
Comparison of Two Bovine Commercial Xenografts in the Regeneration of Critical Cranial Defects
 , and
, and 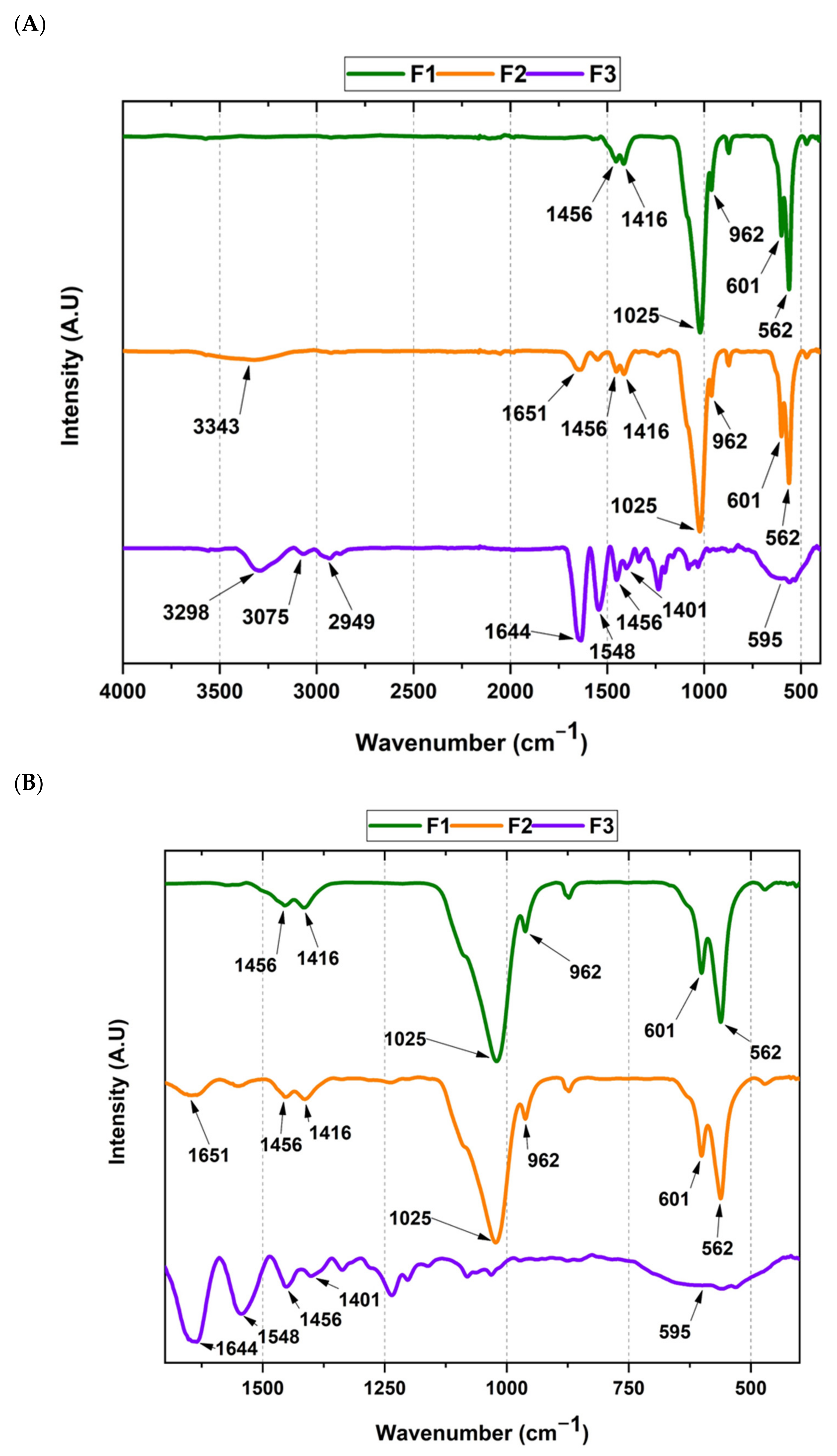{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Results and Discussion
2.1. Composite Characterization
2.1.1. Fourier-Transform Infrared Spectroscopy (FT-IR)
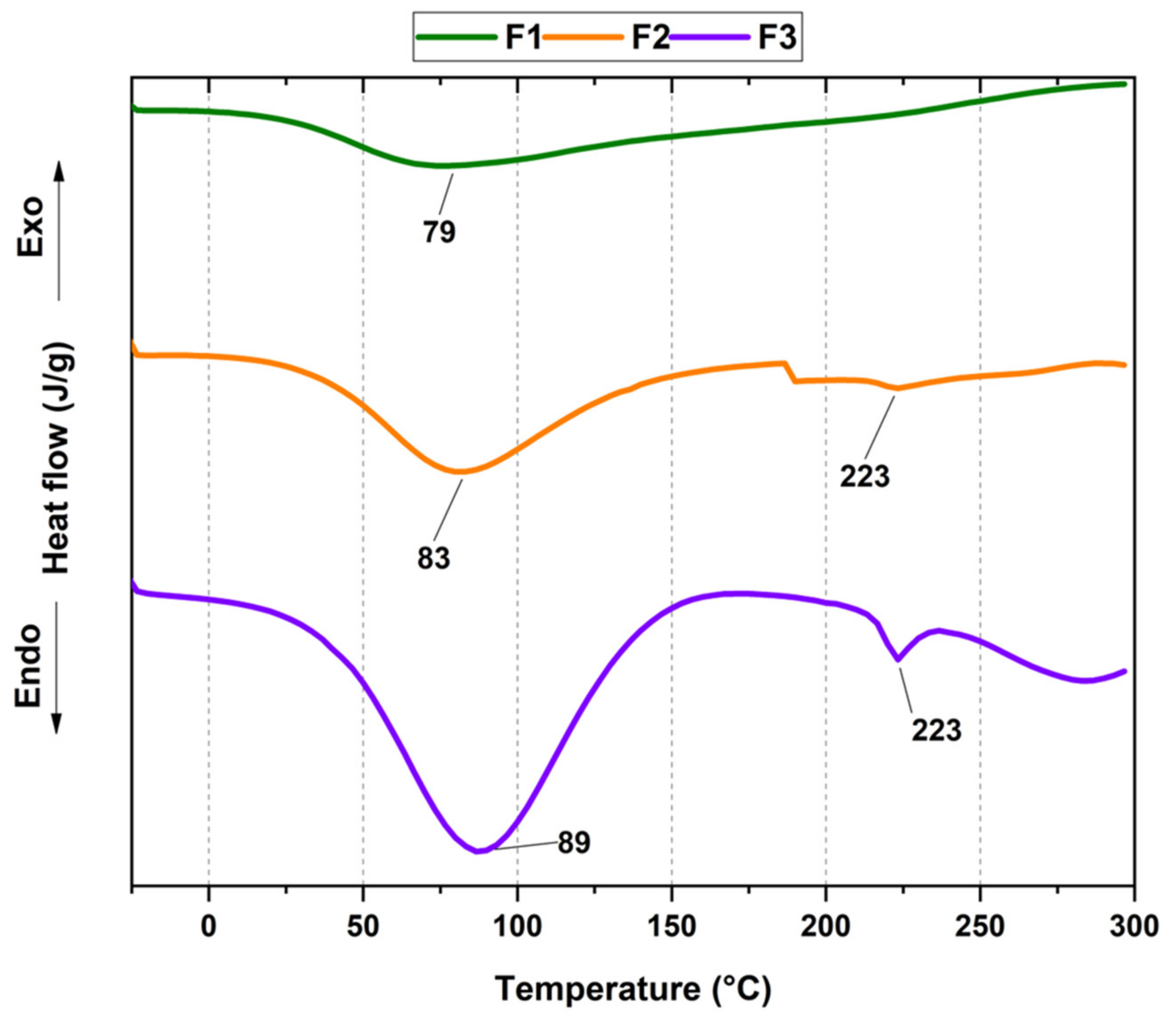
2.1.2. Thermal Characterization
Differential Scanning Calorimetric (DSC)
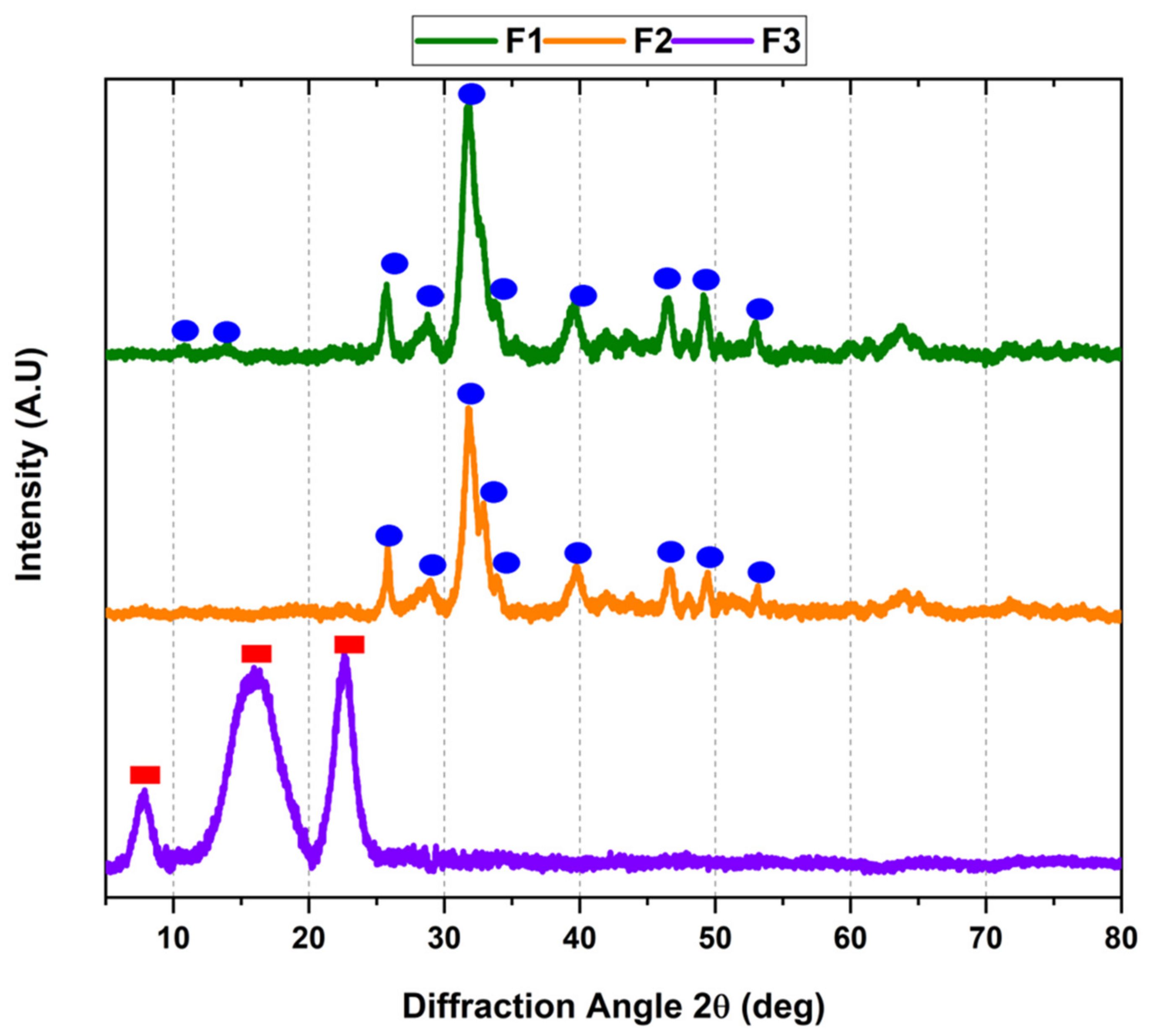
2.1.3. X-ray Diffraction Studies for the Xenografts
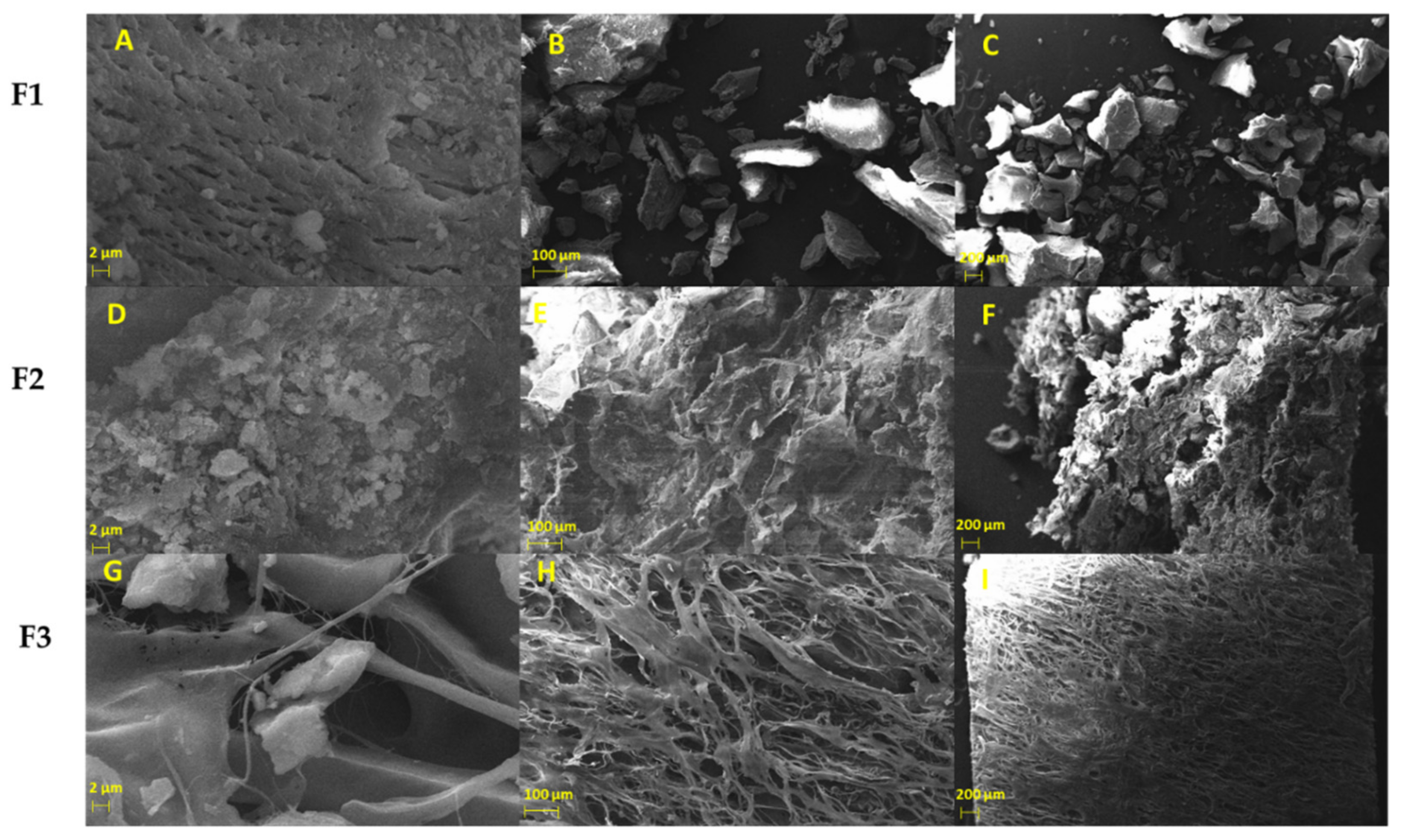
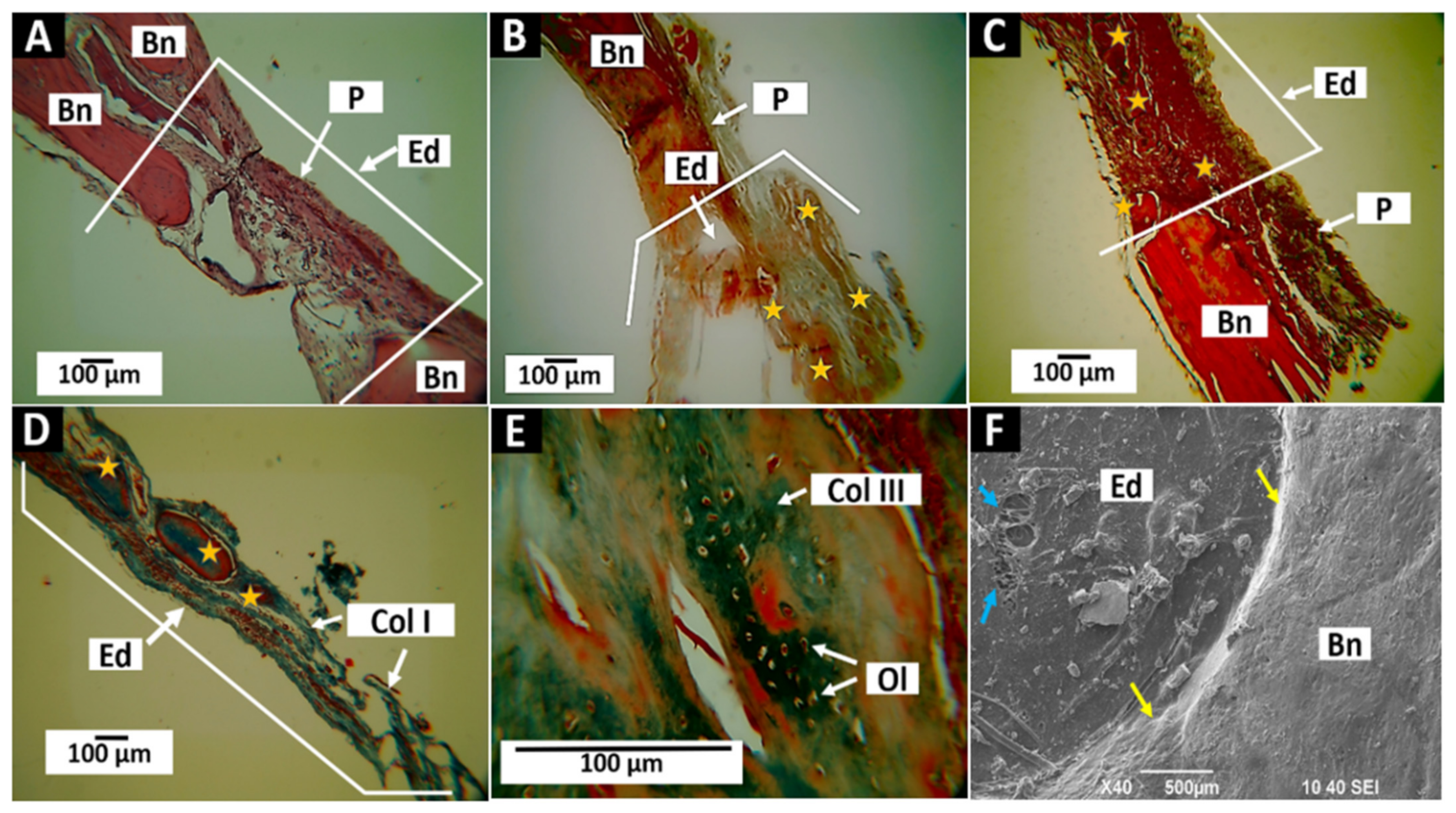
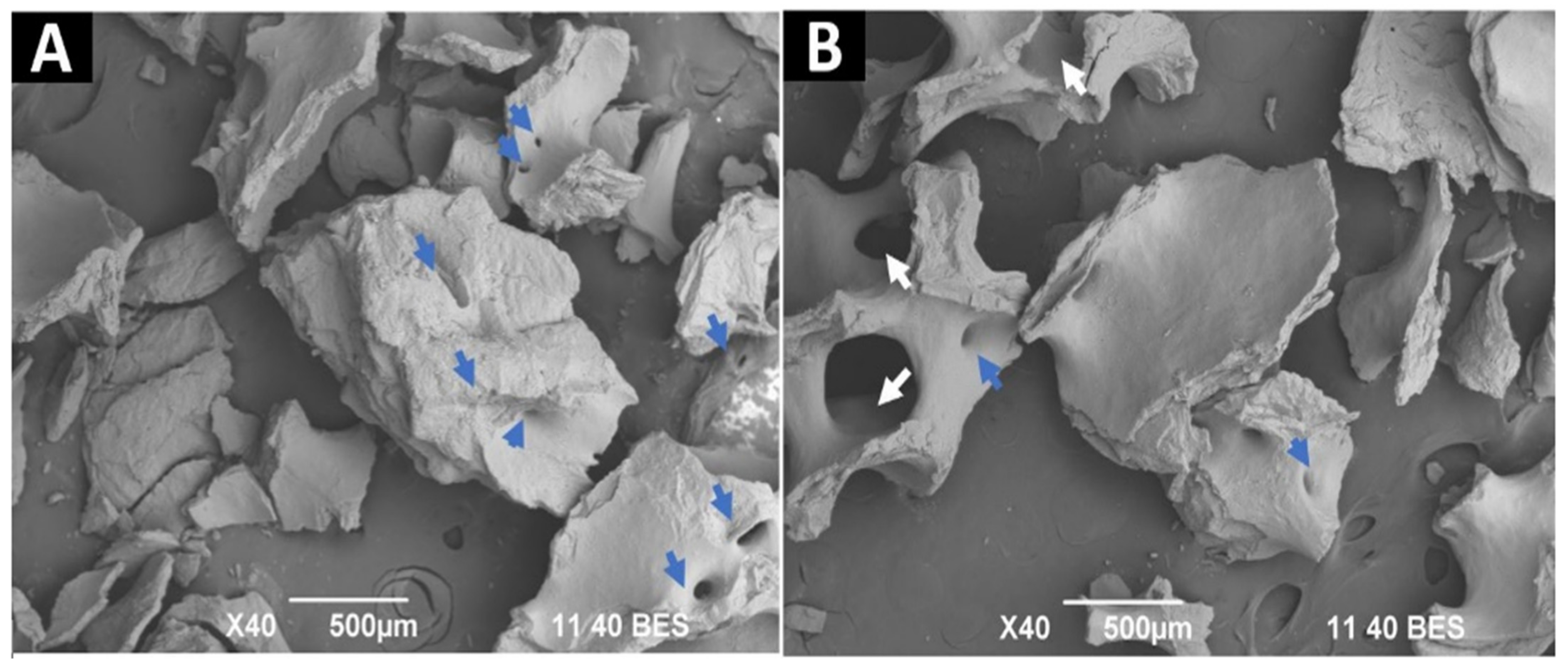
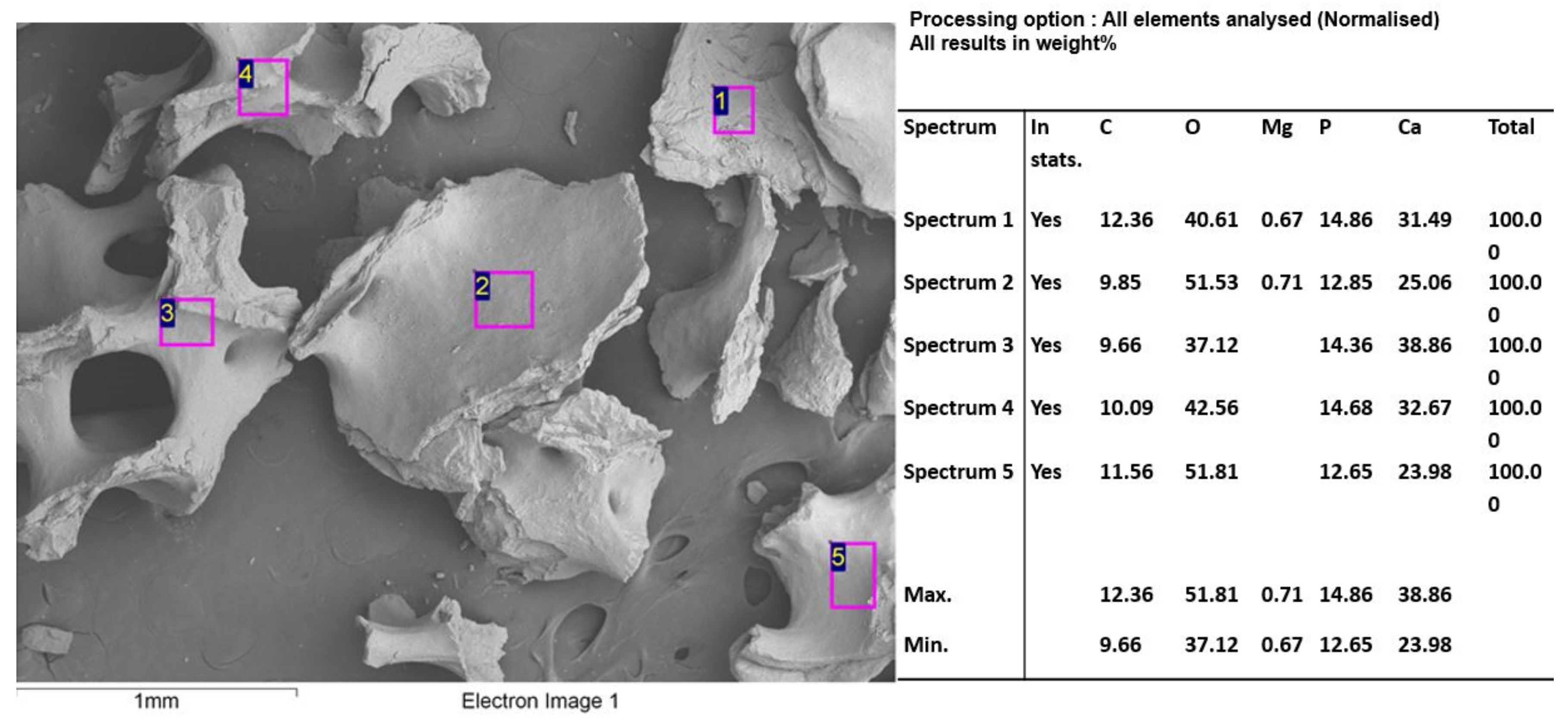
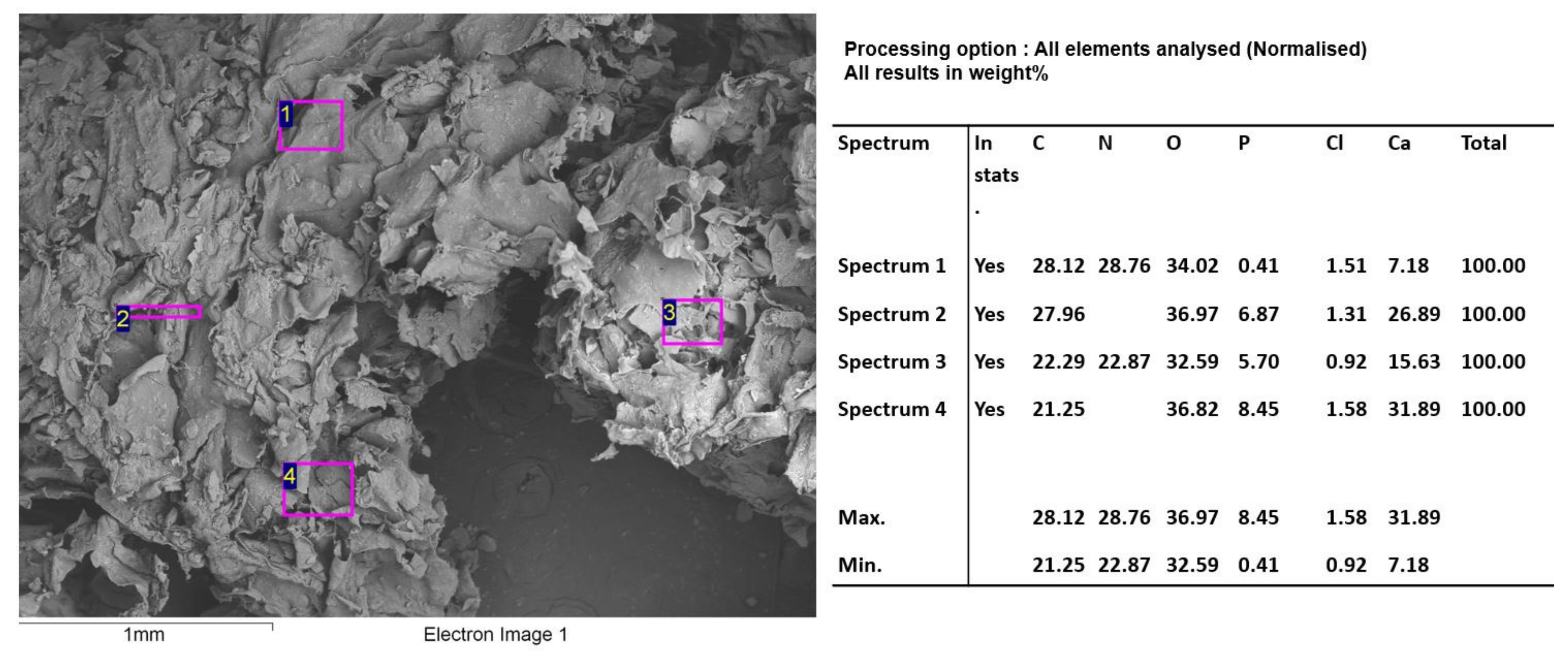
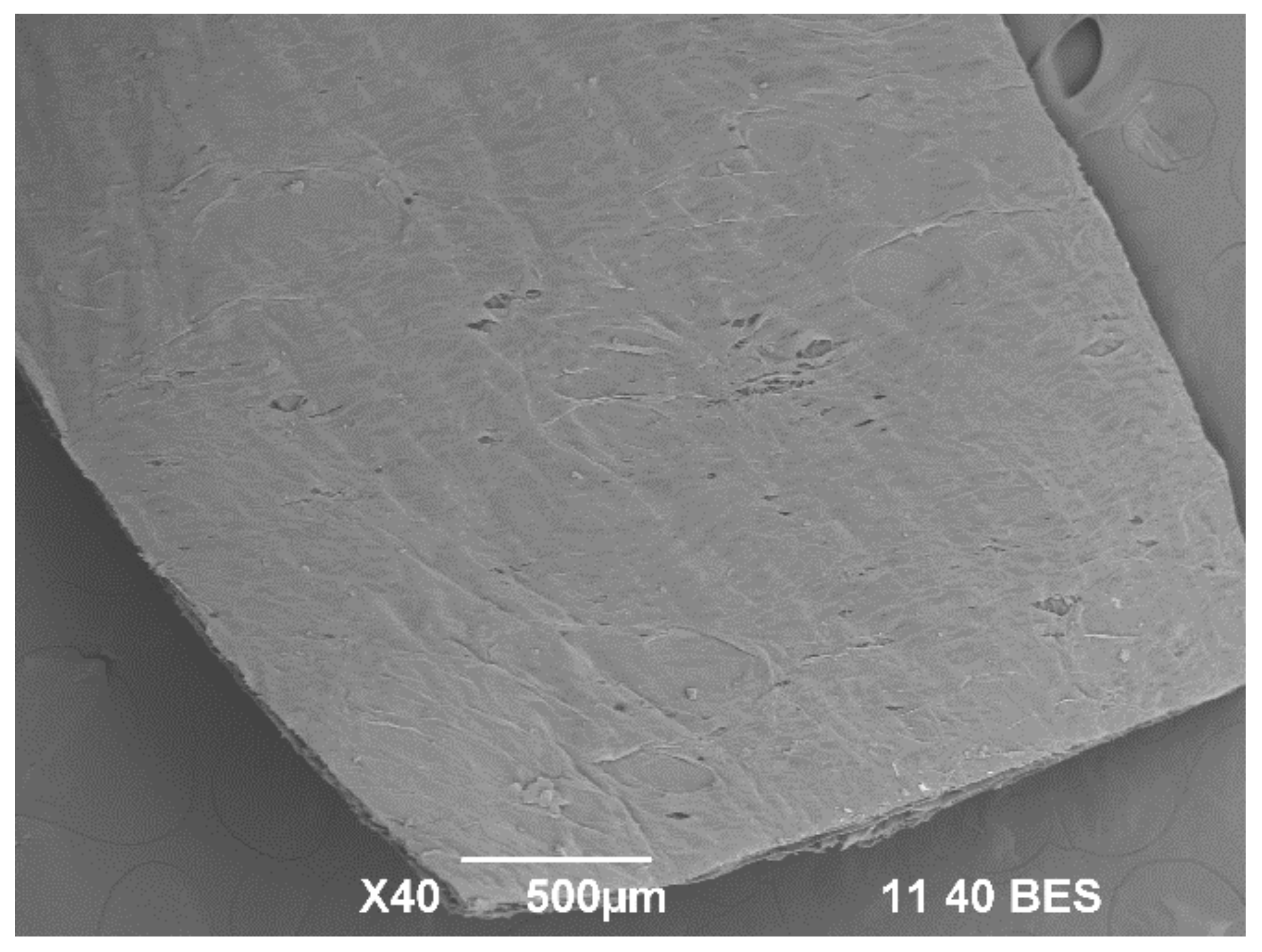
2.1.4. Morphology Studies of Xenografts
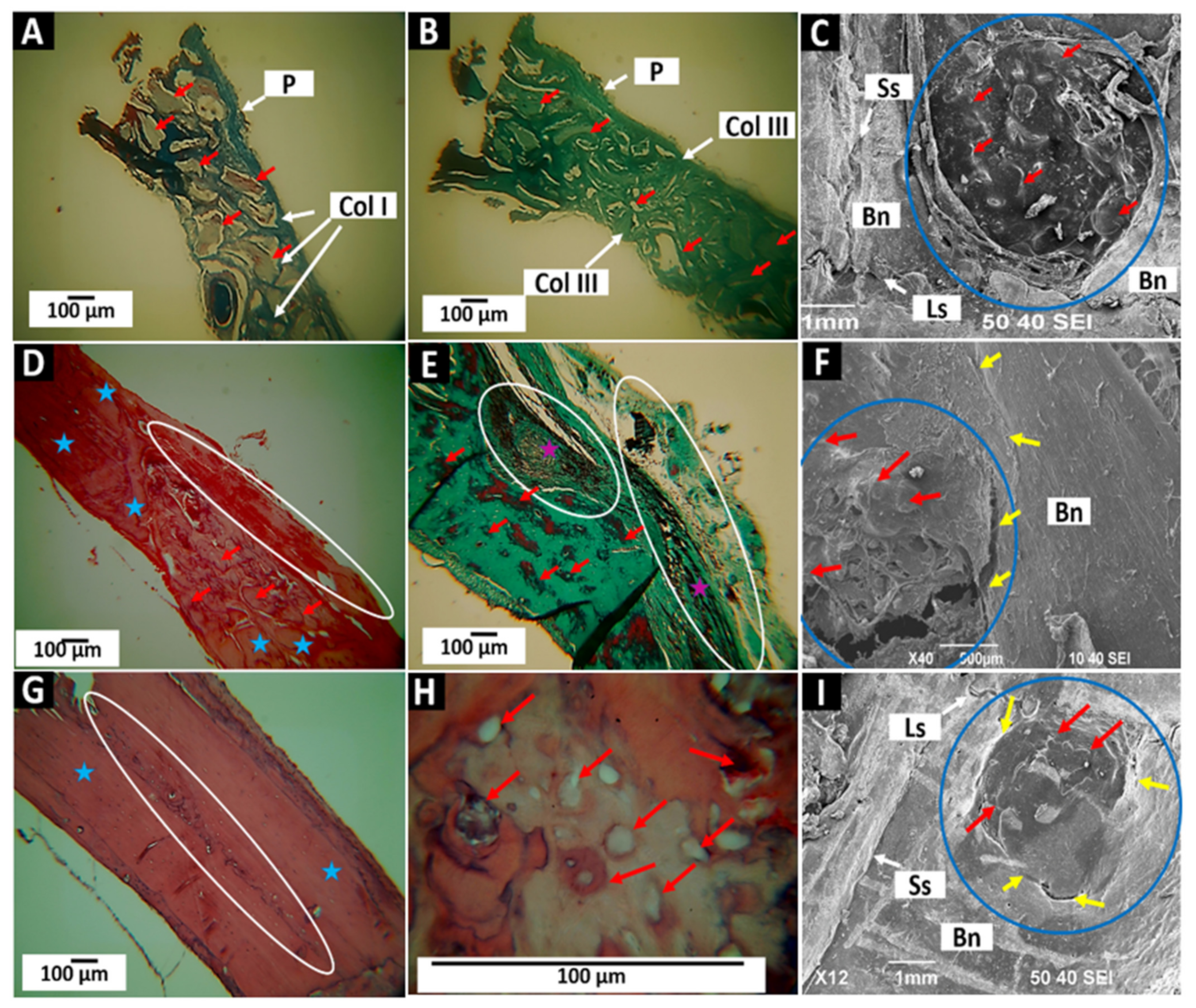
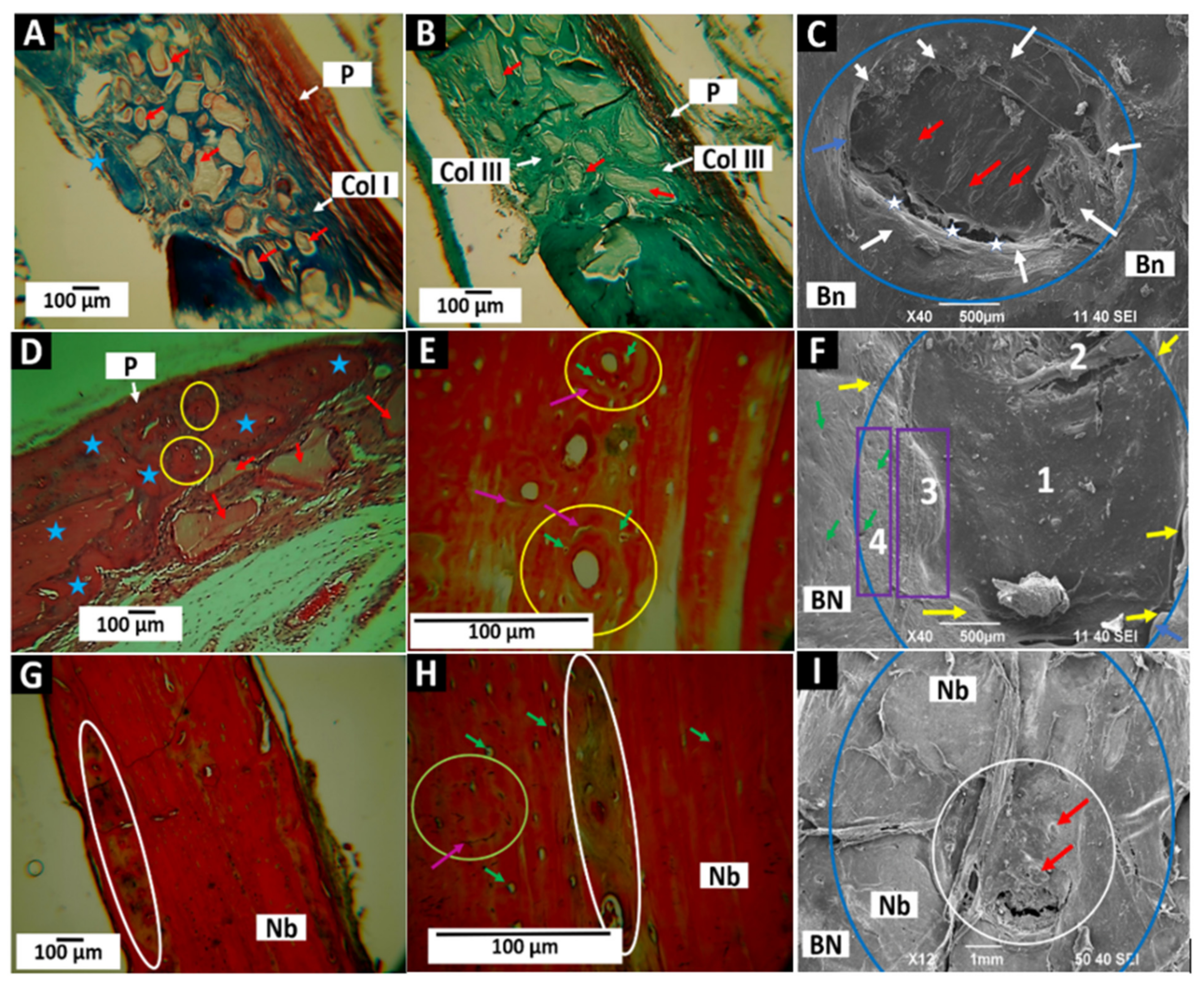
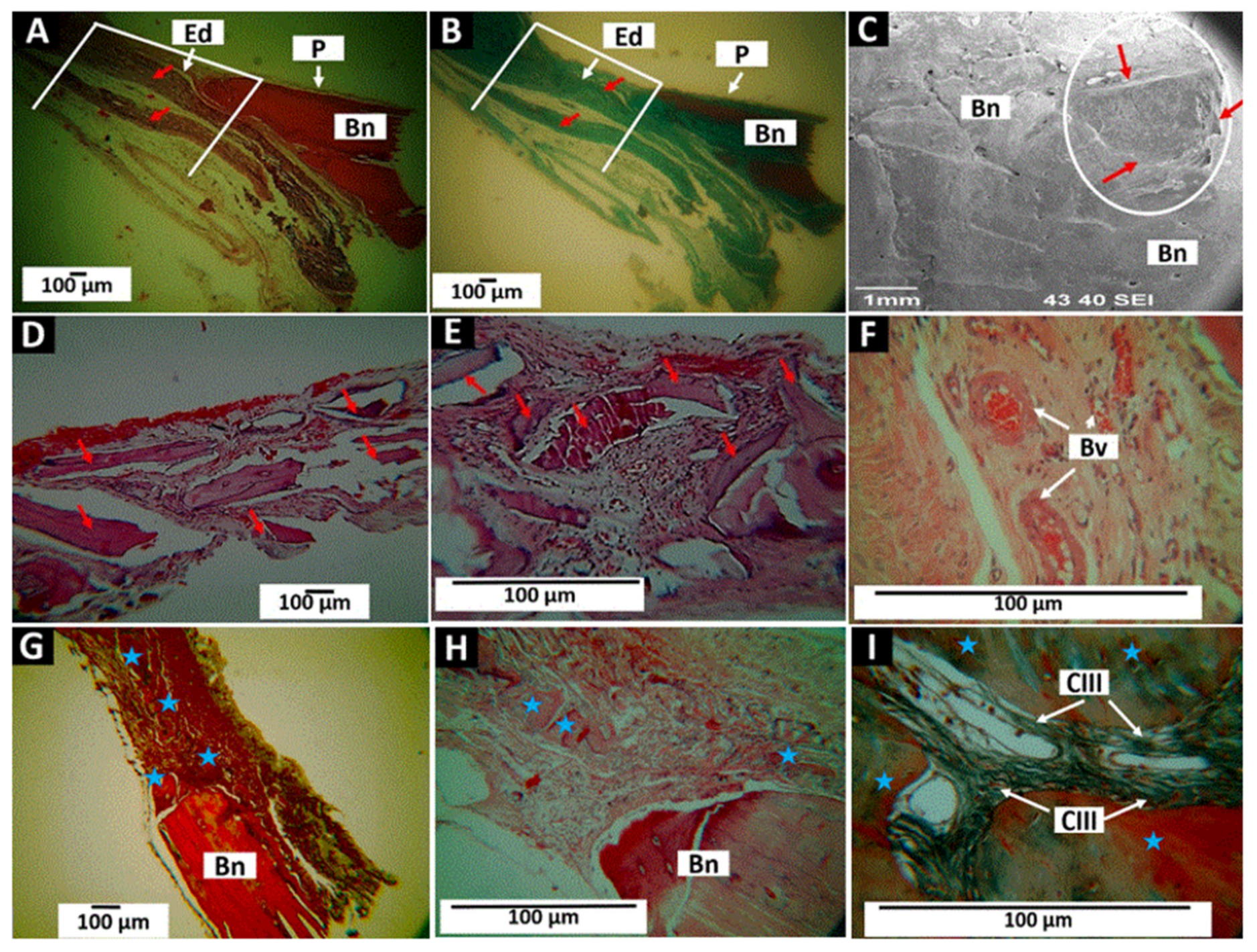
2.2. Histological Analysis of Xenografts
2.2.1. Results of Cranial Implantation of Control (Empty Defect)
2.2.2. Results of Cranial Implantation of F1 (InterOss)
2.2.3. Results of Cranial Implantation of F1 (InterOss)
2.2.4. Results of Cranial Implantation of F2 (InterOss Collagen)
2.2.5. Results of Cranial Implantation of F3 (InterCollagen Guide)
3. Materials and Methods
3.1. Characterization of the Xenografts
3.1.1. Fourier Transform Infrared Spectroscopy (FT-IR)
3.1.2. Thermal Analysis
3.1.3. X-ray Diffraction (XRD)
3.1.4. Scanning Electron Microscopy (SEM)
3.2. Histological Analysis of Xenografts
3.2.1. Surgical Preparations
3.2.2. Sample Preparation
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Sample Availability
References
- Chen, M.-Y.; Fang, J.-J.; Lee, J.-N.; Periasamy, S.; Yen, K.-C.; Wang, H.-C.; Hsieh, D.-J. Supercritical Carbon Dioxide Decellularized Xenograft-3D CAD/CAM Carved Bone Matrix Personalized for Human Bone Defect Repair. Genes 2022, 13, 1–14. [Google Scholar] [CrossRef]
- Zhang, S.; Li, X.; Qi, Y.; Ma, X.; Qiao, S.; Cai, H.X.; Zhao, B.C.; Jiang, H.B.; Lee, E.S. Comparison of Autogenous Tooth Materials and Other Bone Grafts. Tissue Eng. Regen. Med. 2021, 18, 327–341. [Google Scholar] [CrossRef] [PubMed]
- Dimar, J.R.; Glassman, S.D. The Art of Bone Grafting. Contemp. Spine Surg. 2008, 9, 1–7. [Google Scholar] [CrossRef]
- Najafi-Ghalehlou, N.; Feizkhah, A.; Mobayen, M.; Pourmohammadi-Bejarpasi, Z.; Shekarchi, S.; Roushandeh, A.M.; Roudkenar, M.H. Plumping up a Cushion of Human Biowaste in Regenerative Medicine: Novel Insights into a State-of-the-Art Reserve Arsenal; Springer: New York, NY, USA, 2022; ISBN 0123456789. [Google Scholar]
- Singh, R.; Mahesh, L.; Shukla, S. Infections Resulting from Bone Grafting Biomaterials. Int. J. Oral Implantol. Clin. Res. 2013, 4, 68–71. [Google Scholar] [CrossRef]
- Picciolo, G.; Peditto, M.; Irrera, N.; Pallio, G.; Altavilla, D.; Vaccaro, M.; Picciolo, G.; Scarfone, A.; Squadrito, F.; Oteri, G. Preclinical and Clinical Applications of Biomaterialsin the Enhancement of Wound Healing in OralSurgery.Pdf. Pharmaceutics 2020, 12, 1018. [Google Scholar] [CrossRef] [PubMed]
- Bassi, A.P.F.; Bizelli, V.F.; Consolaro, R.B.; de Carvalho, P.S.P. Biocompatibility and Osteopromotor Factor of Bovine Integral Bone—a Microscopic and Histometric Analysis. Front. Oral Maxillofac. Med. 2021, 3, 33. [Google Scholar] [CrossRef]
- Sheikh, Z.; Hamdan, N.; Ikeda, Y.; Grynpas, M.; Ganss, B.; Glogauer, M. Natural Graft Tissues and Synthetic Biomaterials for Periodontal and Alveolar Bone Reconstructive Applications: A Review. Biomater. Res. 2017, 21, 1–20. [Google Scholar] [CrossRef]
- Precheur, H.V. Bone Graft Materials. Dent. Clin. N. Am. 2007, 51, 729–746. [Google Scholar] [CrossRef]
- Tahmasebi, E.; Alam, M.; Yazdanian, M.; Tebyanian, H.; Yazdanian, A.; Seifalian, A.; Mosaddad, S.A. Current Biocompatible Materials in Oral Regeneration: A Comprehensive Overview of Composite Materials. J. Mater. Res. Technol. 2020, 9, 11731–11755. [Google Scholar] [CrossRef]
- Rodríguez, Á.E.; Nowzari, H. The Long-Term Risks and Complications of Bovine-Derived Xenografts. Rev. La Asoc. Dent. Mex. 2020, 77, 108–116. [Google Scholar] [CrossRef]
- Marina, A.; Gentile, P.; Chiono, V.; Ciardelli, G. Acta Biomaterialia Collagen for Bone Tissue Regeneration. Acta Biomater. 2012, 8, 3191–3200. [Google Scholar] [CrossRef]
- Walters, B.D.; Stegemann, J.P. Strategies for Directing the Structure and Function of Three-Dimensional Collagen Biomaterials across Length Scales. Acta Biomater. 2014, 10, 1488–1501. [Google Scholar] [CrossRef] [PubMed]
- Kouketsu, A.; Matsui, K.; Kawai, T.; Ezoe, Y.; Yanagisawa, T.; Yasuda, A.; Takahashi, T.; Kamakura, S. Octacalcium Phosphate Collagen Composite Stimulates the Expression and Activity of Osteogenic Factors to Promote Bone Regeneration. J. Tissue Eng. Regen. Med. 2020, 14, 99–107. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Li, M.; Long, Z.; Yang, D.; Guo, S.; Li, J.; Liu, D.; Gao, P.; Chen, G.; Wang, Z. Collagen/β-TCP Composite as a Bone-Graft Substitute for Posterior Spinal Fusion in Rabbit Model: A Comparison Study. Biomed. Mater. 2019, 14, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Vajgel, A.; Mardas, N.; Farias, B.C.; Petrie, A.; Cimões, R.; Donos, N. A Systematic Review on the Critical Size Defect Model. Clin. Oral Implant. Res. 2014, 25, 879–893. [Google Scholar] [CrossRef]
- Ferreira, V.; Umasi, E.; Santos, A.; Veras, C.; Rampazzo, G.; Faverani, L. Calvaria Critical Size Defects Regeneration Using Collagen Membranes to Assess the Osteopromotive Principle: An Animal Study. Membranes 2022, 12, 1–16. [Google Scholar]
- Valencia-Llano, C.H.; López-Tenorio, D.; Grande-Tovar, C.D. Biocompatibility Assessment of Two Commercial Bone Xenografts by In Vitro and In Vivo Methods. Polymers 2022, 14, 2672. [Google Scholar] [CrossRef]
- Elizalde-Mota, M.K.; Hernández-Romero, C.; Rocha-Rocha, V.M.; Mayoral-García, V.A. Cambios Dimensionales En Técnicas de Preservación Alveolar Bartee y Bio-Col Con Xenoinjerto Inteross®. Int. J. Odontostomatol. 2021, 15, 370–376. [Google Scholar] [CrossRef]
- Shaheen, M.Y.; Basudan, A.M.; Niazy, A.A.; van den Beucken, J.J.; Jansen, J.A.; Alghamdi, H.S. Histological and Histomorphometric Analyses of Bone Regeneration in Osteoporotic Rats Using a Xenograft Material. Materials 2021, 14, 222. [Google Scholar] [CrossRef]
- Kim, D.; Hong, H.; Lin, J.; Nevins, M. Evaluation of the Bone-Regenerating Effects of Two Anorganic Bovine Bone Grafts in a Critical-Sized Alveolar Ridge Defect Model. Int. J. Periodontics Restor. Dent. 2017, 37, e234–e244. [Google Scholar] [CrossRef]
- Jain, G.; Blaauw, D.; Chang, S. A Comparative Study of Two Bone Graft Substitutes—InterOss® Collagen and OCS-B Collagen®. J. Funct. Biomater. 2022, 13, 28. [Google Scholar] [CrossRef]
- Pannarale, L.; Morini, S.; D’Ubaldo, E.; Gaudio, E.; Marinozzi, G. SEM Corrosion-casts Study of the Microcirculation of the Flat Bones in the Rat. Anat. Rec. An. Off. Publ. Am. Assoc. Anat. 1997, 247, 462–471. [Google Scholar] [CrossRef]
- Lee, D.S.H.; Pai, Y.; Chang, S. Physicochemical Characterization of InterOss® and Bio-Oss® Anorganic Bovine Bone Grafting Material for Oral Surgery–A Comparative Study. Mater. Chem. Phys. 2014, 146, 99–104. [Google Scholar] [CrossRef]
- Werner, J.; Linner-Krčmar, B.; Friess, W.; Greil, P. Mechanical Properties and in Vitro Cell Compatibility of Hydroxyapatite Ceramics with Graded Pore Structure. Biomaterials 2002, 23, 4285–4294. [Google Scholar] [CrossRef]
- Ryan, A.J.; Gleeson, J.P.; Matsiko, A.; Thompson, E.M.; O’Brien, F.J. Effect of Different Hydroxyapatite Incorporation Methods on the Structural and Biological Properties of Porous Collagen Scaffolds for Bone Repair. J. Anat. 2015, 227, 732–745. [Google Scholar] [CrossRef]
- Ślósarczyk, A.; Paszkiewicz, Z.; Paluszkiewicz, C. FTIR and XRD Evaluation of Carbonated Hydroxyapatite Powders Synthesized by Wet Methods. J. Mol. Struct. 2005, 744, 657–661. [Google Scholar] [CrossRef]
- Lee, J.H.; Yi, G.S.; Lee, J.W.; Kim, D.J. Physicochemical Characterization of Porcine Bone-Derived Grafting Material and Comparison with Bovine Xenografts for Dental Applications. J. Periodontal Implant. Sci. 2017, 47, 388–401. [Google Scholar] [CrossRef]
- Riaz, T.; Zeeshan, R.; Zarif, F.; Ilyas, K.; Muhammad, N.; Safi, S.Z.; Rahim, A.; Rizvi, S.A.A.; Rehman, I.U. FTIR Analysis of Natural and Synthetic Collagen. Appl. Spectrosc. Rev. 2018, 53, 703–746. [Google Scholar] [CrossRef]
- Ahmadi, A.; Ahmadi, P.; Ehsani, A. Development of an Active Packaging System Containing Zinc Oxide Nanoparticles for the Extension of Chicken Fillet Shelf Life. Food Sci. Nutr. 2020, 8, 5461–5473. [Google Scholar] [CrossRef]
- Stani, C.; Vaccari, L.; Mitri, E.; Birarda, G. FTIR Investigation of the Secondary Structure of Type I Collagen: New Insight into the Amide III Band. Spectrochim. Acta Part A Mol. Biomol. Spectrosc. 2020, 229, 118006. [Google Scholar] [CrossRef]
- Safandowska, M.; Pietrucha, K. Effect of Fish Collagen Modification on Its Thermal and Rheological Properties. Int. J. Biol. Macromol. 2013, 53, 32–37. [Google Scholar] [CrossRef] [PubMed]
- Sionkowska, A.; Kozłowska, J. Characterization of Collagen/Hydroxyapatite Composite Sponges as a Potential Bone Substitute. Int. J. Biol. Macromol. 2010, 47, 483–487. [Google Scholar] [CrossRef] [PubMed]
- León-Mancilla, B.H.; Araiza-Téllez, M.A.; Flores-Flores, J.O.; Piña-Barba, M.C. Physico-Chemical Characterization of Collagen Scaffolds for Tissue Engineering. J. Appl. Res. Technol. 2016, 14, 77–85. [Google Scholar] [CrossRef]
- Rochdi, A.; Foucat, L.; Renou, J.-P. NMR and DSC Studies during Thermal Denaturation of Collagen. Food Chem. 2000, 69, 295–299. [Google Scholar] [CrossRef]
- Rabiei, M.; Palevicius, A.; Monshi, A.; Nasiri, S.; Vilkauskas, A.; Janusas, G. Comparing Methods for Calculating Nano Crystal Size of Natural Hydroxyapatite Using X-Ray Diffraction. Nanomaterials 2020, 10, 1627. [Google Scholar] [CrossRef]
- Accorsi-Mendonça, T.; Conz, M.B.; Barros, T.C.; Sena, L.Á.D.; Soares, G.D.A.; Granjeiro, J.M. Physicochemical Characterization of Two Deproteinized Bovine Xenografts. Braz. Oral Res. 2008, 22, 5–10. [Google Scholar] [CrossRef]
- Becerra, J.; Rodriguez, M.; Leal, D.; Noris-Suarez, K.; Gonzalez, G. Chitosan-Collagen-Hydroxyapatite Membranes for Tissue Engineering. J. Mater. Sci. Mater. Med. 2022, 33, 18. [Google Scholar] [CrossRef]
- Valencia, G.A.; Luciano, C.G.; Lourenço, R.V.; Bittante, A.M.Q.B.; do Amaral Sobral, P.J. Morphological and Physical Properties of Nano-Biocomposite Films Based on Collagen Loaded with Laponite®. Food Packag. Shelf Life 2019, 19, 24–30. [Google Scholar] [CrossRef]
- Andonegi, M.; Peñalba, M.; de la Caba, K.; Guerrero, P. ZnO Nanoparticle-Incorporated Native Collagen Films with Electro-Conductive Properties. Mater. Sci. Eng. C 2020, 108, 110394. [Google Scholar] [CrossRef]
- Chen, J.; Li, L.; Yi, R.; Xu, N.; Gao, R.; Hong, B. Extraction and Characterization of Acid-Soluble Collagen from Scales and Skin of Tilapia (Oreochromis Niloticus). LWT-Food Sci. Technol. 2016, 66, 453–459. [Google Scholar] [CrossRef]
- Chatzipetros, E.; Yfanti, Z.; Christopoulos, P.; Donta, C.; Damaskos, S.; Tsiambas, E.; Tsiourvas, D.; Kalogirou, E.M.; Tosios, K.I.; Tsiklakis, K. Imaging of Nano-Hydroxyapatite/Chitosan Scaffolds Using a Cone Beam Computed Tomography Device on Rat Calvarial Defects with Histological Verification. Clin. Oral Investig. 2020, 24, 437–446. [Google Scholar] [CrossRef]
- Agrali, O.B.; Yildirim, S.; Ozener, H.O.; Köse, K.N.; Ozbeyli, D.; Soluk-Tekkesin, M.; Kuru, L. Evaluation of the Effectiveness of Esterified Hyaluronic Acid Fibers on Bone Regeneration in Rat Calvarial Defects. Biomed. Res. Int. 2018, 2018, 1–8. [Google Scholar] [CrossRef]
- Schmitz, J.P.; Hollinger, J.O. The Critical Size Defect as an Experimental Model for Craniomandibulofacial Nonunions. Clin. Orthop. Relat. Res. 1986, 205, 299–308. [Google Scholar] [CrossRef]
- Gosain, A.K.; Song, L.; Yu, P.; Mehrara, B.J.; Maeda, C.Y.; Gold, L.I.; Longaker, M.T. Osteogenesis in Cranial Defects: Reassessment of the Concept of Critical Size and the Expression of TGF-β Isoforms. Plast. Reconstr. Surg. 2000, 106, 360–371. [Google Scholar] [CrossRef]
- Tovar, N.; Jimbo, R.; Gangolli, R.; Perez, L.; Manne, L.; Yoo, D.; Lorenzoni, F.; Witek, L.; Coelho, P.G. Evaluation of Bone Response to Various Anorganic Bovine Bone Xenografts: An Experimental Calvaria Defect Study. Int. J. Oral Maxillofac. Surg. 2014, 43, 251–260. [Google Scholar] [CrossRef]
- Comuzzi, L.; Tumedei, M.; Piattelli, A.; Tartaglia, G.; Del Fabbro, M. Radiographic Analysis of Graft Dimensional Changes in Transcrestal Maxillary Sinus Augmentation: A Retrospective Study. Materials 2022, 15, 2964. [Google Scholar] [CrossRef]
- Manfro, R.; Fonseca, F.S.; Bortoluzzi, M.C.; Sendyk, W.R. Comparative, Histological and Histomorphometric Analysis of Three Anorganic Bovine Xenogenous Bone Substitutes: Bio-Oss, Bone-Fill and Gen-Ox Anorganic. J. Maxillofac. Oral Surg. 2014, 13, 464–470. [Google Scholar] [CrossRef]
- Saran, U.; Gemini Piperni, S.; Chatterjee, S. Role of Angiogenesis in Bone Repair. Arch. Biochem. Biophys. 2014, 561, 109–117. [Google Scholar] [CrossRef]
- Fernández, T.; Olave, G.; Valencia, C.H.; Arce, S.; Quinn, J.M.W.; Thouas, G.A.; Chen, Q.-Z. Effects of Calcium Phosphate/Chitosan Composite on Bone Healing in Rats: Calcium Phosphate Induces Osteon Formation. Tissue Eng. Part A 2014, 20, 1948–1960. [Google Scholar] [CrossRef]
- Fernández, M.P.R.; Gehrke, S.A.; Martinez, C.P.A.; Guirado, J.L.C.; de Aza, P.N. SEM-EDX Study of the Degradation Process of Two Xenograft Materials Used in Sinus Lift Procedures. Materials 2017, 10, 542. [Google Scholar] [CrossRef]
- Li, Y.; Liu, Y.; Li, R.; Bai, H.; Zhu, Z.; Zhu, L.; Zhu, C.; Che, Z.; Liu, H.; Wang, J.; et al. Collagen-Based Biomaterials for Bone Tissue Engineering. Mater. Des. 2021, 210, 110049. [Google Scholar] [CrossRef]
- Twardowski, T.; Fertala, A.; Orgel, J.; San Antonio, J. Type I Collagen and Collagen Mimetics as Angiogenesis Promoting Superpolymers. Curr. Pharm. Des. 2007, 13, 3608–3621. [Google Scholar] [CrossRef] [PubMed]
- Keil, C.; Gollmer, B.; Zeidler-Rentzsch, I.; Gredes, T.; Heinemann, F. Histological Evaluation of Extraction Sites Grafted with Bio-Oss Collagen: Randomized Controlled Trial. Ann. Anat. 2021, 237, 151722. [Google Scholar] [CrossRef] [PubMed]
- Wessing, B.; Lettner, S.; Zechner, W. Guided Bone Regeneration with Collagen Membranes and Particulate Graft Materials: A Systematic Review and Meta-Analysis. Int. J. Oral Maxillofac. Implant. 2018, 33, 87–100. [Google Scholar] [CrossRef]
- Sbricoli, L.; Guazzo, R.; Annunziata, M.; Gobbato, L.; Bressan, E.; Nastri, L. Selection of Collagen Membranes for Bone Regeneration: A Literature Review. Materials 2020, 13, 786. [Google Scholar] [CrossRef]
- Feher, B.; Apaza Alccayhuaman, K.A.; Strauss, F.J.; Lee, J.-S.; Tangl, S.; Kuchler, U.; Gruber, R. Osteoconductive Properties of Upside-down Bilayer Collagen Membranes in Rat Calvarial Defects. Int. J. Implant. Dent. 2021, 7, 1–10. [Google Scholar] [CrossRef]
- Ramires, G.A.D.; Helena, J.T.; De Oliveira, J.C.S.; Faverani, L.P.; Bassi, A.P.F. Evaluation of Guided Bone Regeneration in Critical Defects Using Bovine and Porcine Collagen Membranes: Histomorphometric and Immunohistochemical Analyses. Int. J. Biomater. 2021, 2021, 1–9. [Google Scholar] [CrossRef]
- Du Sert, N.P.; Hurst, V.; Ahluwalia, A.; Alam, S.; Avey, M.T.; Baker, M.; Browne, W.J.; Clark, A.; Cuthill, I.C.; Dirnagl, U.; et al. The Arrive Guidelines 2.0: Updated Guidelines for Reporting Animal Research. PLoS Biol. 2020, 18, e3000410. [Google Scholar] [CrossRef]












Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Valencia-Llano, C.H.; López-Tenorio, D.; Saavedra, M.; Zapata, P.A.; Grande-Tovar, C.D. Comparison of Two Bovine Commercial Xenografts in the Regeneration of Critical Cranial Defects. Molecules 2022, 27, 5745. https://doi.org/10.3390/molecules27185745
Valencia-Llano CH, López-Tenorio D, Saavedra M, Zapata PA, Grande-Tovar CD. Comparison of Two Bovine Commercial Xenografts in the Regeneration of Critical Cranial Defects. Molecules. 2022; 27(18):5745. https://doi.org/10.3390/molecules27185745
Chicago/Turabian StyleValencia-Llano, Carlos Humberto, Diego López-Tenorio, Marcela Saavedra, Paula A. Zapata, and Carlos David Grande-Tovar. 2022. "Comparison of Two Bovine Commercial Xenografts in the Regeneration of Critical Cranial Defects" Molecules 27, no. 18: 5745. https://doi.org/10.3390/molecules27185745