
3D-Printing of Drug-Eluting Implants: An Overview of the Current Developments Described in the Literature

Abstract
:1. Introduction
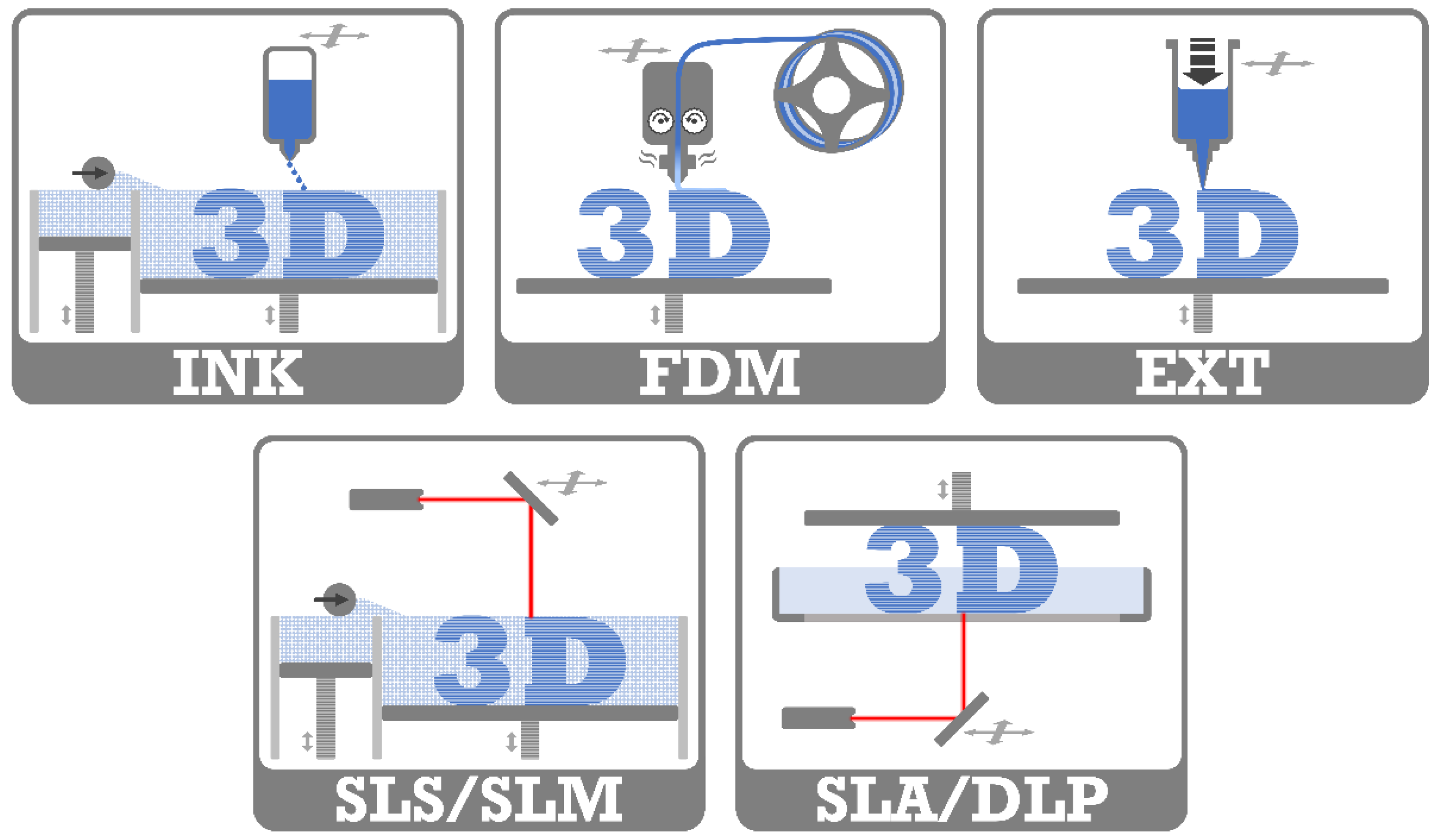
2. 3D-Printing Techniques
2.1. 3D Inkjet Printing (INK)
2.2. Fused Deposition Modeling (FDM)
2.3. Extrusion 3D-Printing (EXT)
2.4. Laser-Based 3D-Printing
3. Drug Loading Mechanisms
4. Current Medical and Pharmaceutical Applications of 3D-Printing
5. 3D-Printing of Drug-Eluting Implants
5.1. Stents and Catheters


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Implant Shape | Material | Drug | Drug Loading | Printer Type | Objective | Source |
|---|---|---|---|---|---|---|
| disc | PLA | nitrofurantoin | HME | FDM | incorporation of an antimicrobial drug in 3D model structure to inhibit biofilms | Sandler et al., (2014) [31] |
| disc, bead, catheter | PLA | gentamicin sulfate, methotrexate | HME | FDM | 3D-printing of different constructs with antibiotic or chemotherapeutic-eluting filament | Weisman et al., (2015) [38] |
| nasal stent | PLA | gentamicin sulfate | HME | FDM | personalized nasal stents with bioactive properties in cleft surgery | Mills et al., (2017) [40] |
| nasal stent | PLA, PVP | penicillin | postprint: dip coating | FDM | postoperative patient-specific nasal supports with bioactive agents | Boyer et al., (2018) [62] |
| mesh, Y-stent | PVA | iodine | postprint: gaseous incubation | FDM | antimicrobial and highly visible (CT image) meshes/stents of iodized (cross-linked) PVA | Boyer et al., (2018) [73] |
| catheter | PLA | gentamicin sulfate, methotrexate | HME | FDM | 3D-printing of bioactive laden bioabsorbable catheters | Weisman et al., (2019) [119] |
| catheter | TPU | tetracycline hydrochloride | HME | FDM | incorporation of an anti-infective drug into 3D-printed catheters | Mathew et al., (2019) [41] |
5.2. Gynecological Devices

| Implant Shape | Material | Drug | Drug Loading | Printer Type | Objective | Source |
|---|---|---|---|---|---|---|
| t-shaped IUD, s.c. rod | EVA | indomethacin | HME | FDM | 3D-printed implants of different grades of EVA | Genina et al., (2016) [34] |
| t-shaped IUS | PCL | indomethacin | HME | FDM | long-lasting biodegradable implants with different drug loads and sustained drug release | Holländer et al., (2016) [45] |
| mesh, s.c. rod, IUD, pessary | PCL | estrogen, progesterone | HME | FDM | hormone-eluting customizable and biodegradable 3D-printed implants | Tappa et al., (2017) [42] |
| O/Y/M-shaped vaginal ring | PLA, PCL, PEG | progesterone | prefused HME | FDM | 3D-printed vaginal rings in various shapes for personalization and controlled drug release | Fu et al., (2018) [39] |
| vaginal mesh | TPU | levofloxacin | HME | FDM | antibacterial vaginal meshes with suitable mechanical properties | Domínguez- Robles et al., (2020) [43] |
| cervical tissue implant | PU | anti-HPV- protein | postprint: immersion | LDM | 3D-printing with LDM and freeze-drying for porous and elastic tissue implants | Zhao et al., (2020) [67] |
| mesh | TPU | estradiol | HME | FDM | influence of mesh geometry on the mechanical properties of 3D-printed surgical meshes | Farmer et al., (2021) [125] |
5.3. Devices for Bone Treatment and Surgical Screws

| Implant Shape | Material | Drug | Drug Loading | Printer Type | Objective | Source |
|---|---|---|---|---|---|---|
| cylinder | ceramics, PLGA | vancomycin hydrochloride, ofloxacin, tetracyline hydrochloride | postprint: immersion | INK | drug adsorption and desorption of low temperature 3D-printed ceramic scaffolds | Gbureck et al., (2007) [68] |
| multi- layered cylinder | PLA | levofloxacin | binder solution | INK | 3D-printing of multilayered implant design for bi-modal release profile | Huang et al., (2007) [54] |
| levofloxacin, rifampicine | Wu et al., (2009) [128] | |||||
| multi- layered cylinder | PLA | isoniazid, rifampizin | binder solution | INK | programmed sequentially release of multidrug implant for bone tuberculosis treatment | Wu et al., (2009) [55] |
| levofloxacin, tobramycin | for treatment of chronic osteomyelitis | Wu et al., (2016) [56] | ||||
| scaffold | ceramic, HPMC | vancomycin, heparin, rhBMP-2 | ink solution | INK | multijet low-temperature 3D-printing of bioceramic implants with high accuracy of drug deposition to modify the release | Vorndran et al., (2010) [60] |
| scaffold | MBG, PVA | dexamethasone | preprint: impreg- nation | EXT | 3D-printing with new bioactive material MBG for implants with controlled pores, high mechanical strength and sustained drug delivery | Wu et al., (2011) [133] |
| cylinder | MBG, PHBHHx | isoniazid, rifampicin | preprint: impreg- nation | EXT | 3D-printed scaffolds with antitubercular drugs in animal model | Zhu et al., (2015) [129] Li et al., (2015) [130] |
| scaffold | PCL, PLGA | tobramycin | embedding | heat EXT | 3D-printing of scaffold for bone tissue formation and antibacterial properties | Shim et al., (2015) [131] |
| scaffold | PCL, poloxamine | dexamethasone | HME (syringe/tube) | FDM | dependence of blend ratios on degradation rates and release profiles | Costa et al., (2015) [134] |
| scaffold | ceramic, PLGA- coating | rifampicin, vancomycin | ink/coating solution, powder mixture | INK | simultaneous local delivery of rifampicin and vancomycin from 3D-printed ceramic scaffolds for bone infection treatment examined in a mouse model | Inzana et al., (2015) [57] |
| cylinder | CoCrMo | gentamicin | postprint: electro- phoretic deposition | SLM | antibacterial coating of 3D-printed porous CoCrMo bone substitutes | Han et al., (2017) [132] |
| disc, bead | PLA | gentamicin sulfate | HME | FDM | 3D-printing of antibacterial drug doped holloysite nanotubes constructs | Weisman et al., (2017) [44] |
| scaffold | ceramic, PLGA- coating | rifampicin, sitafloxacin | powder mixture | INK | 3D-printing of antibacterial scaffolds for osteomyelitis treatment | Trombetta et al., (2019) [59] |
| scaffold | PLA | minocycline | postprint: immersion | FDM | 3D-printing of scaffold with antibiofilm and osteogenic properties | Martin et al., (2019) [72] |
| screw, pin, plate | PLA | gentamicin sulfate, methotrexate | HME | FDM | patient-specific fixation implants for localized drug delivery | Tappa et al., (2019) [35] |
| scaffold | PLA | dexamethasone, prednisolone | pre-/post- print: soaking | FDM | combination of two drug loading mechanisms for different release profiles | Farto-Vaamonde et al., (2019) [135] |
| disc | PCL | rifampicin | embedding | heat EXT | 3D-printing of antibacterial drug containing scaffold at low temperatures | Lee et al., (2020) [137] |
| cuboid | stainless steel | dexamethasone | postprint: airbrush coating | SLM | coating of 3D-printed stainless-steel implants for slow drug release | Poudel et al., (2020) [63] |
| screw | PCL, nHA | vancomycin, ceftazidime | embedding | EXT | influence of printing parameter on drug-eluting screws 3D-printed by a solution-technique | Chou et al., (2021) [46] |
5.4. Antitumoral Devices

| Implant Shape | Material | Drug | Drug Loading | Printer Type | Objective | Source |
|---|---|---|---|---|---|---|
| patch | PLGA, PCL | 5-fluorouracil | melt mixing | heat EXT | biodegradable patch with high concentrations of anti-cancer drug and modifiable release | Yi et al., (2016) [47] |
| wafer | titanium | doxorubicin, Apo2L/TRAIL | postprint: droplets | SLM | enhanced bone osseointegration by drug-loaded 3D-printed titanium alloy implants with microrough surface | Maher et al., (2017) [64] |
| bullet shape | PLA | cytoxan | postprint: immersion | FDM | hollow bullet-shaped implants with modified release properties | Yang et al., (2018) [69] |
| sphere, cylinder | PLA | cisplatin, ifosfamide, methotrexate, doxorubicin | postprint: immersion | INK | 3D-printed multidrug implant for osteosarcoma treatment tested in vitro and in vivo | Wang et al., (2020) [70] |
| scaffold | PLGA | 5-fluorouracil, NVP-BEZ235 | embedding | EXT (E-jet) | controlled drug release of 3D-printed implants for orthotopic breast cancer therapy | Yang et al., (2020) [48] |
5.5. Surgical Meshes

| Implant Shape | Material | Drug | Drug Loading | Printer Type | Objective | Source |
|---|---|---|---|---|---|---|
| mesh | PLA | gentamicin | HME | FDM | antibacterial surgical meshes from 3D-printer as potential on-demand manufacturing | Ballard et al. (2017), [36] |
| mesh | silicone | prednisolone | embedding | semi- solid EXT + UV | room-temperature 3D-printing with UV-crosslinking of silicone into different structures and drug loads resulted in different release profiles | Holländer et al. (2018), [49] |
| mesh | PCL | iodine, gadolinium, barium | embedding | heat EXT | 3D-printing of surgical meshes impregnated with contrast agent and characterization of computer tomography properties | Ballard et al. (2018), [140] |
| mesh | PCL | gentamicin | postprint: droplets | FDM | 3D-printed surgical meshes with antibiotics encapsulated in alginate | Calero Castro et al. (2019), [65] |
| mesh | PP, PVA | ciprofloxacin hydrochloride | preprint: filament soaking | FDM | antibiotic loaded 3D-printed meshes with different pore size, shape and thread thickness of two different materials | Qamar et al. (2019), [51] |
5.6. Other Devices with Simple Geometry
| Implant Shape | Material | Drug | Drug Loading | Printer Type | Objective | Source |
|---|---|---|---|---|---|---|
| cube | nylon | methylene blue | postprint: immersion | SLS | control of the porosity of 3D-printed construct by varying the printing parameter | Leong et al., (2001) [71] |
| (hollow) cylinder | PLA | isoniazid | binder solution | INK | drug release from drug-loaded 3D-printed structures | Wu et al., (2014) [58] |
| disc | PLA, hydroxyl-apatite | nitrofurantoin | HME | FDM | antibacterial feedstock material for 3D-printing | Water et al., (2015) [37] |
| hollow cylinder | PCL, PLA, EC, Eudragit RS | quinine | HME | FDM | long-term drug release from 3D-printed implants of different polymers and drug loads | Kempin et al., (2017) [141] |
| scaffold | PCL | cefazolin | postprint: coating | heat EXT | combination of 3D-printing and salt-leaching method for scaffolds with intrastrut microporosity | Visscher et al., (2018) [66] |
| cuboid | PMMA | flurbiprofen | postprint: super- critical CO2 | SLA | drug loading of 3D-printed constructs using supercritical carbon dioxide | Ngo et al., (2020) [74] |
| bar | poly- urethane, PEG | paracetamol | embedding | heat EXT | drug-loaded thermo-responsive supramolecular polyurethane for 3D-printing | Salimi et al., (2020) [50] |
| disc, bar | PCL | doxycycline, vancomycin, cefazolin | HME | FDM | effect of manufacturing conditions (temperature or UV light) on antibacterial effectiveness | Ranganathan et al., (2020) [142] |
| PEG, PEGDA | embedding | SLA simulation | ||||
| disc, cylinder | PEGDA | dexamethasone | embedding | DLP | influence of relatively high drug loadings on printability and mechanical properties of DLP 3D-printed constructs | Mau et al., (2020) [52] |
| cylinder | PLA, PETG, PMMA | diclofenac sodium | powder filling during printing | FDM | in vitro testing of implantable 3D-printed drug carriers | Arany et al., (2020) [78] |
5.7. Other Devices with Complex Geometry

| Implant Shape | Material | Drug | Drug Loading | Printer Type | Objective | Source |
|---|---|---|---|---|---|---|
| multi- layered cuboid | PEO, PCL | methylene blue, alizarin yellow | manually deposited | INK | first report of 3D-printing for control of release by modifying drug position, composition and microstructure | Wu et al., (1996) [61] |
| window implant | PLA, PVA, PEG, PCL | methylene blue, ibuprofen sodium/base | postprint: powder filling | FDM | different implant designs of biodegradable material for controllable sustained drug release | Stewart et al., (2020) [75] Stewart et al., (2020) [76] |
| multiple shapes | PEGDA, DPPO, PEG | diclofenac sodium, ibuprofen | embedding | DLP | influence of additives, printing parameters and model design on constructs with external and internal structured 3D-printed by DLP | Yang et al., (2020) [53] |
| rod, scaffold, spiral | PCL, poloxamer, alginate | bevacizumab, dexamethasone | embedding, injected | EXT | coaxial coextrusion for drug-loaded core-shell implant design with gel core | Won et al., (2020) [77] |
6. Benefits and Challenges of 3D-Printed Drug-Eluting Implants
7. Regulatory Aspects
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Johnson, A.R.; Forster, S.P.; White, D.; Terife, G.; Lowinger, M.; Teller, R.S.; Barrett, S.E. Drug Eluting Implants in Pharmaceutical Development and Clinical Practice. Expert Opin. Drug Deliv. 2021, 1–17. [Google Scholar] [CrossRef]
- Gao, Z.; Matin, F.; Weber, C.; John, S.; Lenarz, T.; Scheper, V. High Variability of Postsurgical Anatomy Supports the Need for Individualized Drug-Eluting Implants to Treat Chronic Rhinosinusitis. Life 2020, 10, 353. [Google Scholar] [CrossRef] [PubMed]
- Meric, G.; Gracitelli, G.C.; Aram, L.J.; Swank, M.L.; Bugbee, W.D. Variability in Distal Femoral Anatomy in Patients Undergoing Total Knee Arthroplasty: Measurements on 13,546 Computed Tomography Scans. J. Arthroplasty 2015, 30, 1835–1838. [Google Scholar] [CrossRef]
- Bourgouin, S.; Bège, T.; Lalonde, N.; Mancini, J.; Masson, C.; Chaumoitre, K.; Brunet, C.; Berdah, S.V. Three-Dimensional Determination of Variability in Colon Anatomy: Applications for Numerical Modeling of the Intestine. J. Surg. Res. 2012, 178, 172–180. [Google Scholar] [CrossRef] [PubMed]
- Kopf, S.; Pombo, M.W.; Szczodry, M.; Irrgang, J.J.; Fu, F.H. Size Variability of the Human Anterior Cruciate Ligament Insertion Sites. Am. J. Sports Med. 2011, 39, 108–113. [Google Scholar] [CrossRef] [PubMed]
- Blendea, D.; Shah, R.V.; Auricchio, A.; Nandigam, V.; Orencole, M.; Heist, E.K.; Reddy, V.Y.; McPherson, C.A.; Ruskin, J.N.; Singh, J.P. Variability of Coronary Venous Anatomy in Patients Undergoing Cardiac Resynchronization Therapy: A High-Speed Rotational Venography Study. Hear. Rhythm 2007, 4, 1155–1162. [Google Scholar] [CrossRef] [PubMed]
- Rengier, F.; Mehndiratta, A.; von Tengg-Kobligk, H.; Zechmann, C.M.; Unterhinninghofen, R.; Kauczor, H.-U.; Giesel, F.L. 3D Printing Based on Imaging Data: Review of Medical Applications. Int. J. Comput. Assist. Radiol. Surg. 2010, 5, 335–341. [Google Scholar] [CrossRef]
- Pietrabissa, A.; Marconi, S.; Peri, A.; Pugliese, L.; Cavazzi, E.; Vinci, A.; Botti, M.; Auricchio, F. From CT Scanning to 3-D Printing Technology for the Preoperative Planning in Laparoscopic Splenectomy. Surg. Endosc. 2016, 30, 366–371. [Google Scholar] [CrossRef] [PubMed]
- Plavitu, A.; Pogarasteanu, M.E.; Moga, M.; Barbilian, R.C.; Stoica, I.C.; Robu, G.C.; Oproiu, A.M.; Jinga, M.; Ifrim, C.F. MRI versus CT as Image Data Source for 3D Printing Bone. Rev. Chim. 2018, 69, 2881–2884. [Google Scholar] [CrossRef]
- Ripley, B.; Levin, D.; Kelil, T.; Hermsen, J.L.; Kim, S.; Maki, J.H.; Wilson, G.J. 3D Printing from MRI Data: Harnessing Strengths and Minimizing Weaknesses. J. Magn. Reson. Imaging 2017, 45, 635–645. [Google Scholar] [CrossRef]
- Marro, A.; Bandukwala, T.; Mak, W. Three-Dimensional Printing and Medical Imaging: A Review of the Methods and Applications. Curr. Probl. Diagn. Radiol. 2016, 45, 2–9. [Google Scholar] [CrossRef]
- Ventola, C.L. Medical Applications for 3D Printing: Current and Projected Uses. P T 2014, 39, 704–711. [Google Scholar]
- Alhnan, M.A.; Okwuosa, T.C.; Sadia, M.; Wan, K.-W.; Ahmed, W.; Arafat, B. Emergence of 3D Printed Dosage Forms: Opportunities and Challenges. Pharm. Res. 2016, 33, 1817–1832. [Google Scholar] [CrossRef]
- Trenfield, S.J.; Awad, A.; Goyanes, A.; Gaisford, S.; Basit, A.W. 3D Printing Pharmaceuticals: Drug Development to Frontline Care. Trends Pharmacol. Sci. 2018, 39, 440–451. [Google Scholar] [CrossRef] [PubMed]
- Jamróz, W.; Szafraniec, J.; Kurek, M.; Jachowicz, R. 3D Printing in Pharmaceutical and Medical Applications – Recent Achievements and Challenges. Pharm. Res. 2018, 35, 176. [Google Scholar] [CrossRef]
- Lim, S.H.; Kathuria, H.; Tan, J.J.Y.; Kang, L. 3D Printed Drug Delivery and Testing Systems—A Passing Fad or the Future? Adv. Drug Deliv. Rev. 2018, 132, 139–168. [Google Scholar] [CrossRef]
- Jacob, S.; Nair, A.B.; Patel, V.; Shah, J. 3D Printing Technologies: Recent Development and Emerging Applications in Various Drug Delivery Systems. AAPS PharmSciTech 2020, 21, 220. [Google Scholar] [CrossRef] [PubMed]
- Trenfield, S.J.; Awad, A.; Madla, C.M.; Hatton, G.B.; Firth, J.; Goyanes, A.; Gaisford, S.; Basit, A.W. Shaping the Future: Recent Advances of 3D Printing in Drug Delivery and Healthcare. Expert Opin. Drug Deliv. 2019, 16, 1081–1094. [Google Scholar] [CrossRef] [PubMed]
- Tappa, K.; Jammalamadaka, U. Novel Biomaterials Used in Medical 3D Printing Techniques. J. Funct. Biomater. 2018, 9, 17. [Google Scholar] [CrossRef]
- Awad, A.; Trenfield, S.J.; Goyanes, A.; Gaisford, S.; Basit, A.W. Reshaping Drug Development Using 3D Printing. Drug Discov. Today 2018, 23, 1547–1555. [Google Scholar] [CrossRef]
- Ahangar, P.; Cooke, M.E.; Weber, M.H.; Rosenzweig, D.H. Current Biomedical Applications of 3D Printing and Additive Manufacturing. Appl. Sci. 2019, 9, 1713. [Google Scholar] [CrossRef]
- Cui, M.; Pan, H.; Su, Y.; Fang, D.; Qiao, S.; Ding, P.; Pan, W. Opportunities and Challenges of Three-Dimensional Printing Technology in Pharmaceutical Formulation Development. Acta Pharm. Sin. B 2021. [Google Scholar] [CrossRef]
- Ligon, S.C.; Liska, R.; Stampfl, J.; Gurr, M.; Mülhaupt, R. Polymers for 3D Printing and Customized Additive Manufacturing. Chem. Rev. 2017, 117, 10212–10290. [Google Scholar] [CrossRef] [PubMed]
- Tamil Ponni, R.; Swamivelmanickam, M.; Sivakrishnan, S. 3D Printing in Pharmaceutical Technology—A Review. Int. J. Pharm. Investig. 2020, 10, 8–12. [Google Scholar] [CrossRef]
- Daly, R.; Harrington, T.S.; Martin, G.D.; Hutchings, I.M. Inkjet Printing for Pharmaceutics—A Review of Research and Manufacturing. Int. J. Pharm. 2015, 494, 554–567. [Google Scholar] [CrossRef] [PubMed]
- Vicente, M.F.; Canyada, M.; Conejero, A. Identifying Limitations for Design for Manufacturing with Desktop FFF 3D Printers. Int. J. Rapid Manuf. 2015, 5, 116. [Google Scholar] [CrossRef]
- Tan, D.; Maniruzzaman, M.; Nokhodchi, A. Advanced Pharmaceutical Applications of Hot-Melt Extrusion Coupled with Fused Deposition Modelling (FDM) 3D Printing for Personalised Drug Delivery. Pharmaceutics 2018, 10, 203. [Google Scholar] [CrossRef] [PubMed]
- Shaqour, B.; Samaro, A.; Verleije, B.; Beyers, K.; Vervaet, C.; Cos, P. Production of Drug Delivery Systems Using Fused Filament Fabrication: A Systematic Review. Pharmaceutics 2020, 12, 517. [Google Scholar] [CrossRef] [PubMed]
- Rahman, J.; Quodbach, J. Versatility on Demand–The Case for Semi-Solid Micro-Extrusion in Pharmaceutics. Adv. Drug Deliv. Rev. 2021, 172, 104–126. [Google Scholar] [CrossRef] [PubMed]
- Khan, F.A.; Narasimhan, K.; Swathi, C.S.V.; Mustak, S.; Mustafa, G.; Ahmad, M.Z.; Akhter, S. 3D Printing Technology in Customized Drug Delivery System: Current State of the Art, Prospective and the Challenges. Curr. Pharm. Des. 2019, 24, 5049–5061. [Google Scholar] [CrossRef]
- Sandler, N.; Salmela, I.; Fallarero, A.; Rosling, A.; Khajeheian, M.; Kolakovic, R.; Genina, N.; Nyman, J.; Vuorela, P. Towards Fabrication of 3D Printed Medical Devices to Prevent Biofilm Formation. Int. J. Pharm. 2014, 459, 62–64. [Google Scholar] [CrossRef] [PubMed]
- Zema, L.; Melocchi, A.; Maroni, A.; Gazzaniga, A. Three-Dimensional Printing of Medicinal Products and the Challenge of Personalized Therapy. J. Pharm. Sci. 2017, 106, 1697–1705. [Google Scholar] [CrossRef] [PubMed]
- Norman, J.; Madurawe, R.D.; Moore, C.M.V.; Khan, M.A.; Khairuzzaman, A. A New Chapter in Pharmaceutical Manufacturing: 3D-Printed Drug Products. Adv. Drug Deliv. Rev. 2017, 108, 39–50. [Google Scholar] [CrossRef]
- Genina, N.; Holländer, J.; Jukarainen, H.; Mäkilä, E.; Salonen, J.; Sandler, N. Ethylene Vinyl Acetate (EVA) as a New Drug Carrier for 3D Printed Medical Drug Delivery Devices. Eur. J. Pharm. Sci. 2016, 90, 53–63. [Google Scholar] [CrossRef] [PubMed]
- Tappa, K.; Jammalamadaka, U.; Weisman, J.; Ballard, D.; Wolford, D.; Pascual-Garrido, C.; Wolford, L.; Woodard, P.; Mills, D. 3D Printing Custom Bioactive and Absorbable Surgical Screws, Pins, and Bone Plates for Localized Drug Delivery. J. Funct. Biomater. 2019, 10, 17. [Google Scholar] [CrossRef]
- Ballard, D.H.; Weisman, J.A.; Jammalamadaka, U.; Tappa, K.; Alexander, J.S.; Griffen, F.D. Three-Dimensional Printing of Bioactive Hernia Meshes: In Vitro Proof of Principle. Surgery 2017, 161, 1479–1481. [Google Scholar] [CrossRef]
- Water, J.J.; Bohr, A.; Boetker, J.; Aho, J.; Sandler, N.; Nielsen, H.M.; Rantanen, J. Three-Dimensional Printing of Drug-Eluting Implants: Preparation of an Antimicrobial Polylactide Feedstock Material. J. Pharm. Sci. 2015, 104, 1099–1107. [Google Scholar] [CrossRef] [PubMed]
- Weisman, J.A.; Nicholson, J.C.; Tappa, K.; Jammalamadaka, U.; Wilson, C.G.; Mills, D.K. Antibiotic and Chemotherapeutic Enhanced Three-Dimensional Printer Filaments and Constructs for Biomedical Applications. Int. J. Nanomedicine 2015, 10, 357–370. [Google Scholar] [CrossRef] [PubMed]
- Fu, J.; Yu, X.; Jin, Y. 3D Printing of Vaginal Rings with Personalized Shapes for Controlled Release of Progesterone. Int. J. Pharm. 2018, 539, 75–82. [Google Scholar] [CrossRef] [PubMed]
- Mills, D.; Tappa, K.; Jammalamadaka, U.; Weisman, J.; Woerner, J. The Use of 3D Printing in the Fabrication of Nasal Stents. Inventions 2017, 3, 1. [Google Scholar] [CrossRef]
- Mathew, E.; Domínguez-Robles, J.; Stewart, S.A.; Mancuso, E.; O’Donnell, K.; Larrañeta, E.; Lamprou, D.A. Fused Deposition Modeling as an Effective Tool for Anti-Infective Dialysis Catheter Fabrication. ACS Biomater. Sci. Eng. 2019, 5, 6300–6310. [Google Scholar] [CrossRef] [PubMed]
- Tappa, K.; Jammalamadaka, U.; Ballard, D.H.; Bruno, T.; Israel, M.R.; Vemula, H.; Meacham, J.M.; Mills, D.K.; Woodard, P.K.; Weisman, J.A. Medication Eluting Devices for the Field of OBGYN (MEDOBGYN): 3D Printed Biodegradable Hormone Eluting Constructs, a Proof of Concept Study. PLoS ONE 2017, 12, e0182929. [Google Scholar] [CrossRef]
- Domínguez-Robles, J.; Mancinelli, C.; Mancuso, E.; García-Romero, I.; Gilmore, B.F.; Casettari, L.; Larrañeta, E.; Lamprou, D.A. 3D Printing of Drug-Loaded Thermoplastic Polyurethane Meshes: A Potential Material for Soft Tissue Reinforcement in Vaginal Surgery. Pharmaceutics 2020, 12, 63. [Google Scholar] [CrossRef]
- Weisman, J.; Jammalamadaka, U.; Tappa, K.; Mills, D. Doped Halloysite Nanotubes for Use in the 3D Printing of Medical Devices. Bioengineering 2017, 4, 96. [Google Scholar] [CrossRef]
- Holländer, J.; Genina, N.; Jukarainen, H.; Khajeheian, M.; Rosling, A.; Mäkilä, E.; Sandler, N. Three-Dimensional Printed PCL-Based Implantable Prototypes of Medical Devices for Controlled Drug Delivery. J. Pharm. Sci. 2016, 105, 2665–2676. [Google Scholar] [CrossRef] [PubMed]
- Chou, P.-Y.; Chou, Y.-C.; Lai, Y.-H.; Lin, Y.-T.; Lu, C.-J.; Liu, S.-J. Fabrication of Drug-Eluting Nano-Hydroxylapatite Filled Polycaprolactone Nanocomposites Using Solution-Extrusion 3D Printing Technique. Polymers 2021, 13, 318. [Google Scholar] [CrossRef] [PubMed]
- Yi, H.-G.; Choi, Y.-J.; Kang, K.S.; Hong, J.M.; Pati, R.G.; Park, M.N.; Shim, I.K.; Lee, C.M.; Kim, S.C.; Cho, D.-W. A 3D-Printed Local Drug Delivery Patch for Pancreatic Cancer Growth Suppression. J. Control. Release 2016, 238, 231–241. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Qiao, X.; Huang, R.; Chen, H.; Shi, X.; Wang, J.; Tan, W.; Tan, Z. E-Jet 3D Printed Drug Delivery Implants to Inhibit Growth and Metastasis of Orthotopic Breast Cancer. Biomaterials 2020, 230, 119618. [Google Scholar] [CrossRef]
- Holländer, J.; Hakala, R.; Suominen, J.; Moritz, N.; Yliruusi, J.; Sandler, N. 3D Printed UV Light Cured Polydimethylsiloxane Devices for Drug Delivery. Int. J. Pharm. 2018, 544, 433–442. [Google Scholar] [CrossRef]
- Salimi, S.; Wu, Y.; Barreiros, M.I.E.; Natfji, A.A.; Khaled, S.; Wildman, R.; Hart, L.R.; Greco, F.; Clark, E.A.; Roberts, C.J.; et al. A 3D Printed Drug Delivery Implant Formed from a Dynamic Supramolecular Polyurethane Formulation. Polym. Chem. 2020, 11, 3453–3464. [Google Scholar] [CrossRef]
- Qamar, N.; Abbas, N.; Irfan, M.; Hussain, A.; Arshad, M.S.; Latif, S.; Mehmood, F.; Ghori, M.U. Personalized 3D Printed Ciprofloxacin Impregnated Meshes for the Management of Hernia. J. Drug Deliv. Sci. Technol. 2019, 53, 101164. [Google Scholar] [CrossRef]
- Mau, R.; Reske, T.; Eickner, T.; Grabow, N.; Seitz, H. DLP 3D Printing of Dexamethasoneincorporated PEGDA-Based Photopolymers: Compressive Properties and Drug Release. Curr. Dir. Biomed. Eng. 2020, 6, 406–409. [Google Scholar] [CrossRef]
- Yang, Y.; Zhou, Y.; Lin, X.; Yang, Q.; Yang, G. Printability of External and Internal Structures Based on Digital Light Processing 3D Printing Technique. Pharmaceutics 2020, 12, 207. [Google Scholar] [CrossRef] [PubMed]
- Huang, W.; Zheng, Q.; Sun, W.; Xu, H.; Yang, X. Levofloxacin Implants with Predefined Microstructure Fabricated by Three-Dimensional Printing Technique. Int. J. Pharm. 2007, 339, 33–38. [Google Scholar] [CrossRef] [PubMed]
- Wu, W.; Zheng, Q.; Guo, X.; Sun, J.; Liu, Y. A Programmed Release Multi-Drug Implant Fabricated by Three-Dimensional Printing Technology for Bone Tuberculosis Therapy. Biomed. Mater. 2009, 4, 065005. [Google Scholar] [CrossRef] [PubMed]
- Wu, W.; Ye, C.; Zheng, Q.; Wu, G.; Cheng, Z. A Therapeutic Delivery System for Chronic Osteomyelitis via a Multi-Drug Implant Based on Three-Dimensional Printing Technology. J. Biomater. Appl. 2016, 31, 250–260. [Google Scholar] [CrossRef]
- Inzana, J.; Trombetta, R.; Schwarz, E.; Kates, S.; Awad, H. 3D Printed Bioceramics for Dual Antibiotic Delivery to Treat Implant-Associated Bone Infection. Eur. Cells Mater. 2015, 30, 232–247. [Google Scholar] [CrossRef] [PubMed]
- Wu, G.; Wu, W.; Zheng, Q.; Li, J.; Zhou, J.; Hu, Z. Experimental Study of PLLA/INH Slow Release Implant Fabricated by Three Dimensional Printing Technique and Drug Release Characteristics in Vitro. Biomed. Eng. Online 2014, 13, 97. [Google Scholar] [CrossRef]
- Trombetta, R.; Ninomiya, M.; El-Atawneh, I.; Knapp, E.; de Mesy Bentley, K.; Dunman, P.; Schwarz, E.; Kates, S.; Awad, H. Calcium Phosphate Spacers for the Local Delivery of Sitafloxacin and Rifampin to Treat Orthopedic Infections: Efficacy and Proof of Concept in a Mouse Model of Single-Stage Revision of Device-Associated Osteomyelitis. Pharmaceutics 2019, 11, 94. [Google Scholar] [CrossRef]
- Vorndran, E.; Klammert, U.; Ewald, A.; Barralet, J.E.; Gbureck, U. Simultaneous Immobilization of Bioactives During 3D Powder Printing of Bioceramic Drug-Release Matrices. Adv. Funct. Mater. 2010, 20, 1585–1591. [Google Scholar] [CrossRef]
- Wu, B.M.; Borland, S.W.; Giordano, R.A.; Cima, L.G.; Sachs, E.M.; Cima, M.J. Solid Free-Form Fabrication of Drug Delivery Devices. J. Control. Release 1996, 40, 77–87. [Google Scholar] [CrossRef]
- Boyer, C.J.; Woerner, J.E.; Galea, C.; Gatlin, C.A.; Ghali, G.E.; Mills, D.K.; Weisman, J.A.; McGee, D.J.; Alexander, J.S. Personalized Bioactive Nasal Supports for Postoperative Cleft Rhinoplasty. J. Oral Maxillofac. Surg. 2018, 76, 1562.e1–1562.e5. [Google Scholar] [CrossRef]
- Poudel, I.; Annaji, M.; Arnold, R.D.; Kaddoumi, A.; Shamsaei, N.; Lee, S.; Pegues, J.; Ahmadi, Z.; Samani, M.M.; Corriveau, K.; et al. Dexamethasone Eluting 3D Printed Metal Devices for Bone Injuries. Ther. Deliv. 2020, 11, 373–386. [Google Scholar] [CrossRef] [PubMed]
- Maher, S.; Kaur, G.; Lima-Marques, L.; Evdokiou, A.; Losic, D. Engineering of Micro- to Nanostructured 3D-Printed Drug-Releasing Titanium Implants for Enhanced Osseointegration and Localized Delivery of Anticancer Drugs. ACS Appl. Mater. Interfaces 2017, 9, 29562–29570. [Google Scholar] [CrossRef] [PubMed]
- Calero Castro, F.J.; Yuste, Y.; Pereira, S.; Garvín, M.D.; López García, M.Á.; Padillo, F.J.; Portilla, F. Proof of Concept, Design, and Manufacture via 3-D Printing of a Mesh with Bactericidal Capacity: Behaviour in Vitro and in Vivo. J. Tissue Eng. Regen. Med. 2019, 13, 1955–1964. [Google Scholar] [CrossRef] [PubMed]
- Visscher, L.E.; Dang, H.P.; Knackstedt, M.A.; Hutmacher, D.W.; Tran, P.A. 3D Printed Polycaprolactone Scaffolds with Dual Macro-Microporosity for Applications in Local Delivery of Antibiotics. Mater. Sci. Eng. C 2018, 87, 78–89. [Google Scholar] [CrossRef] [PubMed]
- Zhao, C.; Wang, Z.; Hua, C.; Ji, J.; Zhou, Z.; Fang, Y.; Weng, D.; Lu, L.; Pang, Y.; Sun, W. Design, Modeling and 3D Printing of a Personalized Cervix Tissue Implant with Protein Release Function. Biomed. Mater. 2020, 15, 045005. [Google Scholar] [CrossRef]
- Gbureck, U.; Vorndran, E.; Müller, F.A.; Barralet, J.E. Low Temperature Direct 3D Printed Bioceramics and Biocomposites as Drug Release Matrices. J. Control. Release 2007, 122, 173–180. [Google Scholar] [CrossRef]
- Yang, N.; Chen, H.; Han, H.; Shen, Y.; Gu, S.; He, Y.; Guo, S. 3D Printing and Coating to Fabricate a Hollow Bullet-Shaped Implant with Porous Surface for Controlled Cytoxan Release. Int. J. Pharm. 2018, 552, 91–98. [Google Scholar] [CrossRef]
- Wang, Y.; Sun, L.; Mei, Z.; Zhang, F.; He, M.; Fletcher, C.; Wang, F.; Yang, J.; Bi, D.; Jiang, Y.; et al. 3D Printed Biodegradable Implants as an Individualized Drug Delivery System for Local Chemotherapy of Osteosarcoma. Mater. Des. 2020, 186, 108336. [Google Scholar] [CrossRef]
- Leong, K.F.; Phua, K.K.S.; Chua, C.K.; Du, Z.H.; Teo, K.O.M. Fabrication of Porous Polymeric Matrix Drug Delivery Devices Using the Selective Laser Sintering Technique. Proc. Inst. Mech. Eng. Part H J. Eng. Med. 2001, 215, 191–201. [Google Scholar] [CrossRef]
- Martin, V.; Ribeiro, I.A.; Alves, M.M.; Gonçalves, L.; Claudio, R.A.; Grenho, L.; Fernandes, M.H.; Gomes, P.; Santos, C.F.; Bettencourt, A.F. Engineering a Multifunctional 3D-Printed PLA-Collagen-Minocycline-NanoHydroxyapatite Scaffold with Combined Antimicrobial and Osteogenic Effects for Bone Regeneration. Mater. Sci. Eng. C 2019, 101, 15–26. [Google Scholar] [CrossRef]
- Boyer, C.J.; Ballard, D.H.; Weisman, J.A.; Hurst, S.; McGee, D.J.; Mills, D.K.; Woerner, J.E.; Jammalamadaka, U.; Tappa, K.; Alexander, J.S. Three-Dimensional Printing Antimicrobial and Radiopaque Constructs. 3D Print. Addit. Manuf. 2018, 5, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Ngo, T.T.; Hoffman, L.; Hoople, G.D.; Trevena, W.; Shakya, U.; Barr, G. Surface Morphology and Drug Loading Characterization of 3D-Printed Methacrylate-Based Polymer Facilitated by Supercritical Carbon Dioxide. J. Supercrit. Fluids 2020, 160, 104786. [Google Scholar] [CrossRef]
- Stewart, S.; Domínguez-Robles, J.; McIlorum, V.; Mancuso, E.; Lamprou, D.; Donnelly, R.; Larrañeta, E. Development of a Biodegradable Subcutaneous Implant for Prolonged Drug Delivery Using 3D Printing. Pharmaceutics 2020, 12, 105. [Google Scholar] [CrossRef]
- Stewart, S.A.; Domínguez-Robles, J.; McIlorum, V.J.; Gonzalez, Z.; Utomo, E.; Mancuso, E.; Lamprou, D.A.; Donnelly, R.F.; Larrañeta, E. Poly(Caprolactone)-Based Coatings on 3D-Printed Biodegradable Implants: A Novel Strategy to Prolong Delivery of Hydrophilic Drugs. Mol. Pharm. 2020, 17, 3487–3500. [Google Scholar] [CrossRef] [PubMed]
- Won, J.Y.; Kim, J.; Gao, G.; Kim, J.; Jang, J.; Park, Y.-H.; Cho, D.-W. 3D Printing of Drug-Loaded Multi-Shell Rods for Local Delivery of Bevacizumab and Dexamethasone: A Synergetic Therapy for Retinal Vascular Diseases. Acta Biomater. 2020, 116, 174–185. [Google Scholar] [CrossRef] [PubMed]
- Arany, P.; Papp, I.; Zichar, M.; Csontos, M.; Elek, J.; Regdon, G.; Budai, I.; Béres, M.; Gesztelyi, R.; Fehér, P.; et al. In Vitro Tests of FDM 3D-Printed Diclofenac Sodium-Containing Implants. Molecules 2020, 25, 5889. [Google Scholar] [CrossRef] [PubMed]
- Murphy, S.V.; Atala, A. 3D Bioprinting of Tissues and Organs. Nat. Biotechnol. 2014, 32, 773–785. [Google Scholar] [CrossRef] [PubMed]
- Mandrycky, C.; Wang, Z.; Kim, K.; Kim, D.-H. 3D Bioprinting for Engineering Complex Tissues. Biotechnol. Adv. 2016, 34, 422–434. [Google Scholar] [CrossRef]
- Ozbolat, I.T.; Peng, W.; Ozbolat, V. Application Areas of 3D Bioprinting. Drug Discov. Today 2016, 21, 1257–1271. [Google Scholar] [CrossRef]
- Zhang, Y.S.; Yue, K.; Aleman, J.; Mollazadeh-Moghaddam, K.; Bakht, S.M.; Yang, J.; Jia, W.; Dell’Erba, V.; Assawes, P.; Shin, S.R.; et al. 3D Bioprinting for Tissue and Organ Fabrication. Ann. Biomed. Eng. 2017, 45, 148–163. [Google Scholar] [CrossRef]
- Bernhard, J.-C.; Isotani, S.; Matsugasumi, T.; Duddalwar, V.; Hung, A.J.; Suer, E.; Baco, E.; Satkunasivam, R.; Djaladat, H.; Metcalfe, C.; et al. Personalized 3D Printed Model of Kidney and Tumor Anatomy: A Useful Tool for Patient Education. World J. Urol. 2016, 34, 337–345. [Google Scholar] [CrossRef]
- Atalay, H.A.; Canat, H.L.; Ülker, V.; Alkan, İ.; Özkuvanci, Ü.; Altunrende, F. Impact of Personalized Three-Dimensional (3D) Printed Pelvicalyceal System Models on Patient Information in Percutaneous Nephrolithotripsy Surgery: A Pilot Study. Int. Braz. J. Urol. 2017, 43, 470–475. [Google Scholar] [CrossRef]
- Tominaga, T.; Takagi, K.; Takeshita, H.; Miyamoto, T.; Matsuo, A.; Shimoda, K.; Matsumoto, K.; Hidaka, S.; Yamasaki, N.; Sawai, T.; et al. Usefulness Of Three-Dimensional Printing Models for Patients with Stoma Construction. Case Rep. Gastroenterol. 2016, 10, 61–66. [Google Scholar] [CrossRef]
- Ganguli, A.; Pagan-Diaz, G.J.; Grant, L.; Cvetkovic, C.; Bramlet, M.; Vozenilek, J.; Kesavadas, T.; Bashir, R. 3D Printing for Preoperative Planning and Surgical Training: A Review. Biomed. Microdevices 2018, 20, 65. [Google Scholar] [CrossRef] [PubMed]
- Zeng, C.; Xing, W.; Wu, Z.; Huang, H.; Huang, W. A Combination of Three-Dimensional Printing and Computer-Assisted Virtual Surgical Procedure for Preoperative Planning of Acetabular Fracture Reduction. Injury 2016, 47, 2223–2227. [Google Scholar] [CrossRef] [PubMed]
- Wake, N.; Rude, T.; Kang, S.K.; Stifelman, M.D.; Borin, J.F.; Sodickson, D.K.; Huang, W.C.; Chandarana, H. 3D Printed Renal Cancer Models Derived from MRI Data: Application in Pre-Surgical Planning. Abdom. Radiol. 2017, 42, 1501–1509. [Google Scholar] [CrossRef] [PubMed]
- Pacione, D.; Tanweer, O.; Berman, P.; Harter, D.H. The Utility of a Multimaterial 3D Printed Model for Surgical Planning of Complex Deformity of the Skull Base and Craniovertebral Junction. J. Neurosurg. 2016, 125, 1194–1197. [Google Scholar] [CrossRef] [PubMed]
- Wilasrusmee, C.; Suvikrom, J.; Suthakorn, J.; Lertsithichai, P.; Sitthiseriprapip, K.; Proprom, N.; Kittur, D.S. Three-Dimensional Aortic Aneurysm Model and Endovascular Repair: An Educational Tool for Surgical Trainees. Int. J. Angiol. 2008, 17, 129–133. [Google Scholar] [CrossRef] [PubMed]
- Yoo, S.-J.; Spray, T.; Austin, E.H.; Yun, T.-J.; van Arsdell, G.S. Hands-on Surgical Training of Congenital Heart Surgery Using 3-Dimensional Print Models. J. Thorac. Cardiovasc. Surg. 2017, 153, 1530–1540. [Google Scholar] [CrossRef]
- Leary, O.P.; Crozier, J.; Liu, D.D.; Niu, T.; Pertsch, N.J.; Camara-Quintana, J.Q.; Svokos, K.A.; Syed, S.; Telfeian, A.E.; Oyelese, A.A.; et al. Three-Dimensional Printed Anatomic Modeling for Surgical Planning and Real-Time Operative Guidance in Complex Primary Spinal Column Tumors: Single-Center Experience and Case Series. World Neurosurg. 2021, 145, e116–e126. [Google Scholar] [CrossRef]
- Itagaki, M.W. Using 3D Printed Models for Planning and Guidance during Endovascular Intervention: A Technical Advance. Diagnostic Interv. Radiol. 2015, 21, 338–341. [Google Scholar] [CrossRef]
- Jin, Y.; Plott, J.; Chen, R.; Wensman, J.; Shih, A. Additive Manufacturing of Custom Orthoses and Prostheses–A Review. Procedia CIRP 2015, 36, 199–204. [Google Scholar] [CrossRef]
- Ruiters, S.; Sun, Y.; de Jong, S.; Politis, C.; Mombaerts, I. Computer-Aided Design and Three-Dimensional Printing in the Manufacturing of an Ocular Prosthesis. Br. J. Ophthalmol. 2016, 100, 879–881. [Google Scholar] [CrossRef]
- Nuseir, A.; Hatamleh, M.M.; Alnazzawi, A.; Al-Rabab’ah, M.; Kamel, B.; Jaradat, E. Direct 3D Printing of Flexible Nasal Prosthesis: Optimized Digital Workflow from Scan to Fit. J. Prosthodont. 2019, 28, 10–14. [Google Scholar] [CrossRef] [PubMed]
- Tunchel, S.; Blay, A.; Kolerman, R.; Mijiritsky, E.; Shibli, J.A. 3D Printing/Additive Manufacturing Single Titanium Dental Implants: A Prospective Multicenter Study with 3 Years of Follow-Up. Int. J. Dent. 2016, 2016, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Vorndran, E.; Moseke, C.; Gbureck, U. 3D Printing of Ceramic Implants. MRS Bull. 2015, 40, 127–136. [Google Scholar] [CrossRef]
- Mohammed, M.I.; Fitzpatrick, A.P.; Malyala, S.K.; Gibson, I. Customised Design and Development of Patient Specific 3D Printed Whole Mandible Implant. In Proceedings of the SFF Symp 2016: Proceedings of the 27th Annual International Solid Freeform Fabrication Symposium, Austin, TX, USA, 8–10 August 2016; pp. 1708–1717. [Google Scholar]
- Okafor-Muo, O.L.; Hassanin, H.; Kayyali, R.; ElShaer, A. 3D Printing of Solid Oral Dosage Forms: Numerous Challenges With Unique Opportunities. J. Pharm. Sci. 2020, 109, 3535–3550. [Google Scholar] [CrossRef]
- Khaled, S.A.; Burley, J.C.; Alexander, M.R.; Yang, J.; Roberts, C.J. 3D Printing of Five-in-One Dose Combination Polypill with Defined Immediate and Sustained Release Profiles. J. Control. Release 2015, 217, 308–314. [Google Scholar] [CrossRef] [PubMed]
- Kempin, W.; Domsta, V.; Grathoff, G.; Brecht, I.; Semmling, B.; Tillmann, S.; Weitschies, W.; Seidlitz, A. Immediate Release 3D-Printed Tablets Produced Via Fused Deposition Modeling of a Thermo-Sensitive Drug. Pharm. Res. 2018, 35, 124. [Google Scholar] [CrossRef]
- Okwuosa, T.C.; Pereira, B.C.; Arafat, B.; Cieszynska, M.; Isreb, A.; Alhnan, M.A. Fabricating a Shell-Core Delayed Release Tablet Using Dual FDM 3D Printing for Patient-Centred Therapy. Pharm. Res. 2017, 34, 427–437. [Google Scholar] [CrossRef]
- Maroni, A.; Melocchi, A.; Parietti, F.; Foppoli, A.; Zema, L.; Gazzaniga, A. 3D Printed Multi-Compartment Capsular Devices for Two-Pulse Oral Drug Delivery. J. Control. Release 2017, 268, 10–18. [Google Scholar] [CrossRef]
- Matijašić, G.; Gretić, M.; Vinčić, J.; Poropat, A.; Cuculić, L.; Rahelić, T. Design and 3D Printing of Multi-Compartmental PVA Capsules for Drug Delivery. J. Drug Deliv. Sci. Technol. 2019, 52, 677–686. [Google Scholar] [CrossRef]
- Eleftheriadis, G.K.; Ritzoulis, C.; Bouropoulos, N.; Tzetzis, D.; Andreadis, D.A.; Boetker, J.; Rantanen, J.; Fatouros, D.G. Unidirectional Drug Release from 3D Printed Mucoadhesive Buccal Films Using FDM Technology: In Vitro and Ex Vivo Evaluation. Eur. J. Pharm. Biopharm. 2019, 144, 180–192. [Google Scholar] [CrossRef] [PubMed]
- Jamróz, W.; Kurek, M.; Łyszczarz, E.; Szafraniec, J.; Knapik-Kowalczuk, J.; Syrek, K.; Paluch, M.; Jachowicz, R. 3D Printed Orodispersible Films with Aripiprazole. Int. J. Pharm. 2017, 533, 413–420. [Google Scholar] [CrossRef] [PubMed]
- Luzuriaga, M.A.; Berry, D.R.; Reagan, J.C.; Smaldone, R.A.; Gassensmith, J.J. Biodegradable 3D Printed Polymer Microneedles for Transdermal Drug Delivery. Lab Chip 2018, 18, 1223–1230. [Google Scholar] [CrossRef] [PubMed]
- Economidou, S.N.; Lamprou, D.A.; Douroumis, D. 3D Printing Applications for Transdermal Drug Delivery. Int. J. Pharm. 2018, 544, 415–424. [Google Scholar] [CrossRef] [PubMed]
- Pere, C.P.P.; Economidou, S.N.; Lall, G.; Ziraud, C.; Boateng, J.S.; Alexander, B.D.; Lamprou, D.A.; Douroumis, D. 3D Printed Microneedles for Insulin Skin Delivery. Int. J. Pharm. 2018, 544, 425–432. [Google Scholar] [CrossRef]
- Engelhardt, S.; Sauerzapf, S.; Preim, B.; Karck, M.; Wolf, I.; De Simone, R. Flexible and Comprehensive Patient-Specific Mitral Valve Silicone Models with Chordae Tendineae Made from 3D-Printable Molds. Int. J. Comput. Assist. Radiol. Surg. 2019, 14, 1177–1186. [Google Scholar] [CrossRef] [PubMed]
- Gildea, T.R.; Young, B.P.; Machuzak, M.S. Application of 3D Printing for Patient-Specific Silicone Stents: 1-Year Follow-Up on 2 Patients. Respiration 2018, 96, 488–494. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Ruan, X.; Li, H.; Kathuria, H.; Du, G.; Kang, L. Fabrication of Non-Dissolving Analgesic Suppositories Using 3D Printed Moulds. Int. J. Pharm. 2016, 513, 717–724. [Google Scholar] [CrossRef]
- Tan, Y.J.N.; Yong, W.P.; Kochhar, J.S.; Khanolkar, J.; Yao, X.; Sun, Y.; Ao, C.K.; Soh, S. On-Demand Fully Customizable Drug Tablets via 3D Printing Technology for Personalized Medicine. J. Control. Release 2020, 322, 42–52. [Google Scholar] [CrossRef]
- Bosman, W.M.P.F.; Borger van der Burg, B.L.S.; Schuttevaer, H.M.; Thoma, S.; Hedeman Joosten, P.P. Infections of Intravascular Bare Metal Stents: A Case Report and Review of Literature. Eur. J. Vasc. Endovasc. Surg. 2014, 47, 87–99. [Google Scholar] [CrossRef]
- Folch, E.; Keyes, C. Airway Stents. Ann. Cardiothorac. Surg. 2018, 7, 273–283. [Google Scholar] [CrossRef]
- Maki, D. Engineering out the Risk of Infection with Urinary Catheters. Emerg. Infect. Dis. 2001, 7, 342–347. [Google Scholar] [CrossRef]
- Mathew, E.; Domínguez-Robles, J.; Larrañeta, E.; Lamprou, D.A. Fused Deposition Modelling as a Potential Tool for Antimicrobial Dialysis Catheters Manufacturing: New Trends vs. Conventional Approaches. Coatings 2019, 9, 515. [Google Scholar] [CrossRef]
- Weisman, J.A.; Ballard, D.H.; Jammalamadaka, U.; Tappa, K.; Sumerel, J.; D’Agostino, H.B.; Mills, D.K.; Woodard, P.K. 3D Printed Antibiotic and Chemotherapeutic Eluting Catheters for Potential Use in Interventional Radiology. Acad. Radiol. 2019, 26, 270–274. [Google Scholar] [CrossRef]
- Wu, W.; Song, X.; Liang, J.; Xia, R.; Qian, G.; Fang, D. Mechanical Properties of Anti-Tetrachiral Auxetic Stents. Compos. Struct. 2018, 185, 381–392. [Google Scholar] [CrossRef]
- Busch, J.D.; Schröder, H.; Sellenschloh, K.; Adam, G.; Ittrich, H.; Huber, G. Test Method for Mechanical Properties of Implantable Catheters According to DIN 10555-3. J. Mech. Behav. Biomed. Mater. 2018, 82, 183–186. [Google Scholar] [CrossRef] [PubMed]
- Bilian, X. Intrauterine Devices. Best Pract. Res. Clin. Obstet. Gynaecol. 2002, 16, 155–168. [Google Scholar] [CrossRef] [PubMed]
- Boortz, H.E.; Margolis, D.J.A.; Ragavendra, N.; Patel, M.K.; Kadell, B.M. Migration of Intrauterine Devices: Radiologic Findings and Implications for Patient Care. RadioGraphics 2012, 32, 335–352. [Google Scholar] [CrossRef] [PubMed]
- Goldstuck, N. Dimensional Analysis of the Endometrial Cavity: How Many Dimensions Should the Ideal Intrauterine Device or System Have? Int. J. Womens. Health 2018, 10, 165–168. [Google Scholar] [CrossRef]
- Farmer, Z.-L.; Utomo, E.; Domínguez-Robles, J.; Mancinelli, C.; Mathew, E.; Larrañeta, E.; Lamprou, D.A. 3D Printed Estradiol-Eluting Urogynecological Mesh Implants: Influence of Material and Mesh Geometry on Their Mechanical Properties. Int. J. Pharm. 2021, 593, 120145. [Google Scholar] [CrossRef]
- Gitelis, S.; Brebach, G.T. The Treatment of Chronic Osteomyelitis with a Biodegradable Antibiotic-Impregnated Implant. J. Orthop. Surg. 2002, 10, 53–60. [Google Scholar] [CrossRef] [PubMed]
- Montanaro, L.; Testoni, F.; Poggi, A.; Visai, L.; Speziale, P.; Arciola, C.R. Emerging Pathogenetic Mechanisms of the Implant-Related Osteomyelitis by Staphylococcus Aureus. Int. J. Artif. Organs 2011, 34, 781–788. [Google Scholar] [CrossRef]
- Wu, W.; Zheng, Q.; Guo, X.; Huang, W. The Controlled-Releasing Drug Implant Based on the Three Dimensional Printing Technology: Fabrication and Properties of Drug Releasing in Vivo. J. Wuhan Univ. Technol. Sci. Ed. 2009, 24, 977–981. [Google Scholar] [CrossRef]
- Zhu, M.; Li, K.; Zhu, Y.; Zhang, J.; Ye, X. 3D-Printed Hierarchical Scaffold for Localized Isoniazid/Rifampin Drug Delivery and Osteoarticular Tuberculosis Therapy. Acta Biomater. 2015, 16, 145–155. [Google Scholar] [CrossRef]
- Li, K.; Zhu, M.; Xu, P.; Xi, Y.; Cheng, Z.; Zhu, Y.; Ye, X. Three-Dimensionally Plotted MBG/PHBHHx Composite Scaffold for Antitubercular Drug Delivery and Tissue Regeneration. J. Mater. Sci. Mater. Med. 2015, 26, 102. [Google Scholar] [CrossRef]
- Shim, J.-H.; Kim, M.-J.; Park, J.Y.; Pati, R.G.; Yun, Y.-P.; Kim, S.E.; Song, H.-R.; Cho, D.-W. Three-Dimensional Printing of Antibiotics-Loaded Poly-ε-Caprolactone/Poly(Lactic-Co-Glycolic Acid) Scaffolds for Treatment of Chronic Osteomyelitis. Tissue Eng. Regen. Med. 2015, 12, 283–293. [Google Scholar] [CrossRef]
- Han, C.; Yao, Y.; Cheng, X.; Luo, J.; Luo, P.; Wang, Q.; Yang, F.; Wei, Q.; Zhang, Z. Electrophoretic Deposition of Gentamicin-Loaded Silk Fibroin Coatings on 3D-Printed Porous Cobalt–Chromium–Molybdenum Bone Substitutes to Prevent Orthopedic Implant Infections. Biomacromolecules 2017, 18, 3776–3787. [Google Scholar] [CrossRef]
- Wu, C.; Luo, Y.; Cuniberti, G.; Xiao, Y.; Gelinsky, M. Three-Dimensional Printing of Hierarchical and Tough Mesoporous Bioactive Glass Scaffolds with a Controllable Pore Architecture, Excellent Mechanical Strength and Mineralization Ability. Acta Biomater. 2011, 7, 2644–2650. [Google Scholar] [CrossRef]
- Costa, P.F.; Puga, A.M.; Díaz-Gomez, L.; Concheiro, A.; Busch, D.H.; Alvarez-Lorenzo, C. Additive Manufacturing of Scaffolds with Dexamethasone Controlled Release for Enhanced Bone Regeneration. Int. J. Pharm. 2015, 496, 541–550. [Google Scholar] [CrossRef]
- Farto-Vaamonde, X.; Auriemma, G.; Aquino, R.P.; Concheiro, A.; Alvarez-Lorenzo, C. Post-Manufacture Loading of Filaments and 3D Printed PLA Scaffolds with Prednisolone and Dexamethasone for Tissue Regeneration Applications. Eur. J. Pharm. Biopharm. 2019, 141, 100–110. [Google Scholar] [CrossRef]
- Inzana, J.A.; Olvera, D.; Fuller, S.M.; Kelly, J.P.; Graeve, O.A.; Schwarz, E.M.; Kates, S.L.; Awad, H.A. 3D Printing of Composite Calcium Phosphate and Collagen Scaffolds for Bone Regeneration. Biomaterials 2014, 35, 4026–4034. [Google Scholar] [CrossRef]
- Lee, J.-H.; Baik, J.-M.; Yu, Y.-S.; Kim, J.H.; Ahn, C.B.; Son, K.H.; Kim, J.-H.; Choi, E.S.; Lee, J.W. Development of a Heat Labile Antibiotic Eluting 3D Printed Scaffold for the Treatment of Osteomyelitis. Sci. Rep. 2020, 10, 7554. [Google Scholar] [CrossRef]
- Wolinsky, J.B.; Colson, Y.L.; Grinstaff, M.W. Local Drug Delivery Strategies for Cancer Treatment: Gels, Nanoparticles, Polymeric Films, Rods, and Wafers. J. Control. Release 2012, 159, 14–26. [Google Scholar] [CrossRef] [PubMed]
- Baylón, K.; Rodríguez-Camarillo, P.; Elías-Zúñiga, A.; Díaz-Elizondo, J.; Gilkerson, R.; Lozano, K. Past, Present and Future of Surgical Meshes: A Review. Membranes 2017, 7, 47. [Google Scholar] [CrossRef] [PubMed]
- Ballard, D.H.; Jammalamadaka, U.; Tappa, K.; Weisman, J.A.; Boyer, C.J.; Alexander, J.S.; Woodard, P.K. 3D Printing of Surgical Hernia Meshes Impregnated with Contrast Agents: In Vitro Proof of Concept with Imaging Characteristics on Computed Tomography. 3D Print. Med. 2018, 4, 13. [Google Scholar] [CrossRef] [PubMed]
- Kempin, W.; Franz, C.; Koster, L.-C.; Schneider, F.; Bogdahn, M.; Weitschies, W.; Seidlitz, A. Assessment of Different Polymers and Drug Loads for Fused Deposition Modeling of Drug Loaded Implants. Eur. J. Pharm. Biopharm. 2017, 115, 84–93. [Google Scholar] [CrossRef] [PubMed]
- Ranganathan, S.I.; Kohama, C.; Mercurio, T.; Salvatore, A.; Benmassaoud, M.M.; Kim, T.W.B. Effect of Temperature and Ultraviolet Light on the Bacterial Kill Effectiveness of Antibiotic-Infused 3D Printed Implants. Biomed. Microdevices 2020, 22, 59. [Google Scholar] [CrossRef]
- Guerra, A.J.; Cano, P.; Rabionet, M.; Puig, T.; Ciurana, J. Effects of Different Sterilization Processes on the Properties of a Novel 3D-Printed Polycaprolactone Stent. Polym. Adv. Technol. 2018, 29, 2327–2335. [Google Scholar] [CrossRef]
- Diment, L.E.; Thompson, M.S.; Bergmann, J.H.M. Clinical Efficacy and Effectiveness of 3D Printing: A Systematic Review. BMJ Open 2017, 7. [Google Scholar] [CrossRef]
- Goyanes, A.; Madla, C.M.; Umerji, A.; Duran Piñeiro, G.; Giraldez Montero, J.M.; Lamas Diaz, M.J.; Gonzalez Barcia, M.; Taherali, F.; Sánchez-Pintos, P.; Couce, M.L.; et al. Automated Therapy Preparation of Isoleucine Formulations Using 3D Printing for the Treatment of MSUD: First Single-Centre, Prospective, Crossover Study in Patients. Int. J. Pharm. 2019, 567, 118497. [Google Scholar] [CrossRef]
- Lee, U.L.; Lim, J.Y.; Park, S.N.; Choi, B.H.; Kang, H.; Choi, W.C. A Clinical Trial to Evaluate the Efficacy and Safety of 3d Printed Bioceramic Implants for the Reconstruction of Zygomatic Bone Defects. Materials 2020, 13, 4515. [Google Scholar] [CrossRef]
- Yu, D.G.; Zhu, L.-M.; Branford-White, C.J.; Yang, X.L. Three-Dimensional Printing in Pharmaceutics: Promises and Problems. J. Pharm. Sci. 2008, 97, 3666–3690. [Google Scholar] [CrossRef]
- Kotta, S.; Nair, A.; Alsabeelah, N. 3D Printing Technology in Drug Delivery: Recent Progress and Application. Curr. Pharm. Des. 2019, 24, 5039–5048. [Google Scholar] [CrossRef] [PubMed]
- Reddy, C.V.; V., B.; Venkatesh, M.P.; Pramod Kumar, T.M. First FDA Approved 3D Printed Drug Paved New Path for Increased Precision in Patient Care. Appl. Clin. Res. Clin. Trials Regul. Aff. 2020, 7, 93–103. [Google Scholar] [CrossRef]
- Food and Drug Administration. Technical Considerations for Additive Manufactured Medical Devices: Guidance for Industry and Food and Drug Administration Staff; Food and Drug Administration: Silver Spring, MD, USA, 2017.
- Di Prima, M.; Coburn, J.; Hwang, D.; Kelly, J.; Khairuzzaman, A.; Ricles, L. Additively Manufactured Medical Products–the FDA Perspective. 3D Print. Med. 2016, 2, 1. [Google Scholar] [CrossRef]
- Morrison, R.J.; Kashlan, K.N.; Flanangan, C.L.; Wright, J.K.; Green, G.E.; Hollister, S.J.; Weatherwax, K.J. Regulatory Considerations in the Design and Manufacturing of Implantable 3D-Printed Medical Devices. Clin. Transl. Sci. 2015, 8, 594–600. [Google Scholar] [CrossRef] [PubMed]
- Ricles, L.M.; Coburn, J.C.; Di Prima, M.; Oh, S.S. Regulating 3D-Printed Medical Products. Sci. Transl. Med. 2018, 10, eaan6521. [Google Scholar] [CrossRef] [PubMed]
- Adamo, J.E.; Grayson, W.L.; Hatcher, H.; Brown, J.S.; Thomas, A.; Hollister, S.; Steele, S.J. Regulatory Interfaces Surrounding the Growing Field of Additive Manufacturing of Medical Devices and Biologic Products. J. Clin. Transl. Sci. 2018, 2, 301–304. [Google Scholar] [CrossRef] [PubMed]
- Horst, A.; McDonald, F. Uncertain But Not Unregulated: Medical Product Regulation in the Light of Three-Dimensional Printed Medical Products. 3D Print. Addit. Manuf. 2020, 7, 248–257. [Google Scholar] [CrossRef]
- Everett, H. Triastek Receives FDA IND Clearance for 3D Printed Drug to Treat Rheumatoid Arthritis. Available online: https://3dprintingindustry.com/news/triastek-receives-fda-ind-clearance-for-3d-printed-drug-to-treat-rheumatoid-arthritis-184159/ (accessed on 26 June 2021).

| Printing Technique | Advantages | Disadvantages |
|---|---|---|
| INK | + low costs + fast production + multimaterial printing + no need for supporting structures + low temperature process (suitable for thermolabile drugs) + high porosity | − requires postprocessing (drying, powder removal) − low mechanical properties − requires suitable viscosity of ink − powder wastage |
| FDM | + low costs + widely available and compact equipment + multimaterial printing + does not require postprocessing (except for usage of support) + good mechanical properties | − lower resolution − need for supporting structures (depending on printed geometry) − high-temperature process (thermal degradation of drug and excipients) − requires previous filament fabrication |
| EXT | + low costs + multimaterial printing + low temperature process (suitable for thermolabile drugs) + high drug loading | − limited resolution (depending on nozzle size) − requires postprocessing (e.g., drying) − low mechanical properties − requires suitable viscosity of semisolids − risk of nozzle clogging |
| SLA, DLP | + high resolution and accuracy + fast production | − potential material toxicity − requires postprocessing − need for supporting structures − limited material selection − costly equipment |
| SLS, SLM | + high resolution and precision + fast production + no need for supporting structures + highly controllable internal microstructures | − expensive − requires postprocessing − requires suitable particle size − high energy input (degradation of drug and excipients) − wastage of unsintered powder (recycling?) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Domsta, V.; Seidlitz, A. 3D-Printing of Drug-Eluting Implants: An Overview of the Current Developments Described in the Literature. Molecules 2021, 26, 4066. https://doi.org/10.3390/molecules26134066
Domsta V, Seidlitz A. 3D-Printing of Drug-Eluting Implants: An Overview of the Current Developments Described in the Literature. Molecules. 2021; 26(13):4066. https://doi.org/10.3390/molecules26134066
Chicago/Turabian StyleDomsta, Vanessa, and Anne Seidlitz. 2021. "3D-Printing of Drug-Eluting Implants: An Overview of the Current Developments Described in the Literature" Molecules 26, no. 13: 4066. https://doi.org/10.3390/molecules26134066