.-J.; Xie, G.-H.; Wu, J.-H. Chloroquine pretreatment attenuates ischemia-reperfusion injury in the brain of ob/ob diabetic mice as well as wildtype mice. Brain Res. 2020, 1726, 146518. [Google Scholar] [CrossRef]
- Zhang, X.; Dong, Y.; Li, W.-c.; Tang, B.-x.; Li, J.; Zang, Y. Roxithromycin attenuates bleomycin-induced pulmonary fibrosis by targeting senescent cells. Acta Pharmacol. Sin. 2021, 42, 2058–2068. [Google Scholar] [CrossRef]
- Dewson, G.; Kluck, R.M. Bcl-2 family-regulated apoptosis in health and disease. Cell Health Cytoskelet. 2010, 2, 9–22. [Google Scholar]
- Nemec, K.N.; Khaled, A.R. Therapeutic modulation of apoptosis: Targeting the BCL-2 family at the interface of the mitochondrial membrane. Yonsei Med. J. 2008, 49, 689–697. [Google Scholar] [CrossRef] [PubMed]
- Safaeian, L.; Abed, A.; Vaseghi, G. The role of Bcl-2 family proteins in pulmonary fibrosis. Eur. J. Pharmacol. 2014, 741, 281–289. [Google Scholar] [CrossRef]
- Safaeian, L.; Jafarian, A.; Rabbani, M.; Sadeghi, H.; Torabinia, N.; Alavi, S. The role of strain variation in BAX and BCL-2 expression in murine bleomycin-induced pulmonary fibrosis. Pakistan J. Biol. Sci. 2008, 11, 2606. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ali, A.S.; Alrashedi, M.G.; Ahmed, O.A.A.; Ibrahim, I.M. Pulmonary Delivery of Hydroxychloroquine Nanostructured Lipid Carrier as a Potential Treatment of COVID-19. Polymers 2022, 14, 2616. [Google Scholar] [CrossRef] [PubMed]
- Zubata, P.; Ceresole, R.; Rosasco, M.A.; Pizzorno, M.T. A new HPLC method for azithromycin quantitation. J. Pharm. Biomed. Anal. 2002, 27, 833–836. [Google Scholar] [CrossRef]
- Jirjees, F.; Saad, A.K.; Al Hano, Z.; Hatahet, T.; Al Obaidi, H.; Dallal Bashi, Y.H. COVID-19 treatment guidelines: Do they really reflect best medical practices to manage the pandemic? Infect. Dis. Rep. 2021, 13, 259–284. [Google Scholar] [CrossRef]
- Pani, A.; Lauriola, M.; Romandini, A.; Scaglione, F. Macrolides and viral infections: Focus on azithromycin in COVID-19 pathology. Int. J. Antimicrob. Agents 2020, 56, 106053. [Google Scholar] [CrossRef] [PubMed]
- Rau, J.L. The inhalation of drugs: Advantages and problems. Respir. Care 2005, 50, 367–382. [Google Scholar] [PubMed]
- Yang, W.; Qiang, D.; Zhang, M.; Ma, L.; Zhang, Y.; Qing, C.; Xu, Y.; Zhen, C.; Liu, J.; Chen, Y.-H. Isoforskolin pretreatment attenuates lipopolysaccharide-induced acute lung injury in animal models. Int. Immunopharmacol. 2011, 11, 683–692. [Google Scholar] [CrossRef] [PubMed]
- Bancroft, J.D.; Gamble, M. Theory and Practice of Histological Techniques; Elsevier Health Sciences: Amsterdam, The Netherlands, 2008. [Google Scholar]
- Akram, K.M.; Lomas, N.J.; Forsyth, N.R.; Spiteri, M.A. Alveolar epithelial cells in idiopathic pulmonary fibrosis display upregulation of TRAIL, DR4 and DR5 expression with simultaneous preferential over-expression of pro-apoptotic marker p53. Int. J. Clin. Exp. Pathol. 2014, 7, 552. [Google Scholar]
- Ahmed, B.S.; Anwar, N.M. Immunohistochemical study of the expression of Bcl-2 in Leydig’s interstitial cells and primary spermatocyte cells of adult male rabbit under the effect of oral Gossypol intake. Egypt. J. Hosp. Med. 2004, 14, 34–44. [Google Scholar] [CrossRef]
- McDonnell, T.; Beham, A.; Sarkiss, M.; Andersen, M.; Lo, P. Importance of the Bcl-2 family in cell death regulation. Experientia 1996, 52, 1008–1017. [Google Scholar] [CrossRef]






Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alrashedi, M.G.; Ali, A.S.; Ahmed, O.A.; Ibrahim, I.M. Local Delivery of Azithromycin Nanoformulation Attenuated Acute Lung Injury in Mice. Molecules 2022, 27, 8293. https://doi.org/10.3390/molecules27238293
Alrashedi MG, Ali AS, Ahmed OA, Ibrahim IM. Local Delivery of Azithromycin Nanoformulation Attenuated Acute Lung Injury in Mice. Molecules. 2022; 27(23):8293. https://doi.org/10.3390/molecules27238293
Chicago/Turabian StyleAlrashedi, Mohsen G., Ahmed Shaker Ali, Osama Abdelhakim Ahmed, and Ibrahim M. Ibrahim. 2022. "Local Delivery of Azithromycin Nanoformulation Attenuated Acute Lung Injury in Mice" Molecules 27, no. 23: 8293. https://doi.org/10.3390/molecules27238293