




Cancers 2024, 16(1), 64; https://doi.org/10.3390/cancers16010064 - 21 Dec 2023
Viewed by 683
Abstract
►
Show Figures
For high-grade glioma (HGG) patients with old age or poor performance status, hypofractionated radiotherapy (hypoRT) in 10–15 fractions is recommended. Also, limited data exist on the impact of salvage treatment after progression in frail patients. We retrospectively analyzed the outcomes of dose-escalated hypoRT
[...] Read more.
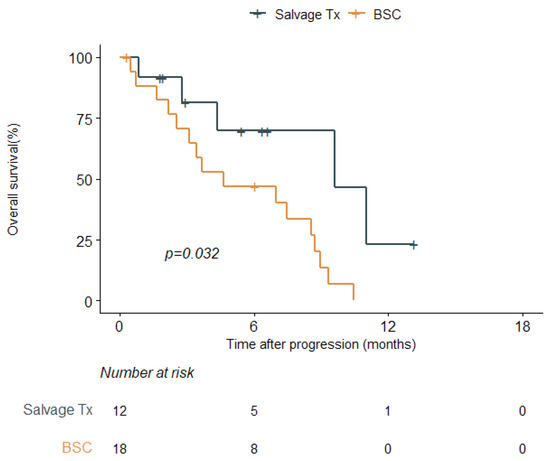
For high-grade glioma (HGG) patients with old age or poor performance status, hypofractionated radiotherapy (hypoRT) in 10–15 fractions is recommended. Also, limited data exist on the impact of salvage treatment after progression in frail patients. We retrospectively analyzed the outcomes of dose-escalated hypoRT in 40 frail HGG patients who were treated with hypoRT between 2013 and 2021. With a median biologically effective dose of 71.7 Gy, a total dose of 56 Gy in 20 fractions was the most frequently used regimen (53.7%). The median age and Karnofsky Performance Status of patients were 74 years and 70, respectively. Most patients (n = 31, 77.5%) were diagnosed with glioblastoma, IDH-wildtype, CNS WHO grade 4. Only 10 (25.0%) patients underwent surgical resection, and 28 (70.0%) patients received concurrent temozolomide during hypoRT. With a median follow-up of 9.7 months, the median overall survival (OS) was 12.2 months. Of the 30 (75.0%) patients with disease progression, only 12 patients received salvage treatment. The OS after progression differed significantly depending on salvage treatment (median OS, 9.6 vs. 4.6 months, p = 0.032). Dose-escalated hypoRT in 20 fractions produced survival outcomes outperforming historical data for frail patients.
Full article
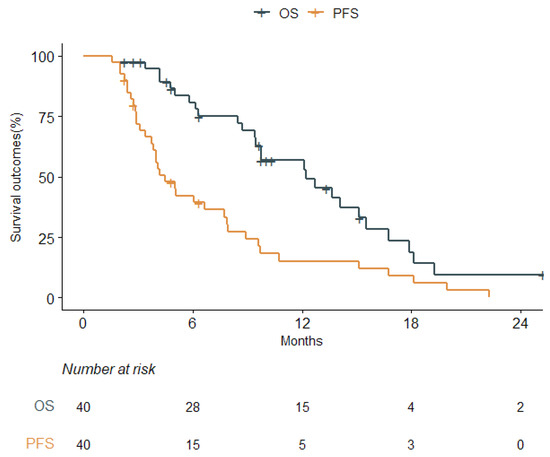
Figure 1





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}