
Human Remains Identification Using Micro-CT, Chemometric and AI Methods in Forensic Experimental Reconstruction of Dental Patterns after Concentrated Sulphuric Acid Significant Impact

 ,
,  , , , , and
, , , , and
Abstract
:
1. Introduction
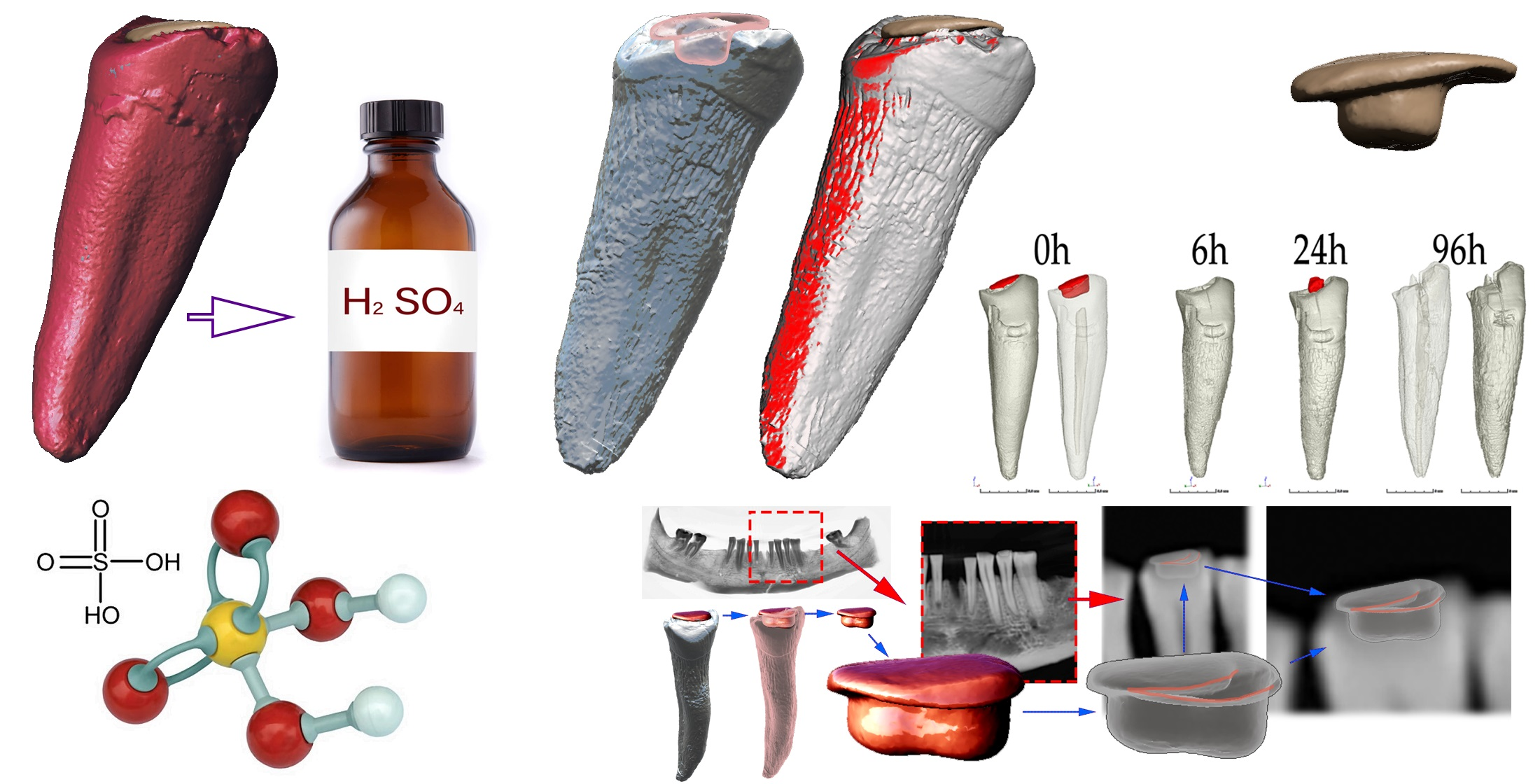
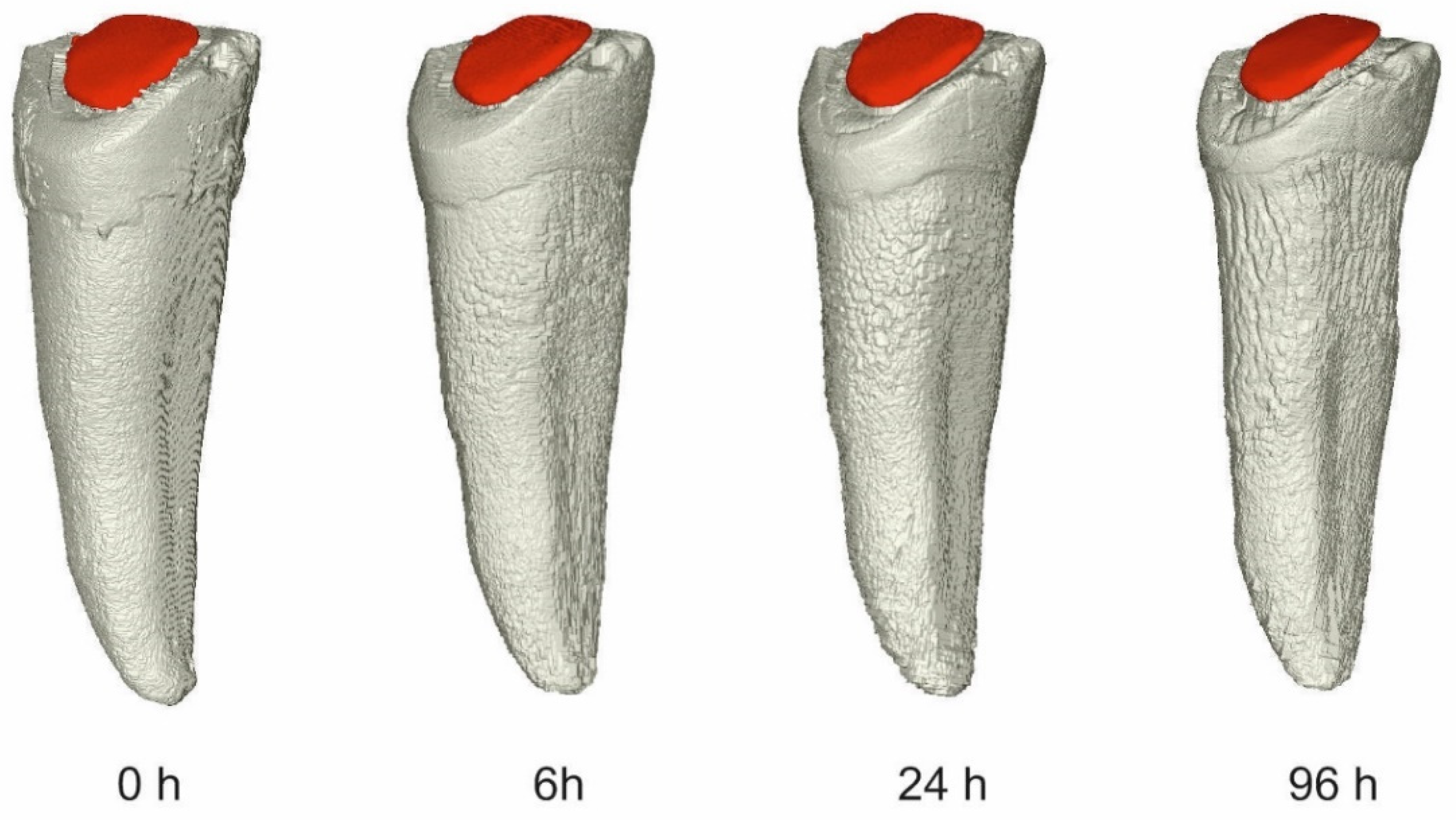
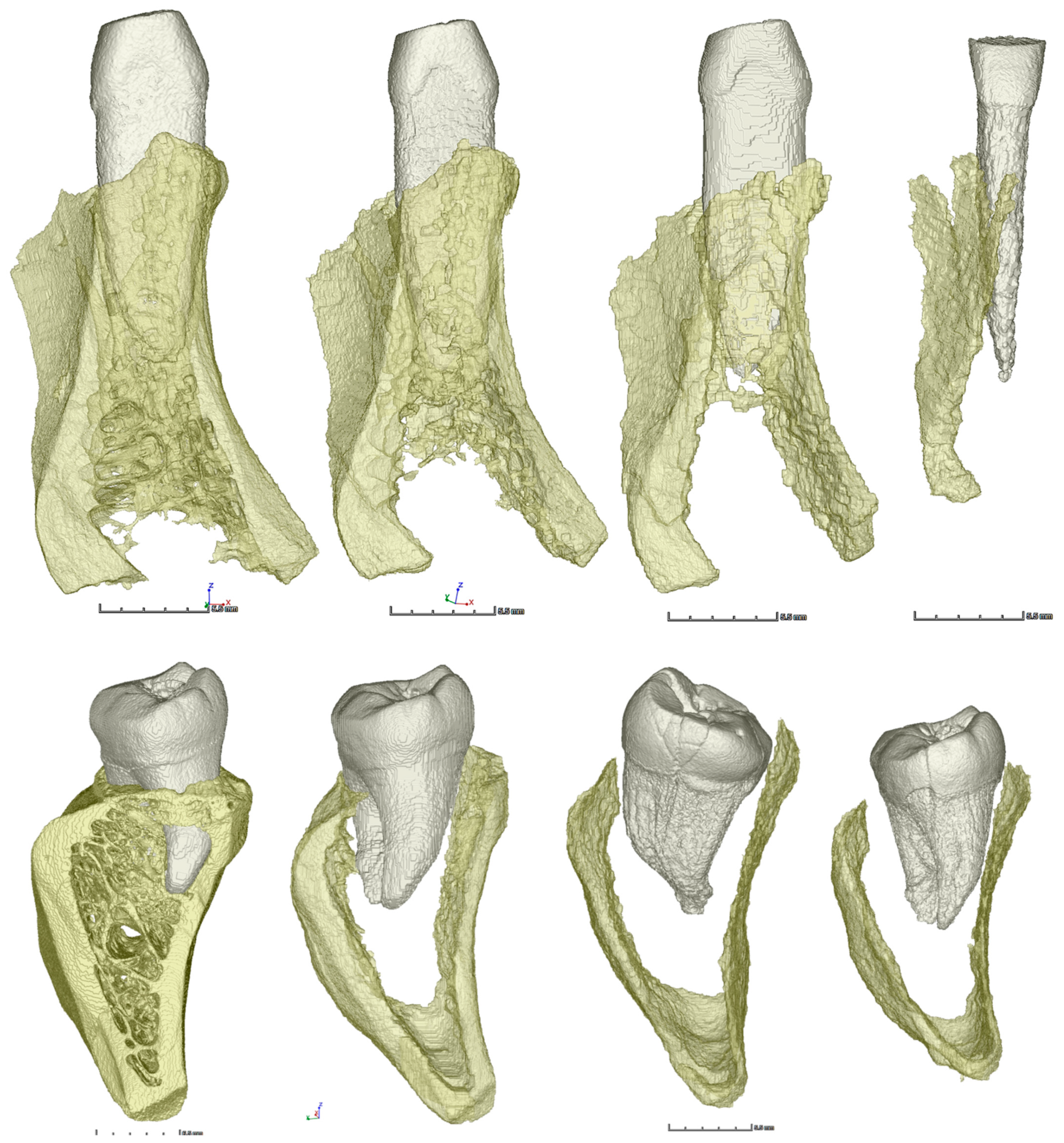
- A human mandible with teeth (treated post-mortem) was degraded in 75% sulfuric acid, and the accompanying morphological and chemical changes were documented;
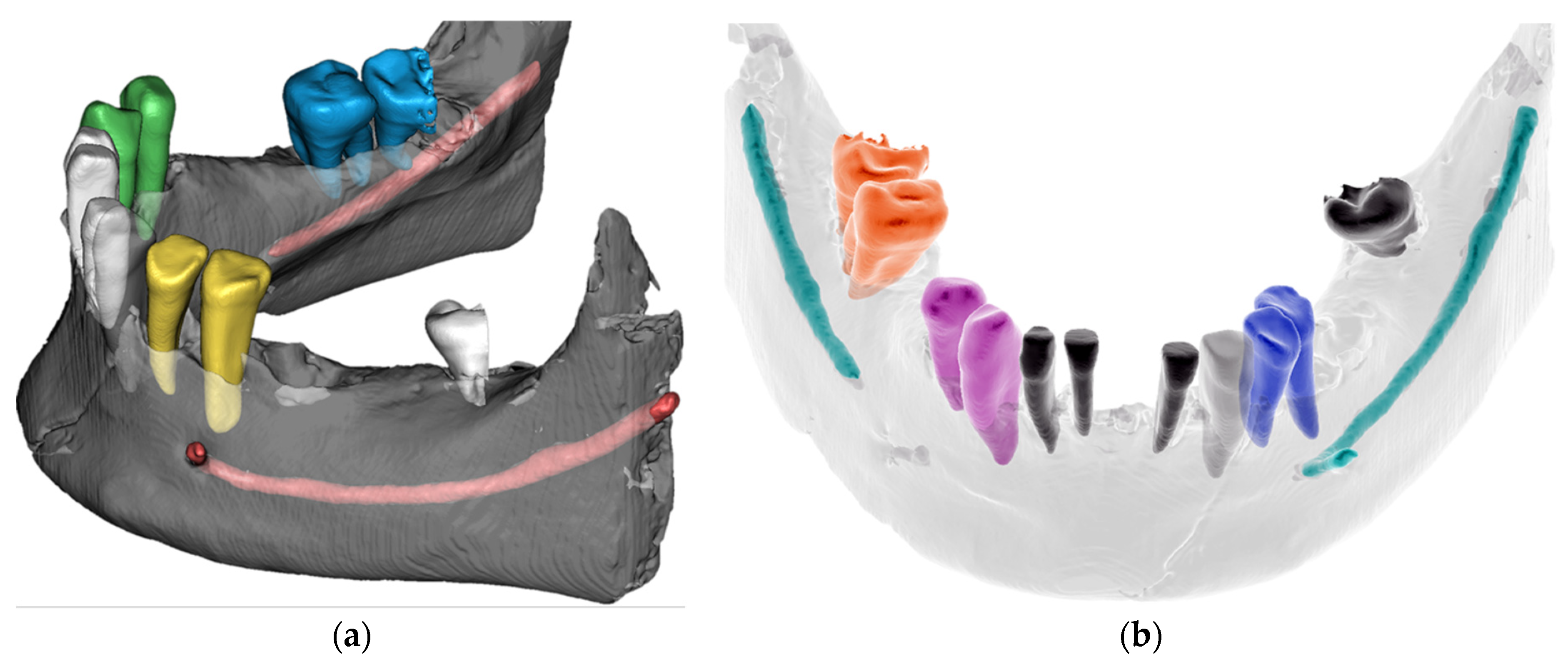
- CBCT and micro-CT technologies were used for the 3D reconstruction of dental patterns and descriptive morphological evaluation;
- ATR-FTIR spectroscopy was utilized to investigate the changes in dental restorations;
- The advanced AI–CNN algorithm was utilized for automated mandible segmentation;
- This research provides an unprecedented 3D morphological set of four stages of degradation of human mandibular bone and teeth presented in five different regions.
2. Materials and Methods
2.1. Materials
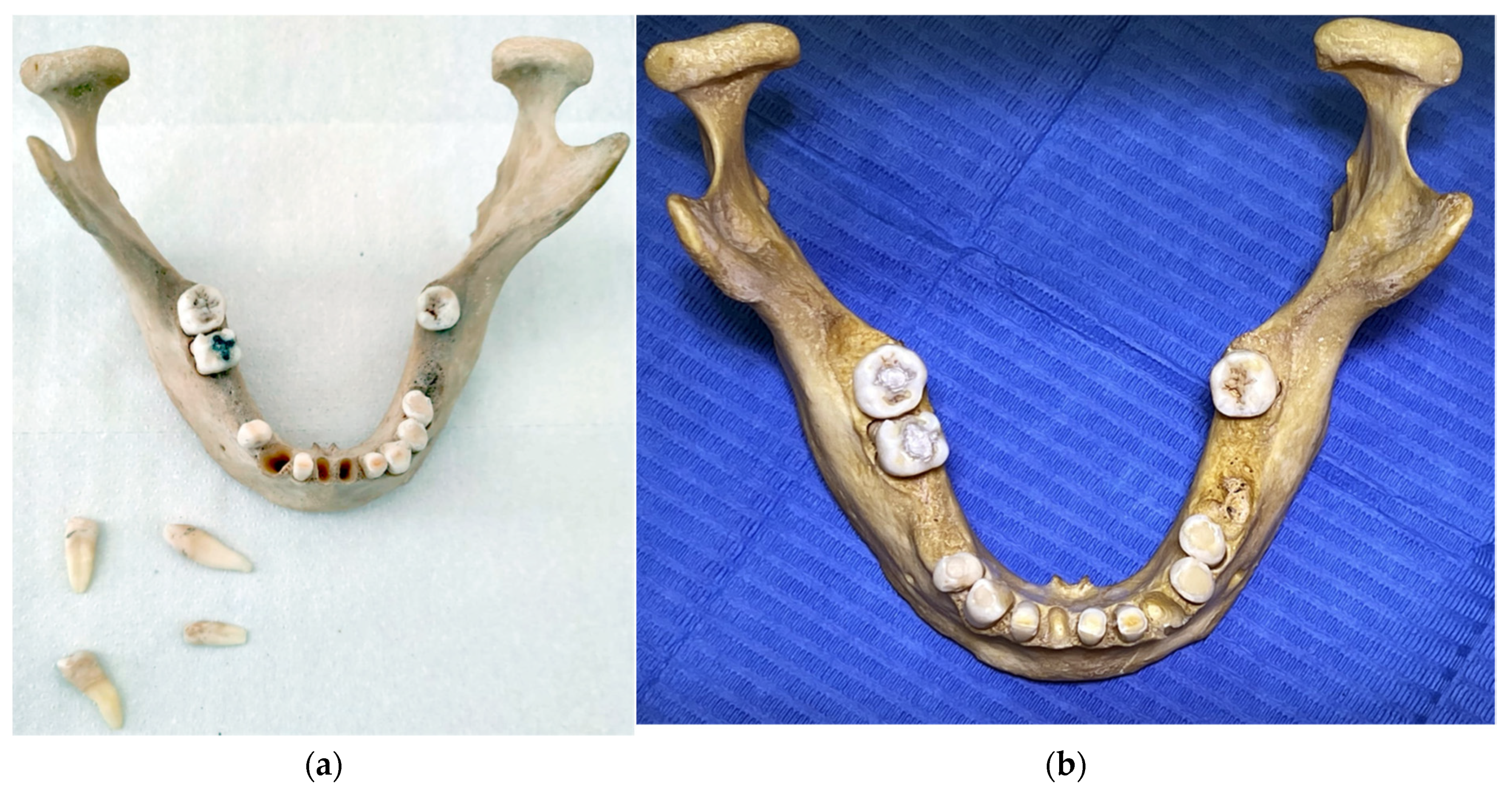
2.1.1. The Bone of Human Mandible with Teeth
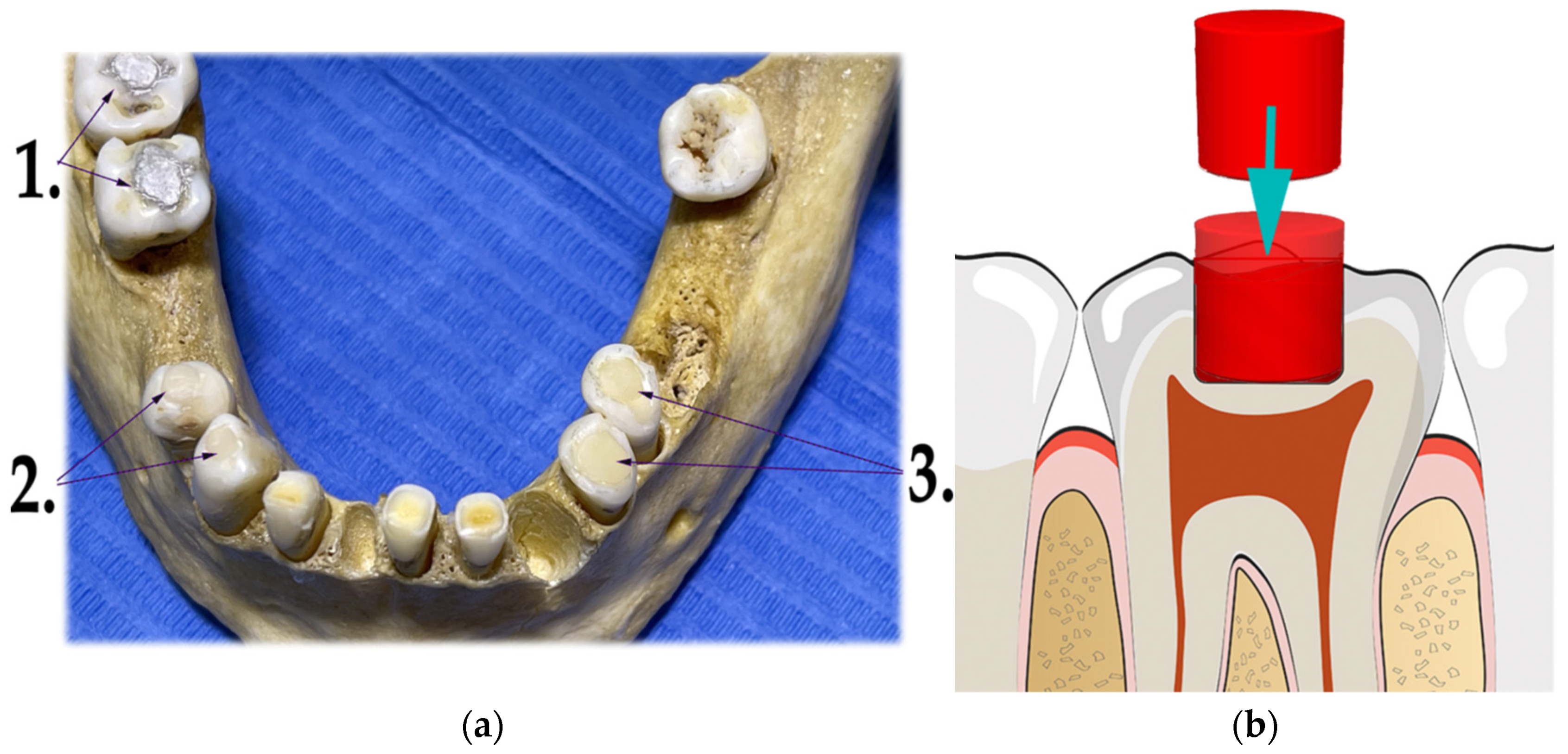
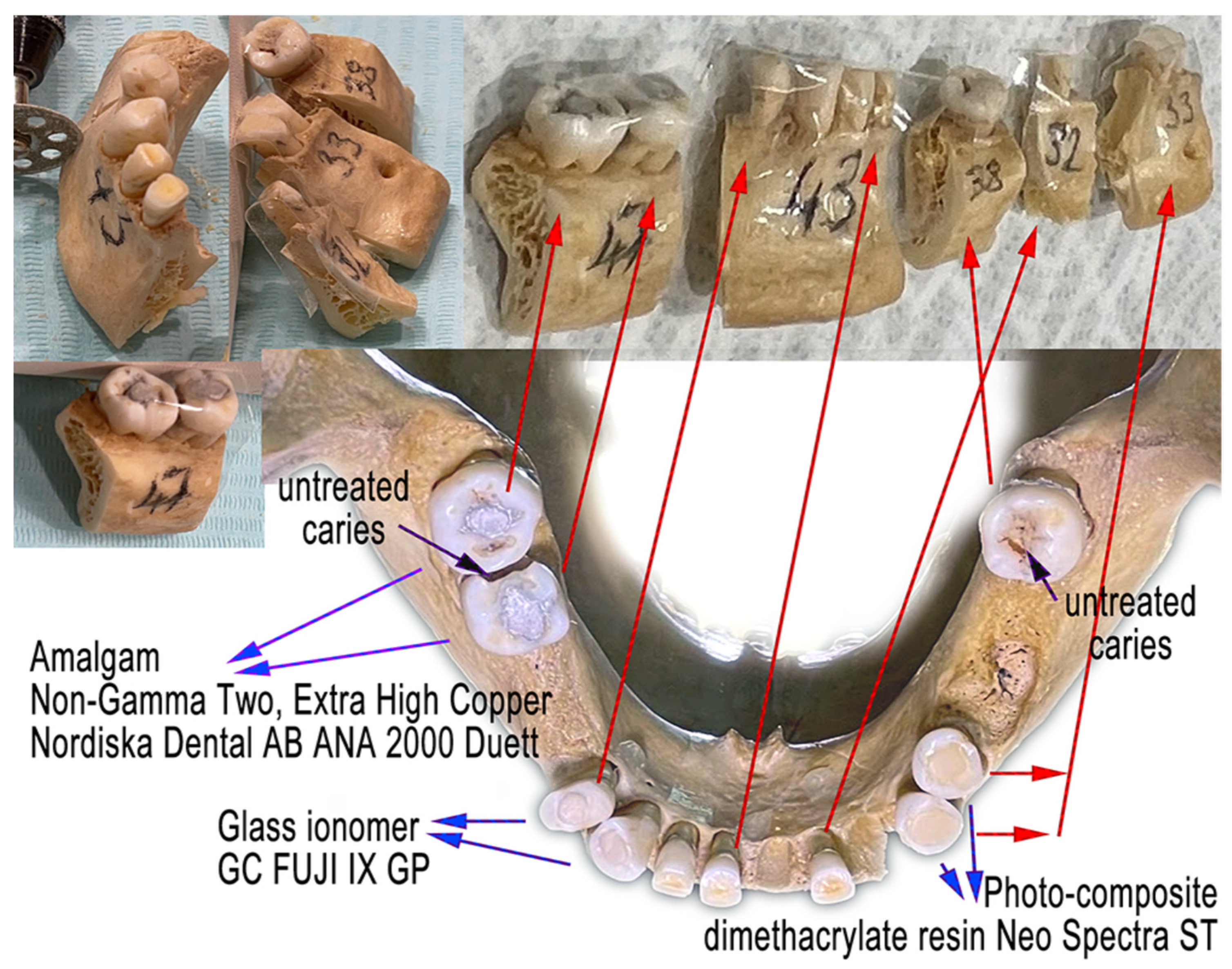
2.1.2. Various Dental Materials
- Dental amalgam—Ana 2000 capsules non-gamma-two, extra-high copper (containing 43% silver, 26.1% copper, 30.8% tin);
- Glass ionomer—GC FUJI IX GP wear-resistant multipurpose (containing powder: 95% Fluro alumino silicate glass, 5% Polyacrylic acid powder; liquid: 40% Polyacrylic acid and tartaric acid, 50% distilled water, 10% Polybasic carboxylic acid);
- Dental composite—Neo Spectra ST (containing methacrylate-modified polysiloxane, dimethacrylate resins, fluorescent pigment, UV stabilizer, Camphorquinone, Ethyl-4 (dimethylamino)benzoate, Bis (4-methyl-phenyl) iodonium hexafluorophosphate, Barium–aluminium–borosilicate glass, Ytterbium fluoride, iron-oxide pigments and titanium-oxide pigments, according to shade). Prime and Bond Universal were used as an adhesive system in the dental filling/restorations with a composite.
2.2. Methods
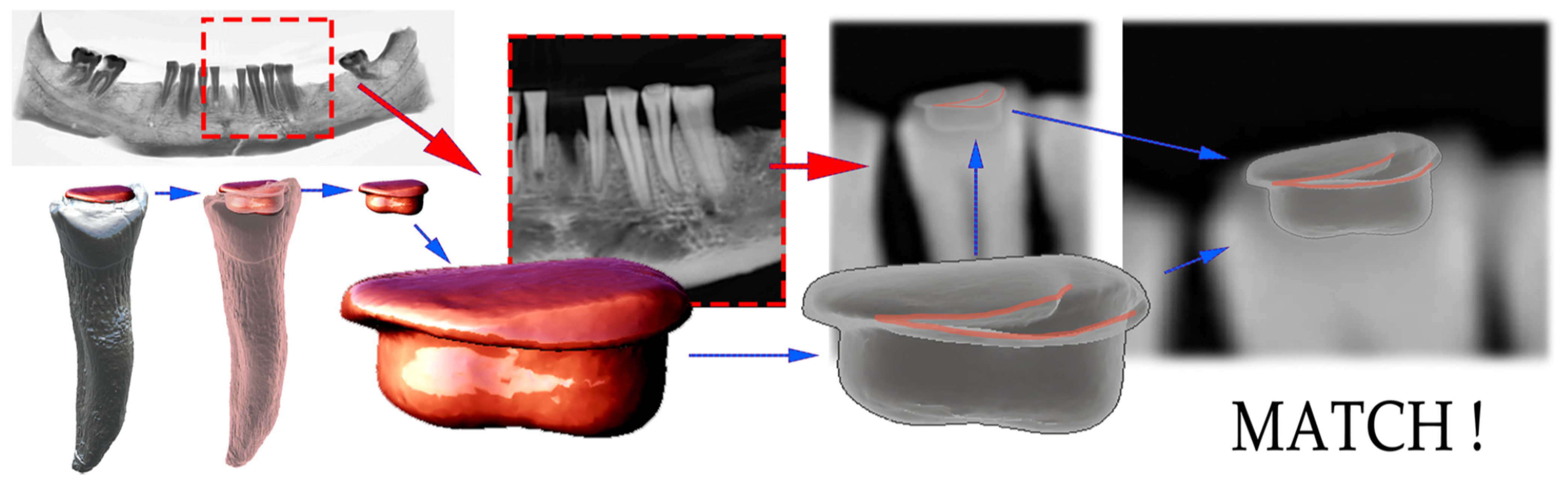
- The 2D shape of each dental filling was extracted graphically from the panoramic X-ray 2D image;
- The outer contours and inner contours with shades of gray gradient were identified, thus creating a unique grayscale image pattern with contours;
- The 3D-CBCT dental fillings were segmented and extracted from the tooth;
- The semitranslucent 3D model from the CBCT of each dental filling was transposed over each 2D unique grayscale image pattern with contours in supposed positions;
- In the basic match, a viewer’s perspective was adapted to achieve an exact match.
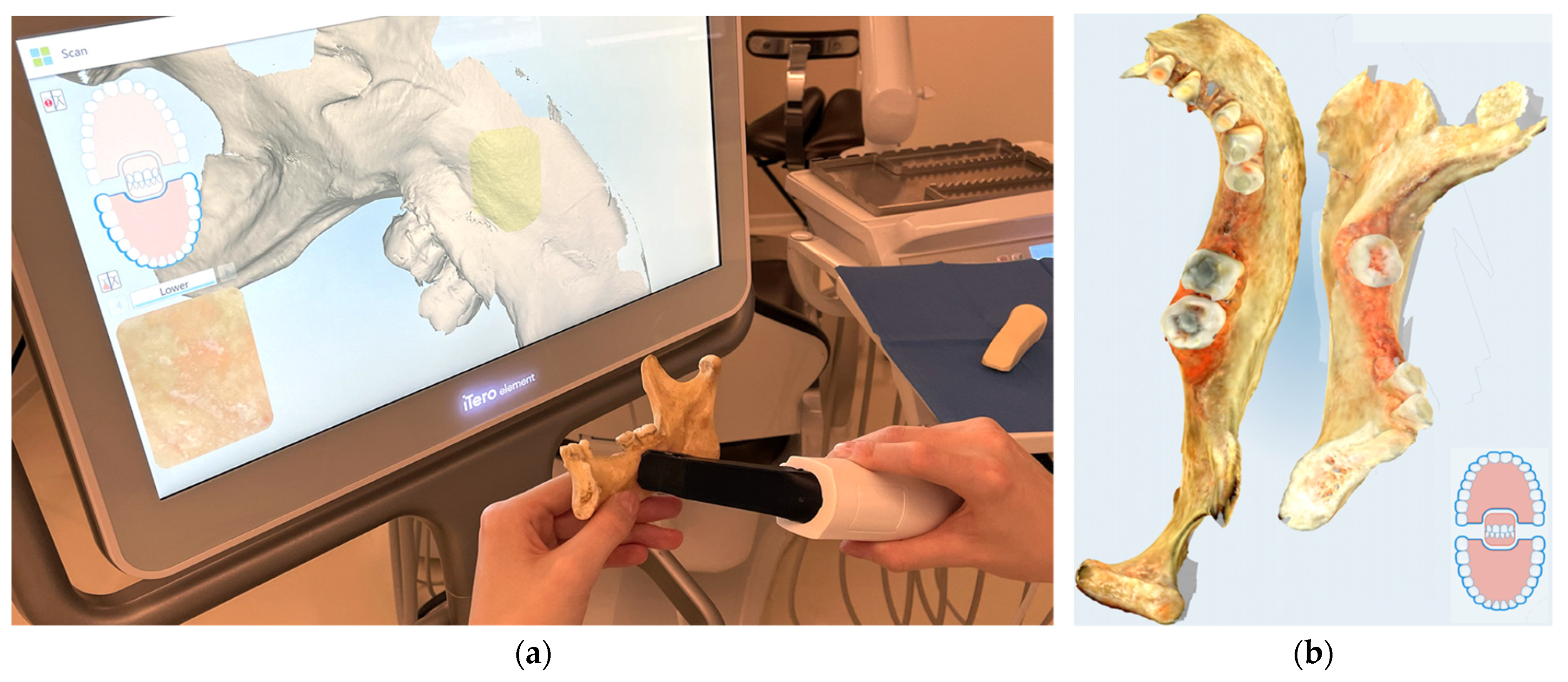
2.3. Digital Optical Scanning
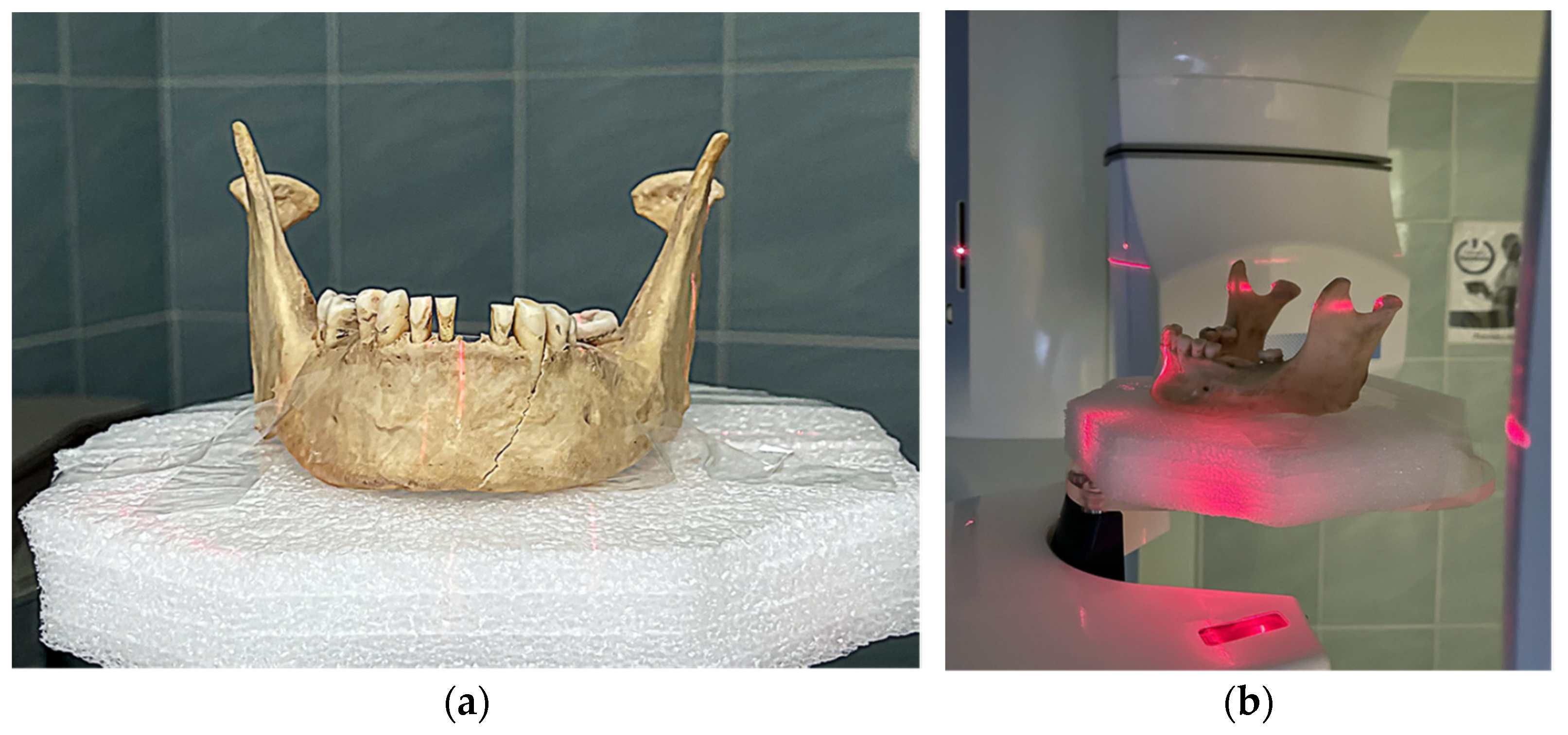
2.4. CBCT Scanning
- -
- A panoramic exposure with the following settings and values: 2D panoramic, standard, patient size M = medium-sized adult, 67 kV, 11 mA, 15 s;
- -
- The 3D exposure was performed with the following settings: CBCT volume Ø100 × 100 in a high-definition (HD) mode, voxel size 150 μm;
- -
- Two pairs of OPG and CBCT were created. The first scan was before the teeth preparative treatment, and the final scan was after the dental filling/restoration.
2.5. STL Segmentation
2.6. Micro-CT Scanning
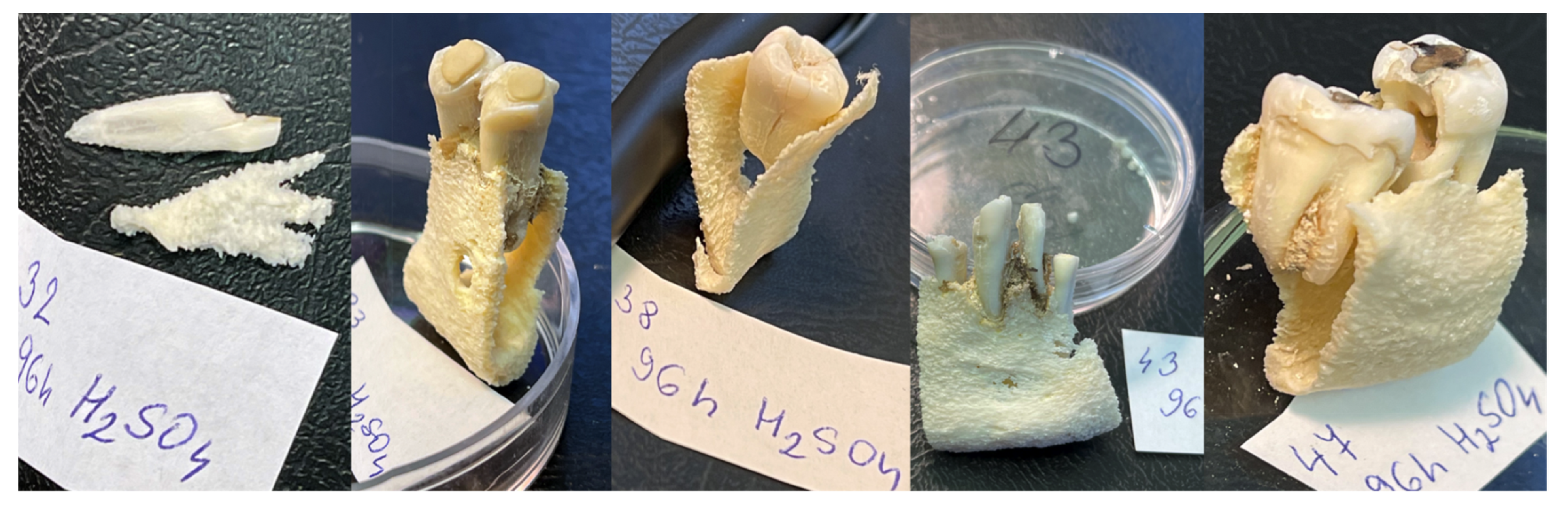
2.7. Acid Exposure
2.8. FTIR Spectroscopy
3. Results
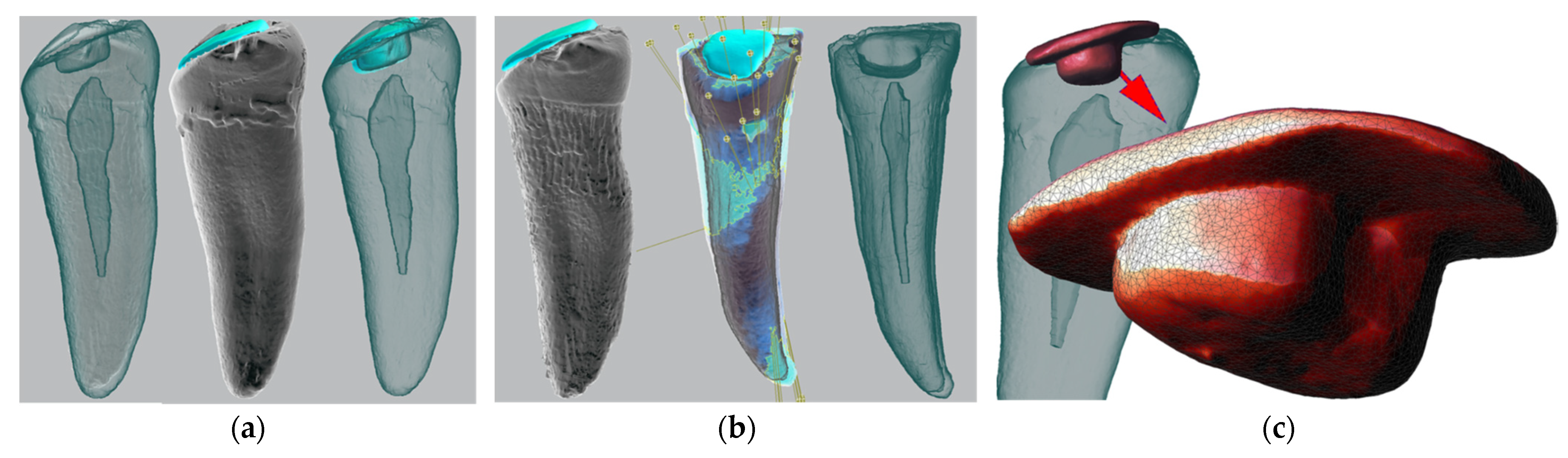
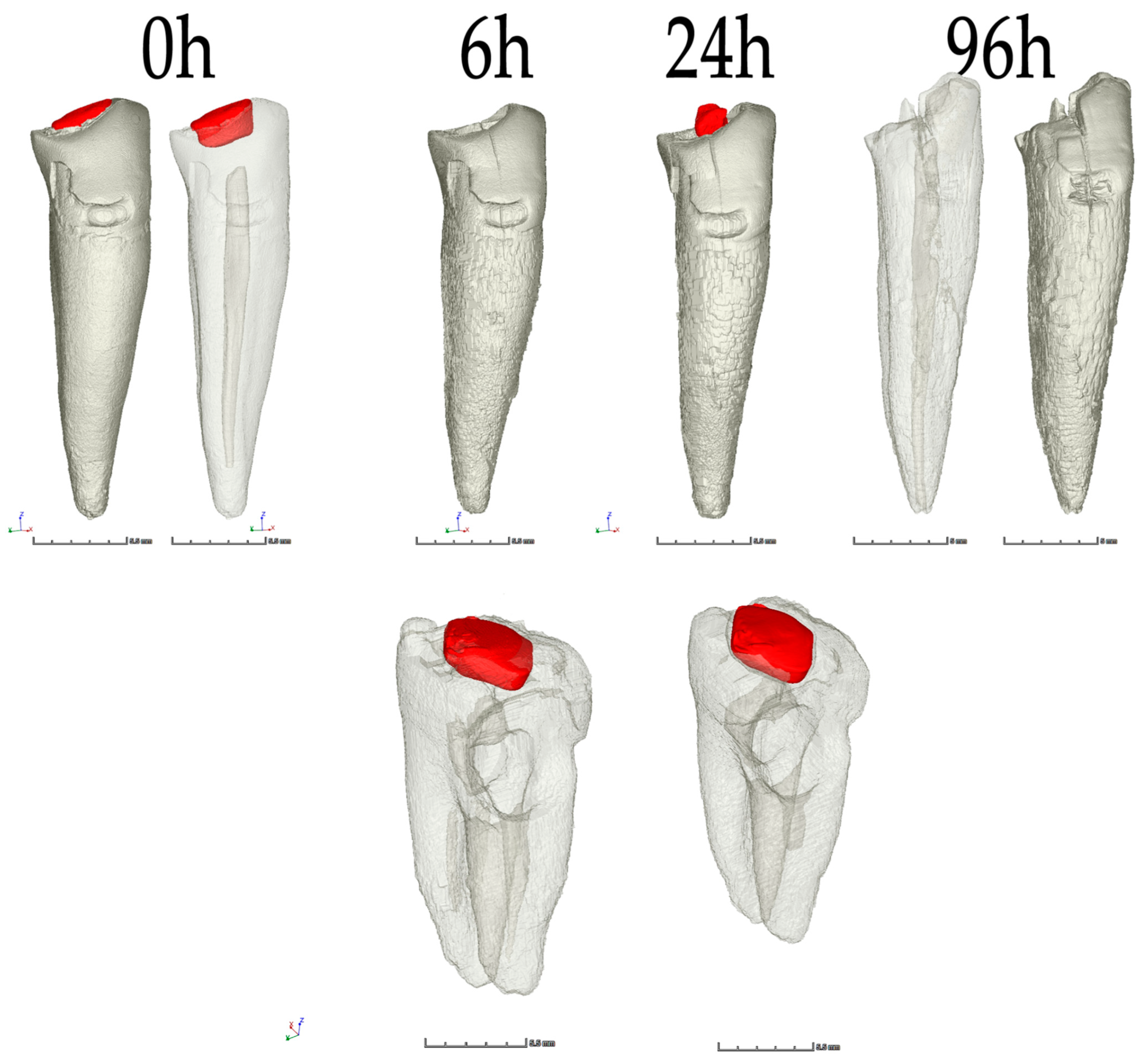
3.1. Descriptive Morphological Evaluation Based on Micro-CT Analysis
3.2. Digital Matching and AI Implementation in CBCT Segmentation
3.3. ATR-FTIR Spectroscopy
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A



References
- Ata-Ali, J.; Ata-Ali, F. Forensic Dentistry in Human Identification: A Review of the Literature. J. Clin. Exp. Dent. 2014, 6, e162–e167. [Google Scholar] [CrossRef] [PubMed]
- Martin-de-las-Heras, S.; Valenzuela, A.; de Dios Luna, J.; Bravo, M. The Utility of Dental Patterns in Forensic Dentistry. Forensic. Sci. Int. 2010, 195, 166.e1–166.e5. [Google Scholar] [CrossRef] [PubMed]
- Latham, K.E.; Bartelink, E.J.; Finnegan, M. New Perspectives in Forensic Human Skeletal Identification. In New Perspectives in Forensic Human Skeletal Identification; Academic Press: Cambridge, MA, USA, 2017; pp. 1–356. [Google Scholar]
- Sowmya, K.; Sudheendra, U.; Khan, S.; Nagpal, N.; Prathamesh, S. Assessment of Morphological Changes and DNA Quantification: An in Vitro Study on Acid-Immersed Teeth. J. Forensic Dent. Sci. 2013, 5, 42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Symes, S.A.; Rainwater, C.W.; Chapman, E.N.; Gipson, D.R.; Piper, A.L. Patterned Thermal Destruction of Human Remains in A Forensic Setting. In The Analysis of Burned Human Remains; Elsevier: Amsterdam, The Netherlands, 2008; pp. 15–20. [Google Scholar]
- Corte-Real, A.; Anjos, M.J.; Vieira, D.N.; Gamero, J.J. The Tooth for Molecular Analysis and Identification: A Forensic Approach. J. Forensic Odonto-Stomatol. 2012, 30, 22–28. [Google Scholar]
- Papaioannou, A.; Zorba, G.K.; Chrysostomou, P.; Balman, M. An Integrated Multidisciplinary Approach to Resolve Long-Standing Unidentified Human Skeletal Remains in Cyprus. Forensic Sci. Int. 2021, 320, 110679. [Google Scholar] [CrossRef]
- Grévin, G.; Bailet, P.; Quatrehomme, G.; Ollier, A. Anatomical Reconstruction of Fragments of Burned Human Bones: A Necessary Means for Forensic Identification. Forensic Sci. Int. 1998, 96, 129–134. [Google Scholar] [CrossRef]
- Mahfouz, M.R.; Mustafa, A.; Abdel Fatah, E.E.H.; Herrmann, N.P.; Langley, N.R. Computerized Reconstruction of Fragmentary Skeletal Remains. Forensic Sci. Int. 2017, 275, 212–223. [Google Scholar] [CrossRef]
- Ebert, L.C.; Rahbani, D.; Lüthi, M.; Thali, M.J.; Christensen, A.M.; Fliss, B. Reconstruction of Full Femora from Partial Bone Fragments for Anthropological Analyses Using Statistical Shape Modeling. Forensic Sci. Int. 2022, 332, 111196. [Google Scholar] [CrossRef]
- Deng, Q.; Zhou, M.; Wu, Z.; Shui, W.; Ji, Y.; Wang, X.; Liu, C.Y.J.; Huang, Y.; Jiang, H. A Regional Method for Craniofacial Reconstruction Based on Coordinate Adjustments and a New Fusion Strategy. Forensic Sci. Int. 2016, 259, 19–31. [Google Scholar] [CrossRef]
- Malfroy Camine, L.; Varlet, V.; Campana, L.; Grabherr, S.; Moghaddam, N. The Big Puzzle: A Critical Review of Virtual Re-Association Methods for Fragmented Human Remains in a DVI Context’. Forensic Sci. Int. 2022, 330, 111033. [Google Scholar] [CrossRef]
- Scott, G.R.; Pilloud, M.A.; Navega, D.; d’Oliveira, C.J.; Cunha, E.; Irish, J.D. RASUDAS: A New Web-Based Application for Estimating Ancestry from Tooth Morphology. Forensic Anthropol. 2018, 1, 18–31. [Google Scholar] [CrossRef] [Green Version]
- David, T.J.; Lewis, J.M. Forensic Odontology: Principles and Practice. Forensic Odontol. Princ. Pract. 2018, 1–320. [Google Scholar] [CrossRef]
- Lee, C.; Lim, S.H.; Huh, K.H.; Han, S.S.; Kim, J.E.; Heo, M.S.; Yi, W.J.; Lee, S.S.; Choi, S.C. Performance of Dental Pattern Analysis System with Treatment Chronology on Panoramic Radiography. Forensic Sci. Int. 2019, 299, 229–234. [Google Scholar] [CrossRef]
- Lucas, V.S.; McDonald, F.; Andiappan, M.; Roberts, G. Dental Age Estimation—Root Pulp Visibility (RPV) Patterns: A Reliable Mandibular Maturity Marker at the 18 Year Threshold. Forensic Sci. Int. 2017, 270, 98–102. [Google Scholar] [CrossRef] [PubMed]
- Acharya, A.B.; Taylor, J.A. Are a Minimum Number of Concordant Matches Needed to Establish Identity in Forensic Odontology? J. Forensic Odontostomatol. 2003, 21, 6–13. [Google Scholar] [PubMed]
- Sand, L.P.; Rasmusson, L.G.; Borrman, H. Accuracy of Dental Registrations in Forensic Odontology among Dentists and Dental Students. J. Forensic Odontostomatol. 1994, 12, 12–14. [Google Scholar] [PubMed]
- Bush, M.A.; Miller, R.G.; Prutsman-Pfeiffer, J.; Bush, P.J. Identification through X-Ray Fluorescence Analysis of Dental Restorative Resin Materials: A Comprehensive Study of Noncremated, Cremated, and Processed-Cremated Individuals. J. Forensic Sci. 2007, 52, 157–165. [Google Scholar] [CrossRef]
- Franco, A.; Willems, G.; Souza, P.H.C.; Bekkering, G.E.; Thevissen, P. The Uniqueness of the Human Dentition as Forensic Evidence: A Systematic Review on the Technological Methodology. Int. J. Legal. Med. 2015, 129, 1277–1283. [Google Scholar] [CrossRef]
- Pretty, I.A. Forensic Dentistry: 1. Identification of Human Remains. Dent. Update 2007, 34, 621–634. [Google Scholar] [CrossRef]
- Franco, A.; Willems, G.; Couto Souza, P.H.; Coucke, W.; Thevissen, P. Three-Dimensional Validation of the Impact of the Quantity of Teeth or Tooth Parts on the Morphological Difference between Twin Dentitions. J. Forensic Odontostomatol. 2016, 34, 27–37. [Google Scholar]
- Franco, A.; Willems, G.; Souza, P.H.C.; Tanaka, O.M.; Coucke, W.; Thevissen, P. Three-Dimensional Analysis of the Uniqueness of the Anterior Dentition in Orthodontically Treated Patients and Twins. Forensic Sci. Int. 2017, 273, 80–87. [Google Scholar] [CrossRef] [PubMed]
- Kadashetti, V.; Shivakumar, K.; Baad, R.; Vibhute, N.; Belgaumi, U.; Bommanavar, S.; Kamate, W. Effect of Concentrated Acids on Teeth: A Forensic Approach; An In-Vitro Study. J. Datta Meghe Inst. Med. Sci. Univ. 2021, 16, 283. [Google Scholar] [CrossRef]
- Guendalina, G.; Stefano, T.; Salvatore, A.; Paolo, B.; Giorgia, B.; Ilaria, G.; Riccardo, Z. Analysis of the Corrosive Effects of Hydrochloric Acid (HCl) on Human Bone: Preliminary Microscopic Study and Observations for Forensic Purposes. Forensic Sci. Int. 2021, 329, 111095. [Google Scholar] [CrossRef]
- Jackowski, C. Special Issue on Postmortem Imaging 2013. Forensic Sci. Int. 2013, 225, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Jackowski, C. Invited Commentary on Diagnostic Accuracy of Postmortem Computed Tomography, Magnetic Resonance Imaging, and Computed Tomography-Guided Biopsies for the Detection of Ischaemic Heart Disease in a Hospital Setting. Eur. Heart J. Cardiovasc. Imaging 2018, 19, 729. [Google Scholar] [CrossRef]
- Sarment, D.P.; Christensen, A.M. The Use of Cone Beam Computed Tomography in Forensic Radiology. J. Forensic Radiol. Imaging 2014, 2, 173–181. [Google Scholar] [CrossRef]
- Trochesset, D.A.; Serchuk, R.B.; Colosi, D.C. Generation of Intra-Oral-like Images from Cone Beam Computed Tomography Volumes for Dental Forensic Image Comparison. J. Forensic Sci. 2014, 59, 510–513. [Google Scholar] [CrossRef]
- Damera, A.; Mohanalakhsmi, J.; Yellarthi, P.; Rezwana, B. Radiographic Evaluation of Mandibular Ramus for Gender Estimation: Retrospective Study. J. Forensic Dent. Sci. 2016, 8, 74. [Google Scholar] [CrossRef] [Green Version]
- Lucena, J.; Mora, E.; Rodriguez, L.; Muñoz, M.; Cantin, M.G.; Fonseca, G.M. Cone Beam Computed Tomography (CBCT) as a Tool for the Analysis of Nonhuman Skeletal Remains in a Medico-Legal Setting. Forensic Sci. Int. 2016, 266, e32–e37. [Google Scholar] [CrossRef]
- Rutty, G.N.; Brough, A.; Biggs, M.J.P.; Robinson, C.; Lawes, S.D.A.; Hainsworth, S.V. The Role of Micro-Computed Tomography in Forensic Investigations. Forensic Sci. Int. 2013, 225, 60–66. [Google Scholar] [CrossRef]
- Wang, Q.; Zhang, Y.; Lin, H.; Zha, S.; Fang, R.; Wei, X.; Fan, S.; Wang, Z. Estimation of the Late Postmortem Interval Using FTIR Spectroscopy and Chemometrics in Human Skeletal Remains. Forensic Sci. Int. 2017, 281, 113–120. [Google Scholar] [CrossRef] [PubMed]
- Chophi, R.; Sharma, S.; Singh, R. Forensic Analysis of Red Lipsticks Using ATR-FTIR Spectroscopy and Chemometrics. Forensic Chem. 2020, 17, 100209. [Google Scholar] [CrossRef]
- Delgadoi, A.N.H.S.; Young, A.M. Methacrylate Peak Determination and Selection Recommendations Using ATR-FTIR to Investigate Polymerisation of Dental Methacrylate Mixtures. PLoS ONE 2021, 16, e0252999. [Google Scholar] [CrossRef] [PubMed]
- Thurzo, A.; Kosnáčová, H.S.; Kurilová, V.; Kosmeľ, S.; Beňuš, R.; Moravanský, N.; Kováč, P.; Kuracinová, K.M.; Palkovič, M.; Varga, I. Use of Advanced Artificial Intelligence in Forensic Medicine, Forensic Anthropology and Clinical Anatomy. Healthcare 2021, 9, 1545. [Google Scholar] [CrossRef]
- Reesu, G.V.; Mânica, S.; Revie, G.F.; Brown, N.L.; Mossey, P.A. Forensic Dental Identification Using Two-Dimensional Photographs of a Smile and Three-Dimensional Dental Models: A 2D-3D Superimposition Method. Forensic Sci. Int. 2020, 313, 110361. [Google Scholar] [CrossRef]
- Pinchi, V.; Norelli, G.A.; Caputi, F.; Fassina, G.; Pradella, F.; Vincenti, C. Dental Identification by Comparison of Antemortem and Postmortem Dental Radiographs: Influence of Operator Qualifications and Cognitive Bias. Forensic Sci. Int. 2012, 222, 252–255. [Google Scholar] [CrossRef]
- Izham, A.; Auerkari, E.I. The Use of Radiology CBCT in Odontology Forensic. AIP Conf. Proc. 2021, 2344, 050012. [Google Scholar] [CrossRef]
- Qiu, B.; van der Wel, H.; Kraeima, J.; Glas, H.H.; Guo, J.; Borra, R.J.H.; Witjes, M.J.H.; van Ooijen, P.M.A. Mandible Segmentation of Dental CBCT Scans Affected by Metal Artifacts Using Coarse-to-Fine Learning Model. J. Pers. Med. 2021, 11, 560. [Google Scholar] [CrossRef]
- Pinchi, V.; Pradella, F.; Buti, J.; Baldinotti, C.; Focardi, M.; Norelli, G.A. A New Age Estimation Procedure Based on the 3D CBCT Study of the Pulp Cavity and Hard Tissues of the Teeth for Forensic Purposes: A Pilot Study. J. Forensic Leg. Med. 2015, 36, 150–157. [Google Scholar] [CrossRef]
- Issrani, R.; Prabhu, N.; Sghaireen, M.G.; Ganji, K.K.; Mosfer, A.; Alqahtani, A.; Aljamaan, S.; Alanazi, A.M.; Alanazi, S.H.; Alam, M.K.; et al. Cone-Beam Computed Tomography: A New Tool on the Horizon for Forensic Dentistry. Int. J. Environ. Res. Public Health 2022, 19, 5352. [Google Scholar] [CrossRef]
- Gaêta-Araujo, H.; Nascimento, E.H.L.; Brasil, D.M.; Madlum, D.V.; Haiter-Neto, F.; Oliveira-Santos, C. Influence of Reconstruction Parameters of Micro-Computed Tomography on the Analysis of Bone Mineral Density. Imaging Sci. Dent. 2020, 50, 153. [Google Scholar] [CrossRef] [PubMed]
- Ezhov, M.; Gusarev, M.; Golitsyna, M.; Yates, J.M.; Kushnerev, E.; Tamimi, D.; Aksoy, S.; Shumilov, E.; Sanders, A.; Orhan, K. Clinically Applicable Artificial Intelligence System for Dental Diagnosis with CBCT. Sci. Rep. 2021, 11, 15006. [Google Scholar] [CrossRef] [PubMed]
- Mudrak Jörg Artificial Intelligence and Deep Learning in Dental Radiology. Available online: https://www.oralhealthgroup.com/features/artificial-intelligence-and-deep-learning-in-dental-radiology-a-way-forward-in-point-of-care-radiology/ (accessed on 28 December 2021).
- Baig, Z.; Khan, M.A.; Mohammad, N.; Ben Brahim, G. Drone Forensics and Machine Learning: Sustaining the Investigation Process. Sustainability 2022, 14, 4861. [Google Scholar] [CrossRef]
- Lebon, M.; Zazzo, A.; Reiche, I. Screening in Situ Bone and Teeth Preservation by ATR-FTIR Mapping. Palaeogeogr. Palaeoclimatol. Palaeoecol. 2014, 416, 110–119. [Google Scholar] [CrossRef]
- France, C.A.M.; Sugiyama, N.; Aguayo, E. Establishing a Preservation Index for Bone, Dentin, and Enamel Bioapatite Mineral Using ATR-FTIR. J. Archaeol. Sci. Rep. 2020, 33, 102551. [Google Scholar] [CrossRef]
- Orhan, K.; Bayrakdar, I.S.; Ezhov, M.; Kravtsov, A.; Özyürek, T. Evaluation of Artificial Intelligence for Detecting Periapical Pathosis on Cone-Beam Computed Tomography Scans. Int. Endod. J. 2020, 53, 680–689. [Google Scholar] [CrossRef]
- Orhan, K.; Bilgir, E.; Bayrakdar, I.S.; Ezhov, M.; Gusarev, M.; Shumilov, E. Evaluation of Artificial Intelligence for Detecting Impacted Third Molars on Cone-Beam Computed Tomography Scans. J. Stomatol. Oral Maxillofac. Surg. 2021, 122, 333–337. [Google Scholar] [CrossRef]
- Bayrakdar, S.K.; Orhan, K.; Bayrakdar, I.S.; Bilgir, E.; Ezhov, M.; Gusarev, M.; Shumilov, E. A Deep Learning Approach for Dental Implant Planning in Cone-Beam Computed Tomography Images. BMC Med. Imaging 2021, 21, 86. [Google Scholar] [CrossRef]
- Ciglanská, M.; Jančovičová, V.; Havlínová, B.; Machatová, Z.; Brezová, V. The Influence of Pollutants on Accelerated Ageing of Parchment with Iron Gall Inks. J. Cult. Herit. 2014, 15, 373–381. [Google Scholar] [CrossRef]
- Legan, L.; Leskovar, T.; Črešnar, M.; Cavalli, F.; Innocenti, D.; Ropret, P. Non-Invasive Reflection FTIR Characterization of Archaeological Burnt Bones: Reference Database and Case Studies. J. Cult. Herit. 2020, 41, 13–26. [Google Scholar] [CrossRef]
- De Carvalho Almança Lopes, C.; Limirio, P.H.J.O.; Novais, V.R.; Dechichi, P. Fourier Transform Infrared Spectroscopy (FTIR) Application Chemical Characterization of Enamel, Dentin and Bone. Appl. Spectrosc. Rev. 2018, 53, 747–769. [Google Scholar] [CrossRef]
- Trapp, B.M. The Effects of Household Corrosive Substances on Restored and Non-Restored Teeth. Master’s Thesis, School of Medicine, Boston University, Boston, MA, USA, 2018. Available online: https://open.bu.edu/ds2/stream/?#/documents/252372/page/13 (accessed on 12 April 2022).
- Trapp, B.M.; Tallman, S.D. The Effects of Household Corrosive Substances on Silver Amalgam and Porcelain-Fused-to-Metal Restorations and Non-Restored Teeth. Forensic Sci. Int. 2018, 293, 77–85. [Google Scholar] [CrossRef] [PubMed]
- Raj, M.; Boaz, K.; Srikant, N. Are Teeth Evidence in Acid Environment. J. Forensic Dent. Sci. 2013, 5, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mazza, A.; Merlati, G.; Savio, C.; Fassina, G.; Menghini, P.; Danesino, P. Observations on Dental Structures When Placed in Contact with Acids: Experimental Studies to Aid Identification Processes. J. Forensic Sci. 2005, 50, 1–5. [Google Scholar] [CrossRef]
- Vermeij, E.; Zoon, P.; van Wijk, M.; Gerretsen, R. Microscopic Residues of Bone from Dissolving Human Remains in Acids. J. Forensic Sci. 2015, 60, 770–776. [Google Scholar] [CrossRef] [PubMed]
- Vermeij, E. Going Down. New Sci. 2014, 224, 44–45. [Google Scholar] [CrossRef]
- Bernauer, S.A.; Zitzmann, N.U.; Joda, T. The Use and Performance of Artificial Intelligence in Prosthodontics: A Systematic Review. Sensors 2021, 21, 6628. [Google Scholar] [CrossRef]
- Müller, A.; Mertens, S.M.; Göstemeyer, G.; Krois, J.; Schwendicke, F. Barriers and Enablers for Artificial Intelligence in Dental Diagnostics: A Qualitative Study. J. Clin. Med. 2021, 10, 1612. [Google Scholar] [CrossRef]
- Bouletreau, P.; Makaremi, M.; Ibrahim, B.; Louvrier, A.; Sigaux, N. Artificial Intelligence: Applications in Orthognathic Surgery. J.Stomatol. Oral Maxillofac. Surg. 2019, 120, 347–354. [Google Scholar] [CrossRef]
- Pathak, M.; Narang, H. Himanshi Narang Application of Artificial Intelligence in the Field of Forensic Medicine. Indian J. Forensic Med. Toxicol. 2021, 15. [Google Scholar] [CrossRef]
- Van Rijn, R.R.; de Luca, A. Three Reasons Why Artificial Intelligence Might Be the Radiologist’s Best Friend. Radiology 2020, 296, 159–160. [Google Scholar] [CrossRef] [PubMed]
- Khanagar, S.B.; Vishwanathaiah, S.; Naik, S.; Al-Kheraif, A.A.; Devang Divakar, D.; Sarode, S.C.; Bhandi, S.; Patil, S. Application and Performance of Artificial Intelligence Technology in Forensic Odontology—A Systematic Review. Leg. Med. 2021, 48, 101826. [Google Scholar] [CrossRef] [PubMed]
- Makaremi, M.; Lacaule, C.; Mohammad-Djafari, A. Deep Learning and Artificial Intelligence for the Determination of the Cervical Vertebra Maturation Degree from Lateral Radiography. Entropy 2019, 21, 1222. [Google Scholar] [CrossRef] [Green Version]
- Almalki, Y.E.; Qayyum, A.; Irfan, M.; Haider, N.; Glowacz, A.; Alshehri, F.M.; Alduraibi, S.K.; Alshamrani, K.; Basha, M.A.A.; Alduraibi, A.; et al. A Novel Method for COVID-19 Diagnosis Using Artificial Intelligence in Chest X-Ray Images. Healthcare 2021, 9, 522. [Google Scholar] [CrossRef]
- Ren, K.; Li, N.; Liang, X.; Wang, L.; Li, J.; Sun, J. Investigating the New Orientation of Wound Age Estimation in Forensic Medicine Based on Biological Omics Data Combined with Artificial Intelligence Algorithms. Pervasive Health Pervasive Comput. Technol. Healthc. 2020, 54–59. [Google Scholar] [CrossRef]
- Li, L.; Qin, L.; Xu, Z.; Yin, Y.; Wang, X.; Kong, B.; Bai, J.; Lu, Y.; Fang, Z.; Song, Q.; et al. Using Artificial Intelligence to Detect COVID-19 and Community-Acquired Pneumonia Based on Pulmonary CT: Evaluation of the Diagnostic Accuracy. Radiology 2020, 296, E65–E71. [Google Scholar] [CrossRef]
- Thurzo, A.; Kurilová, V.; Varga, I. Artificial Intelligence in Orthodontic Smart Application for Treatment Coaching and Its Impact on Clinical Performance of Patients Monitored with AI-TeleHealth System. Healthcare 2021, 9, 1695. [Google Scholar] [CrossRef]
- Punyani, P.; Gupta, R.; Kumar, A. Neural Networks for Facial Age Estimation: A Survey on Recent Advances. Artif. Intell. Rev. 2019, 53, 3299–3347. [Google Scholar] [CrossRef]
- Silva, T.P.; Hughes, M.M.; dos Santos Menezes, L.; de Fátima Batista de Melo, M.; Takeshita, W.M.; de Freitas, P.H.L. Artificial Intelligence-Based Cephalometric Landmark Annotation and Measurements According to Arnett’s Analysis: Can We Trust a Bot to Do That? Dentomaxillofac. Radiol. 2021, 20200548. [Google Scholar] [CrossRef]
- Hamet, P.; Tremblay, J. Artificial Intelligence in Medicine. Metabolism 2017, 69, S36–S40. [Google Scholar] [CrossRef]
- Bewes, J.; Low, A.; Morphett, A.; Pate, F.D.; Henneberg, M. Artificial Intelligence for Sex Determination of Skeletal Remains: Application of a Deep Learning Artificial Neural Network to Human Skulls. J. Forensic Leg. Med. 2019, 62, 40–43. [Google Scholar] [CrossRef] [PubMed]
- Fang, Y.T.; Lan, Q.; Xie, T.; Liu, Y.F.; Mei, S.Y.; Zhu, B.F. New Opportunities and Challenges for Forensic Medicine in the Era of Artificial Intelligence Technology. Fa Yi Xue Za Zhi 2020, 36, 77–85. [Google Scholar] [CrossRef] [PubMed]
- Hung, K.; Montalvao, C.; Tanaka, R.; Kawai, T.; Bornstein, M.M. The Use and Performance of Artificial Intelligence Applications in Dental and Maxillofacial Radiology: A Systematic Review. Dentomaxillofacial Radiol. 2019, 49. [Google Scholar] [CrossRef] [PubMed]
- Tanikawa, C.; Yamashiro, T. Development of Novel Artificial Intelligence Systems to Predict Facial Morphology after Orthognathic Surgery and Orthodontic Treatment in Japanese Patients. Sci. Rep. 2021, 11, 15853. [Google Scholar] [CrossRef] [PubMed]
- Matsuda, S.; Yoshida, H.; Ebata, K.; Shimada, I.; Yoshimura, H. Forensic Odontology with Digital Technologies: A Systematic Review. J. Forensic Leg. Med. 2020, 74, 102004. [Google Scholar] [CrossRef] [PubMed]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Time (h) | 0 | 6 | 24 | 96 |
|---|---|---|---|---|
| Volume 0 h (mm3) | Volume 6 h (mm3) | Volume 24 h (mm3) | Volume 96 h (mm3) | |
| sample 32 | ||||
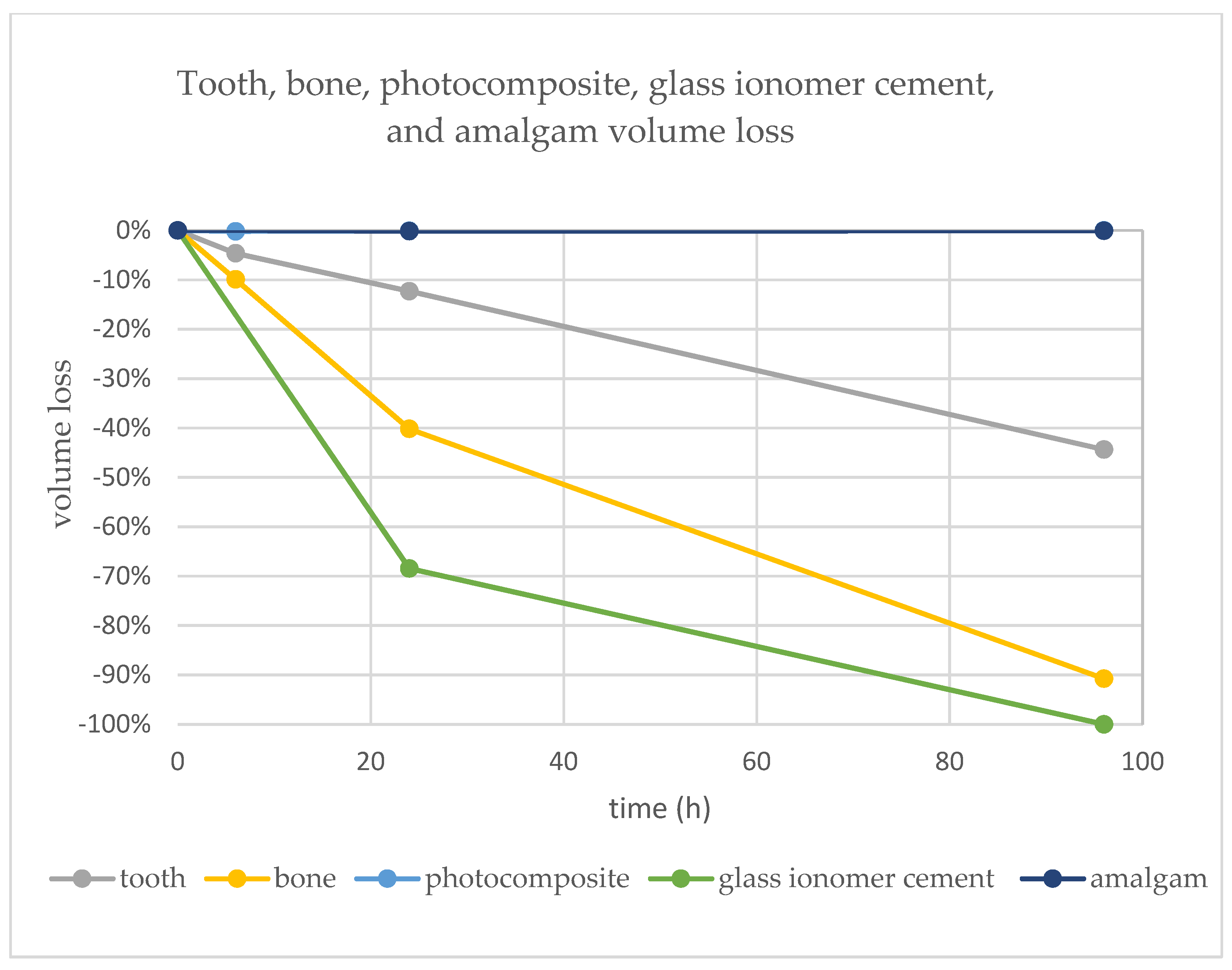
| dentine | 190.29 | 185.1 | 170.5 | 110.95 |
| percentage loss | 0.0% | −2.7% | −10.4% | −41.7% |
| enamel | 12.81 | 8.56 | 7.64 | 2.03 |
| percentage loss | 0.0% | −33.2% | −40.4% | −84.2% |
| tooth | 203.1 | 193.7 | 178.12 | 112.98 |
| percentage loss | 0.0% | −4.6% | −12.3% | −44.4% |
| bone | 668.1 | 601.85 | 399.56 | 61.77 |
| percentage loss | 0.0% | −9.9% | −40.2% | −90.8% |
| sample 33 | 324.45 | 299.16 | 290.64 | 270.57 |
| 0.0% | −7.8% | −10.4% | −16.6% | |
| Composite | 16.46 | 16.43 | 16.45 | 16.46 |
| 0.0% | −0.2% | −0.1% | 0.0% | |
| sample 43 | ||||
| glass ionomer | 11.57 | 1 | 3.65 | 0 |
| 0.0% | 1 | −68.5% | −100.0% | |
| sample 47 | ||||
| amalgam | 33.42 | 33.43 | 33.37 | 33.4 |
| 0.0% | 0.0% | −0.1% | −0.1% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thurzo, A.; Jančovičová, V.; Hain, M.; Thurzo, M.; Novák, B.; Kosnáčová, H.; Lehotská, V.; Varga, I.; Kováč, P.; Moravanský, N. Human Remains Identification Using Micro-CT, Chemometric and AI Methods in Forensic Experimental Reconstruction of Dental Patterns after Concentrated Sulphuric Acid Significant Impact. Molecules 2022, 27, 4035. https://doi.org/10.3390/molecules27134035
Thurzo A, Jančovičová V, Hain M, Thurzo M, Novák B, Kosnáčová H, Lehotská V, Varga I, Kováč P, Moravanský N. Human Remains Identification Using Micro-CT, Chemometric and AI Methods in Forensic Experimental Reconstruction of Dental Patterns after Concentrated Sulphuric Acid Significant Impact. Molecules. 2022; 27(13):4035. https://doi.org/10.3390/molecules27134035
Chicago/Turabian StyleThurzo, Andrej, Viera Jančovičová, Miroslav Hain, Milan Thurzo, Bohuslav Novák, Helena Kosnáčová, Viera Lehotská, Ivan Varga, Peter Kováč, and Norbert Moravanský. 2022. "Human Remains Identification Using Micro-CT, Chemometric and AI Methods in Forensic Experimental Reconstruction of Dental Patterns after Concentrated Sulphuric Acid Significant Impact" Molecules 27, no. 13: 4035. https://doi.org/10.3390/molecules27134035