
Year in Review: Gout Clinical Research
1
Division of Clinical Immunology and Rheumatology, University of Alabama at Birmingham, Birmingham, AL 35233, USA
2
Acute and Subspecialty Care Section, Birmingham VA Medical Center, Birmingham, AL 35233, USA
*
Author to whom correspondence should be addressed.
Gout Urate Cryst. Depos. Dis. 2023, 1(1), 37-48; https://doi.org/10.3390/gucdd1010005
Submission received: 22 November 2022
/
Revised: 23 February 2023
/
Accepted: 15 March 2023
/
Published: 20 March 2023
Abstract
:Gout is a prevalent and burdensome condition despite the advances in our knowledge of its underlying mechanisms, prevention, and treatment. There is still work to be done to elucidate relevant questions that could lead to better patient care. This conference report summarizes eight impactful publications which inform and improve clinical care in gout from October 2021 to October 2022. The articles we present here address innovative management approaches, the use of serum urate as a surrogate marker, the occurrence of complications such as cardiovascular events and lower extremity amputation, the evaluation of mortality in patients with chronic kidney disease and gout, the effect of intensive serum urate control on radiographic outcomes, and the impact of COVID-19 infection in patients with gout. The conclusions reached by these publications are noteworthy. Some of them are potentially practice-changing, and all provide exciting follow-up questions.
1. Introduction
Gout continues to be a significant burden on patients who experience it and still represents a large proportion of inflammatory joint diseases. We have elucidated key aspects of its pathogenesis, prevention, and treatment. However, there are still unanswered, relevant questions. The community of gout investigators has continued its efforts to provide answers to these questions over the past year.
The contributions to the field of clinical gout since the 2021 Gout, Hyperuricemia and Crystal-Associated Disease Network (GCAN) meeting span the study of gout prevention, its treatment, the evaluation of clinical and radiographic outcomes, the occurrence of complications like cardiovascular events, amputations, and death; and the impact of comorbidities such as chronic kidney disease and COVID-19.
This conference report presents an expanded overview of the plenary presentation “Year in Review: Gout Clinical Research” conducted at the eighth GCAN annual scientific meeting in Washington, DC, in October 2022.
2. Conference Sections
2.1. Evaluation of Supported Self-Management in Gout (GoutSMART): A Randomized Controlled Feasibility Trial [1]
Urate lowering is a standard objective of gout treatments and is associated with improved clinical outcomes. In routine clinical practice, patients often do not reach serum urate targets [2]. However, the UK’s Nottingham nurse-led study shows that most patients will achieve target urate levels with sufficient support and a treat-to-target approach to urate-lowering therapy [3]. Urate self-monitoring devices exist and have been reported as reliable [4]. Providers have successfully used patient self-management approaches in other chronic health conditions, like hypertension and congestive heart failure [5]. This knowledge led investigators to consider if a supported self-management approach to gout could work.
The researchers designed this study to compare the outcomes of a supported self-management approach with a standard treatment model in patients with gout. They developed a randomized, controlled, unblinded feasibility trial. They enrolled adults referred to the National Health System Lothian rheumatology service and patients from the Scottish Health Research Register (SHARE) with a diagnosis of gout, a physician recommendation of initiation or escalation of urate-lowering therapy (ULT), and a serum urate of 6 mg/dL (360 mmol/L) or higher. The group in the study that received the intervention had a cell phone app that allowed them to maintain a serum urate diary, report gout flares, keep quality of life diaries, and message the study team. They also received a hand-held device to check their serum urate level. They were instructed to self-test every two or four weeks depending on their current urate level and recent flares and logged their results in the app. The study group could then instruct them to adjust their allopurinol dose if needed. The usual care group continued to be managed by their primary care providers, who were instructed to change patients’ doses for a target urate of less than 5 mg/dL (300 mmol/L).
The study found that significantly more patients in the supported self-management group achieved the serum urate goal of less than 5 mg/dL at 24 weeks compared to patients in the usual care group (29/40 (73%) vs. 3/20 (14%), risk difference 0.58 (95% CI, 0.37 to 0.78)) (Figure 1). The intervention group took a significantly higher dose of allopurinol without a higher number of reported adverse events. Secondary outcomes, like the number of flares, medical appointments, and days missed at work, were better in the supported self-management group.
The authors concluded that the self-monitoring of urate levels was more effective than usual care in reaching target urate levels of less than 5 mg/dL at 24 weeks. Additionally, tighter urate control was associated with improved clinical outcomes, seemingly without more medication adverse events. This study provides an innovative approach to gout management and additional support for a treat-to-target strategy in gout. Its most significant limitation is its small sample size. However, as expressed above, this was a feasibility study. It will be necessary to see it replicated in a larger group. Generally, it seems like “augmented” strategies, with frequent follow-up, serum urate monitoring, and ULT dose adjustments, are beneficial in achieving target urate levels and improving clinical outcomes. The patients in the study appeared to be content with the app, albeit the authors did not gather the provider’s opinion.
2.2. Association between Serum Urate and Flares in People with Gout and Evidence for Surrogate Status: A Secondary Analysis of Two Randomized Controlled Trials [6]
Patient-centered outcomes are meaningful to patients and, as such, should be important to providers and researchers. Rheumatologists often use a surrogate, serum urate, under the assumption that achieving a target serum urate is associated with improved clinical outcomes. In line with this, the European Alliance of Associations for Rheumatology (EULAR) and American College of Rheumatology (ACR) guidelines recommend a treat-to-target approach [7,8]. Most clinical trials for ULT use serum urate as a primary efficacy outcome [9]. However, this is not universally accepted, as evidenced by the American College of Physicians (ACP) clinical practice guidelines recommendation of a treat-to-symptom approach [10]. Studies that have tried to examine the relationship of serum urate to symptoms, in particular gout flares, face multiple challenges: uniformity in reporting of flares and urate, the initial increase in flares after starting or dose escalating ULT, differences in the pattern of flares, differing approaches to pharmacological flare prophylaxis, and lastly, the delay in achieving a decrease in the frequency of flares after achieving a urate target. Recently, two trials of ULT were published that had a sufficiently long follow-up to allow a better understanding of the relationship between serum urate and the occurrence of gout flares [3,11,12].
The two clinical trials included individual-level data of participants randomly assigned to immediate dose escalation in a New Zealand study and from all the participants from a UK study. They compared individuals who, on average, achieved a serum urate concentration of less than 6 mg/dL at 6-, 9-, and 12-months post-baseline (serum urate responders) with those who did not reach the target urate. Their primary and secondary outcomes were related to gout flares, determined by self-report.
They found that fewer serum urate responders had a gout flare compared to non-responders between 12 and 24 months (91/343 (27%) vs. 156/245 (64%), adjusted odds ratio of 0.29 (95% CI, 0.17 to 0.51)). Moreover, the mean number of flares per individual was significantly lower in serum urate responders than in non-responders in the same period (adjusted mean difference of −1.41 (95% CI, −1.77 to −1.04)) (Table 1).
The study concludes that achieving a target serum urate of less than 6 mg/dL in patients with gout is associated with an absence of flares and a reduction in the number of flares in the subsequent year. It argues that the findings support a treat-to-target approach in the management of patients with gout. Additionally, it supports the continued use of serum urate as a surrogate outcome in gout trials, in which clinical outcomes are frequently impractical and even unfeasible due to the length of follow-up it would require to use them. Interestingly, in the New Zealand study, the association between serum urate responders and the occurrence of flares was not significant, and it appears that the UK study results mostly drive the study results. This could be because of the small number of participants in the former. There are certain things that this study could not address: the use of a ULT other than allopurinol, a subset analysis by sex, and the influence of foods and alcohol as triggers for flares. Additionally, there was some missing data regarding flare prophylaxis and serum urate results, which the authors managed with a carry-forward strategy.
2.3. Association between Gout Flare and Subsequent Cardiovascular Events among Patients with Gout [13]
Cardiovascular disease is the leading global cause of death, and inflammation is an important non-traditional risk factor for the development of cardiovascular disease [14,15]. People with gout, a common inflammatory condition, appear to have higher rates of cardiovascular disease independent of traditional cardiovascular risk factors [16,17,18,19].
This study aimed to evaluate if gout flares were associated with a transient increase in the rates of cardiovascular events. Using data from the Clinical Practice Research Datalink (a database with health records from primary care practices in the United Kingdom), the authors performed both a nested case-control study (cardiovascular event vs. not) and a self-controlled case series (patients with at least one gout flare and cardiovascular event). Participants were adults with a new diagnosis of gout. They defined a cardiovascular event as an acute myocardial infarction or stroke. Gout flares were defined using records from hospitalizations, primary care outpatient visits, and prescription records.
The researchers found that patients with cardiovascular events had significantly higher odds of having had a gout flare in the previous 0 to 60 days compared to patients without cardiovascular events (204/10,475 (2.0%) vs. 743/52,099 (1.4%); adjusted OR 1.93 (95% CI, 1.57 to 2.38)). There was no difference in the odds of a gout flare in the previous 121 to 180 days. In the self-controlled case series, there were significantly more cardiovascular events during the 180 days after the gout flare compared with the 150 days before or the 181 to 540 days after the gout flare (incidence rate ratio 1.65 (95% CI, 1.48 to 1.84)).
The study concludes that among individuals with gout, gout flares appear to be associated with a subsequent transient increase in cardiovascular events. The findings are robust to sensitivity analyses. Additionally, they derived from a large database representative of the general population in the UK, and the researchers ascertained the occurrence of gout flares and cardiovascular events with care. Two limitations worth mentioning are that data was only available for gout flares captured in the electronic health records and that the authors could not consider the severity of the flares as data were not consistently available. It will be interesting to continue to explore the mechanisms underlying the association, and perhaps causality, of inflammation in general and inflammation in gout with cardiovascular events. Alternatively, perhaps an opposite direction of effect, with individuals with cardiovascular events or risk factors being at higher risk of flares. Another question is if patients might benefit from anti-inflammatories for a prolonged time following a gout flare to reduce the probability of a cardiovascular event, which then raises the follow-up question of differences between anti-inflammatory drugs.
2.4. Allopurinol Initiation and All-Cause Mortality among Patients with Gout and Concurrent Chronic Kidney Disease [20]
Chronic kidney disease (CKD) is a common comorbidity in patients with gout [21,22]. Previous studies have examined the association between hyperuricemia with incident CKD and the therapeutic effects of ULT on the onset and progression of CKD with inconsistent results. Recently, two randomized controlled trials published in 2020 showed that allopurinol did not preserve renal function in patients with a renal disease without gout. Both also unexpectedly showed an association between allopurinol use and death, raising concern [23,24].
This group of investigators aimed to investigate the relationship between allopurinol initiation, reaching target serum urate, and escalating allopurinol dose with mortality in patients with gout and concomitant moderate-severe CKD. They designed propensity score-matched cohort studies using data from The Health Improvement Network (THIN), a database of primary care practices in the United Kingdom. They included adults aged 40 to 89 with gout and concomitant moderate-to-severe CKD. Their primary outcome was all-cause mortality in the five years following the date of initiation of allopurinol and a randomly selected index date for their controls.
They found that mortality was lower in people that initiated allopurinol when compared to those who did not (Hazard Ratio (HR) 0.85 (95% CI, 0.77 to 0.93)). Patients who achieved a target serum urate did not have higher mortality compared to those who did not reach it (risk difference −1.6 (95% CI, −3.6 to −0.5), HR 0.87 (95% CI, 0.75 to 1.01)). People who had their allopurinol dose-escalated and those who did not have dose escalation had no differences in mortality (risk difference −1.4 (95% CI, −3.7 to 0.4), HR 0.88 (95% CI 0.73 to 1.07)).
The study concludes that starting allopurinol, escalating its dose, and reaching target serum urate levels in people with gout and CKD is not associated with increased mortality. The results of this study are highly relevant to routine clinical practice since CKD and gout are frequently comorbid. This was a large study with results with the same direction of effect for the three evaluated associations, speaking to the robustness of the data. As an observational study using an existing database, there is a risk for residual confounding. The protective effect of starting allopurinol on mortality could be related to an indication bias: patients who started allopurinol might have received better healthcare. Alternatively, patients who did not receive allopurinol or have its dose escalated could be sicker, more frail adults. These results contribute to lay to rest some of the concerns of using allopurinol in patients with CKD generated by previous data.
2.5. Association of Sodium-Glucose Transport Protein 2 Inhibitor Use for Type 2 Diabetes and Incidence of Gout in Taiwan [25]
Type 2 diabetes (T2DM) is associated with hyperuricemia and is a common comorbidity for patients with gout [22]. Sodium-glucose transport protein 2 (SGLT2) inhibitors are the agent of choice for preventing diabetic kidney disease and cardiovascular disease in patients with T2DM. Previous studies have shown that SGLT2 inhibitors lowered serum urate levels [26]. Since hyperuricemia is a requisite risk factor for the development of gout, the investigators formulated the hypothesis that the use of SGLT2 inhibitors in patients with T2DM is associated with a decreased incidence of gout.
This study used data from Taiwan’s National Health Insurance database, which contains medical information on approximately 23 million Taiwanese citizens, to conduct a retrospective cohort study. They identified patients with T2DM with SGLT2 inhibitor prescriptions and compared them with patients with dipeptidyl peptidase 4 (DPP4) inhibitor prescriptions. They used propensity score matching to account for differences between the two treatment groups. Their primary outcome was the incidence of gout, ascertained with ICD codes. They followed patients from the prescription of SGLT2 inhibitors or DPP4 inhibitors starting in May 2016 until gout diagnosis, death, or the study ended in December 2018.
The researchers found that patients with T2DM receiving SLGT2 inhibitors had a lower risk of gout compared to patients receiving DPP4 inhibitors in univariate analysis (HR 0.89 (95% CI, 0.82 to 0.97)) as well as in a model adjusting for covariates (HR 0.89 (95% CI, 0.82 to 0.96)). In a sensitivity analysis in which they defined gout as the presence of an ICD code plus prescription of gout-specific medicine or acute medicine up to 14 days after diagnosis, the association of SGLT2 inhibitor use and the risk of gout was still present (HR 0.85 (95% CI, 0.69 to 0.98)).
The study concludes that using SLGT2 inhibitors is associated with a lower risk of gout than DPP4 inhibitors in patients with T2DM. The authors present three potential explanations for this association. First, SGLT2 inhibitors reduce serum urate levels via kidney tubular exchange. Second, SLGT2 inhibitors might enhance sirtuin-1, which inhibits xanthine oxidase, the sole enzyme responsible for the two final steps in the production of uric acid in mammals. These first two both work via reduced serum urate levels. Lastly, SLGT2 inhibitors might have a role in suppressing the NOD-, LRR-, and pyrin domain-containing 3 (NLRP3) inflammasome activation, which is key in gout flares. This study’s main strength is its large size. Its main limitation is the short follow-up period and the lack of serum urate results. These results pose the question of whether we should select SLGT2 inhibitors in patients with T2DM when they have hyperuricemia or gout.
2.6. Intensive Serum Urate Lowering with Oral Urate-Lowering Therapy for Erosive Gout: A Randomized Double-Blind Controlled Trial [27]
Bone erosions are the most common feature of structural joint damage in gout and can lead to joint deformity and disability [28,29,30]. Monosodium urate (MSU) crystal deposition closely relates to the sites of bone erosions and influences osteoblast and osteocyte function and viability [31,32,33,34]. This knowledge has led to the hypothesis that dissolving MSU crystals could prevent or heal gouty bone erosions. Previous studies have explored the association between achieving a target serum urate and the healing of bone erosions [35,36,37]. However, their results have yet to be consistent.
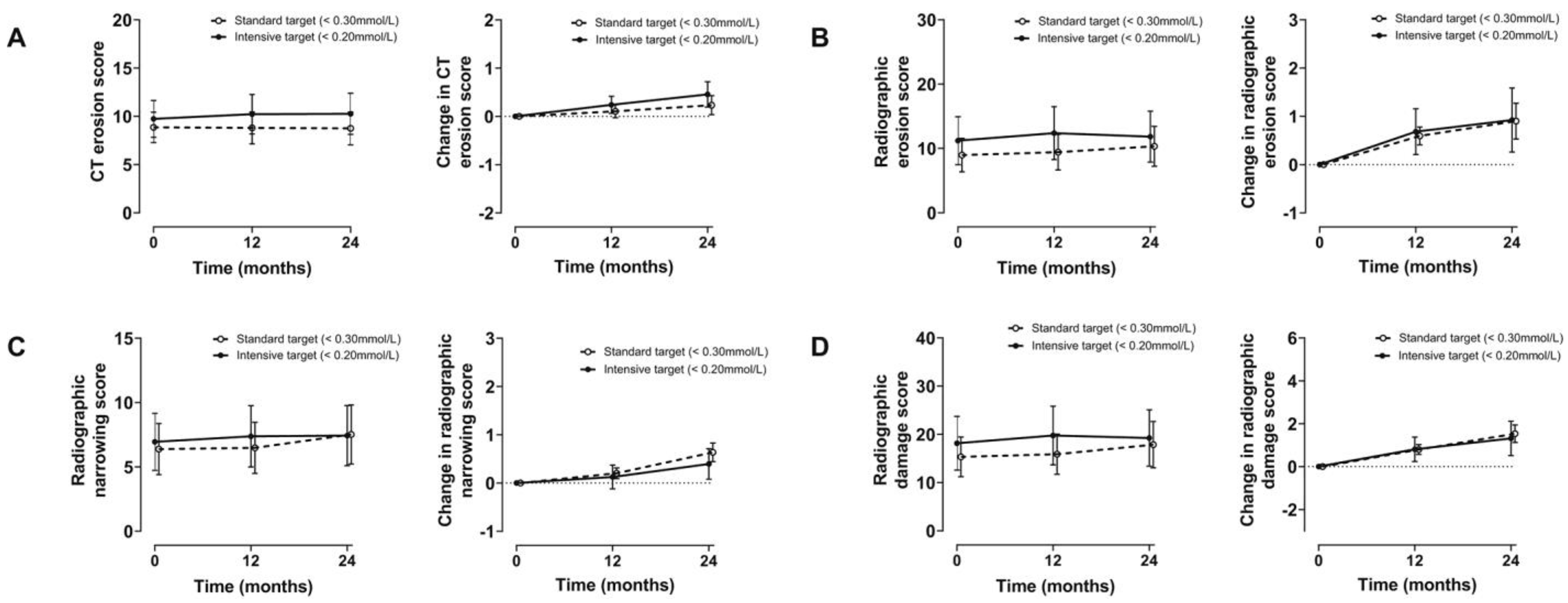
The researchers designed a randomized, double-blind, controlled trial to determine if intensive oral ULT with a serum urate goal of less than 3.3 mg/dL (0.2 mmol/L) was superior to a standard serum urate goal of less than 5 mg/dL (0.3 mmol/L) in improving computerized tomography bone erosion scores using oral ULT. Their primary outcome was the change in total computed tomography bone erosion score at 1 and 2 years compared to baseline.
The investigators found that the score increased minimally in both groups, and there was no difference between them (Figure 2). Additionally, patients in the intensive control group required higher doses of allopurinol and the addition of second agents more frequently than the standard control group. Both groups had improvements in the Outcome Measures in Rheumatology (OMERACT) gout core outcome domains, which include the number of gout flares, tophi, pain, patient’s global assessment of disease activity, quality of life, and activity limitation. However, there was no difference between them. Despite high doses of allopurinol and combination therapy, only 62% and 83% of patients achieved their serum urate target in the intensive and standard goal groups, respectively.
The study concludes that an intensive serum urate lowering strategy with oral medications is not superior to one aiming for a serum urate target goal of less than 5 mg/dL in improving bone erosions scores. It is also challenging to achieve intensive serum urate goals with oral ULT, and it causes a high medication burden. A significant achievement is that this is the first randomized controlled study to compare serum urate target goals. Its most significant limitation in comparing the targets is the inability to achieve and maintain the serum urate goals, especially the intensive goal of less than 3.3 mg/dL. The difficulty in reaching the intensive target with oral agents likely explains this study’s negative results. It is also possible that the control group, most of which reached a target serum urate of less than 5 mg/dL, was too good a comparator. Alternatively, perhaps, one must achieve profound serum urate reductions or maintain intensive control for a more prolonged period to see improvement in erosions.
2.7. Comparison of Rates of Lower Extremity Amputation in Patients with and without Gout in the US Department of Veterans Affairs Health System [38]
Gout is associated with comorbidities such as cardiovascular disease, hypertension, diabetes, and chronic kidney disease [39]. Many of these conditions are linked to an increased risk of lower extremity amputation (LEA) [40]. It is common to find reports of amputations in the context of gout, be it as comorbidity or as a postoperative diagnosis [41,42,43]. This link could be related to the comorbidities mentioned above. However, it is also possible that hyperuricemia and inflammation have an additive deleterious effect on vascular function or that gout manifestations are confused with foot infections.
This study aimed to evaluate the rate of LEA and the factors associated with it among patients with gout. The investigators used Veterans Affairs (VA) Clinical Data Warehouse data to conduct a matched cohort study. They included adult veterans with a diagnosis of gout based on ICD codes and age- and sex-matched them to controls without gout. The outcome was the occurrence of an LEA.
They found that patients with gout had a higher rate of LEA than people without gout, and the association remained significant after adjusting for covariates (adjusted Hazard Ratio (aHR) 1.20 (95% CI, 1.16 to 1.24)). Among patients with gout, suboptimal urate control -defined as serum urate greater than 7 mg/dL and the absence of ULT prescription- was associated with an increased LEA (aHR 1.26 (95% CI, 1.12 to 1.41)) in the year of observation. Patients with gout and diabetes had the highest rate of amputations (aHR 3.36 (95% CI, 3.02 to 3.75)).
The authors conclude that gout, independent of comorbidities, is associated with a 20% increase in the rate of LEA. LEA is undoubtedly a patient-centered outcome, so the results of this study are highly relevant. Another significant strength is its large sample size. Its limitations lie in its observational nature and inherent biases. It will be interesting to continue exploring gout’s association with LEA, including evaluating potential underlying mechanisms that could causally link gout, hyperuricemia, and inflammation to lower extremity damage leading to amputation. The goal would be to identify interventions that could prevent LEA among patients with gout.
2.8. Gout and the Risk of COVID-19 Diagnosis and Death in the UK Biobank: A Population-Based Study [44]
Gout is among the most common inflammatory joint conditions [2]. However, there was a paucity of data on the risk of acquiring COVID-19 or having bad outcomes from the infection in patients with gout. The investigators considered it essential to evaluate the association, given the potential for an increased risk that might require preventive strategies.
This study aims to evaluate the impact of gout on the risk of COVID-19 infection and its associated mortality with sufficient power to sex stratify and evaluate subsets of the population. The investigators used data from the UK Biobank, a large resource of approximately 500,000 volunteers aged 49 to 86 years at enrolment. They completed four analyses: (1) association between gout and COVID-19 diagnosis in a population-based cohort; (2) association between gout and COVID-19 death in patients diagnosed with COVID-19; (3) association between gout and COVID-19 death in a population-based cohort; (4) association between prescription of colchicine and ULT and the risk of COVID-19 related death among people with gout.
They found that people with gout were more likely to be diagnosed with COVID-19 in an unadjusted model (odds ratio (OR) 1.49 (95% CI, 1.31 to 1.51)) and a first model that included age, sex, ethnicity, socioeconomic index, BMI, and smoking status (OR 1.20 (95% CI, 1.11 to 1.29)). There was no association in a second model that included the above plus a list of 16 comorbidities (asthma, cancer, cerebrovascular diseases, chronic kidney disease, chronic obstructive pulmonary disease, dementia, diabetes, heart failure, hypertensive diseases, immunodeficiencies, interstitial lung disease, ischemic heart disease, lipoprotein disorders, liver failure, osteoarthritis, and pulmonary heart diseases).
Among patients diagnosed with COVID-19, patients with gout were more likely to die in the unadjusted test (OR 2.97 (95% CI, 2.45 to 3.62)) and model 1 (OR 1.44 (95% CI, 1.16 to 1.78)), but not in model 2.
In the population-based cohort, gout was associated with COVID-19-related death in the unadjusted analysis (OR 3.93 (95% CI, 3.28 to 4.70)), model 1 (OR 1.76 (95% CI, 1.46 to 2.12)), and model 2 (OR 1.29 (95% CI, 1.06 to 1.56)). In this analysis, women with gout had an increased risk of COVID-19-related death. The OR did not overlap with men’s risk in the unadjusted model (OR 9.37 (95% CI, 6.58 to 13.35)) or model 1 (OR 3.49 (95% CI, 2.41 to 5.04)). In model 2, women with gout continued to have an association with COVID-19-related death (OR 1.98 (95% CI, 1.34 to 2.94)), but the OR overlapped with the men’s OR (Table 2).
In the final analysis, there were no differences in the risk for COVID-19-related death between individuals with gout with and without a colchicine prescription and with and without a ULT prescription. All four groups had overlapping confidence intervals in their comparisons against non-gout controls.
The study concludes that gout is a risk factor for COVID-19 diagnosis and COVID-19-related death in women, independently of metabolic comorbidities. To our knowledge, it was the first study to evaluate the association of gout with COVID-19 by sex stratification, which it could do due to its large size. Unfortunately, the authors could not account for the severity of gout, medication adherence, and the role of vaccination. Based on these results, we should target women with gout for COVID-19-related prevention based on these results more deliberately.
3. Concluding Remarks
The conclusions reached by these publications are noteworthy and span different aspects of gout care. A summary of the main findings, strengths, and limitations of the studies discussed are presented in Table 3.
Two studies prove that treat-to-target approaches via an innovative guided self-management approach or traditional care are associated with improved clinical outcomes. At the same time, an intensive control strategy with a urate goal of less than 3.3 mg/dL was challenging to achieve with oral ULT and not superior to the more standard goal of less than 5 mg/dL in improving radiographic erosion scores.
We have further evidence of the negative impact of gout. A study showed that gout flares are associated with a subsequent transient increase in cardiovascular events. Patients with gout undergo lower extremity amputations more often than their peers, independent of comorbidities. Lastly, gout is a risk factor for acquiring COVID-19 and COVID-19-related death.
On the other hand, we get some reassurance that using allopurinol, escalating its dose, and reaching target urate levels in patients with gout and CKD are not associated with an increase in mortality.
Lastly, a novel class of agents in gout care, SLGT2 inhibitors, appears as an option that, asides from their known hypouricemic effect, seems to lower the risk for incident gout among patients with diabetes.
Multiple follow-up questions have arisen from these publications. It will be interesting to see the development of studies that address them over the next few years.
Author Contributions
Conceptualization, M.U. and A.L.G.; investigation, M.U. and A.L.G.; resources, M.U. and A.L.G.; writing—original draft preparation, M.U.; writing—review and editing, A.L.G. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Riches, P.L.; Alexander, D.; Hauser, B.; Kuske, B.; Krause, A. Evaluation of supported self-management in gout (GoutSMART): A randomised controlled feasibility trial. Lancet Rheumatol. 2022, 4, e320–e328. [Google Scholar] [CrossRef]
- Kuo, C.-F.; Grainge, M.J.; Mallen, C.; Zhang, W.; Doherty, M. Rising burden of gout in the UK but continuing suboptimal management: A nationwide population study. Ann. Rheum. Dis. 2014, 74, 661–667. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doherty, M.; Jenkins, W.; Richardson, H.; Sarmanova, A.; Abhishek, A.; Ashton, D.; Barclay, C.; Doherty, S.; Duley, L.; Hatton, R.; et al. Efficacy and cost-effectiveness of nurse-led care involving education and engagement of patients and a treat-to-target urate-lowering strategy versus usual care for gout: A randomised controlled trial. Lancet 2018, 392, 1403–1412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paraskos, J.; Berke, Z.; Cook, J.; Miner, J.N.; Braddock, M.; Platt, A.; Hughes, G. An analytical comparison between point-of-care uric acid testing meters. Expert Rev. Mol. Diagn. 2016, 16, 373–382. [Google Scholar] [CrossRef] [PubMed]
- Hammersley, V.; Parker, R.; Paterson, M.; Hanley, J.; Pinnock, H.; Padfield, P.; Stoddart, A.; Park, H.G.; Sheikh, A.; McKinstry, B. Telemonitoring at scale for hypertension in primary care: An implementation study. PLoS Med. 2020, 17, e1003124. [Google Scholar] [CrossRef]
- Stamp, L.K.; Frampton, C.; Morillon, M.B.; Taylor, W.J.; Dalbeth, N.; Singh, J.; Doherty, M.; Zhang, W.; Richardson, H.; Sarmanova, A.; et al. Association between serum urate and flares in people with gout and evidence for surrogate status: A secondary analysis of two randomised controlled trials. Lancet Rheumatol. 2021, 4, e53–e60. [Google Scholar] [CrossRef]
- FitzGerald, J.D.; Dalbeth, N.; Mikuls, T.; Brignardello-Petersen, R.; Guyatt, G.; Abeles, A.M.; Neogi, T. 2020 American College of Rheumatology Guideline for the Management of Gout. Arthritis Care Res. 2020, 72, 744–760. [Google Scholar] [CrossRef]
- Richette, P.; Doherty, M.; Pascual, E.; Barskova, V.; Becce, F.; Castañeda-Sanabria, J.; Bardin, T. 2016 updated EULAR evidence-based recommendations for the management of gout. Ann. Rheum. Dis. 2017, 76, 29–42. [Google Scholar] [CrossRef] [Green Version]
- Schumacher, H.R.; Taylor, W.; Edwards, L.; Grainger, R.; Schlesinger, N.; Dalbeth, N.; Sivera, F.; Singh, J.; Evans, R.; Waltrip, R.W.; et al. Outcome Domains for Studies of Acute and Chronic Gout. J. Rheumatol. 2009, 36, 2342–2345. [Google Scholar] [CrossRef]
- Qaseem, A.; Harris, R.P.; Forciea, M.A.; Denberg, T.D.; Barry, M.J.; Boyd, C.; Clinical Guidelines Committee of the American College of Physicians. Management of Acute and Recurrent Gout: A Clinical Practice Guideline from the American College of Physicians. Ann. Intern. Med. 2017, 166, 58–68. [Google Scholar] [CrossRef] [Green Version]
- Stamp, L.K.; Chapman, P.T.; Barclay, M.; Horne, A.; Frampton, C.; Tan, P.; Drake, J.; Dalbeth, N. Allopurinol dose escalation to achieve serum urate below 6 mg/dL: An open-label extension study. Ann. Rheum. Dis. 2017, 76, 2065–2070. [Google Scholar] [CrossRef]
- Stamp, L.K.; Chapman, P.T.; Barclay, M.L.; Horne, A.; Frampton, C.; Tan, P.; Drake, J.; Dalbeth, N. A randomised controlled trial of the efficacy and safety of allopurinol dose escalation to achieve target serum urate in people with gout. Ann. Rheum. Dis. 2017, 76, 1522–1528. [Google Scholar] [CrossRef]
- Cipolletta, E.; Tata, L.J.; Nakafero, G.; Avery, A.J.; Mamas, M.A.; Abhishek, A. Association Between Gout Flare and Subsequent Cardiovascular Events among Patients with Gout. JAMA 2022, 328, 440–450. [Google Scholar] [CrossRef]
- Roth, G.A.; Mensah, G.A.; Johnson, C.O.; Addolorato, G.; Ammirati, E.; Baddour, L.M.; Barengo, N.C.; Beaton, A.Z.; Benjamin, E.J.; Benziger, C.P.; et al. Global Burden of Cardiovascular Diseases and Risk Factors, 1990–2019: Update from the GBD 2019 Study. J. Am. Coll. Cardiol. 2020, 76, 2982–3021. [Google Scholar] [CrossRef]
- Willerson, J.T.; Ridker, P.M. Inflammation as a cardiovascular risk factor. Circulation 2004, 109 (Suppl. 1), Ii2–Ii10. [Google Scholar] [CrossRef] [Green Version]
- De Vera, M.A.; Rahman, M.M.; Bhole, V.; Kopec, J.A.; Choi, H.K. Independent impact of gout on the risk of acute myocardial infarction among elderly women: A population-based study. Ann. Rheum. Dis. 2010, 69, 1162–1164. [Google Scholar] [CrossRef]
- Choi, H.K.; Curhan, G. Independent Impact of Gout on Mortality and Risk for Coronary Heart Disease. Circulation 2007, 116, 894–900. [Google Scholar] [CrossRef] [Green Version]
- Kuo, C.-F.; Yu, K.-H.; See, L.-C.; Chou, I.-J.; Ko, Y.-S.; Chang, H.-C.; Chiou, M.-J.; Luo, S.-F. Risk of myocardial infarction among patients with gout: A nationwide population-based study. Rheumatology 2012, 52, 111–117. [Google Scholar] [CrossRef] [Green Version]
- Krishnan, E.; Baker, J.F.; Furst, D.E.; Schumacher, H.R. Gout and the risk of acute myocardial infarction. Arthritis Rheumatol. 2006, 54, 2688–2696. [Google Scholar] [CrossRef]
- Wei, J.; Choi, H.K.; Neogi, T.; Dalbeth, N.; Terkeltaub, R.; Stamp, L.K.; Zhang, Y. Allopurinol Initiation and All-Cause Mortality among Patients with Gout and Concurrent Chronic Kidney Disease: A Population-Based Cohort Study. Ann. Intern. Med. 2022, 175, 461–470. [Google Scholar] [CrossRef]
- Zhu, Y.; Pandya, B.J.; Choi, H.K. Comorbidities of gout and hyperuricemia in the US general population: NHANES 2007–2008. Am. J. Med. 2012, 125, 679–687.e1. [Google Scholar] [CrossRef] [PubMed]
- Bevis, M.; Blagojevic-Bucknall, M.; Mallen, C.; Hider, S.; Roddy, E. Comorbidity clusters in people with gout: An observational cohort study with linked medical record review. Rheumatology 2018, 57, 1358–1363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Badve, S.V.; Pascoe, E.M.; Tiku, A.; Boudville, N.; Brown, F.G.; Cass, A.; Clarke, P.; Dalbeth, N.; Day, R.O.; de Zoysa, J.R.; et al. Effects of Allopurinol on the Progression of Chronic Kidney Disease. N. Engl. J. Med. 2020, 382, 2504–2513. [Google Scholar] [CrossRef] [PubMed]
- Doria, A.; Galecki, A.T.; Spino, C.; Pop-Busui, R.; Cherney, D.Z.; Lingvay, I.; Parsa, A.; Rossing, P.; Sigal, R.J.; Afkarian, M.; et al. Serum Urate Lowering with Allopurinol and Kidney Function in Type 1 Diabetes. N. Engl. J. Med. 2020, 382, 2493–2503. [Google Scholar] [CrossRef]
- Chung, M.-C.; Hung, P.-H.; Hsiao, P.-J.; Wu, L.-Y.; Chang, C.-H.; Wu, M.-J.; Shieh, J.-J.; Chung, C.-J. Association of Sodium-Glucose Transport Protein 2 Inhibitor Use for Type 2 Diabetes and Incidence of Gout in Taiwan. JAMA Netw. Open 2021, 4, e2135353. [Google Scholar] [CrossRef]
- Van Bommel, E.J.M.; Muskiet, M.H.A.; Tonneijck, L.; Kramer, M.H.H.; Nieuwdorp, M.; van Raalte, D.H. SGLT2 Inhibition in the Diabetic Kidney—From Mechanisms to Clinical Outcome. Clin. J. Am. Soc. Nephrol. 2017, 12, 700–710. [Google Scholar] [CrossRef] [Green Version]
- Dalbeth, N.; Doyle, A.J.; Billington, K.; Gamble, G.D.; Tan, P.; Latto, K.; Ram, T.P.; Narang, R.; Murdoch, R.; Bursill, D.; et al. Intensive Serum Urate Lowering with Oral Urate-Lowering Therapy for Erosive Gout: A Randomized Double-Blind Controlled Trial. Arthritis Rheumatol. 2022, 74, 1059–1069. [Google Scholar] [CrossRef]
- Dalbeth, N.; Clark, B.; McQueen, F.; Doyle, A.; Taylor, W. Validation of a radiographic damage index in chronic gout. Arthritis Rheumatol. 2007, 57, 1067–1073. [Google Scholar] [CrossRef]
- Stewart, S.; Aati, O.; Horne, A.; Doyle, A.J.; Dalbeth, N. Radiographic damage scores predict grip strength in patients with tophaceous gout. Rheumatology 2019, 59, 1440–1442. [Google Scholar] [CrossRef]
- Stewart, S.; Rome, K.; Eason, A.; House, M.E.; Horne, A.; Doyle, A.J.; Knight, J.; Taylor, W.J.; Dalbeth, N. Predictors of activity limitation in people with gout: A prospective study. Clin. Rheumatol. 2018, 37, 2213–2219. [Google Scholar] [CrossRef]
- Dalbeth, N.; Aati, O.; Kalluru, R.; Gamble, G.D.; Horne, A.; Doyle, A.J.; McQueen, F.M. Relationship between structural joint damage and urate deposition in gout: A plain radiography and dual-energy CT study. Ann. Rheum. Dis. 2014, 74, 1030–1036. [Google Scholar] [CrossRef]
- Towiwat, P.; Doyle, A.J.; Gamble, G.D.; Tan, P.; Aati, O.; Horne, A.; Dalbeth, N. Urate crystal deposition and bone erosion in gout: ‘Inside-out’ or ‘outside-in’? A dual-energy computed tomography study. Arthritis Res. Ther. 2016, 18, 208. [Google Scholar] [CrossRef] [Green Version]
- Chhana, A.; Callon, K.E.; Pool, B.; Naot, D.; Watson, M.; Gamble, G.D.; McQueen, F.M.; Cornish, J.; Dalbeth, N. Monosodium urate monohydrate crystals inhibit osteoblast viability and function: Implications for development of bone erosion in gout. Ann. Rheum. Dis. 2011, 70, 1684–1691. [Google Scholar] [CrossRef]
- Chhana, A.; Pool, B.; Callon, K.E.; Tay, M.L.; Musson, D.; Naot, D.; McCarthy, G.; McGlashan, S.; Cornish, J.; Dalbeth, N. Monosodium urate crystals reduce osteocyte viability and indirectly promote a shift in osteocyte function towards a proinflammatory and proresorptive state. Thromb. Haemost. 2018, 20, 208. [Google Scholar] [CrossRef] [Green Version]
- Dalbeth, N.; Billington, K.; Doyle, A.; Frampton, C.; Tan, P.; Aati, O.; Allan, J.; Drake, J.; Horne, A.; Stamp, L.K. Effects of Allopurinol Dose Escalation on Bone Erosion and Urate Volume in Gout: A Dual-Energy Computed Tomography Imaging Study within a Randomized, Controlled Trial. Arthritis Rheumatol. 2019, 71, 1739–1746. [Google Scholar] [CrossRef]
- Sundy, J.S.; Baraf, H.S.; Yood, R.A.; Edwards, N.L.; Gutierrez-Urena, S.R.; Treadwell, E.L.; Becker, M.A. Efficacy and tolerability of pegloticase for the treatment of chronic gout in patients refractory to conventional treatment: Two randomized controlled trials. Jama 2011, 306, 711–720. [Google Scholar]
- Dalbeth, N.; Doyle, A.J.; McQueen, F.M.; Sundy, J.; Baraf, H.S.B. Exploratory study of radiographic change in patients with tophaceous gout treated with intensive urate-lowering therapy. Arthritis Care Res. 2013, 66, 82–85. [Google Scholar] [CrossRef]
- Mikuls, T.R.; Soto, Q.; Petro, A.; Helget, L.; Roul, P.; Sayles, H.; Cope, B.; Neogi, T.; LaMoreaux, B.; O’Dell, J.R.; et al. Comparison of Rates of Lower Extremity Amputation in Patients with and without Gout in the US Department of Veterans Affairs Health System. JAMA Netw. Open 2022, 5, e2142347. [Google Scholar] [CrossRef]
- Mikuls, T.R.; Farrar, J.T.; Bilker, W.B.; Fernandes, S.; Schumacher, H.R., Jr.; Saag, K.G. Gout epidemiology: Results from the UK General Practice Research Database, 1990–1999. Ann. Rheum. Dis. 2005, 64, 267–272. [Google Scholar] [CrossRef]
- Cai, M.; Xie, Y.; Bowe, B.; Gibson, A.K.; Zayed, M.A.; Li, T.; Al-Aly, Z. Temporal Trends in Incidence Rates of Lower Extremity Amputation and Associated Risk Factors among Patients Using Veterans Health Administration Services from 2008 to 2018. JAMA Netw. Open 2021, 4, e2033953. [Google Scholar] [CrossRef]
- Sariyilmaz, K.; Eren, I.; Ozkunt, O.; Sungur, M.; Kilicoglu, O.I.; Dikici, F. Bilateral First-Ray Amputation of the Foot Due to Severe Tophaceous Gout Complicated by Infection and Discharged Sinus (A Case Report). J. Am. Podiatr. Med. Assoc. 2018, 108, 58–62. [Google Scholar] [CrossRef] [PubMed]
- Yu, K.H.; Luo, S.F.; Liou, L.B.; Wu, Y.J.; Tsai, W.P.; Chen, J.Y.; Ho, H.H. Concomitant septic and gouty arthritis—An analysis of 30 cases. Rheumatology 2003, 42, 1062–1066. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, C.; Xue, C.; Yang, B.; Wang, W.; Xu, Y.; Huang, F.; Wang, Y. Amputation of the first metatarsophalangeal joint due to a giant gouty tophi: A case report. Medicine 2017, 96, e8441. [Google Scholar] [CrossRef] [PubMed]
- Topless, R.K.; Gaffo, A.; Stamp, L.K.; Robinson, P.C.; Dalbeth, N.; Merriman, T.R. Gout and the risk of COVID-19 diagnosis and death in the UK Biobank: A population-based study. Lancet Rheumatol. 2022, 4, e274–e281. [Google Scholar] [CrossRef]
Figure 1.
Urate results (mean urate (SD)) over the course of the study. (Reprinted from [1], with permission from Elsevier).
Figure 1.
Urate results (mean urate (SD)) over the course of the study. (Reprinted from [1], with permission from Elsevier).

Figure 2.
Imaging outcomes. (A), Computed tomography (CT) bone erosion scores. (B), Plain radiographic bone erosion scores. (C), Plain radiographic joint space narrowing scores. (D), Plain radiographic joint damage scores. Values are the observed mean and 95% confidence interval. (Reprinted from [27], with permission from Wiley).
Figure 2.
Imaging outcomes. (A), Computed tomography (CT) bone erosion scores. (B), Plain radiographic bone erosion scores. (C), Plain radiographic joint space narrowing scores. (D), Plain radiographic joint damage scores. Values are the observed mean and 95% confidence interval. (Reprinted from [27], with permission from Wiley).


{kind=link}
{kind=link}
Table 1.
Primary and secondary outcomes by serum urate responder status. (Reprinted from [6], with permission from Elsevier).
Table 1.
Primary and secondary outcomes by serum urate responder status. (Reprinted from [6], with permission from Elsevier).
| Serum Urate Responder | Serum Urate Non-Responder | OR (95% CI) or Mean Difference between Groups (95% CI) | p Value | |
|---|---|---|---|---|
| Unadjusted | ||||
| Nottingham | n = 290 | n = 227 | ||
| Participants with gout flare | 75 (26%) | 148 (65%) | 0.19 (0.13 to 0.27) | <0.0001 |
| Number of gout flares | 0.63 (0.05) | 2.41 (0.10) | −1.78 (−2.0 to −1.55) | <0.0001 |
| New Zealand | n = 53 | n = 18 | ||
| Participants with gout flare | 16 (30%) | 8 (44%) | 0.54 (0.18 to 1.62) | 0.27 |
| Number of gout flares | 0.81 (0.12) | 1.0 (0.24) | −0.19 (−0.71 to 0.33) | 0.48 |
| Combined | n = 343 | n = 245 | ||
| Participants with gout flare | 91 (27%) | 156 (64%) | 0.20 (0.15 to 0.29) | <0.0001 |
| Number of gout flares | 0.66 (0.04) | 2.31 (0.10) | −1.64 (−1.85 to −1.44) | <0.0001 |
| Adjusted * | ||||
| Nottingham | n = 290 | n = 227 | ||
| Participants with gout flare | 75 (26%) | 148 (65%) | 0.18 (0.10 to 0.32) | <0.0001 |
| Number of gout flares | 0.55 (0.05) | 2.17 (0.16) | −1.62 (−1.97 to −1.28) | <0.0001 |
| New Zealand | n = 53 | n = 18 | ||
| Participants with gout flare | 16 (30%) | 8 (44%) | 0.53 (0.17 to 1.61) | 0.26 |
| Number of gout flares | 0.86 (0.13) | 1.06 (0.25) | −0.20 (−0.76 to 0.35) | 0.47 |
| Combined | n = 343 | n = 245 | ||
| Participants with gout flare | 91 (27%) | 156 (64%) | 0.22 (0.13 to 0.37) | <0.0001 |
| Number of gout flares | 0.61 (0.05) | 1.94 (0.14) | −1.33 (−1.64 to −1.03) | <0.0001 |
| Adjusted ** | ||||
| Nottingham | n = 290 | n = 227 | ||
| Participants with gout flare | 76 (26%) | 148 (65%) | 0.24 (0.12 to 0.47) | <0.0001 |
| Number of gout flares | 0.65 (0.06) | 2.52 (0.22) | −1.88 (−2.34 to −1.41) | <0.0001 |
| New Zealand | n = 53 | n = 18 | ||
| Participants with gout flare | 16 (30%) | 8 (44%) | 0.53 (0.17 to 1.62) | 0.26 |
| Number of gout flares | 0.81 (0.13) | 0.99 (0.24) | −0.18 (−0.70 to 0.34) | 0.50 |
| Combined | n = 343 | n = 245 | ||
| Participants with gout flare | 91 (27%) | 156 (64%) | 0.29 (0.17 to 0.51) | <0.0001 |
| Number of gout flares | 0.69 (0.06) | 2.09 (0.17) | −1.41 (−1.77 to −1.04) | <0.0001 |
Data are n (%) or mean (SE). OR = odds ratio. OR for primary outcome; mean difference for secondary outcome. * Adjusted for flare history (and randomised group for the Nottingham data). ** Adjusted for flare history, baseline serum urate, and baseline tophi (and randomised group for Nottingham data).
Table 2.
Association of gout with diagnosis and outcomes of COVID-19. (Reprinted from [44], with permission from Elsevier).
Table 2.
Association of gout with diagnosis and outcomes of COVID-19. (Reprinted from [44], with permission from Elsevier).
| Diagnosis of COVID-19 | COVID-19-Related Death in COVID-19 Cohort | COVID-19-Related Death in Entire Cohort | ||||
|---|---|---|---|---|---|---|
| OR (95% CI) | p Value | OR (95% CI) | p Value | OR (95% CI) | p Value | |
| Unadjusted | ||||||
| Combined | 1.49 (1.39–1.60) | <0.0001 | 2.97 (2.45–3.62) | <0.0001 | 3.93 (3.28–4.70) | <0.0001 |
| Men | 1.34 (1.24–1.45) | <0.0001 | 1.99 (1.58–2.50) | <0.0001 | 2.43 (1.97–3.00) | <0.0001 |
| Women | 1.96 (1.67–2.30) | <0.0001 | 5.74 (3.86–8.53) | <0.0001 | 9.37 (6.58–13.35) | <0.0001 |
| Model 1 * | ||||||
| Combined | 1.41 (1.31–1.51) | <0.0001 | 1.44 (1.16–1.78) | 0.00091 | 1.76 (1.46–2.12) | <0.0001 |
| Men | 1.27 (1.17–1.38) | <0.0001 | 1.25 (0.98–1.60) | 0.073 | 1.47 (1.19–1.83) | 0.00044 |
| Women | 1.91 (1.62–2.24) | <0.0001 | 2.34 (1.51–3.62) | 0.00013 | 3.49 (2.41–5.04) | <0.0001 |
| Model 2 ** | ||||||
| Combined | 1.20 (1.11–1.29) | <0.0001 | 1.20 (0.96–1.51) | 0.11 | 1.29 (1.06–1.56) | 0.013 |
| Men | 1.12 (1.03–1.22) | 0.0066 | 1.11 (0.85–1.44) | 0.44 | 1.16 (0.93–1.45) | 0.20 |
| Women | 1.44 (1.22–1.70) | <0.0001 | 1.65 (1.04–2.64) | 0.035 | 1.98 (1.34–2.94) | 0.00062 |
OR = odds ratio. * Model 1 was adjusted for age group, sex, ethnicity, Townsend deprivation index, BMI, and smoking status. ** Model 2 was adjusted for age group, sex, ethnicity, Townsend deprivation index, BMI, and smoking status, plus 16 other diseases.
Table 3.
Summary of main findings, strengths, and limitations.
| Study | Main Finding | Strengths | Limitations |
|---|---|---|---|
| Evaluation of supported self-management in gout (GoutSMART): a randomized controlled feasibility trial | More patients in a supported self-management group achieved a serum urate goal of less than 5 mg/dL at 24 weeks compared to patients in a usual care group. | Innovative approach to gout management. | Feasibility study with a small sample size. |
| Association between serum urate and flares in people with gout and evidence for surrogate status: a secondary analysis of two randomized controlled trials | Fewer serum urate responders had a gout flare compared to non-responders between 12 and 24 months. | Validates serum urate as a surrogate for a patient-centered outcome: acute flares. | Unable to account for the use of ULT other than allopurinol, subset by sex, or analyze the influence of foods and alcohol as triggers for flares. |
| Association between gout flare and subsequent cardiovascular events among patients with gout | Patients with cardiovascular events had significantly higher odds of having had a gout flare in the previous 0 to 60 days compared to patients without cardiovascular events. | Findings were robust to sensitivity analyses. Derived from a large database representative of the general population. Care in the ascertainment of predictors and outcomes. | Data is only available for events captured in electronic health records. Unable to consider the severity of flares. |
| Allopurinol initiation and all-cause mortality among patients with gout and concurrent chronic kidney disease | Mortality was lower in people that initiated allopurinol when compared to those who did not. | Large study. Robust results, with the same direction of effect for the evaluated associations. | Observational study using an existing database, hence with risk for residual confounding. |
| Association of Sodium-Glucose Transport Protein 2 Inhibitor Use for Type 2 Diabetes and Incidence of Gout in Taiwan | Individuals with type 2 diabetes receiving SLGT2 inhibitors had a lower risk of gout compared to those receiving DPP4 inhibitors. | Large size. Novel gout treatment target. | Short follow-up period. Lack of serum urate results. |
| Intensive serum urate lowering with oral urate-lowering therapy for erosive gout: a randomized, double-blind controlled trial | A radiographic bone erosion score worsened in individuals with an intensive serum urate control goal of less than 3.3 mg/dL and those with a goal of less than 5 mg/dL. There was no difference between the two. | First randomized controlled study to compare serum urate target goals. | Unable to obtain and maintain the serum urate goals. |
| Comparison of rates of lower extremity amputation in patients with and without gout in the US Department of Veterans Affairs health system | Individuals with gout had a higher rate of lower extremity amputations than people without gout. | Use of a patient-centered outcome. Large sample size. | Observational study. |
| Gout and the risk of COVID-19 diagnosis and death in the UK Biobank: a population-based study | Gout is a risk factor for COVID-19 diagnosis and COVID-19-related death in women, independent of metabolic comorbidities. | First study to evaluate the association of gout with COVID-19 by sex stratification. Large sample size. | Unable to account for the severity of gout, medication adherence, and the role of vaccination. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Urquiaga, M.; Gaffo, A.L. Year in Review: Gout Clinical Research. Gout Urate Cryst. Depos. Dis. 2023, 1, 37-48. https://doi.org/10.3390/gucdd1010005
AMA Style
Urquiaga M, Gaffo AL. Year in Review: Gout Clinical Research. Gout, Urate, and Crystal Deposition Disease. 2023; 1(1):37-48. https://doi.org/10.3390/gucdd1010005
Chicago/Turabian StyleUrquiaga, Mariana, and Angelo L. Gaffo. 2023. "Year in Review: Gout Clinical Research" Gout, Urate, and Crystal Deposition Disease 1, no. 1: 37-48. https://doi.org/10.3390/gucdd1010005