



Cancers 2024, 16(8), 1498; https://doi.org/10.3390/cancers16081498 - 14 Apr 2024
Viewed by 245
Abstract
►
Show Figures
The aim of this study was to retrospectively evaluate the effects of conventional transarterial chemoembolization (cTACE) for the treatment of hepatocellular carcinoma over 20 years regarding overall survival (OS) and prognostic factors for OS. During the period from 1996 to 2016, 836 patients
[...] Read more.
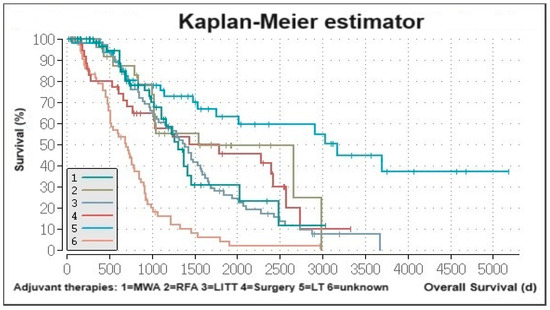
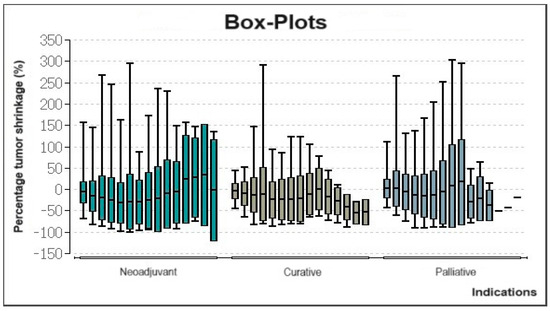
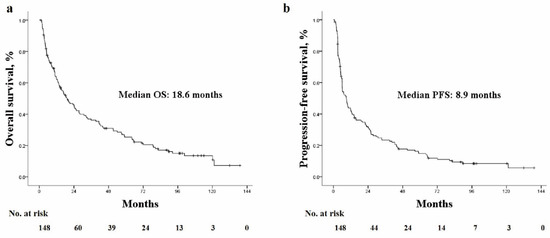
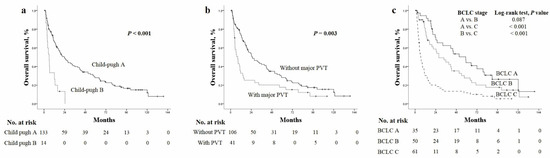
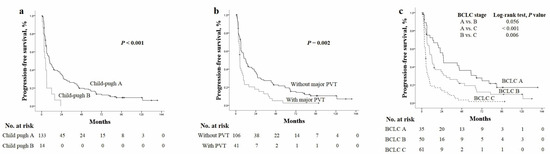
The aim of this study was to retrospectively evaluate the effects of conventional transarterial chemoembolization (cTACE) for the treatment of hepatocellular carcinoma over 20 years regarding overall survival (OS) and prognostic factors for OS. During the period from 1996 to 2016, 836 patients with HCC were treated with cTACE. Data evaluation was performed on the basis of pre- and postinterventional MRI and CT scans. Survival analysis was performed by Kaplan–Meier estimator; prognostic factors were determined by the use of Cox regression analysis. Overall, 4084 (mean 4.89 TACE sessions/patient) procedures were assessed. Median OS was 700 days (99% CI, 632.8–767.2). Depending on the indication, patients treated with a neoadjuvant intention showed the best OS (1229 days, 99% CI 983.8–1474.2) followed by curative intention (787 days, 99% CI 696.3–877.7), and then palliative intention (360 days, 99% CI 328.4–391.6). Portal vein thrombosis (HR 2.19, CI 1.63–2.96, and p < 0.01) and Child–Pugh class B or worse (HR 1.44, CI 1.11–1.86, and p < 0.001) were significantly associated with shorter OS. Patients with HCC benefit from TACE after careful patient selection. Portal vein thrombosis and Child–Pugh class B or worse are significantly unfavorable prognostic factors for patients’ survival.
Full article
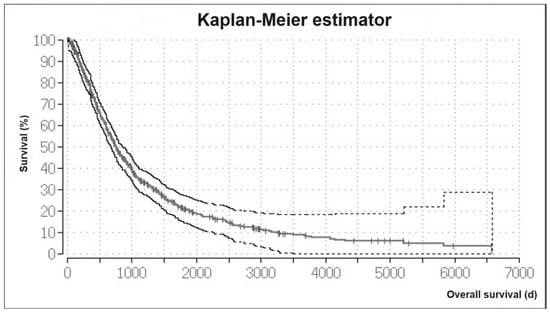
Figure 1



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}