



Cancers 2023, 15(13), 3343; https://doi.org/10.3390/cancers15133343 - 25 Jun 2023
Viewed by 1368
Abstract
►
Show Figures
PURPOSE: Hepatocellular carcinoma (HCC) is one of the most severe complications in chronic hepatitis B virus (HBV) infection. HCC can still develop in patients with chronic HBV (CHB) infection undergoing antiviral therapy. Several effective scoring systems for the prediction of HCC risk in
[...] Read more.
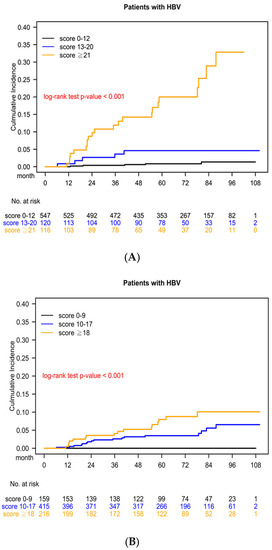
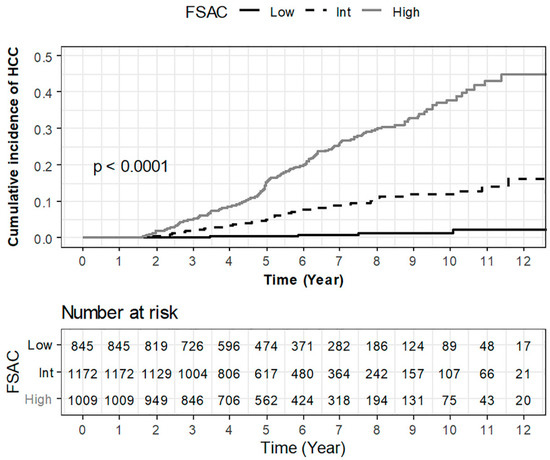
PURPOSE: Hepatocellular carcinoma (HCC) is one of the most severe complications in chronic hepatitis B virus (HBV) infection. HCC can still develop in patients with chronic HBV (CHB) infection undergoing antiviral therapy. Several effective scoring systems for the prediction of HCC risk in CHB patients have been established. However, very few of them are designed for CHB patients receiving nucleos(t)ide analogues (NAs) therapy. Furthermore, none are available for HCC risk prediction in CHB patients receiving finite periods of antiviral therapy. METHODS: This study enrolled 790 consecutive treatment-naïve patients with CHB infection who had visited our liver clinics from 2008 to 2012 for pretreatment assessment before receiving antiviral therapies. The treatments were provided at finite periods according to the National Health Insurance Policy in Taiwan. The last follow-up date was 31 December 2021. We analyzed the virological and clinical factors in these 790 CHB patients receiving finite periods of NA treatments and identified the most significant risk factors for HCC to establish a novel predictive scoring system. By using stepwise selection in a multivariate Cox proportional hazards model, we divided the patients into three risk groups. RESULTS: Our predictive scoring system included five independent variables: genotype C (adjusted HR [aHR] = 2.23), NA-withdraw-related hepatitis relapse (aHR = 6.96), male (aHR = 4.19), liver cirrhosis (aHR = 11.14), and T1768A core promoter mutation (aHR = 3.21). This model revealed significant differences in HCC incidence among the three risk groups. The 5-year cumulative HCC risk significantly differed among the three risk groups (low risk: 1.33%, moderate risk: 4.99%, and high risk: 17.46%), with log-rank test p < 0.001. CONCLUSION: Our predictive scoring system is a promising tool for the prediction of HCC in CHB patients receiving finite NA treatments. Genotype C, NA-withdraw-related hepatitis relapse, male gender, liver cirrhosis, and the T1768A HBV core promoter mutation were significant independent risk factors.
Full article
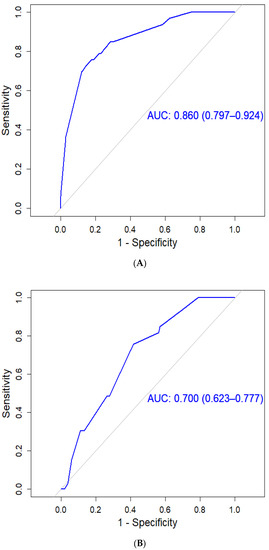
Figure 1
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}