



Geriatrics 2023, 8(5), 92; https://doi.org/10.3390/geriatrics8050092 - 15 Sep 2023
Cited by 2 | Viewed by 1246
Abstract
►
Show Figures
Good musculoskeletal quality dramatically influences the outcome of an arthroplasty operation in geriatric patients, as well as is a key element for optimal osseointegration. In this context, metallosis is a complication associated with the type of prosthesis used, as implants with a chromium–cobalt
[...] Read more.
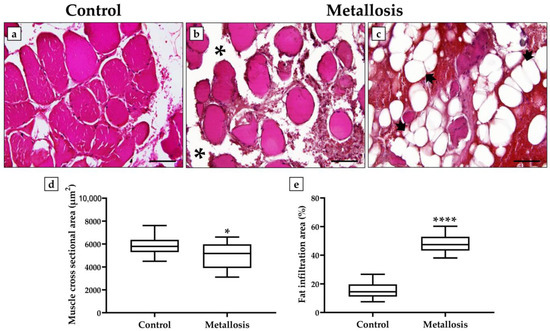
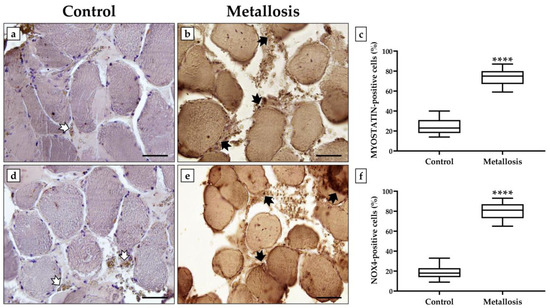
Good musculoskeletal quality dramatically influences the outcome of an arthroplasty operation in geriatric patients, as well as is a key element for optimal osseointegration. In this context, metallosis is a complication associated with the type of prosthesis used, as implants with a chromium–cobalt interface are known to alter the bone microarchitecture and reduce the ratio of muscle to fat, resulting in lipid accumulation. Therefore, the aim of our study was to investigate possible muscle changes by histological, morphometric, and immunohistochemical analyses in a patient undergoing hip replacement revision with elevated blood and urinary concentrations of chromium and cobalt. Interestingly, the muscle tissue showed significant structural changes and a massive infiltration of adipose tissue between muscle fibers in association with an altered expression pattern of important biomarkers of musculoskeletal health and oxidative stress, such as myostatin and NADPH Oxidase 4. Overall, our results confirm the very serious impact of metallosis on musculoskeletal health, suggesting the need for further studies to adopt a diagnostic approach to identify the cause of metallosis early and eliminate it as part of the prosthesis revision surgery.
Full article
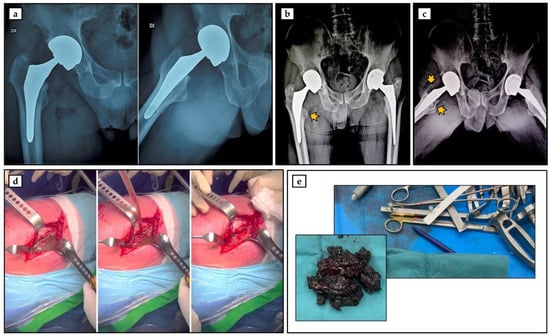
Figure 1
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}