A NMR-Based Metabonomics Approach to Determine Protective Effect of a Combination of Multiple Components Derived from Naodesheng on Ischemic Stroke Rats

Abstract
:1. Introduction
2. Results
2.1. Neurobehavioral Dysfunction Evaluation of TCNDS on MCAO Rats
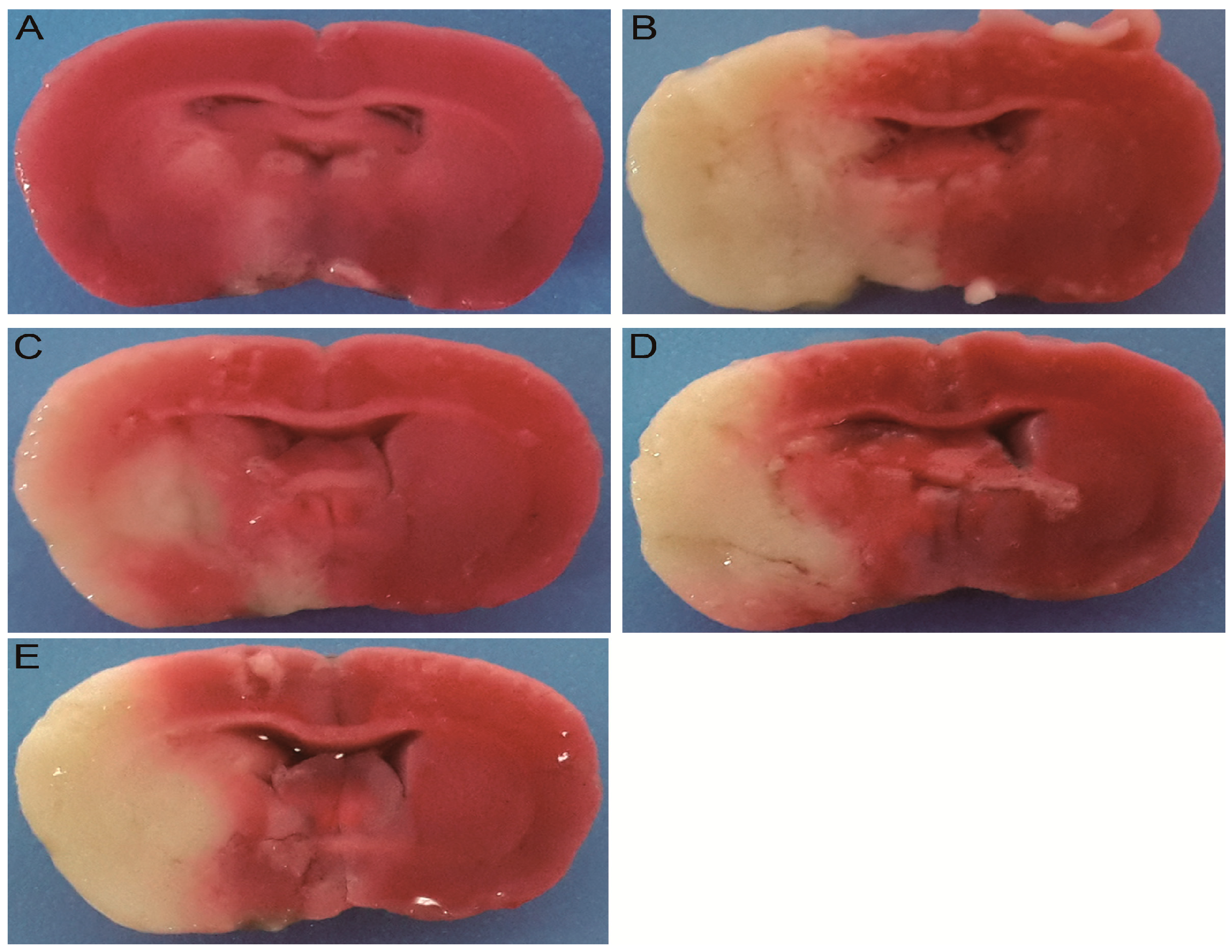
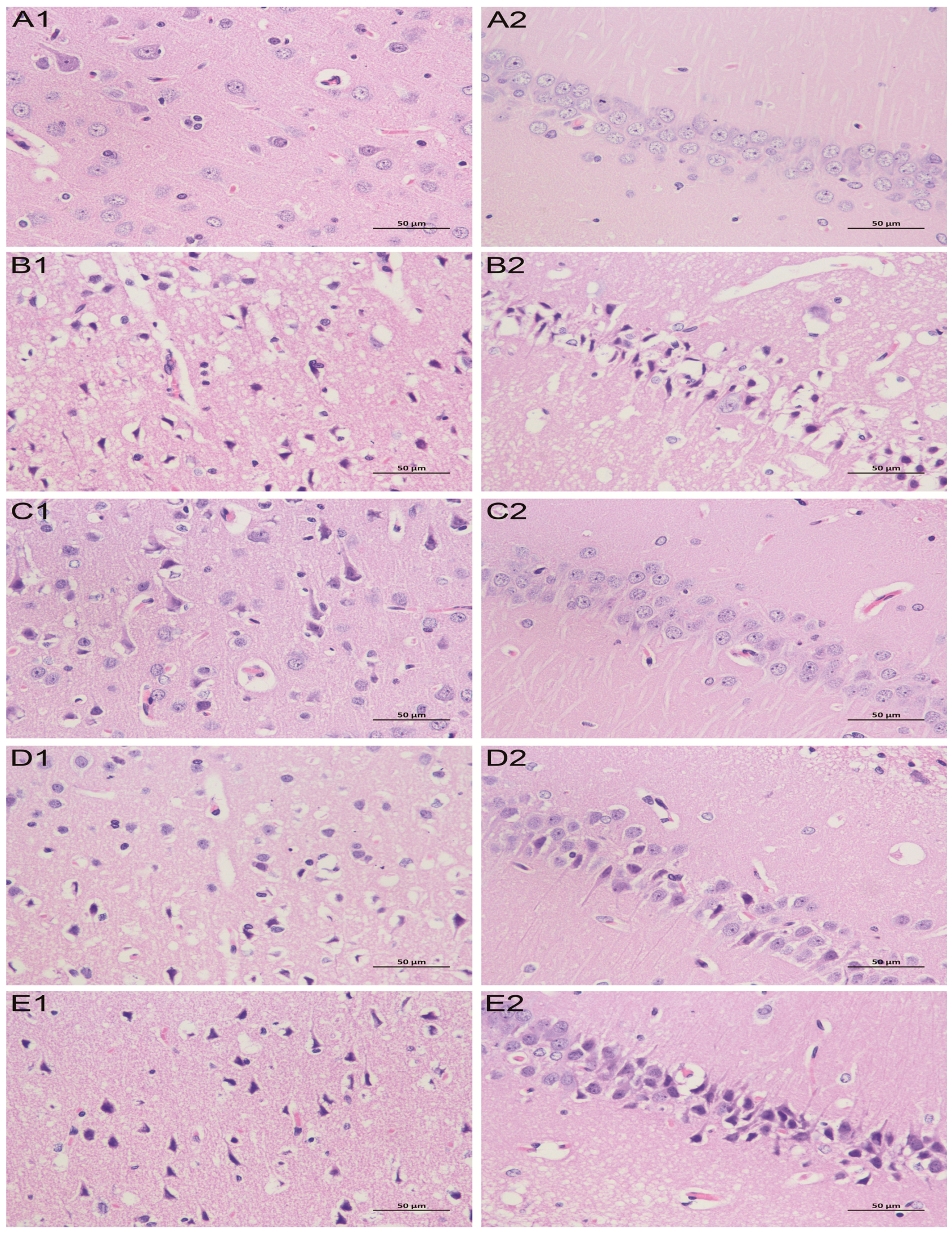
2.2. Effect of TCNDS on Cerebral Infarct Area and Pathological Changes in MACO Rats
2.3. Effect of TCNDS on Plasma LDH, MDA and SOD Levels in MCAO Rats
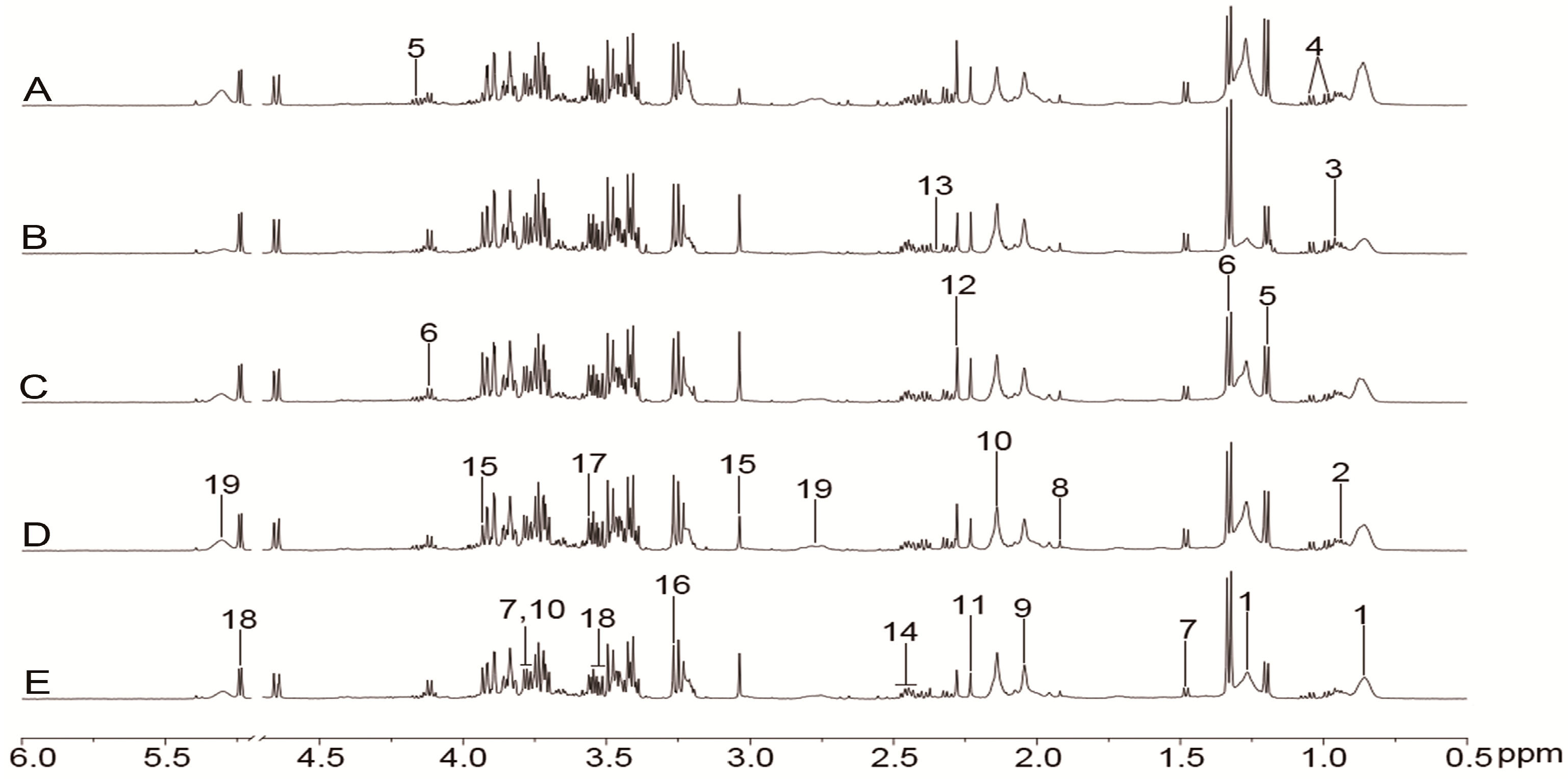
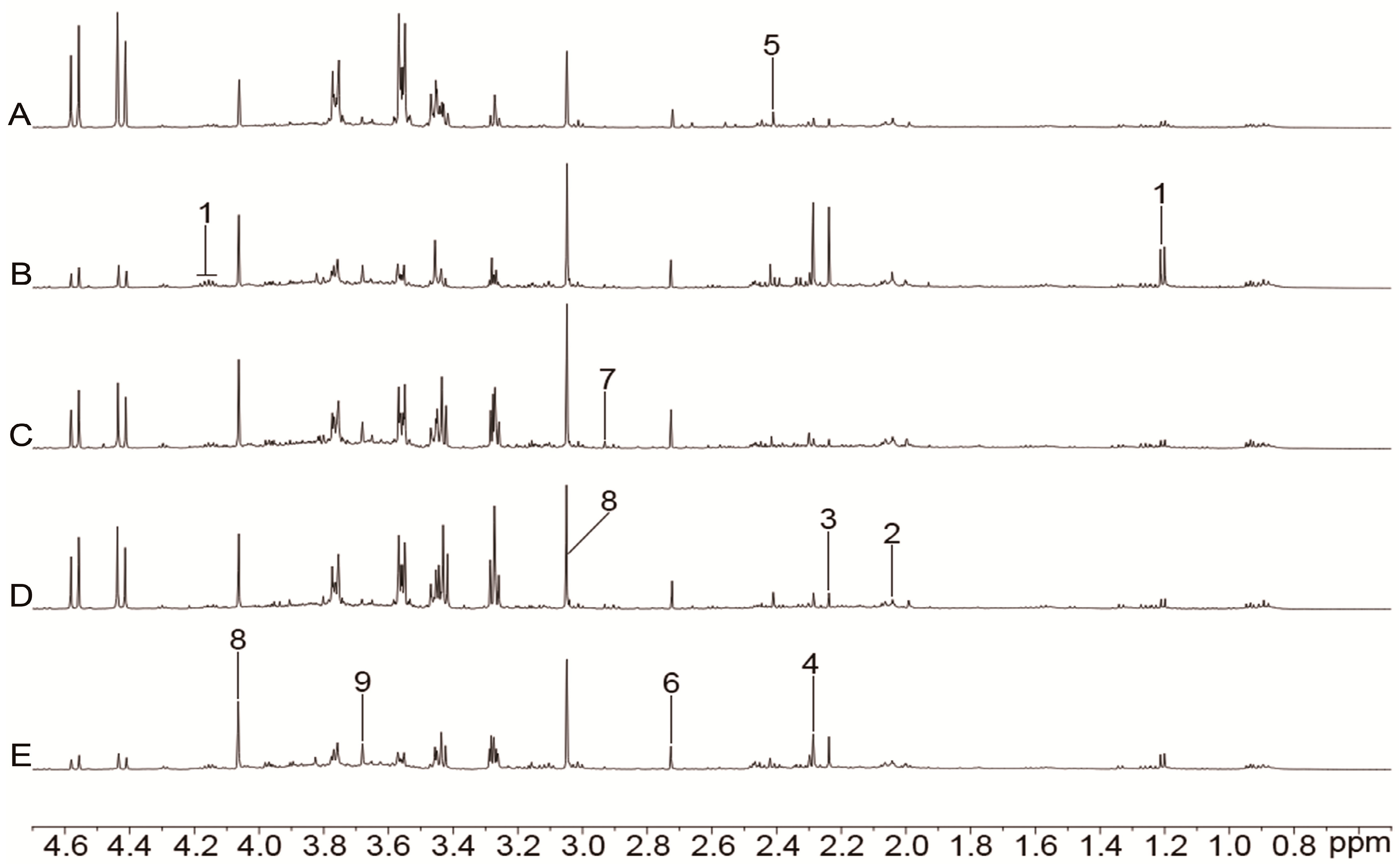
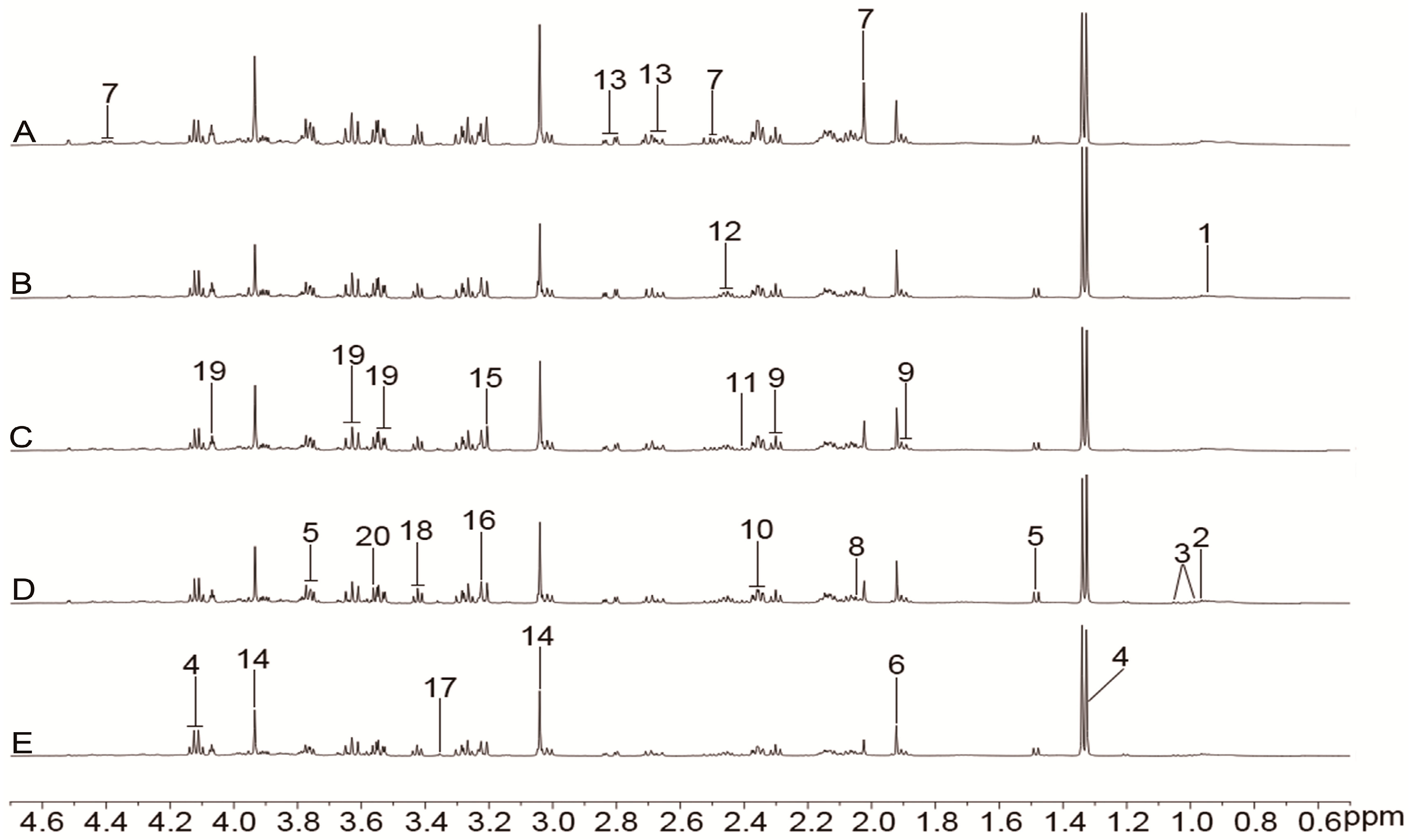
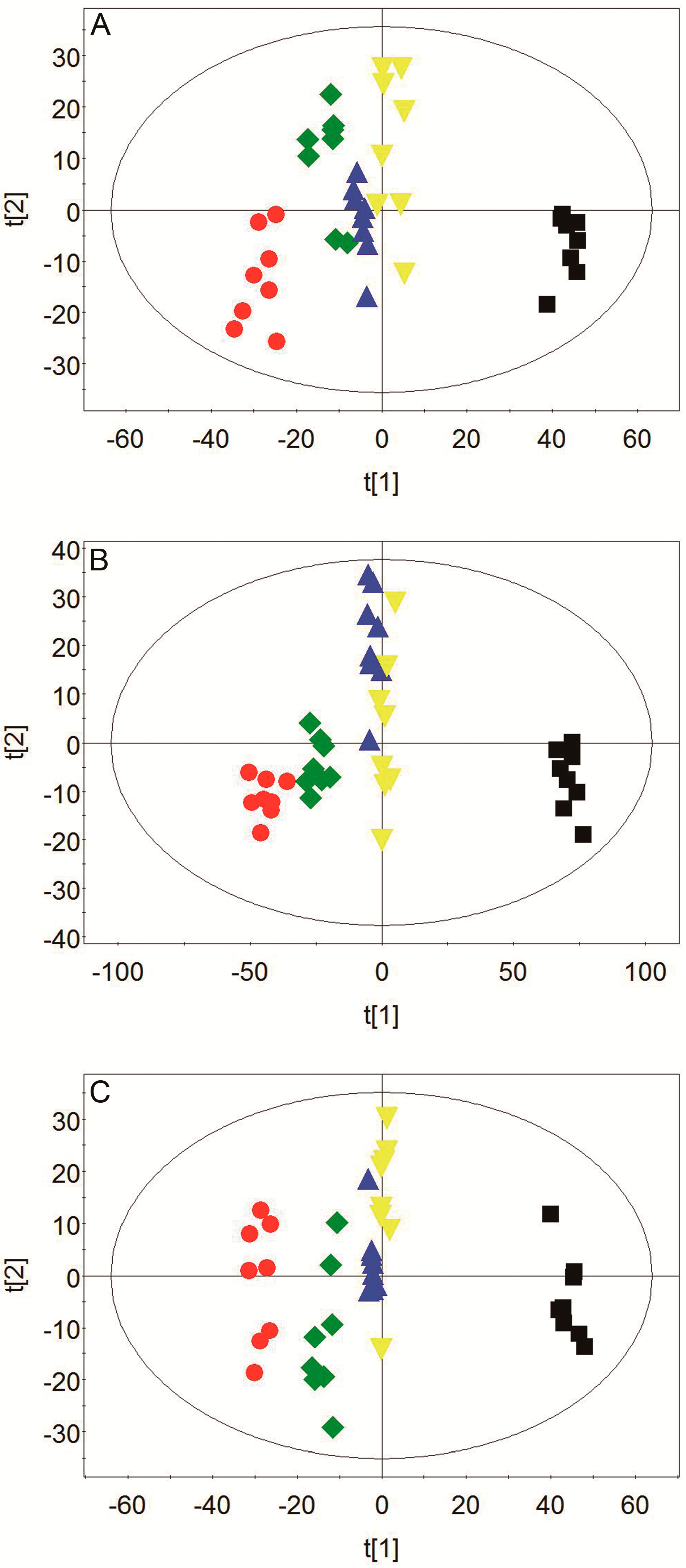
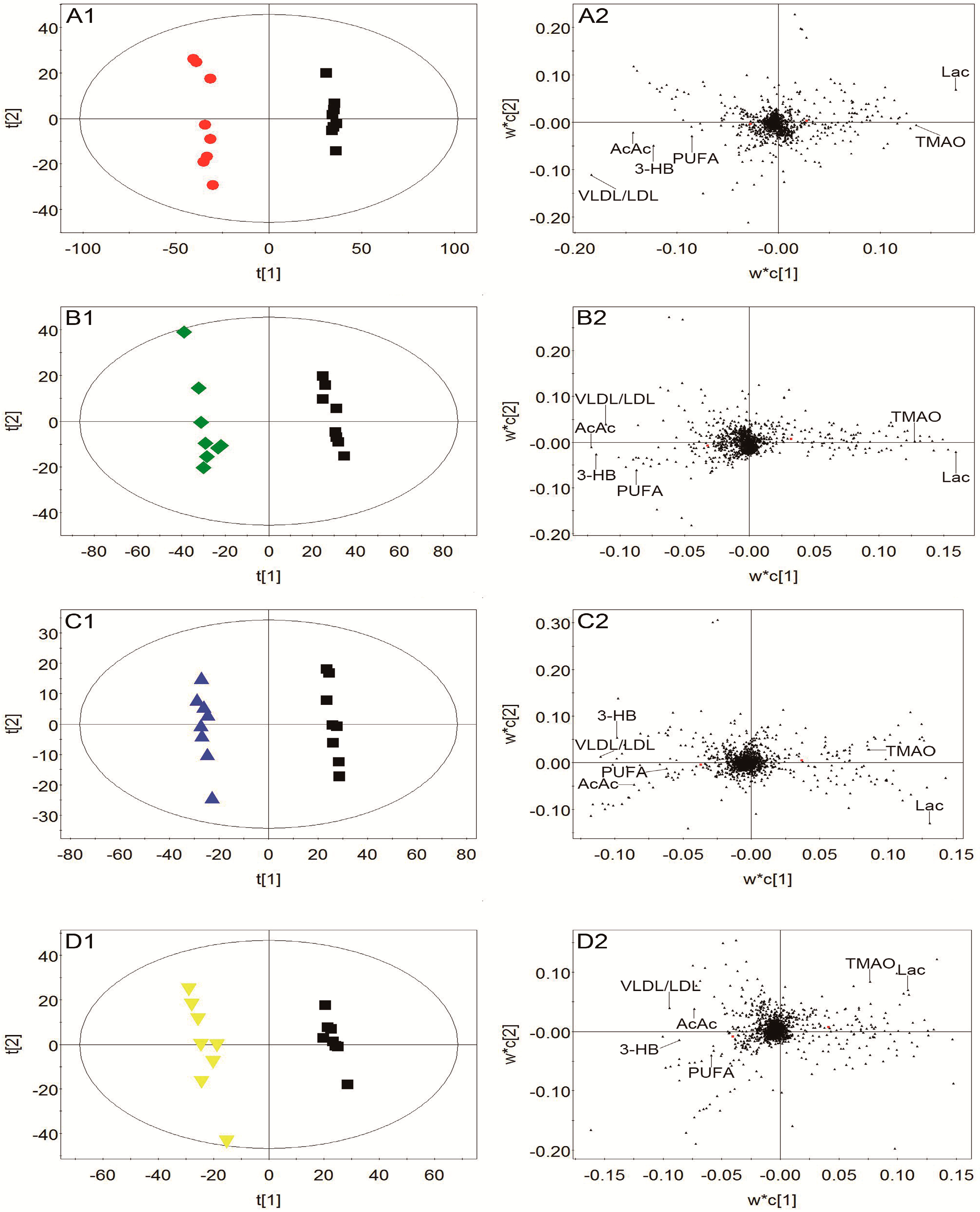
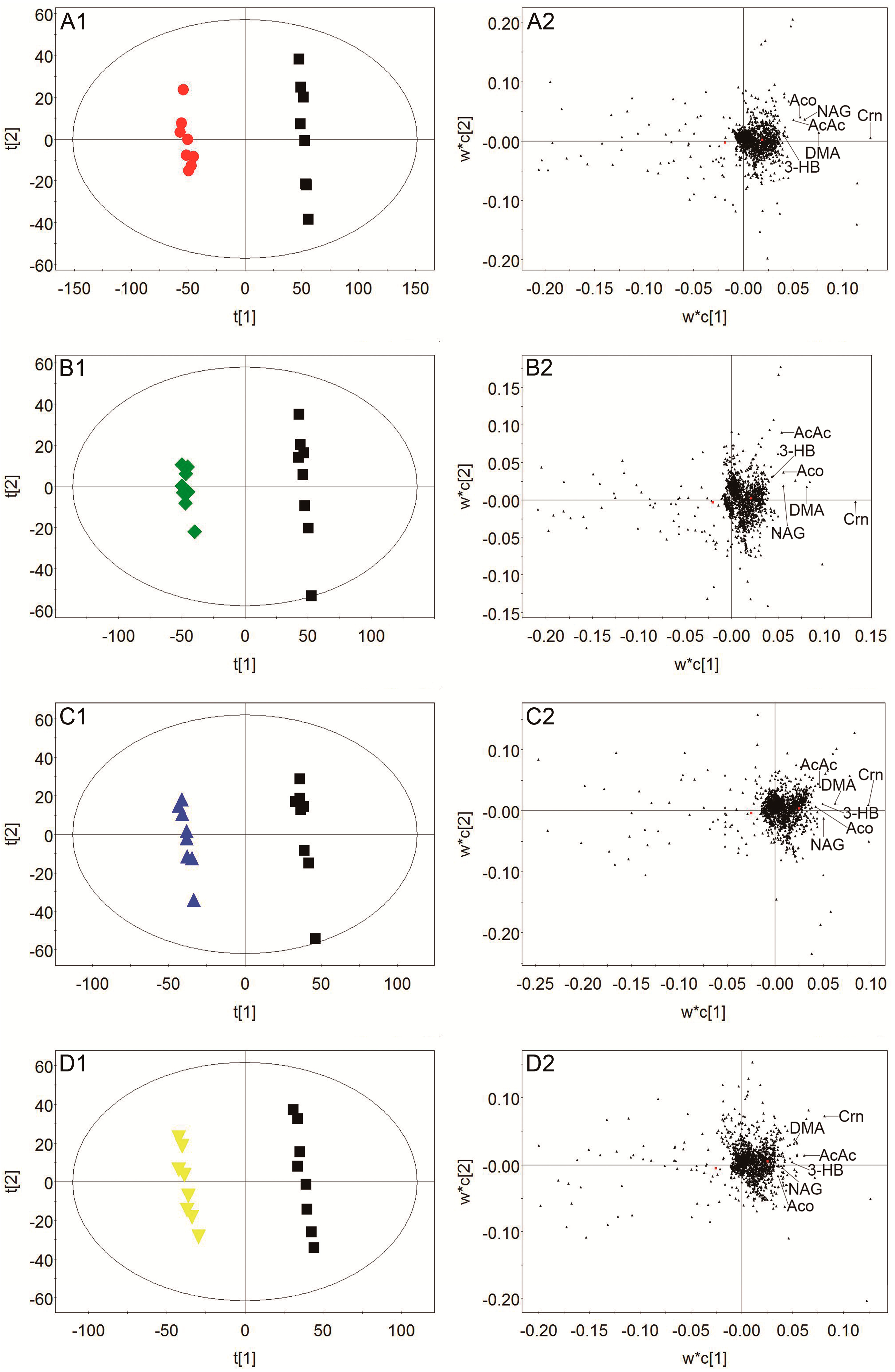
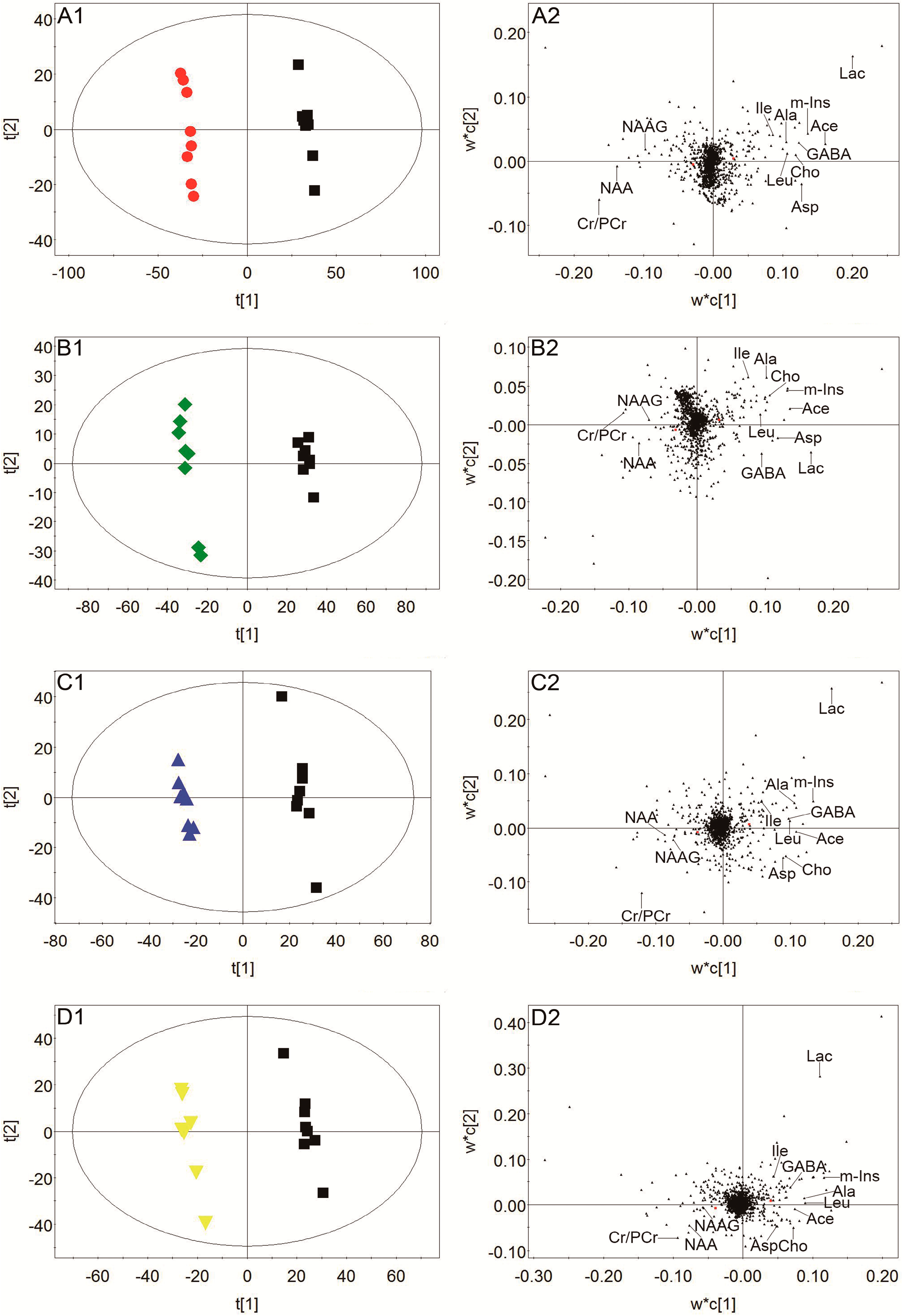
2.4. Effect of TCNDS on Metabolic Profiles of MCAO Rats by 1H-NMR-Based Metabonomics
2.5. Correlation between Biochemical Factors and Discriminatory Metabolites in Plasma.
3. Discussion
4. Materials and Methods
4.1. Chemicals and Reagents
4.2. Animal and Experiment Design
4.3. Animal Model Preparation
4.4. Neurobehavioral Dysfunction Evaluation
4.5. Plasma, Urine and Brain Tissue Collection
4.6. TTC Staining and Measurement of Cerebral Infract Area
4.7. HE Staining of Brain Tissue and Pathological Examination
4.8. Measurement of LDH, MDA and SOD Levels in Plasma
4.9. Sample Processing for NMR Measurement
4.10. Data Acquisition
4.11. Data Processing and Multivariate Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Deb, P.; Sharma, S.; Hassan, K.M. Pathophysiologic mechanisms of acute ischemic stroke: An overview with emphasis on therapeutic significance beyond thrombolysis. Pathophysiology 2010, 17, 197–218. [Google Scholar] [CrossRef]
- Xu, K.L.; Fan, F.C. Clinical observation of 100 cases on treatment of cerebral infarction with Lei’s Naodesheng tablets. Med. Recapitulate 2011, 17, 2525–2528. [Google Scholar]
- Zhang, A.L.; Chen, F.M.; Zhang, H.Y.; Ni, W. “Naodesheng” for cerebral infarction in 30 cases. Shanghai J. Tradit. Chin. Med. 2002, 36, 18–19. [Google Scholar]
- Zhang, L.; Cheng, X.R.; Chen, R.Y.; Zhu, X.M.; Du, G.H. Protective effect of effective composite of Chinese medicine prescription Naodesheng against focal cerebral ischemia in rats. Chin. J. Integr. Med. 2009, 15, 377–383. [Google Scholar] [CrossRef]
- Tian, H.; Lam, S.M.; Shui, G. Metabolomics, a powerful tool for agricultural research. Int. J. Mol. Sci. 2016, 17, 1871. [Google Scholar] [CrossRef]
- Monteiro, M.S.; Barros, A.S.; Pinto, J.; Carvalho, M.; Pires-Luís, A.S.; Henrique, R.; Jerónimo, C.; Bastos, M.L.; Gil, A.M.; Guedes de Pinho, P. Nuclear magnetic resonance metabolomics reveals an excretory metabolic signature of renal cell carcinoma. Sci. Rep. 2016, 6, 37275–37288. [Google Scholar] [CrossRef]
- Guan, Q.; Liang, S.; Wang, Z.; Yang, Y.; Wang, S. (1)H-NMR-based metabonomic analysis of the effect of optimized rhubarb aglycone on the plasma and urine metabolic fingerprints of focal cerebral ischemia-reperfusion rats. J. Ethnopharmacol. 2014, 154, 65–75. [Google Scholar] [CrossRef]
- Palisi, A.; Grimaldi, M.; Sabatini, P.; Montoro, P.; Scrima, M.; Rodriquez, M.; D’Ursi, A.M. A serum nuclear magnetic resonance-based metabolomic signature of antiphospholipid syndrome. J. Pharm. Biomed. Anal. 2017, 133, 90–95. [Google Scholar] [CrossRef]
- Vignoli, A.; Rodio, D.M.; Bellizzi, A.; Sobolev, A.P.; Anzivino, E.; Mischitelli, M.; Tenori, L.; Marini, F.; Priori, R.; Scrivo, R.; et al. NMR-based metabolomic approach to study urine samples of chronic inflammatory rheumatic disease patients. Anal. Bioanal. Chem. 2017, 409, 1405–1413. [Google Scholar] [CrossRef]
- Wang, P.R.; Wang, J.S.; Yang, M.H.; Kong, L.Y. Neuroprotective effects of Huang-Lian-Jie-Du-Decoction on ischemic stroke rats revealed by (1)H-NMR metabolomics approach. J. Pharm. Biomed. Anal. 2014, 88, 106–116. [Google Scholar] [CrossRef]
- Zielman, R.; Postma, R.; Verhoeven, A.; Bakels, F.; van Oosterhout, W.P.; Meissner, A.; van den Maagdenberg, A.M.; Terwindt, G.M.; Mayboroda, O.A.; Ferrari, M.D. Metabolomic changes in CSF of migraine patients measured with 1H-NMR spectroscopy. Mol. Biosyst. 2016, 12, 3674–3682. [Google Scholar] [CrossRef]
- Chen, C.; Li, S.X.; Wang, S.M.; Liang, S.W. Investigation into the anti-thrombosis effect and contents of total saponins and flavonoids in the bioactive fraction of Naodesheng prescription. J. Ethnopharmacol. 2012, 144, 208–212. [Google Scholar] [CrossRef]
- Luo, L.; Zhen, L.F.; Xu, Y.T.; Yang, Y.X.; Feng, S.X.; Wang, S.M.; Liang, S.W. 1HNMR-based metabonomics revealed protective effect of Naodesheng bioactive extract on ischemic stroke rats. J. Ethnopharmacol. 2016, 186, 257–269. [Google Scholar] [CrossRef]
- Huo, J.Y. Study on LC-MS determination of effective components in Naodesheng multiple combination samples. Ph.D. Thesis, Guangdong Pharmaceutical University, Guangzhou, China, 2016. [Google Scholar]
- Kang, J.Z. Study on serum chemistry of effective fraction of Naodesheng. Ph.D. Thesis, Guangdong Pharmaceutical University, Guangzhou, China, 2018. [Google Scholar]
- Wei, L.; Liao, P.Q.; Wu, H.F.; Li, X.J.; Pei, F.K.; Li, W.S.; Wu, Y.J. Metabolic profiling studies on the toxicological effects of realgar in rats by (1)H-NMR spectroscopy. Toxicol. Appl. Pharmacol. 2009, 234, 314–325. [Google Scholar] [CrossRef]
- Zou, Z.J.; Liu, Z.H.; Gong, M.J.; Han, B.; Wang, S.M.; Liang, S.W. Intervention effects of puerarin on blood stasis in rats revealed by a (1)H-NMR-based metabonomic approach. Phytomedicine 2015, 22, 333–343. [Google Scholar] [CrossRef]
- Govindaraju, V.; Young, K.; Maudsley, A.A. Proton NMR chemical shifts and coupling constants for brain metabolites. NMR Biomed. 2000, 13, 129–153. [Google Scholar] [CrossRef]
- Wang, X.J.; Zhang, A.H.; Zhou, X.H.; Liu, Q.; Nan, Y.; Guan, Y.; Kong, L.; Han, Y.; Sun, H.; Yan, G.L. An integrated chinmedomics strategy for discovery of effective constituents from traditional herbal medicine. Sci. Rep. 2016, 6, 18997. [Google Scholar] [CrossRef] [Green Version]
- Yang, S.; Ning, F.B.; Li, J.; Guo, D.M.; Zhang, L.; Cui, R.T.; Liu, Y.L. Therapeutic effect analysis of Sinomenine on rat cerebral ischemia-reperfusion injury. J. Stroke Cerebrovasc. Dis. 2016, 25, 1263–1269. [Google Scholar] [CrossRef]
- Ye, Y.J.; Li, J.; Cao, X.L.; Chen, Y.J.; Ye, C.J.; Chen, K.L. Protective effect of n-butyl alcohol extracts from Rhizoma Pinelliae Pedatisectae against cerebral ischemia-reperfusion injury in rats. J. Ethnopharmacol. 2016, 188, 259–265. [Google Scholar] [CrossRef]
- Satoh, K. Serum lipid peroxide in cerebrovascular disorders determined by a new colorimetric method. Clin. Chim. Acta 1978, 90, 37–43. [Google Scholar]
- Vani, J.R.; Mohammadi, M.T.; Foroshani, M.S.; Jafari, M. Polyhydroxylated fullerene nanoparticles attenuate brain infarction and oxidative stress in rat model of ischemic stroke. EXCLI J. 2016, 15, 378–390. [Google Scholar]
- Niizuma, K.; Yoshioka, H.; Chen, H.; Kim, G.S.; Jung, J.E.; Katsu, M.; Okami, N.; Chan, P.H. Mitochondrial and apoptotic neuronal death signaling pathways in cerebral ischemia. Biochim. Biophys. Acta 2010, 1802, 92–99. [Google Scholar] [CrossRef]
- Rodrigo, R.; Fernandez-Gajardo, R.; Gutierrez, R.; Matamala, J.M.; Carrasco, R.; Miranda -Merchak, A.; Feuerhake, W. Oxidative stress and pathophysiology of ischemic stroke: Novel therapeutic opportunities. CNS Neurol. Disord. Drug Targets 2013, 12, 698–714. [Google Scholar] [CrossRef]
- Slemmer, J.E.; Shacka, J.J.; Sweeney, M.I.; Weber, J.T. Antioxidants and free radical scavengers for the treatment of stroke, traumatic brain injury and aging. Curr. Med. Chem. 2008, 15, 404–414. [Google Scholar]
- Liu, M.; Liu, X.; Wang, H.; Xiao, H.; Jing, F.; Tang, L.; Li, D.; Zhang, Y.; Wu, H.; Yang, H. Metabolomics study on the effects of Buchang Naoxintong capsules for treating cerebral ischemia in rats using UPLC-Q/TOF-MS. J. Ethnopharmacol. 2016, 180, 1–11. [Google Scholar] [CrossRef]
- Chen, K.C.; Liao, Y.C.; Wang, J.Y.; Lin, Y.C.; Chen, C.H.; Juo, S.H. Oxidized low-density lipoprotein is a common risk factor for cardiovascular diseases and gastroenterological cancers via epigenomical regulation of microRNA-210. Oncotarget 2015, 6, 24105–24118. [Google Scholar] [CrossRef] [Green Version]
- Huang, X.P.; Ding, H.; Wang, B.; Qiu, Y.Y.; Tang, Y.H.; Zeng, R.; Deng, C.Q. Effects of the main active components combinations of Astragalus and Panax notoginseng on energy metabolism in brain tissues after cerebral ischemia-reperfusion in mice. Pharmacogn. Mag. 2015, 11, 732–739. [Google Scholar] [Green Version]
- Lensman, M.; Korzhevskii, D.E.; Mourovets, V.O.; Kostkin, V.B.; Izvarina, N.; Perasso, L.; Gandolfo, C.; Otellin, V.A.; Polenov, S.A.; Balestrino, M. Intracerebroventricular administration of creatine protects against damage by global cerebral ischemia in rat. Brain Res. 2006, 1114, 187–194. [Google Scholar] [CrossRef]
- Zhang, J.; Fang, X.; Zhou, Y.Y.; Deng, X.; Lu, Y.; Li, J.; Li, S.J.; Wang, B.; Xu, R.S. The possible damaged mechanism and the preventive effect of monosialotetrahexosylganglioside in a rat model of cerebral ischemia-reperfusion injury. J. Stroke Cerebrovasc. Dis. 2015, 24, 1471–1478. [Google Scholar] [CrossRef]
- Doyle, K.P.; Simon, R.P.; Stenzel-Poore, M.P. Mechanisms of ischemic brain damage. Neuropharmacology 2008, 55, 310–318. [Google Scholar] [CrossRef]
- Shah, A.J.; Crespi, F.; Heidbreder, C. Amino acid neurotransmitters: Separation approaches and diagnostic value. J. Chromatogr. B Anal. Technol. Biomed. Life Sci. 2002, 781, 151–163. [Google Scholar] [CrossRef]
- Berthet, C.; Xin, L.; Buscemi, L.; Benakis, C.; Gruetter, R.; Hirt, L.; Lei, H. Non-invasive diagnostic biomarkers for estimating the onset time of permanent cerebral ischemia. J. Cereb. Blood Flow Metab. 2014, 34, 1848–1855. [Google Scholar] [CrossRef] [Green Version]
- Xian, W.; Wu, Y.; Xiong, W.; Li, L.; Li, T.; Pan, S.; Song, L.; Hu, L.; Pei, L.; Yao, S.; et al. The pro-resolving lipid mediator Maresin 1 protects against cerebral ischemia/reperfusion injury by attenuating the pro-inflammatory response. Biochem. Biophys. Res. Commun. 2016, 472, 175–181. [Google Scholar] [CrossRef]
- Gupta, S.; Sharma, U.; Jagannathan, N.R.; Gupta, Y.K. Neuroprotective effect of lercanidipine in middle cerebral artery occlusion model of stroke in rats. Exp. Neurol. 2016, 288, 25–37. [Google Scholar] [CrossRef]
Sample Availability: Notoginsenoside R1, ginsenoside Rg1, ginsenoside b1, ginsenoside Rd, hydroxysafflor yellow A, senkyunolide I, puerarin, daidzein, vitexin and ferulic acid of NDS are available from the authors. |










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Neurobehavioral Score | Cerebral Infarct Area Percentage (%) |
|---|---|---|
| Control group | 0.00 ± 0.00 | 0.00 ± 0.00 |
| Model group | 3.75 ± 0.46 ### | 46.05 ± 6.09 ### |
| Nimodipine group | 1.88 ± 0.35 *** | 18.44 ± 2.68 *** |
| H-TCNDS group | 2.38 ± 0.52 ** | 23.93 ± 3.88 *** |
| L-TCNDS group | 2.75 ± 0.46 ** | 29.53 ± 5.81 ** |
| Group | LDH Level (U·L−1) | MDA Level (nmol·mL−1) | SOD Level (U·mL−1) |
|---|---|---|---|
| Control group | 9112.26 ± 1210.75 | 4.84 ± 0.71 | 144.68 ± 21.48 |
| Model group | 14,963.58 ± 2355.44 ## | 8.50 ± 1.33 ### | 78.45 ± 11.23 ### |
| Nimodipine group | 10,014.76 ± 1339.41 ** | 5.56 ± 0.89 ** | 125.90 ± 20.27 ** |
| H-TCNDS group | 10,362.75 ± 1363.21 ** | 5.88 ± 0.94 ** | 115.61 ± 17.20 ** |
| L-TCNDS group | 11,335.10 ± 1483.57 * | 6.44 ± 0.99 * | 102.38 ± 14.97 * |
| Metabolites | Chemical Shift (ppm) | VIP Score | Model Group | Nimodipine Group | H-TCNDS Group | L-TCNDS Group |
|---|---|---|---|---|---|---|
| Plasma | ||||||
| VLDL/LDL | 0.86m, 1.27m | 7.58 | ↓ ### | ↑ ** | ↑ ** | ↑ * |
| 3-HB | 4.15dt, 1.20d | 7.18 | ↓ ### | ↑ *** | ↑ ** | ↑ * |
| AcAc | 2.28s | 5.88 | ↓ ### | ↑ *** | ↑ ** | ↑ * |
| Lac | 1.33d, 4.11q | 5.58 | ↑ ### | ↓ *** | ↓ ** | ↓ * |
| TMAO/Bet | 3.27s | 5.06 | ↑ # | ↓ *** | ↓ ** | ↓ * |
| PUFA | 5.30m, 2.77m | 3.51 | ↓ ### | ↑ *** | ↑ ** | ↑ ** |
| Urine | ||||||
| Crn | 3.05s, 4.06s | 5.02 | ↑ ### | ↓ *** | ↓ ** | ↓ * |
| AcAc | 2.28s | 2.97 | ↑ ### | ↓ *** | ↓ ** | ↓ * |
| Aco | 2.23s | 2.42 | ↑ ### | ↓ *** | ↓ ** | ↓ * |
| NAG | 2.04s | 2.24 | ↑ ### | ↓ *** | ↓ ** | ↓ * |
| DMA | 2.72s | 1.64 | ↑ ### | ↓ *** | ↓ ** | ↓ * |
| 3-HB | 4.15dt, 1.20d | 1.63 | ↑ ### | ↓ ** | ↓ ** | ↓ * |
| Brain tissue | ||||||
| Lac | 1.33d, 4.11q | 8.25 | ↑ ### | ↓ *** | ↓ ** | ↓ * |
| Cr/PCr | 3.04s, 3.93s | 6.72 | ↓ ### | ↑ ** | ↑ ** | ↑ * |
| Ace | 1.92s | 6.64 | ↑ ### | ↓ *** | ↓ ** | ↓ * |
| NAA | 2.02s, 2.49dd, 4.39dd | 5.67 | ↓ ### | ↑ ** | ↑ ** | ↑ * |
| m-Ins | 3.53dd, 3.63t, 4.07t | 5.60 | ↑ ### | ↓ *** | ↓ *** | ↓ ** |
| GABA | 2.30t, 1.89m | 5.24 | ↑ ### | ↓ *** | ↓ ** | ↓ * |
| Asp | 2.81dd, 2.66dd | 5.07 | ↑ ### | ↓ *** | ↓ ** | ↓ * |
| Leu | 0.96t | 4.89 | ↑ ### | ↓ *** | ↓ *** | ↓ ** |
| Ala | 1.48d, 3.78q | 4.39 | ↑ ### | ↓ *** | ↓ *** | ↓ ** |
| Ile | 0.94t | 4.32 | ↑ ### | ↓ *** | ↓ ** | ↓ * |
| Cho | 3.21s | 4.00 | ↑ ### | ↓ *** | ↓ ** | ↓ * |
| NAAG | 2.05s | 3.52 | ↓ ### | ↑ *** | ↑ ** | ↑ * |
| Metabolites/Factors | LDH | MDA | SOD |
|---|---|---|---|
| VLDL/LDL | −0.818 | −0.851 | 0.840 |
| 3-HB | −0.816 | −0.781 | 0.851 |
| AcAc | −0.752 | −0.796 | 0.766 |
| Lac | 0.753 | 0.815 | −0.774 |
| TMAO/Bet | 0.746 | 0.744 | −0.843 |
| PUFA | −0.751 | −0.791 | 0.807 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Luo, L.; Kang, J.; He, Q.; Qi, Y.; Chen, X.; Wang, S.; Liang, S. A NMR-Based Metabonomics Approach to Determine Protective Effect of a Combination of Multiple Components Derived from Naodesheng on Ischemic Stroke Rats. Molecules 2019, 24, 1831. https://doi.org/10.3390/molecules24091831
Luo L, Kang J, He Q, Qi Y, Chen X, Wang S, Liang S. A NMR-Based Metabonomics Approach to Determine Protective Effect of a Combination of Multiple Components Derived from Naodesheng on Ischemic Stroke Rats. Molecules. 2019; 24(9):1831. https://doi.org/10.3390/molecules24091831
Chicago/Turabian StyleLuo, Lan, Jiazhen Kang, Qiong He, Yue Qi, Xingyu Chen, Shumei Wang, and Shengwang Liang. 2019. "A NMR-Based Metabonomics Approach to Determine Protective Effect of a Combination of Multiple Components Derived from Naodesheng on Ischemic Stroke Rats" Molecules 24, no. 9: 1831. https://doi.org/10.3390/molecules24091831