



J. Clin. Med. 2024, 13(2), 343; https://doi.org/10.3390/jcm13020343 - 07 Jan 2024
Viewed by 915
Abstract
►
Show Figures
Background: Medication use during acute illness increases the risk of experiencing drug related problems (DRPs), including acute kidney injuries. It is recommended that potentially nephrotoxic medications are withheld during acute illness, including sulfonylureas, angiotensin converting enzyme inhibitors, diuretics, metformin, angiotensin receptor blockers, non-steroidal
[...] Read more.
Background: Medication use during acute illness increases the risk of experiencing drug related problems (DRPs), including acute kidney injuries. It is recommended that potentially nephrotoxic medications are withheld during acute illness, including sulfonylureas, angiotensin converting enzyme inhibitors, diuretics, metformin, angiotensin receptor blockers, non-steroidal anti-inflammatories and sodium glucose co-transporter 2 inhibitors (SADMANS). It is unknown if Australian pharmacists currently provide sick day medication management advice regarding SADMANS medications. Hence, we aimed to identify current DRPs and the recommendations made during residential medication management reviews (RMMRs), especially with SADMANS medications. Methods: A retrospective review of 408 RMMRs was conducted. DRPs and pharmacist recommendations were classified according to a modified DOCUMENT system. General practitioners’ (GP) recommendations were also categorised. Results: Over 97% of residents experienced at least one DRP. Common problems for non-SADMANS medications were “toxicity or adverse drug reaction”, “drug selection” and “over/underdosing” and those for SADMANS medications included “toxicity or adverse drug reaction”, “monitoring” and “drug selection”. GPs agreed with pharmacist recommendations approximately 40% of the time. No pharmacists provided sick day medication management advice for SADMANS medications. Conclusion: DRPs remain highly prevalent in aged care facilities. Medication reviews effectively identify and resolve DRPs approximately 40% of the time, but do not currently minimise the risk associated with using SADMANS medications during sick days, which is a potential area of improvement.
Full article
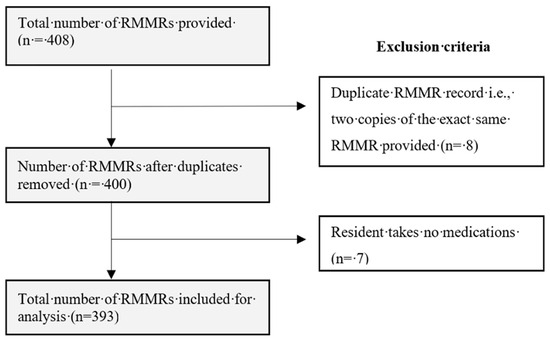
Figure 1


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}