



Cancers 2024, 16(4), 835; https://doi.org/10.3390/cancers16040835 - 19 Feb 2024
Viewed by 617
Abstract
Introduction: Image-guided renal mass biopsy is gaining increased diagnostic acceptance, but there are limited data concerning the safety and diagnostic yield of biopsy for small renal masses (≤4 cm). This study evaluated the safety, diagnostic yield, and management after image-guided percutaneous biopsy for
[...] Read more.
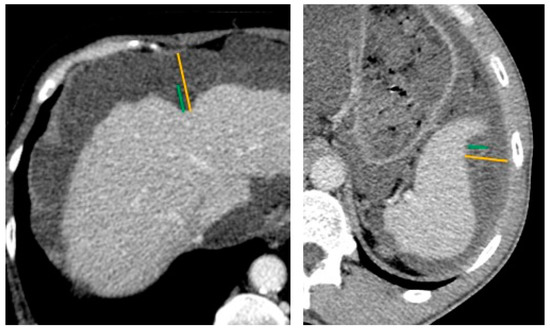
Introduction: Image-guided renal mass biopsy is gaining increased diagnostic acceptance, but there are limited data concerning the safety and diagnostic yield of biopsy for small renal masses (≤4 cm). This study evaluated the safety, diagnostic yield, and management after image-guided percutaneous biopsy for small renal masses. Methods: A retrospective IRB-approved study was conducted on patients who underwent renal mass biopsy for histopathologic diagnosis at a single center from 2015 to 2021. Patients with a prior history of malignancy or a renal mass >4 cm were excluded. Descriptive statistics were used to summarize patient demographics, tumor size, the imaging modality used for biopsy, procedure details, complications, pathological diagnosis, and post-biopsy management. A biopsy was considered successful when the specimen was sufficient for diagnosis without need for a repeat biopsy. Complications were graded according to the SIR classification of adverse events. A chi-squared test (significance level set at p ≤ 0.05) was used to compare the success rate of biopsies in different lesion size groups. Results: A total of 167 patients met the inclusion criteria. The median age was 65 years (range: 26–87) and 51% were male. The median renal mass size was 2.6 cm (range: one–four). Ultrasound was solely employed in 60% of procedures, CT in 33%, a combination of US/CT in 6%, and MRI in one case. With on-site cytopathology, the median number of specimens obtained per procedure was four (range: one–nine). The overall complication rate was 5%. Grade A complications were seen in 4% (n = 7), consisting of perinephric hematoma (n = 6) and retroperitoneal hematoma (n = 1). There was one grade B complication (0.5%; pain) and one grade D complication (0.5%; pyelonephritis). There was no patient mortality within 30 days post-biopsy. Biopsy was successful in 88% of cases. A sub-group analysis showed a success rate of 85% in tumors <3 cm and 93% in tumors ≥3 cm (p = 0.01). Pathological diagnoses included renal cell carcinoma (65%), oncocytoma (18%), clear cell papillary renal cell tumors (9%), angiomyolipoma (4%), xanthogranulomatous pyelonephritis (1%), lymphoma (1%), high-grade papillary urothelial carcinoma (1%), and metanephric adenoma (1%), revealing benign diagnosis in 30% of cases. The most common treatment was surgery (40%), followed by percutaneous cryoablation (22%). In total, 37% of patients were managed conservatively, and one patient received chemotherapy. Conclusion: This study demonstrates the safety and diagnostic efficacy of image-guided biopsy of small renal masses. The diagnostic yield was significantly higher for masses 3–4 cm in size compared to those <3 cm. The biopsy results showed a high percentage of benign diagnoses and informed treatment decisions in most patients.
Full article

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}