
Inhibition of Oral Streptococci Growth Induced by the Complementary Action of Berberine Chloride and Antibacterial Compounds




Abstract
:1. Introduction
2. Results and Discussion
2.1. Anti-Streptococcal Effect of Berberine Based on MIC/MBC Results

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reference Oral Streptococcus Strain | MIC | MICAB | MBC |
|---|---|---|---|
| Streptococcus mutans ATCC 25175 | 1024 µg/mL | 32 µg/mL | 1024 µg/mL |
| Streptococcus sanguinis ATCC 10556 | 512 µg/mL | 1 µg/mL | 1024 µg/mL |
| Streptococcus oralis ATCC 9811 | 1024 µg/mL | 8 µg/mL | 2058 µg/mL |
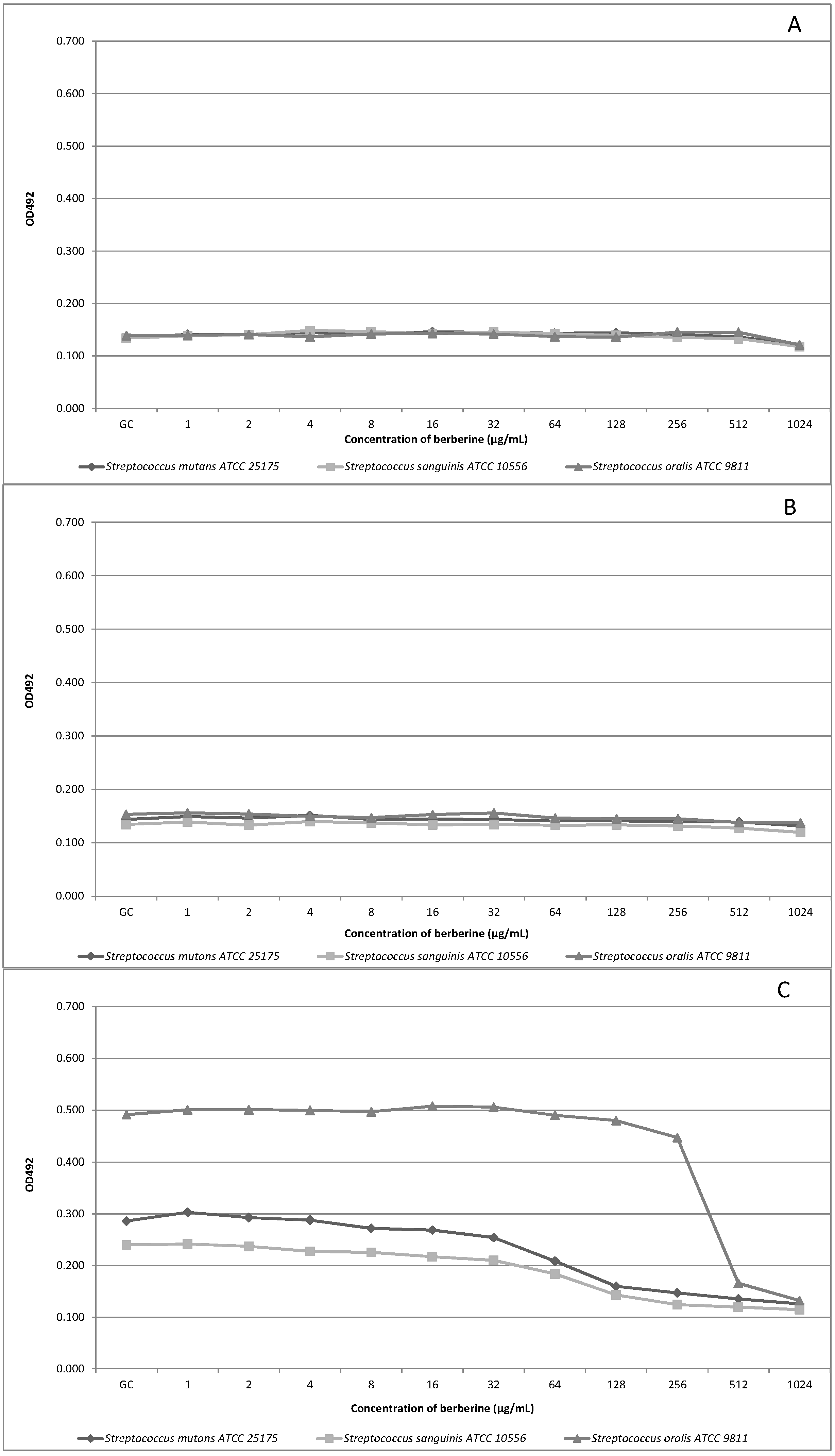
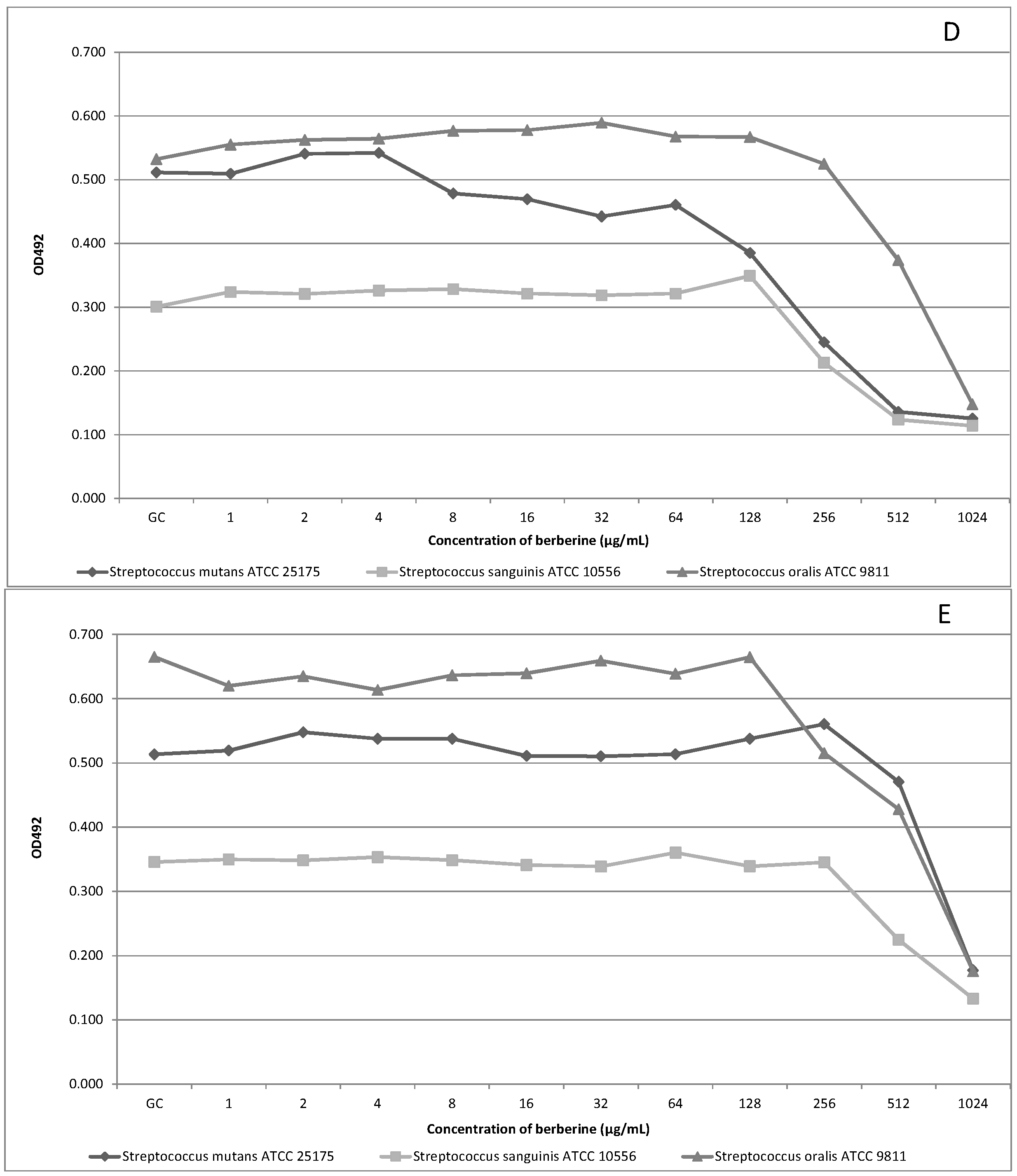
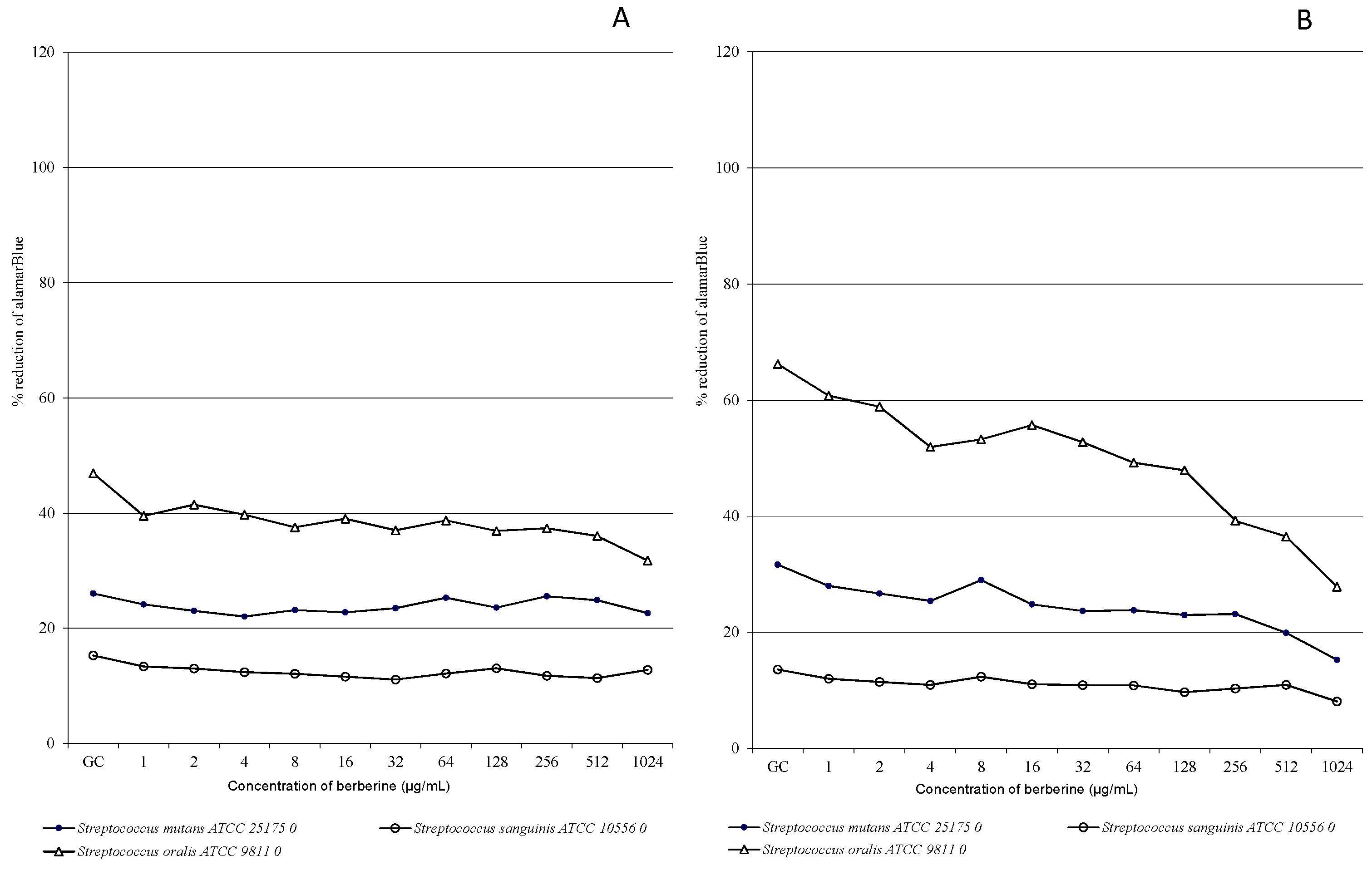
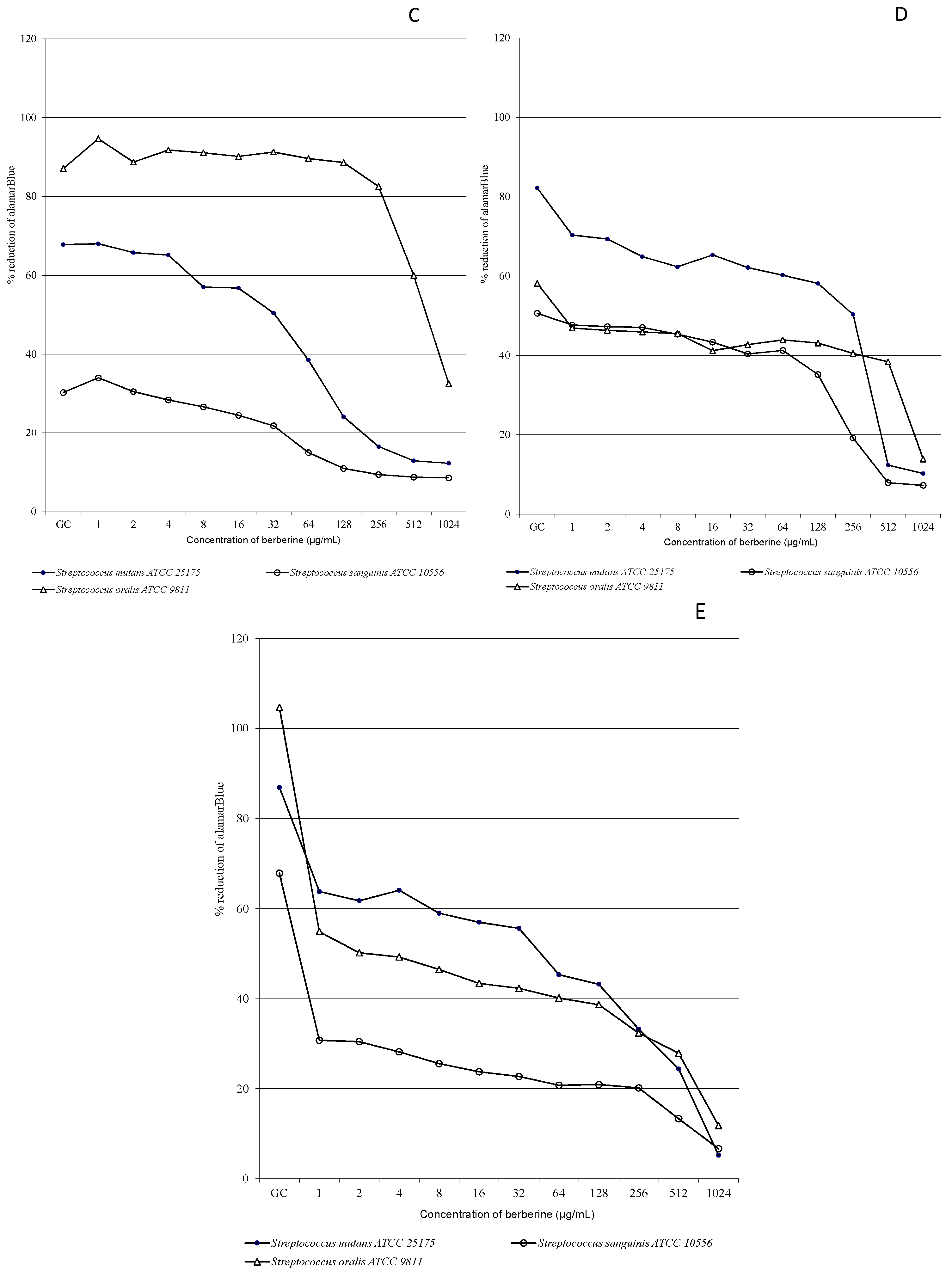
2.2. Time-Kill Kinetics of Oral Streptococci Growth Exposed to Different Concentrations of Berberine
| Variables | df | Sum of Squares | Mean Squares | F | % of Variance | p |
|---|---|---|---|---|---|---|
| strain (S) | 2 | 2.678 | 1.339 | 3328.3 | 12.32 | <0.001 |
| time (T) | 4 | 12.426 | 3.106 | 7722.5 | 57.17 | <0.001 |
| concentration (C) | 11 | 2.334 | 0.212 | 527.5 | 10.74 | <0.001 |
| SxT | 8 | 1.909 | 0.239 | 593.3 | 8.78 | <0.001 |
| SxC | 22 | 0.259 | 0.012 | 29.3 | 1.19 | <0.001 |
| TxC | 44 | 1.610 | 0.037 | 91.0 | 7.41 | <0.001 |
| SxTxC | 88 | 0.519 | 0.006 | 14.7 | 2.39 | <0.001 |
| Variables | df | Sum of Squares | Mean Squares | F | % of Variance | p |
|---|---|---|---|---|---|---|
| strain (S) | 2 | 136148 | 68074 | 2294.61 | 33.42 | <0.001 |
| time (T) | 4 | 91946 | 22986 | 774.82 | 22.57 | <0.001 |
| concentration (C) | 11 | 56632 | 5148 | 173.54 | 13.9 | <0.001 |
| SxT | 8 | 38938 | 4867 | 164.06 | 9.56 | <0.001 |
| SxC | 22 | 5743 | 261 | 8.80 | 1.41 | <0.001 |
| TxC | 44 | 46605 | 1059 | 35.70 | 11.44 | <0.001 |
| SxTxC | 88 | 31359 | 356 | 12.01 | 7.7 | <0.001 |




2.3. Effects of Interaction of Berberine Chloride and Antibacterial Agents against Oral Streptococci
| AB | Inhibition Growth Zone of Antibiotic Alone (mm) SM–SS–SO | Inhibition Growth Zone of Antibiotic + BECl (mm) SM–SS–SO | Difference in Inhibition Growth Zone (mm) SM–SS–SO |
|---|---|---|---|
| PEN | 43–39–48 | 76–61–82 | 33–22–34 |
| ERY | 41–43–43 | 56–59–61 | 15–26–18 |
| DA | 48–41–51 | 64–59–68 | 16–28–17 |
| OXA | 35–31–33 | 55–48–49 | 20–17–16 |
| CIP | 27–24–34 | 26–25–31 | (−)1–1–(−)3 |
| LIN | 36–33–36 | 54–49–59 | 18–16–23 |
| TET | 37–35–41 | 48–45–53 | 11–10–12 |
| SXT | 23–21–21 | 26–22–24 | 3–1–3 |
| mean | 36.3–33.3–38.4 | 50.6–46–53.3 | 16.5–17.1–17.5 |
| AB | Antibiotic Alone | Antibiotic + BECl | Mean Difference |
|---|---|---|---|
| PEN | 43.33 ± 4.5 SD | 73.00 ± 10.8 SD | 29.67 ± 6.6 SD |
| ERY | 42.33 ± 1.1 SD | 58.67 ± 2.5 SD | 19.67 ± 5.6 SD |
| DA | 46.65 ± 5.1 SD | 63.67 ± 4.4 SD | 20.33 ± 6.6 SD |
| OXA | 33.00 ± 2.0 SD | 50.67 ± 3.7 SD | 17.67 ± 2.0 SD |
| CIP | 28.33 ± 5.1 SD | 27.33 ± 3.2 SD | n/a |
| LIN | 35.00 ± 1.7 SD | 54.00 ± 5.0 SD | 19.00 ± 3.6 SD |
| TET | 37.67 ± 3.0 SD | 48.67 ± 4.0 SD | 11.00 ± 1.0 SD |
| SXT | 21.67 ± 1.1 SD | 24.00 ± 2.0 SD | 2.33 ± 1.1 SD |
3. Experimental Section
3.1. Oral Bacteria Strains, Media and Reagents

3.2. Microdilution Method of Determination of Minimal Inhibiting Concentration and Minimal Bactericidal Concentration for Oral Streptococci
3.3. AlamarBlue Susceptibility/Viability Colorimetric Assay
3.4. Antibacterial Susceptibility Testing; Disk Diffusion Method
3.5. Statistical Analysis
4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Kreth, J.; Merritt, J.; Qi, F. Bacterial and Host Interactions of Oral Streptococci. DNA Cell Biol. 2009, 28, 397–403. [Google Scholar] [CrossRef] [PubMed]
- Avila, M.; Ojcius, D.M.; Yilmaz, Ö. The Oral Microbiota: Living with a Permanent Guest. DNA Cell Biol. 2009, 28, 405–411. [Google Scholar] [CrossRef] [PubMed]
- Aas, J.A.; Paster, B.J.; Stokes, L.N.; Olsen, I.; Dewhirst, F.E. Defining the Normal Bacterial Flora of the Oral Cavity. J. Clin. Microbiol. 2005, 43, 5721–5732. [Google Scholar] [CrossRef] [PubMed]
- Nicolas, G.G.; Lavoie, M.C. Streptococcus mutans and oral streptococci in dentalplaque. Can. J. Microbiol. 2011, 57, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.Y.; Kuramitsu, H.K. Interactions between oral bacteria: Inhibition of Streptococcus mutans bacteriocin production by Streptococcus gordonii. Appl. Environ. Microbiol. 2005, 71, 354–362. [Google Scholar] [CrossRef] [PubMed]
- Krzyściak, W.; Jurczak, A.; Kościelniak, D.; Bystrowska, B.; Skalniak, A. The virulence of Streptococcus mutans and the ability to form biofilms. Eur. J. Clin. Microbiol. Infect. Dis. 2013, 33, 499–515. [Google Scholar] [CrossRef] [PubMed]
- Loesche, W.J. Role of Streptococcus mutans in human dental decay. Microbiol. Rev. 1986, 50, 353–380. [Google Scholar] [PubMed]
- Banas, J.A. Virulence properties of Streptococcus mutans. Front. Biosci. 2004, 19, 1267–1277. [Google Scholar] [CrossRef]
- Kreth, J.; Merritt, J.; Shi, W.; Qi, F. Competition and coexistence between Streptococcus mutans and Streptococcus sanguinis in the dental biofilm. J. Bacteriol. 2005, 187, 7193–7203. [Google Scholar] [CrossRef] [PubMed]
- Herzberg, M.C.; Gong, K.; MacFarlane, G.D.; Erickson, P.R.; Soberay, A.H.; Krebsbach, P.H.; Manjula, G.; Schilling, K.; Bowen, W.H. Phenotypic characterization of Streptococcus sanguis virulence factors associated with bacterial endocarditis. Infect. Immun. 1990, 58, 515–522. [Google Scholar] [PubMed]
- Paik, S.; Senty, L.; Das, S.; Noe, J.C.; Munro, C.L.; Kitten, T. Identification of virulence determinants for endocarditis in Streptococcus sanguinis by signature-tagged mutagenesis. Infect. Immun. 2005, 73, S6064–S6074. [Google Scholar] [CrossRef] [PubMed]
- Biswas, S.; Bowler, I.C.; Bunch, C.; Prendergast, B.; Webster, D.P. Streptococcus mutans infective endocarditis complicated by vertebral discitis following dental treatment without antibiotic prophylaxis. J. Med. Microbiol. 2010, 59, 1257–1259. [Google Scholar] [CrossRef] [PubMed]
- Caufield, P.W.; Dasanayake, A.P.; Li, Y.; Pan, Y.; Hsu, J.; Hardin, J.M. Natural history of Streptococcus sanguinis in the oral cavity of infants: Evidence for a discrete window of infectivity. Infect. Immun. 2000, 68, 4018–4023. [Google Scholar] [CrossRef] [PubMed]
- Kuramitsu, H.K.; Wang, B.Y. The whole is greater than the sum of its parts: Dental plaque bacterial interactions can affect the virulence properties of cariogenic Streptococcus mutans. Am. J. Dent. 2011, 24, 153–154. [Google Scholar] [PubMed]
- Do, T.; Jolley, K.A.; Maiden, M.C.J. Population structure of Streptococcus oralis. Microbiology 2009, 155, 2593–2602. [Google Scholar] [CrossRef] [PubMed]
- Huang, W.T.; Chang, L.Y.; Hsueh, P.R.; Lu, C.Y.; Shao, P.L.; Huang, F.Y.; Lee, P.I.; Chen, C.M.; Lee, C.Y.; Huang, L.M. Clinical features and complications of viridans streptococci bloodstream infection in pediatric hemato-oncology patients. J. Microbiol. Immunol. Infect. 2007, 40, 349–354. [Google Scholar] [PubMed]
- Doyuk, E.; Ormerod, O.J.; Bowler, I.C. Native valve endocarditis due to Streptococcus vestibularis and Streptococcus oralis. J. Infect. 2002, 45, 39–41. [Google Scholar] [CrossRef] [PubMed]
- Renton, B.J.; Clague, J.E.; Cooke, R.P. Streptococcus oralis endocarditis presenting as infective discitis in an edentulous patient. Int. J. Cardiol. 2009, 137, e13–e14. [Google Scholar] [CrossRef] [PubMed]
- Whatmore, A.M.; Efstratiou, A.; Pickerill, A.P.; Broughton, K.; Woodard, G.; Sturgeon, D.; George, R.; Dowson, C.G. Genetic relationships between clinical isolates of Streptococcus pneumoniae, Streptococcus oralis, and Streptococcus mitis: Characterization of “Atypical” pneumococci and organisms allied to S. mitis harboring S. pneumoniae virulence factor-encoding genes. Infect. Immun. 2000, 68, 1374–1382. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, H.F.; Morrison, D.; Tomlinson, D.; Gibson, B.E.; Bagg, J.; Gemmell, C.G. Gingivitis and toothbrushes: Potential roles in viridans streptococcal bacteraemia. J. Infect. 2003, 46, 67–70. [Google Scholar] [CrossRef] [PubMed]
- Maeda, K.; Nagata, H.; Kuboniwa, M.; Ojima, M.; Osaki, T.; Minamino, N.; Amano, A. Identification and Characterization of Porphyromonas gingivalis Client Proteins That Bind to Streptococcus oralis Glyceraldehyde-3-Phosphate Dehydrogenase. Infect. Immun. 2013, 81, 753–763. [Google Scholar] [CrossRef] [PubMed]
- Montejo, M.; Aguirrebeugere, K. Streptococcus oralis meningitis after dental manipulation. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 1998, 85, 126–127. [Google Scholar] [CrossRef]
- Wilson, W.; Taubert, K.A.; Gewitz, M.; Lockhart, P.B.; Baddour, L.M.; Levison, M.; Bolger, A.; Cabell, C.H.; Takahashi, M.; Baltimore, R.S.; et al. Prevention of infective endocarditis: Guidelines from the American Heart Association: A guideline from the American Heart Association Rheumatic Fever, Endocarditis and Kawasaki Disease Committee, Council on Cardiovascular Disease in the Young, and the Council on Clinical Cardiology, Council on Cardiovascular Surgery and Anesthesia, and the Quality of Care and Outcomes Research Interdisciplinary Working Group. Circultion 2007, 116, 1736–1754. [Google Scholar]
- Centre for Clinical Practice. Prophylaxis against Infective Endocarditis. Antimicrobial Prophylaxis against Infective Endocarditis in Adults and Children Undergoing Interventional Procedures; NICE clinical guideline; National Institute for Health and Clinical Excellence: London, UK, 2008. [Google Scholar]
- Vuddanda, P.R.; Chakraborty, S.; Singh, S. Berberine: A potential phytochemical with multispectrum therapeutic activities. Expert Opin. Investig. Drugs 2010, 19, 1297–1307. [Google Scholar] [CrossRef] [PubMed]
- Cernáková, M.; Kostálová, D. Antimicrobial activity of berberine—A constituent of Mahonia aquifolium. Folia Microbiol. 2002, 47, 375–378. [Google Scholar] [CrossRef]
- Freilea, M.L.; Giannini, F.; Pucci, G.; Sturniolo, A.; Rodero, L.; Pucci, O.; Balzareti, V.; Enriz, R.D. Antimicrobial activity of aqueous extracts and of berberine isolated from Berberis. Heterophylla Fitoter. 2003, 74, 602–705. [Google Scholar] [CrossRef]
- Cowan, M.M. Plant products as antimicrobial agents. Clin. Microbiol. Rev. 1999, 12, 564–582. [Google Scholar] [PubMed]
- Park, K.S.; Kang, K.C.; Kim, J.H.; Adams, D.J.; Johng, T.N.; Paik, Y.K. Differential inhibitory effects of protoberberines on sterol and chitin biosyntheses in Candida albicans. J. Antimicrob. Chemother. 1999, 43, 667–674. [Google Scholar] [CrossRef] [PubMed]
- Birdsall, T.C.; Kelly, G.S. Berberine: Therapeutic potential of an alkaloid found in several medicinal plants. Altern. Med. Rev. 1997, 2, 94–103. [Google Scholar]
- Hu, J.P.; Takahashi, N.; Yamada, T. Coptidis rhizoma inhibits growth and proteases of oral bacteria. Oral Dis. 2000, 6, 297–302. [Google Scholar] [CrossRef] [PubMed]
- Rohrer, U.; Kunz, E.M.; Lenkeit, K.; Schaffner, W.; Meyer, J. Antimicrobial activity of Mahonia aquifolium and two of its alkaloids against oral bacteria. Schweiz. Mon. Zahnmed. 2007, 117, 1126–1131. [Google Scholar]
- Hwang, B.Y.; Roberts, S.K.; Chadwick, L.R.; Wu, C.D.; Kinghorn, A.D. Antimicrobial constituents from goldenseal (the Rhizomes of Hydrastis canadensis) against selected oral pathogens. Planta Med. 2003, 69, 623–637. [Google Scholar] [PubMed]
- Mogi, A.; Nishi, J.I.; Yoshinaga, M.; Harada, H.; Narahara, S.; Kawakami, K.; Maruyama, I. Increased prevalence of penicillin-resistant viridans group streptococci in Japanese children with upper respiratory infection treated by beta-lactam agents and in those with oncohematologic diseases. Pediatr. Infect. Dis. J. 1997, 16, 1140–1144. [Google Scholar] [CrossRef] [PubMed]
- Doern, G.V.; Ferraro, M.J.; Brueggemann, A.B.; Ruoff, K.L. Emergence of high rates of antimicrobial resistance among viridans group streptococci in the United States. Antimicrob. Agents Chemother. 1996, 40, 891–894. [Google Scholar] [PubMed]
- Dziedzic, A.; Kubina, R.; Wojtyczka, R.D.; Kabała-Dzik, A.; Tanasiewicz, M.; Morawiec, T. The antibacterial effect of ethanol extract of polish propolis on mutans streptococci and lactobacilli isolated from saliva. Evid. Based Complement. Altern. Med. 2013, 2013. [Google Scholar] [CrossRef] [PubMed]
- Zuo, G.Y.; Li, Y.; Han, J.; Wang, G.C.; Zhang, Y.L.; Bian, Z.Q. Antibacterial and synergy of berberines with antibacterial agents against clinical multi-drug resistant isolates of Methicillin-Resistant Staphylococcus aureus (MRSA). Molecules 2012, 17, 10322–10330. [Google Scholar] [CrossRef] [PubMed]
- Yu, H.H.; Kim, K.J.; Cha, J.D.; Kim, H.K.; Lee, Y.E.; Choi, N.Y.; You, Y.O. Antimicrobial activity of berberine alone and in combination with ampicillin or oxacillin against methicillin-resistant Staphylococcus aureus. J. Med. Food 2005, 8, 454–461. [Google Scholar] [CrossRef] [PubMed]
- Wojtyczka, R.D.; Dziedzic, A.; Kępa, M.; Kubina, R.; Kabała-Dzik, A.; Mularz, T.; Idzik, D. Berberine Enhances the Antibacterial Activity of Selected Antibiotics against Coagulase-Negative Staphylococcus Strains in Vitro. Molecules 2014, 19, 6583–6596. [Google Scholar] [CrossRef] [PubMed]
- Kinghorn, D.; Roberts, S.K.; Wu, C.D. Composition containing berberine or a derivative thereof and an antimicrobial agent or an antibiotic agent, and their use for treating oral pathogens and other disorders. Patent WO 2004093876 A2, 13 October 2005. Available online: http://www.google.com/patents/WO2004093876A2?cl=en (accessed on 27 July 2015). [Google Scholar]
- Koh, J.; Wilson, M.; Vidic, J.; Newman, H.N. Amoxycillin-resistant streptococci in dental plaque. Microbios 1986, 45, 41–53. [Google Scholar] [PubMed]
- Hall, G.E.; Baddour, L.M. Apparent failure of endocarditis prophylaxis caused by penicillin-resistant Streptococcus mitis. Am. J. Med. Sci. 2002, 324, 51–53. [Google Scholar] [CrossRef] [PubMed]
- Masuda, K.; Nemoto, H.; Nakano, K.; Naka, S.; Nomura, R.; Ooshima, T. Amoxicillin-resistant oral streptococci identified in dental plaque specimens from healthy Japanese adults. J. Cardiol. 2012, 59, 285–290. [Google Scholar] [CrossRef] [PubMed]
- Nemoto, H.; Nomura, R.; Ooshima, T.; Nakano, K. Distribution of amoxicillin-resistant oral streptococci in dental plaque specimens obtained from Japanese children and adolescents at risk for infective endocarditis. J. Cardiol. 2013, 62, 296–300. [Google Scholar] [CrossRef] [PubMed]
- Palombo, E.A. Traditional Medicinal Plant Extracts and Natural Products with Activity against Oral Bacteria: Potential Application in the Prevention and Treatment of Oral Diseases. Evid. Based Complement. Altern. Med. 2011, 2011. [Google Scholar] [CrossRef] [PubMed]
- Wong, R.W.; Hägg, U.; Samaranayake, L.; Yuen, M.K.; Seneviratne, C.J.; Kao, R. Antimicrobial activity of Chinese medicine herbs against common bacteria in oral biofilm. A pilot study. Int. J. Oral Maxillofac. Surg. 2010, 39, 599–605. [Google Scholar] [CrossRef] [PubMed]
- Xie, Q.; Johnson, B.R.; Wenckus, C.S.; Fayad, M.I.; Wu, C.D. Efficacy of berberine, an antimicrobial plant alkaloid, as an endodontic irrigant against a mixed-culture biofilm in an in vitro tooth model. J. Endod. 2012, 38, 1114–1117. [Google Scholar] [CrossRef] [PubMed]
- Scazzocchio, F.; Cometa, M.F.; Tomassini, L.; Palmery, M. Antibacterial activity of Hydrastis canadensis extract and its major isolated alkaloids. Planta Med. 2001, 67, 561–564. [Google Scholar] [CrossRef] [PubMed]
- Ettefagh, K.A.; Burns, J.T.; Junio, H.A.; Kattz, G.W.; Cech, N.B. Goldenseal (Hydrastis canadensis L.) extracts synergistically enhance the antibacterial activity of berberine via efflux pump inhibition. Planta Med. 2011, 77, 835–840. [Google Scholar] [PubMed]
- Stermitz, F.R.; Lorenz, P.; Tawara, J.N.; Zenewicz, L.A.; Lewis, K. Synergy in a medicinal plant: Antimicrobial action of berberine potentiated by 5′′-methoxyhydnocarpin, a multidrug pump inhibitor. Proc. Natl. Acad. Sci. USA 2000, 97, 1433–1437. [Google Scholar] [CrossRef] [PubMed]
- Jin, J.L.; Hua, G.G.; Meng, Z.; Gao, P.J. Antibacterial mechanisms of berberine and reasons for little resistance of bacteria. Chin. Herb. Med. 2010, 3, 27–35. [Google Scholar]
- Sun, N.; Chan, F.Y.; Lu, Y.J.; Neves, M.A.C.; Lui, H.K.; Wang, Y.; Chow, K.Y.; Chan, K.F.; Yan, S.C.; Leung, Y.C.; et al. Rational Design of Berberine-Based FtsZ Inhibitors with Broad-Spectrum Antibacterial Activity. PLoS ONE 2014, 9, e97514. [Google Scholar] [CrossRef] [PubMed]
- Amsterdam, D. Susceptibility Testing of Antimicrobials in Liquid Media. In Antibiotics in Laboratory Medicine, 5th ed.; Loman, V., Ed.; Williams and Wilkins: Philadelphia, PA, USA, 2005; pp. 61–143. [Google Scholar]
- European Committee for Antimicrobial Susceptibility Testing (EUCAST) of the European Society of Clinical Microbiology and Infectious Diseases (ESCMID). Determination of minimum inhibitory concentrations (MICs) of antibacterial agents by broth dilution. Clin. Microbiol. Infect. 2003, 9, 1–7.
- Devienne, K.F.; Raddi, M.S.G. Screening for antimicrobial activity of natural Products using a microplate photometer. Braz. J. Microbiol. 2002, 33, 166–168. [Google Scholar] [CrossRef]
- European Committee for Antimicrobial Susceptibility Testing (EUCAST) of the European Society of Clinical Microbiology and Infectious Diseases (ESCMID). Terminology relating to methods for the determination of susceptibility of bacteria to antimicrobial agents. EUCAST definitive document E. Def. 1.2. Clin. Microbiol. Infect. 2000, 6, 503–508.
- Bär, W.; Bäde-Schumann, U.; Krebs, A.; Cromme, L. Rapid method for detection of minimal bactericidal concentration of antibiotics. J. Microbiol. Methods 2009, 77, 85–89. [Google Scholar] [CrossRef] [PubMed]
- Pettit, R.K.; Weber, C.A.; Kean, M.J.; Hoffmann, H.; Pettit, G.R.; Tan, R.; Franks, K.S.; Horton, M.L. Microplate Alamar Blue Assay for Staphylococcus epidermidis Biofilm Susceptibility Testing. Antimicrob. Agents Chemother. 2005, 49, 2612–2617. [Google Scholar] [CrossRef] [PubMed]
- Fernandes Junior, A.; Balestrin, E.C.; Betoni, J.E.C.; Orsi, R.O.; da Cunha, M.R.S.; Montelli, A.C. Propolis: Anti-Staphylococcus aureus activity and synergism with antimicrobial drugs. Mem. Inst. Oswaldo Cruz 2005, 100, 563–566. [Google Scholar] [CrossRef] [PubMed]
- Mahon, C.R.; Manuselis, J.R.G. Textbook of Diagnostic Microbiology; WB Saunders: Philadelphia, PA, USA, 1995; p. 1134. [Google Scholar]
- Sample Availability: Samples of the berbrine chloride and refefence ATCC strains are available from the authors.
© 2015 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dziedzic, A.; Wojtyczka, R.D.; Kubina, R. Inhibition of Oral Streptococci Growth Induced by the Complementary Action of Berberine Chloride and Antibacterial Compounds. Molecules 2015, 20, 13705-13724. https://doi.org/10.3390/molecules200813705
Dziedzic A, Wojtyczka RD, Kubina R. Inhibition of Oral Streptococci Growth Induced by the Complementary Action of Berberine Chloride and Antibacterial Compounds. Molecules. 2015; 20(8):13705-13724. https://doi.org/10.3390/molecules200813705
Chicago/Turabian StyleDziedzic, Arkadiusz, Robert D. Wojtyczka, and Robert Kubina. 2015. "Inhibition of Oral Streptococci Growth Induced by the Complementary Action of Berberine Chloride and Antibacterial Compounds" Molecules 20, no. 8: 13705-13724. https://doi.org/10.3390/molecules200813705