
The Skeletal Effects of Tanshinones: A Review




Abstract
:1. Introduction
2. Results
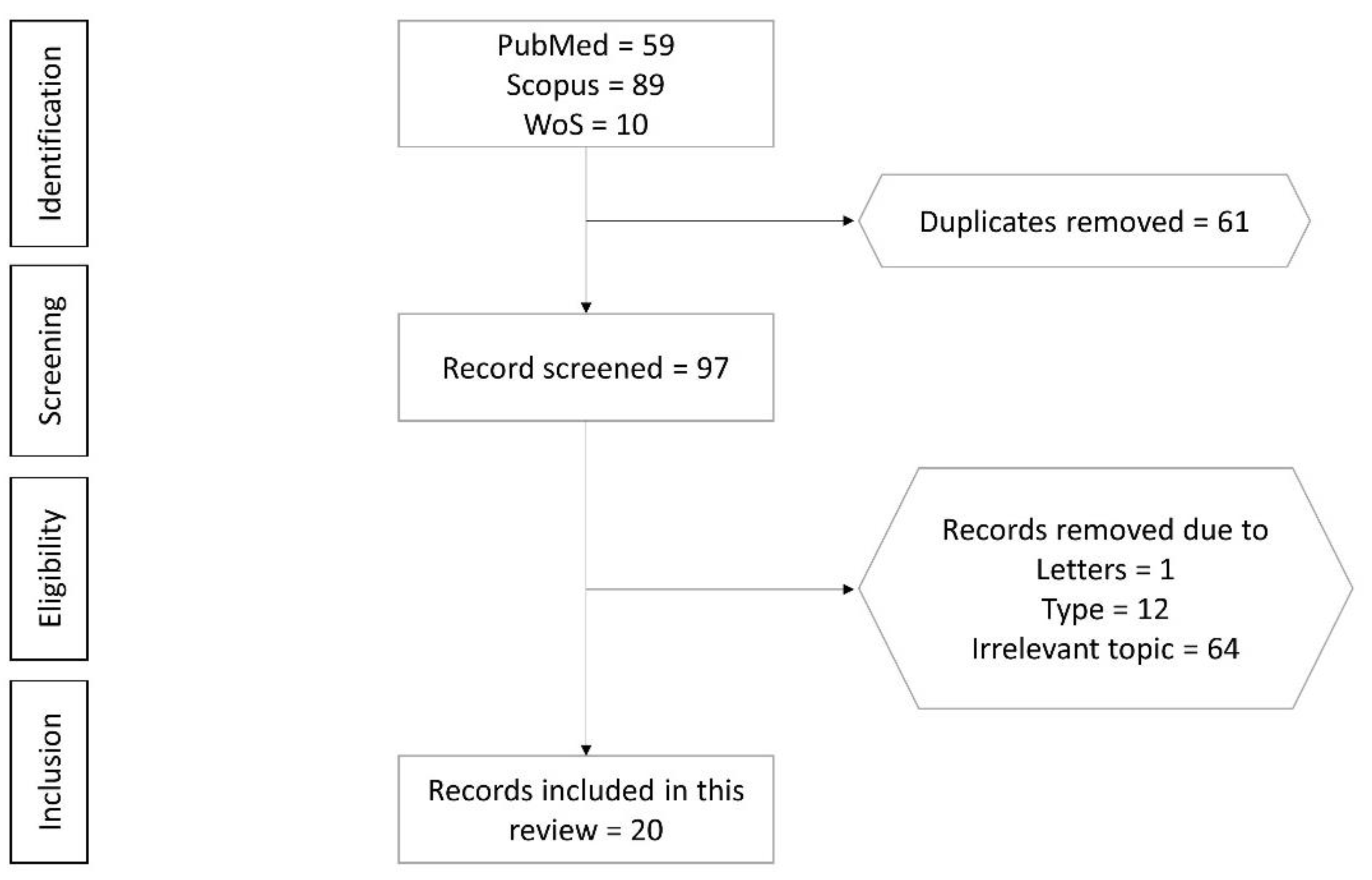
2.1. Selection of Articles
2.2. Study Characteristics
2.3. Results from Cell Culture Studies
2.4. Results from Animal Studies
3. Materials and Methods
3.1. Literature Review
3.2. Article Selection
3.3. Data Extraction
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Black, D.M.; Rosen, C.J. Postmenopausal Osteoporosis. N. Engl. J. Med. 2016, 374, 254–262. [Google Scholar] [CrossRef]
- Eastell, R.; O’Neill, T.W.; Hofbauer, L.C.; Langdahl, B.; Reid, I.R.; Gold, D.T.; Cummings, S.R. Postmenopausal osteoporosis. Nat. Rev. Dis. Prim. 2016, 2, 16069. [Google Scholar] [CrossRef]
- Deeks, E.D. Author Correction to: Denosumab: A Review in Postmenopausal Osteoporosis. Drugs Aging 2018, 35, 261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cosman, F.; De Beur, S.J.; LeBoff, M.S.; Lewiecki, E.M.; Tanner, B.; Randall, S.; Lindsay, R. Clinician’s Guide to Prevention and Treatment of Osteoporosis. Osteoporos. Int. 2014, 25, 2359–2381. [Google Scholar] [CrossRef] [Green Version]
- Jeremiah, M.P.; Unwin, B.K.; Greenawald, M.H.; Casiano, V.E. Diagnosis and Management of Osteoporosis. Am. Fam. Physician 2015, 92, 261–268. [Google Scholar] [PubMed]
- Odén, A.; McCloskey, E.V.; Kanis, J.A.; Harvey, N.C.; Johansson, H. Burden of high fracture probability worldwide: Secular increases 2010–2040. Osteoporos. Int. 2015, 26, 2243–2248. [Google Scholar] [CrossRef] [PubMed]
- Burge, R.; Dawson-Hughes, B.; Solomon, D.H.; Wong, J.B.; King, A.; Tosteson, A. Incidence and Economic Burden of Osteoporosis-Related Fractures in the United States, 2005-2025. J. Bone Miner. Res. 2006, 22, 465–475. [Google Scholar] [CrossRef]
- Camacho, P.M.; Petak, S.M.; Binkley, N.; Clarke, B.L.; Harris, S.T.; Hurley, D.L.; Kleerekoper, M.; Lewiecki, E.M.; Miller, P.D.; Narula, H.S.; et al. American Association of Clinical Endocrinologists and American College of Endocrinology Clinical Practice Guidelines for the Diagnosis and Treatment of Postmenopausal Osteoporosis—2016. Endocr. Pr. 2016, 22, 1–42. [Google Scholar] [CrossRef] [Green Version]
- Chapurlat, R.D.; Arlot, M.; Burt-Pichat, B.; Chavassieux, P.; Roux, J.P.; Portero-Muzy, N.; Delmas, P.D. Microcrack Frequency and Bone Remodeling in Postmenopausal Osteoporotic Women on Long-Term Bisphosphonates: A Bone Biopsy Study. J. Bone Miner. Res. 2007, 22, 1502–1509. [Google Scholar] [CrossRef]
- Stepan, J.J.; Burr, D.B.; Pavo, I.; Sipos, A.; Michalska, D.; Li, J.; Fahrleitner-Pammer, A.; Petto, H.; Westmore, M.; Michalsky, D.; et al. Low bone mineral density is associated with bone microdamage accumulation in postmenopausal women with osteoporosis. Bone 2007, 41, 378–385. [Google Scholar] [CrossRef]
- Chan, C.K.Y.; Mason, A.; Cooper, C.; Dennison, E. Novel advances in the treatment of osteoporosis. Br. Med Bull. 2016, 119, 129–142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peroni, A.; Zini, A.; Braga, V.; Colato, C.; Adami, S.; Girolomoni, G. Drug-induced morphea: Report of a case induced by balicatib and review of the literature. J. Am. Acad. Dermatol. 2008, 59, 125–129. [Google Scholar] [CrossRef] [PubMed]
- Rünger, T.M.; Quintanilla-Dieck, M.J.; Bhawan, J. Role of Cathepsin K in the Turnover of the Dermal Extracellular Matrix during Scar Formation. J. Investig. Dermatol. 2007, 127, 293–297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanaka, M.; Yamada, H.; Nishikawa, S.; Mori, H.; Ochi, Y.; Horai, N.; Li, M.; Amizuka, N. Joint Degradation in a Monkey Model of Collagen-Induced Arthritis: Role of Cathepsin K Based on Biochemical Markers and Histological Evaluation. Int. J. Rheumatol. 2016, 2016, 1–10. [Google Scholar] [CrossRef] [Green Version]
- McClung, M.R.; O’Donoghue, M.L.; Papapoulos, S.E.; Bone, H.; Langdahl, B.; Saag, K.G.; Reid, I.R.; Kiel, D.P.; Cavallari, I.; Bonaca, M.P.; et al. Odanacatib for the treatment of postmenopausal osteoporosis: Results of the LOFT multicentre, randomised, double-blind, placebo-controlled trial and LOFT Extension study. Lancet Diabetes Endocrinol. 2019, 7, 899–911. [Google Scholar] [CrossRef]
- Rongchen, D.; Wu, Z.; Chu, H.Y.; Lu, J.; Lyu, A.; Liu, J.; Zhang, G. Cathepsin K: The Action in and Beyond Bone. Front. Cell Dev. Biol. 2020, 8, 433. [Google Scholar] [CrossRef]
- Tang, B.M.P.; Eslick, G.D.; Nowson, C.; Smith, C.; Bensoussan, A. Use of calcium or calcium in combination with vitamin D supplementation to prevent fractures and bone loss in people aged 50 years and older: A meta-analysis. Lancet 2007, 370, 657–666. [Google Scholar] [CrossRef]
- The DIPART (Vitamin D Individual Patient Analysis of Randomized Trials) Group. Patient level pooled analysis of 68 500 patients from seven major vitamin D fracture trials in US and Europe. BMJ 2010, 340, b5463. [Google Scholar] [CrossRef] [Green Version]
- Dong, Y.; Morris-Natschke, S.L.; Lee, K.-H. Biosynthesis, total syntheses, and antitumor activity of tanshinones and their analogs as potential therapeutic agents. Nat. Prod. Rep. 2011, 28, 529–542. [Google Scholar] [CrossRef]
- Chen, X.; Guo, J.; Bao, J.; Lu, J.; Wang, Y. The Anticancer Properties of Salvia Miltiorrhiza Bunge (Danshen): A Systematic Review. Med. Res. Rev. 2013, 34, 768–794. [Google Scholar] [CrossRef]
- Xing, L.; Tan, Z.-R.; Cheng, J.-L.; Huang, W.-H.; Zhang, W.; Deng, W.; Yuan, C.-S.; Zhou, H.-H. Bioavailability and pharmacokinetic comparison of tanshinones between two formulations of Salvia miltiorrhiza in healthy volunteers. Sci. Rep. 2017, 7, 4709. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Panwar, P.; Søe, K.; Guido, R.V.C.; Bueno, R.V.C.; Delaisse, J.-M.; Brömme, D. A novel approach to inhibit bone resorption: Exosite inhibitors against cathepsin K. Br. J. Pharmacol. 2015, 173, 396–410. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ren, Z.H.; Tong, Y.H.; Xu, W.; Ma, J.; Chen, Y. Tanshinone II A attenuates inflammatory responses of rats with myocardial infarction by reducing MCP-1 expression. Phytomedicine 2010, 17, 212–218. [Google Scholar] [CrossRef]
- Li, X.; Lian, L.-H.; Bai, T.; Wu, Y.-L.; Wan, Y.; Xie, W.-X.; Jin, X.; Nan, J.-X. Cryptotanshinone inhibits LPS-induced proinflammatory mediators via TLR4 and TAK1 signaling pathway. Int. Immunopharmacol. 2011, 11, 1871–1876. [Google Scholar] [CrossRef] [PubMed]
- Li, X.-X.; Zheng, X.; Liu, Z.; Xu, Q.; Tang, H.; Feng, J.; Yang, S.; Vong, C.T.; Gao, H.; Wang, Y. Cryptotanshinone from Salvia miltiorrhiza Bunge (Danshen) inhibited inflammatory responses via TLR4/MyD88 signaling pathway. Chin. Med. 2020, 15, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Jang, S.I.; Kim, H.J.; Kim, Y.-J.; Jeong, S.-I.; You, Y.-O. Tanshinone IIA inhibits LPS-induced NF-κB activation in RAW 264.7 cells: Possible involvement of the NIK–IKK, ERK1/2, p38 and JNK pathways. Eur. J. Pharmacol. 2006, 542, 1–7. [Google Scholar] [CrossRef]
- Liu, X.; Niu, Y.; Xie, W.; Wei, D.; Du, Q. Tanshinone IIA promotes osteogenic differentiation of human periodontal ligament stem cells via ERK1/2-dependent Runx2 induction. Am. J. Trans. Res. 2019, 11, 340–350. [Google Scholar]
- Qian, K.; Xu, H.; Dai, T.; Shi, K. Effects of Tanshinone IIA on osteogenic differentiation of mouse bone marrow mesenchymal stem cells. Naunyn-Schmiedeberg’s Arch. Pharmacol. 2015, 388, 1201–1209. [Google Scholar] [CrossRef]
- Lee, S.-Y.; Choi, D.-Y.; Woo, E.-R. Inhibition of osteoclast differentiation by tanshinones from the root ofSalvia miltiorrhiza Bunge. Arch. Pharmacal Res. 2005, 28, 909–913. [Google Scholar] [CrossRef]
- Panwar, P.; Xue, L.; Søe, K.; Srivastava, K.; Law, S.; Delaisse, J.-M.; Brömme, D. An Ectosteric Inhibitor of Cathepsin K Inhibits Bone Resorption in Ovariectomized Mice. J. Bone Miner. Res. 2017, 32, 2415–2430. [Google Scholar] [CrossRef] [Green Version]
- Kwak, H.B.; Yang, D.; Ha, H.; Lee, J.-H.; Kim, H.-N.; Woo, E.-R.; Lee, S.; Kim, H.-H.; Lee, Z.H. Tanshinone IIA inhibits osteoclast differentiation through down-regulation of c-Fos and NFATc1. Exp. Mol. Med. 2006, 38, 256–264. [Google Scholar] [CrossRef] [PubMed]
- Kwak, H.B.; Sun, H.-M.; Ha, H.; Kim, H.-N.; Lee, J.-H.; Kim, H.-H.; Shin, H.-I.; Lee, Z.H. Tanshinone IIA suppresses inflammatory bone loss by inhibiting the synthesis of prostaglandin E2 in osteoblasts. Eur. J. Pharmacol. 2008, 601, 30–37. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.-H.; Kim, J.H.; Kwak, H.B.; Huang, H.; Han, S.-H.; Ha, H.; Lee, S.W.; Woo, E.-R.; Lee, Z.H. Inhibition of osteoclast differentiation and bone resorption by tanshinone IIA isolated from Salvia miltiorrhiza Bunge. Biochem. Pharmacol. 2004, 67, 1647–1656. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.-K.; Woo, E.-R.; Lee, H.-W.; Park, H.-R.; Kim, H.-N.; Jung, Y.-K.; Choi, J.-Y.; Chae, S.-W.; Kim, H.-R.; Chae, H.-J. The Correlation ofSalvia miltiorrhizaExtract–Induced Regulation of Osteoclastogenesis with the Amount of Components Tanshinone I, Tanshinone IIA, Cryptotanshinone, and Dihydrotanshinone. Immunopharmacol. Immunotoxicol. 2008, 30, 347–364. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Kim, S.H. Tanshinone IIA enhances BMP-2-stimulated commitment of C2C12 cells into osteoblasts via p38 activation. Amino Acids 2010, 39, 1217–1226. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Chen, H.; Zhang, H. Tanshinone IIA exerts beneficial effects on fracture healing in vitro and in vivo. Chem. Interactions 2019, 310, 108748. [Google Scholar] [CrossRef]
- Zhu, S.; Wei, W.; Liu, Z.; Yang, Y.; Jia, H. Tanshinone-IIA attenuates the deleterious effects of oxidative stress in osteoporosis through the NF-κB signaling pathway. Mol. Med. Rep. 2018, 17, 6969–6976. [Google Scholar] [CrossRef] [Green Version]
- Li, J.; He, C.; Tong, W.; Zou, Y.; Li, D.; Zhang, C.; Xu, W. Tanshinone IIA blocks dexamethasone-induced apoptosis in osteoblasts through inhibiting Nox4-derived ROS production. Int. J. Clin. Exp. Pathol. 2015, 8, 13695–13706. [Google Scholar]
- Cheng, L.; Zhou, S.; Zhao, Y.; Sun, Y.; Xu, Z.; Yuan, B.; Chen, X. Tanshinone IIA attenuates osteoclastogenesis in ovariectomized mice by inactivating NF-kB and Akt signaling pathways. Am. J. Transl. Res. 2018, 10, 1457–1468. [Google Scholar]
- Wang, L.; Cheng, L.; Zhang, B.; Wang, N.; Wang, F. Tanshinone prevents alveolar bone loss in ovariectomized osteoporosis rats by up-regulating phosphoglycerate dehydrogenase. Toxicol. Appl. Pharmacol. 2019, 376, 9–16. [Google Scholar] [CrossRef]
- Yao, J.; Ma, S.; Feng, W.; Wei, Y.; Lu, H.; Zhong, G.; Wu, Z.; Wang, H.; Su, W.; Li, J. Tanshinone IIA protects against polyethylene particle-induced osteolysis response in a mouse calvarial model. International Journal of Clinical and Experimental Pathology 2018, 11, 4461–4471. [Google Scholar]
- Zhang, J.; Cai, Z.; Yang, M.; Tong, L.; Zhang, Y. Inhibition of tanshinone IIA on renin activity protected against osteoporosis in diabetic mice. Pharm. Biol. 2020, 58, 219–224. [Google Scholar] [CrossRef] [PubMed]
- Cui, L.; Wu, T.; Liu, Y.-Y.; Deng, Y.-F.; Ai, C.-M.; Chen, H.-Q. Tanshinone prevents cancellous bone loss induced by ovariectomy in rats. Acta Pharmacol. Sin. 2004, 25, 678–684. [Google Scholar]
- Zhou, Y.; Liu, Y.; Gao, Y. Effect of tanshitone on prevention and treatment of retinoic acid induced osteoporosis in mice. China J. Chin. Mater. Medica 2010, 35, 2923–2926. [Google Scholar]
- Zhang, S.Y.; Liu, J.G.; Zhao, G. Tanshinone type IIA inhibits osteoprotegerin and osteoclast differentiation factor expression at relapse stage after orthodontic tooth movement. Chinese J. Tissue Engineering Res. 2014, 18, 1730–1736. [Google Scholar] [CrossRef]
- Yang, F.-F.; Gao, Y.-H.; Xi, H.-R.; Li, W.-Y.; Ma, H.-P.; Chen, K.-M. Effect of Compound Medicine of Tanshinone 2A and Resveratrol on Peak Bone Mass in Growing Rats. Zhongguo Yi Xue Ke Xue Yuan Xue Bao 2018, 40, 456–462. [Google Scholar]
- Dirckx, N.; Moorer, M.C.; Clemens, T.L.; Riddle, R.C. The role of osteoblasts in energy homeostasis. Nat. Rev. Endocrinol. 2019, 15, 651–665. [Google Scholar] [CrossRef]
- Katagiri, T.; Yamaguchi, A.; Komaki, M.; Abe, E.; Takahashi, N.; Ikeda, T.; Rosen, V.; Wozney, J.M.; Fujisawa-Sehara, A.; Suda, T. Bone morphogenetic protein-2 converts the differentiation pathway of C2C12 myoblasts into the osteoblast lineage [published erratum appears in J Cell Biol 1995 Feb;128(4):following 713]. J. Cell Biol. 1994, 127, 1755–1766. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goettsch, C.; Babelova, A.; Trummer, O.; Erben, R.G.; Rauner, M.; Rammelt, S.; Weissmann, N.; Weinberger, V.; Benkhoff, S.; Kampschulte, M.; et al. NADPH oxidase 4 limits bone mass by promoting osteoclastogenesis. J. Clin. Investig. 2013, 123, 4731–4738. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, D.H.; Lim, B.-S.; Lee, Y.-K.; Yang, H.-C. Effects of hydrogen peroxide (H2O2) on alkaline phosphatase activity and matrix mineralization of odontoblast and osteoblast cell lines. Cell Biol. Toxicol. 2006, 22, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Z.-Y.; Zhao, W.-R.; Zhang, J.; Chen, X.-L.; Tang, J.-Y. Sodium tanshinone IIA sulfonate: A review of pharmacological activity and pharmacokinetics. Biomed. Pharmacother. 2019, 118, 109362. [Google Scholar] [CrossRef] [PubMed]
- Shang, Q.; Xu, H.; Huang, L. Tanshinone IIA: A Promising Natural Cardioprotective Agent. Evid. Based Complementary Altern. Med. 2012, 2012, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, J.-Y.; Kim, J.H.; Kim, Y.M.; Jeong, H.J.; Kim, D.W.; Park, K.H.; Kwon, H.-J.; Park, S.-J.; Lee, W.S.; Ryu, Y.B. Tanshinones as selective and slow-binding inhibitors for SARS-CoV cysteine proteases. Bioorganic Med. Chem. 2012, 20, 5928–5935. [Google Scholar] [CrossRef] [PubMed]
- Tella, S.H.; Gallagher, J.C. Prevention and treatment of postmenopausal osteoporosis. J. Steroid Biochem. Mol. Biol. 2014, 142, 155–170. [Google Scholar] [CrossRef] [Green Version]
- Joeng, K.S.; Lee, Y.-C.; Jiang, M.-M.; Bertin, T.K.; Chen, Y.; Abraham, A.M.; Ding, H.; Bi, X.; Ambrose, C.G.; Lee, B.H. The swaying mouse as a model of osteogenesis imperfecta caused by WNT1 mutations. Hum. Mol. Genet. 2014, 23, 4035–4042. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vestergaard, P. Diabetes and Bone. J. Diabetes Metab. 2012, 01, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Shivaswamy, V.; Mack, L.R.; Larsen, J. Diabetes, Bone Density, and Fractures. J. Diabetes Met. 2012, 2012, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Ginaldi, L.; Di Benedetto, M.C.; De Martinis, M. Osteoporosis, inflammation and ageing. Immun. Ageing I A 2005, 2, 14. [Google Scholar] [CrossRef] [Green Version]
- Xiao, G.; Gopalakrishnan, R.; Jiang, D.; Reith, E.; Benson, M.D.; Franceschi, R.T. Bone Morphogenetic Proteins, Extracellular Matrix, and Mitogen-Activated Protein Kinase Signaling Pathways Are Required for Osteoblast-Specific Gene Expression and Differentiation in MC3T3-E1 Cells. J. Bone Miner. Res. 2002, 17, 101–110. [Google Scholar] [CrossRef]
- Nohe, A.; Hassel, S.; Ehrlich, M.; Neubauer, F.; Sebald, W.; Henis, Y.I.; Knaus, P. The Mode of Bone Morphogenetic Protein (BMP) Receptor Oligomerization Determines Different BMP-2 Signaling Pathways. J. Biol. Chem. 2002, 277, 5330–5338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Massagué, J.; Blain, S.W.; Lo, R.S. TGFβ Signaling in Growth Control, Cancer, and Heritable Disorders. Cell 2000, 103, 295–309. [Google Scholar] [CrossRef] [Green Version]
- Guo, X.; Wang, X.-F. Signaling cross-talk between TGF-β/BMP and other pathways. Cell Res. 2009, 19, 71–88. [Google Scholar] [CrossRef] [PubMed]
- Baek, K.H.; Oh, K.W.; Lee, W.Y.; Lee, S.S.; Kim, M.K.; Kwon, H.S.; Rhee, E.J.; Han, J.H.; Song, K.H.; Cha, B.Y.; et al. Association of Oxidative Stress with Postmenopausal Osteoporosis and the Effects of Hydrogen Peroxide on Osteoclast Formation in Human Bone Marrow Cell Cultures. Calcif. Tissue Int. 2010, 87, 226–235. [Google Scholar] [CrossRef]
- Yin, H.; Shi, Z.-G.; Yu, Y.-S.; Hu, J.; Wang, R.; Luan, Z.-P.; Guo, D.-H. Protection against osteoporosis by statins is linked to a reduction of oxidative stress and restoration of nitric oxide formation in aged and ovariectomized rats. Eur. J. Pharmacol. 2012, 674, 200–206. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Zhao, L.; Liu, J.; Liu, A.-L.; Zeng, W.-S.; Luo, S.-Q.; Bai, X.-C. Hydrogen Peroxide Induces G2Cell Cycle Arrest and Inhibits Cell Proliferation in Osteoblasts. Anat. Rec. Adv. Integr. Anat. Evol. Biol. 2009, 292, 1107–1113. [Google Scholar] [CrossRef] [PubMed]
- Zhong, Z.-M.; Bai, L.; Chen, J.-T. Advanced Oxidation Protein Products Inhibit Proliferation and Differentiation of Rat Osteoblast-like Cells via NF-κB Pathway. Cell. Physiol. Biochem. 2009, 24, 105–114. [Google Scholar] [CrossRef] [PubMed]
- Almeida, M.; Han, L.; Ambrogini, E.; Bartell, S.M.; Manolagas, S.C. Oxidative Stress Stimulates Apoptosis and Activates NF-κB in Osteoblastic Cells via a PKCβ/p66shc Signaling Cascade: Counter Regulation by Estrogens or Androgens. Mol. Endocrinol. 2010, 24, 2030–2037. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, Y.; Wang, D.; Wang, X.; Wang, Y.; Ren, F.; Chang, D.; Chang, Z.; Jia, B. Caspase 3 is Activated through Caspase 8 instead of Caspase 9 during H2O2-induced Apoptosis in HeLa Cells. Cell. Physiol. Biochem. 2011, 27, 539–546. [Google Scholar] [CrossRef] [PubMed]
- Moriishi, T.; Kawai, Y.; Komori, H.; Rokutanda, S.; Eguchi, Y.; Tsujimoto, Y.; Asahina, I.; Komori, T. Bcl2 Deficiency Activates FoxO through Akt Inactivation and Accelerates Osteoblast Differentiation. PLoS ONE 2014, 9, e86629. [Google Scholar] [CrossRef]
- Schroeder, K.; Zhang, M.; Benkhoff, S.; Mieth, A.; Pliquett, R.; Kosowski, J.; Kruse, C.; Luedike, P.; Michaelis, U.R.; Weissmann, N.; et al. Nox4 Is a Protective Reactive Oxygen Species Generating Vascular NADPH Oxidase. Circ. Res. 2012, 110, 1217–1225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cabiscol, E.; Tamarit, J.; Ros, J. Oxidative stress in bacteria and protein damage by reactive oxygen species. Int. Microbiol. 2000, 3, 3–8. [Google Scholar]
- Yao, Z.; Li, Y.; Yin, X.; Dong, Y.; Xing, L.; Boyce, B.F. NF-κB RelB Negatively Regulates Osteoblast Differentiation and Bone Formation. J. Bone Miner. Res. 2014, 29, 866–877. [Google Scholar] [CrossRef]
- Gallois, A.; Lachuer, J.; Yvert, G.; Wierinckx, A.; Brunet, F.; Rabourdin-Combe, C.; Delprat, C.; Jurdic, P.; Mazzorana, M. Genome-wide expression analyses establish dendritic cells as a new osteoclast precursor able to generate bone-resorbing cells more efficiently than monocytes. J. Bone Miner. Res. 2010, 25, 661–672. [Google Scholar] [CrossRef]
- De Vries, T.J.; Schoenmaker, T.; Aerts, D.; Grevers, L.C.; Souza, P.P.; Nazmi, K.; Van De Wiel, M.A.; Ylstra, B.; Van Lent, P.L.V.; Leenen, P.J.M.; et al. M-CSF Priming of Osteoclast Precursors Can Cause Osteoclastogenesis-Insensitivity, Which Can be Prevented and Overcome on Bone. J. Cell. Physiol. 2015, 230, 210–225. [Google Scholar] [CrossRef]
- Mun, S.H.; Park, P.S.U.; Park-Min, K.-H. The M-CSF receptor in osteoclasts and beyond. Exp. Mol. Med. 2020, 52, 1239–1254. [Google Scholar] [CrossRef]
- Suda, T.; Takahashi, N.; Udagawa, N.; Jimi, E.; Gillespie, M.T.; Martin, T.J. Modulation of Osteoclast Differentiation and Function by the New Members of the Tumor Necrosis Factor Receptor and Ligand Families. Endocr. Rev. 1999, 20, 345–357. [Google Scholar] [CrossRef]
- Bharti, A.C.; Takada, Y.; Shishodia, S.; Aggarwal, B.B. Evidence That Receptor Activator of Nuclear Factor (NF)-κB Ligand Can Suppress Cell Proliferation and Induce Apoptosis through Activation of a NF-κB-independent and TRAF6-dependent Mechanism. J. Biol. Chem. 2004, 279, 6065–6076. [Google Scholar] [CrossRef] [Green Version]
- Takayanagi, H.; Kim, S.; Koga, T.; Nishina, H.; Isshiki, M.; Yoshida, H.; Saiura, A.; Isobe, M.; Yokochi, T.; Inoue, J.-I.; et al. Induction and Activation of the Transcription Factor NFATc1 (NFAT2) Integrate RANKL Signaling in Terminal Differentiation of Osteoclasts. Dev. Cell 2002, 3, 889–901. [Google Scholar] [CrossRef] [Green Version]
- Johnson, R.S.; Spiegelman, B.M.; Papaioannou, V. Pleiotropic effects of a null mutation in the c-fos proto-oncogene. Cell 1992, 71, 577–586. [Google Scholar] [CrossRef]
- Ishida, N.; Hayashi, K.; Hoshijima, M.; Ogawa, T.; Koga, S.; Miyatake, Y.; Kumegawa, M.; Kimura, T.; Takeya, T. Large Scale Gene Expression Analysis of Osteoclastogenesisin Vitro and Elucidation of NFAT2 as a Key Regulator. J. Biol. Chem. 2002, 277, 41147–41156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakashima, T.; Hayashi, M.; Fukunaga, T.; Kurata, K.; Oh-Hora, M.; Feng, J.Q.; Bonewald, L.F.; Kodama, T.; Wutz, A.; Wagner, E.F.; et al. Evidence for osteocyte regulation of bone homeostasis through RANKL expression. Nat. Med. 2011, 17, 1231–1234. [Google Scholar] [CrossRef]
- Li, L.; Pettit, A.R.; Gregory, L.S.; Forwood, M.R. Regulation of bone biology by prostaglandin endoperoxide H synthases (PGHS): A rose by any other name…. Cytokine Growth Factor Rev. 2006, 17, 203–216. [Google Scholar] [CrossRef]
- Ono, K.; Akatsu, T.; Murakami, T.; Kitamura, R.; Yamamoto, M.; Shinomiya, N.; Rokutanda, M.; Sasaki, T.; Amizuka, N.; Ozawa, H.; et al. Involvement of Cyclo-Oxygenase-2 in Osteoclast Formation and Bone Destruction in Bone Metastasis of Mammary Carcinoma Cell Lines. J. Bone Miner. Res. 2002, 17, 774–781. [Google Scholar] [CrossRef]
- Ono, K.; Akatsu, T.; Kugai, N.; Pilbeam, C.C.; Raisz, L.G. The effect of deletion of cyclooxygenase-2, prostaglandin receptor EP2, or EP4 in bone marrow cells on osteoclasts induced by mouse mammary cancer cell lines. Bone 2003, 33, 798–804. [Google Scholar] [CrossRef]
- Kellinsalmi, M.; Parikka, V.; Risteli, J.; Hentunen, T.; Leskelä, H.-V.; Lehtonen, S.; Selander, K.; Väänänen, K.; Lehenkari, P. Inhibition of cyclooxygenase-2 down-regulates osteoclast and osteoblast differentiation and favours adipocyte formation in vitro. Eur. J. Pharmacol. 2007, 572, 102–110. [Google Scholar] [CrossRef]
- Troen, B.R. The Regulation of Cathepsin K Gene Expression. Ann. N. Y. Acad. Sci. 2006, 1068, 165–172. [Google Scholar] [CrossRef] [Green Version]
- Brömme, D.; Panwar, P.; Turan, S. Cathepsin K osteoporosis trials, pycnodysostosis and mouse deficiency models: Commonalities and differences. Expert Opin. Drug Discov. 2016, 11, 457–472. [Google Scholar] [CrossRef]
- Drake, M.T.; Clarke, B.L.; Oursler, M.J.; Khosla, S. Cathepsin K Inhibitors for Osteoporosis: Biology, Potential Clinical Utility, and Lessons Learned. Endocr. Rev. 2017, 38, 325–350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martin, T.J.; Sims, N.A. Osteoclast-derived activity in the coupling of bone formation to resorption. Trends Mol. Med. 2005, 11, 76–81. [Google Scholar] [CrossRef] [PubMed]
- Li, C.Y.; Jepsen, K.J.; Majeska, R.J.; Zhang, J.; Ni, R.; Gelb, B.D.; Schaffler, M.B. Mice Lacking Cathepsin K Maintain Bone Remodeling but Develop Bone Fragility Despite High Bone Mass. J. Bone Miner. Res. 2006, 21, 865–875. [Google Scholar] [CrossRef]
- George, E.L.; Lin, Y.-L.; Saunders, M.M. Bisphosphonate-related osteonecrosis of the jaw: A mechanobiology perspective. Bone Rep. 2018, 8, 104–109. [Google Scholar] [CrossRef]
- Noordin, S.; Masri, B. Periprosthetic osteolysis: Genetics, mechanisms and potential therapeutic interventions. Can. J. Surg. 2012, 55, 408–417. [Google Scholar] [CrossRef] [Green Version]
- Neuerburg, C.; Loer, T.; Mittlmeier, L.; Polan, C.; Farkas, Z.; Holdt, L.M.; Utzschneider, S.; Schwiesau, J.; Grupp, T.M.; Böcker, W.; et al. Impact of vitamin E-blended UHMWPE wear particles on the osseous microenvironment in polyethylene particle-induced osteolysis. Int. J. Mol. Med. 2016, 38, 1652–1660. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, T.; Wang, C.; Wu, Q.; Zheng, K.; Chen, J.; Lan, Y.; Qin, Y.; Mei, W.; Wang, B. Evaluation of Tanshinone IIA Developmental Toxicity in Zebrafish Embryos. Molecules 2017, 22, 660. [Google Scholar] [CrossRef] [Green Version]
- Yang, L.-J.; Jeng, C.-J.; Kung, H.-N.; Chang, C.-C.; Wang, A.-G.; Chau, G.-Y.; Don, M.-J.; Chau, Y.-P. Tanshinone IIA isolated from Salvia miltiorrhiza elicits the cell death of human endothelial cells. J. Biomed. Sci. 2005, 12, 347–361. [Google Scholar] [CrossRef]
- Zhang, Y.; Jiang, P.; Ye, M.; Kim, S.-H.; Jiang, C.; Lü, J. Tanshinones: Sources, Pharmacokinetics and Anti-Cancer Activities. Int. J. Mol. Sci. 2012, 13, 13621–13666. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.; Huang, M.; Guan, S.; Bi, H.-C.; Pan, Y.; Duan, W.; Chan, S.Y.; Chen, X.; Hong, Y.-H.; Bian, J.-S.; et al. A Mechanistic Study of the Intestinal Absorption of Cryptotanshinone, the Major Active Constituent ofSalvia miltiorrhiza. J. Pharmacol. Exp. Ther. 2006, 317, 1285–1294. [Google Scholar] [CrossRef] [Green Version]
- Yu, X.-Y.; Lin, S.-G.; Zhou, Z.-W.; Chen, X.; Liang, J.; Liu, P.-Q.; Duan, W.; Chowbay, B.; Wen, J.-Y.; Li, C.-G.; et al. Role of P-Glycoprotein in the Intestinal Absorption of Tanshinone IIA, a Major Active Ingredient in the Root of Salvia miltiorrhiza Bunge. Curr. Drug Metab. 2007, 8, 325–340. [Google Scholar] [CrossRef]
- Xu, S.; Liu, P. Tanshinone II-A: New perspectives for old remedies. Expert Opin. Ther. Pat. 2012, 23, 149–153. [Google Scholar] [CrossRef]
- Wang, L.; Lai, Y.; Li, C.; Jiang, X. Study on the intestinal absorption profiles of tanshinone IIA and its inclusion complex with cyclodextrin in rats. PDA J. Pharm. Sci. Technol. 2010, 63, 390–400. [Google Scholar]
- Liu, X.; An, C.; Jin, P.; Liu, X.; Wang, L. Protective effects of cationic bovine serum albumin-conjugated PEGylated tanshinone IIA nanoparticles on cerebral ischemia. Biomater. 2013, 34, 817–830. [Google Scholar] [CrossRef]
- Ma, H.; Fan, Q.; Yu, J.; Xin, J.; Zhang, C. Anticancer activities of tanshinone microemulsion against hepatocellular carcinoma in vitro and in vivo. Mol. Med. Rep. 2012, 7, 59–64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jia, X.-B.; Yan, H.-M.; Zhang, Z.-H.; Jiang, Y.-R.; Ding, D.-M.; Sun, E. An attempt to stabilize tanshinone IIA solid dispersion by the use of ternary systems with nano-CaCO3and poloxamer 188. Pharmacogn. Mag. 2014, 10, 311–S317. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, M.; Cai, Y.; Zhang, W.; Chen, Z.; Shi, Z.; He, C. Recent insights into the biological activities and drug delivery systems of tanshinones. Int. J. Nanomed. 2016, 11, 121–130. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Studies | Study Design | Changes with Tanshinone Treatment |
|---|---|---|
| Cell Culture Studies | ||
| Liu et al. [27] | Cell: hPDLSC from the premolars of 20 donors without oral or systematic diseases (10 men and 10 women aged 12–25 years old) Model: osteogenic differentiation Treatment: 2.5 and 5 μM of T-IIA for 48 h Negative control: Untreated cells Positive control: N.A. |
|
| Qian et al. [28] | Cell: BM-MSCs isolated from the tibia and femur of BALB/cJ mice (4–6 weeks old) Model: dexamethasone-induced osteogenic differentiation Treatment: 1, 5, 10 and 20 μM of T-IIA for 7 days Negative control: Untreated cells Positive control: N.A. |
|
| Kim and Kim [35] | Cell: C2C12 cells Model: BMP-2-induced osteoblast differentiation Treatment: 2.5, 5, 10 and 20 μM of T-IIA for 7 days Negative control: Untreated cells Positive control: N.A. |
|
| Wang et al. [36] | Cell: MC3T3-E1 cells Model: osteoblast differentiation Treatment: 5, 10, 15 and 20 μM of T-IIA for 48 h Negative control: Untreated cells Positive control: N.A. |
|
| Li et al. [38] | Cell: MC3T3-E1 cells Model: dexamethasone-induced osteoblast apoptosis Treatment: 1 μM of T-IIA for 24 h Negative control: Untreated cells Positive control: N.A. |
|
| Zhu et al. [37] | Cell: Osteoblast cells from 10 weeks old female Wnt1sw/sw mice Model: H2O2-induced osteoblast apoptosis Treatment: 1.5 mg/mL of T-IIA for 24 h Negative control: PBS-treated cells Positive control: 1.5 mg/kg alendronate |
|
| Cheng et al. [39] | Cell: RAW264.7 cells and BMMCs isolated from the femoral bone marrow of 8-week-old C57BL/6 mice. Model: RANKL-induced osteoclastogenesis Treatment: 1, 2 or 5 μg/mL of T-IIA for 7 days Negative control: Untreated cells Positive control: N.A. |
|
| Lee et al. [29] | Cell: Primary osteoblasts from calvarial cells of ICR newborn mice/bone marrow cells obtained from tibiae of 6- to 7-week-old ICR mice (coculture) Model: M-CSF-induced osteoclast differentiation Treatment: 0.5, 1 and 2.5 μg/mL of T-IIA, T-I, C-T, D-T for 3 days (osteoblasts) and 6-7 days (osteoclasts) Negative control: Untreated cells Positive control: N.A. |
|
| Panwar et al. [30] | Cell: mononuclear cells from human bone marrow and bone marrow cells from femur and tibia from 4 months old mice Model: M-CSF and RANKL-induced osteoclastogenesis Treatment: 1 and 3 μM of T06 for 72 h Negative control: DMSO (1%)-treated cells Positive control: N.A. |
|
| Kim et al. [34] | Cell: MC3T3-E1 cells and bone marrow cells isolated from the long bone of 7-weeks-old ICR male mice Model: M-CSF and RANKL-induced osteoclastogenesis Treatment: 1 μg/mL of T-IIA, T-I, D-T, and C-T for 7 days Negative control: DMSO-treated cells Positive control: N.A. |
|
| Kwak et al. [31] | Cell: Bone marrow cells from tibia and femur and mouse calvariae from pericranium of 5 weeks old male ICR mice. Model: M-CSF and RANKL-induced osteoclastogenesis Treatment: 10 μg/mL of T-IIA for 4 days Negative control: M-CSF-treated cells Positive control: N.A. |
|
| Kim et al. [33] | Cell: Calvarial osteoblasts from the new bone of ICR mice and bone marrow cells from tibiae of 6–7 weeks old ICR mice (Mouse bone marrow cells and calvarial osteoblast coculture) Model: M-CSF and RANKL-induced osteoclastogenesis Treatment: 2.5–20 μg/mL of T-IIA for 15 min–20 h Negative control: Untreated cells Positive control: N.A. |
|
| Kwak et al. [32] | Cell: Calvarial osteoblasts and bone marrow cells isolated from the femur and tibias of 5-weeks-old ICR male mice (Mouse bone marrow cells and calvarial osteoblast coculture) Model: TNF-α, IL-1α or LPS-induced osteoclast differentiation Treatment: 5 μg/mL of T-IIA for 7 days Negative control: Untreated cells Positive control: N.A. |
|
| Animal studies | ||
| Zhang, et al. [45] | Animals: 48 male Wistar rats (2 months old) Experimental model: Relapse stage after orthodontic mesial movement of maxillary first molar tooth Treatment: 0.36, 0.72 and 1.44 mg/day of T-IIA for 4 weeks (localised gingival mucosa injection) Negative control: Normal saline injection Positive control: N.A. |
|
| Yang, et al. [46] | Animals: 40 female Wistar rats (1 month old, 97 ± 3 g Disease model: N.A. Treatment: 22 mg/kg/day of T-IIA for 8 weeks (oral) Negative control: untreated rats Positive control: N.A. Comparative groups: 16.8 mg/kg/day of resveratrol and T-IIA (11 mg/kg/day) + resveratrol (8.4 mg/kg/day) for 8 weeks |
|
| Wang et al. [36] | Animals: 40 male C57BL/J6 mice (3 months old) Disease model: Open osteotomy at femur diaphysis Treatment: 10, 20 and 30 mg/kg/day of T-IIA for 4 weeks (oral) Negative control: Mice with open osteotomy received with methanol Normal control: No treatment or surgery Positive control: N.A. |
|
| Yao et al. [41] | Animals: 24 male C57BL/J6 mice (2 months old) Disease model: PE particle-induced calvarial osteolysis Treatment: 1 and 2 μg/g/day of T-IIA for 21 days (periosteum injection) Negative control: PE-induced mice treated with PBS Normal control: Sham treated with PBS Positive control: N.A. |
|
| Kwak et al. [32] | Animals: ICR mice Disease model: LPS-induced bone loss Treatment: 5 μg/g of T-IIA (i.p.) on the day before LPS induction, the day 1, 3, 5 and 7 after LPS induction Negative control: Mice with LPS-induced bone loss Normal control: Mice with PBS treatment Positive control: N.A. |
|
| Zhu et al. [37] | Animals: 64 female Wnt1sw/sw mice with osteoporosis (2.5 months old, 32–40 g) Disease model: Spontaneous WNT1 mutation for osteogenesis imperfecta Treatment: 10 mg/kg of T-IIA (i.p.)/day for 6 weeks (i.p.) Negative control: Osteoporotic mice with PBS injection Normal control: N.A. Positive control: 10 mg/kg alendronate for 6 weeks |
|
| Zhang et al. [42] | Animals: 40 male C57BL/J6 mice (2 months old) Disease model: STZ-induced diabetic osteoporosis Treatment: 10 and 30 mg/kg of T-IIA 3 times per week for 8 weeks (i.p.) Negative control: Diabetic mice with corn oil (vehicle) Normal control: Non-diabetic mice with corn oil Positive control: 2 mg/kg aliskiren, 3 times a week for 8 weeks |
|
| Wang et al. [40] | Animals: 32 female Sprague Dawley rats (3 months old) Disease model: OVX-induced osteoporosis Treatment: 10 mg/kg/day of T-IIA for 2 weeks (i.v.) Negative control: untreated OVX rats Normal control: Sham-operated rats Positive control: N.A. |
|
| Cheng et al. [39] | Animals: 18 female C57BL/6 mice (2 months old) Disease model: OVX-induced osteoporosis Treatment: 10 mg/kg T-IIA for 6 weeks (i.p.) Negative control: OVX with normal saline Normal control: Sham with normal saline Positive control: N.A. |
|
| Panwar et al. [30] | Animals: 29 female C57BL/6 mice (8 months old, 25g) Disease model: OVX-induced osteoporosis Treatment: 40 mg/kg/day of T06 for 3 months (oral) Negative control: OVX with an unknown vehicle Normal control: Sham with an unknown vehicle Positive control: N.A. |
|
| Cui et al. [43] | Animals: 32 female Sprague-Dawley (4 months old) Disease model: OVX-induced osteoporosis Treatment: 200 mg/kg/day of total tanshinone (5 mg/kg/day of T-IIA and 16 mg/kg/day of C-T) for 10 weeks (oral) Negative control: OVX with oral deionised water Normal control: Sham with oral deionised water Positive control: 30 μg/kg/day of 17α-37 for 10 weeks |
|
| Zhou et al. [44] | Animals: 30 male and 30 female KM mice (3 months old, 30 ± 5 g) Disease model: retinoic acid-induced osteoporosis Treatment: 40–160 mg/kg/day of tanshinone for 14 days (oral) Negative control: Untreated osteoporotic mice Normal control: sham-operated normal mice Positive control: 3 mg/kg/day of vitamin D3 for 14 days |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ekeuku, S.O.; Pang, K.-L.; Chin, K.-Y. The Skeletal Effects of Tanshinones: A Review. Molecules 2021, 26, 2319. https://doi.org/10.3390/molecules26082319
Ekeuku SO, Pang K-L, Chin K-Y. The Skeletal Effects of Tanshinones: A Review. Molecules. 2021; 26(8):2319. https://doi.org/10.3390/molecules26082319
Chicago/Turabian StyleEkeuku, Sophia Ogechi, Kok-Lun Pang, and Kok-Yong Chin. 2021. "The Skeletal Effects of Tanshinones: A Review" Molecules 26, no. 8: 2319. https://doi.org/10.3390/molecules26082319