
Colchicine Use and Major Adverse Cardiovascular Events in Male Patients with Gout and Established Coronary Artery Disease: A Veterans Affairs Nested Retrospective Cohort Study
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Patient Identification
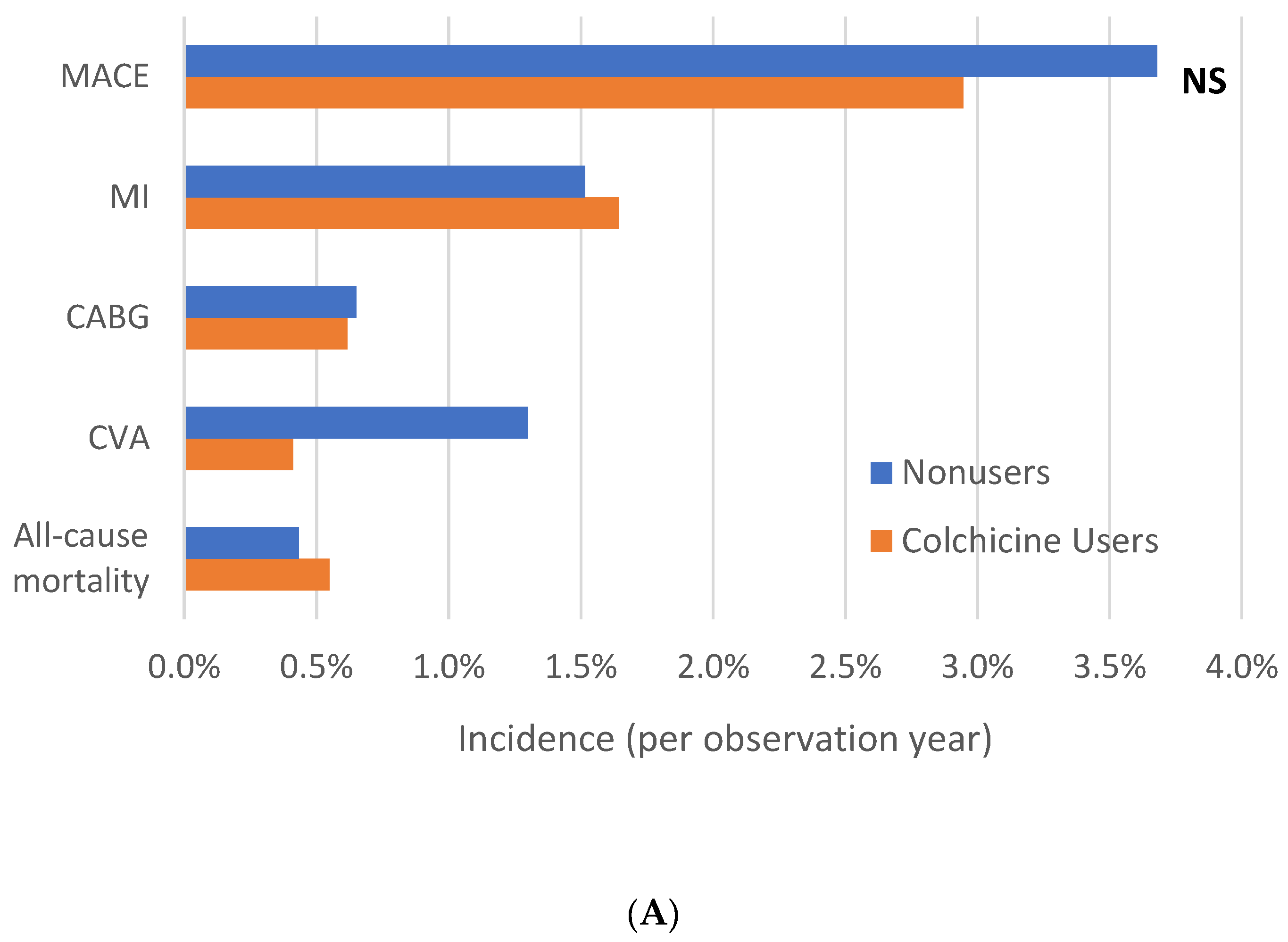
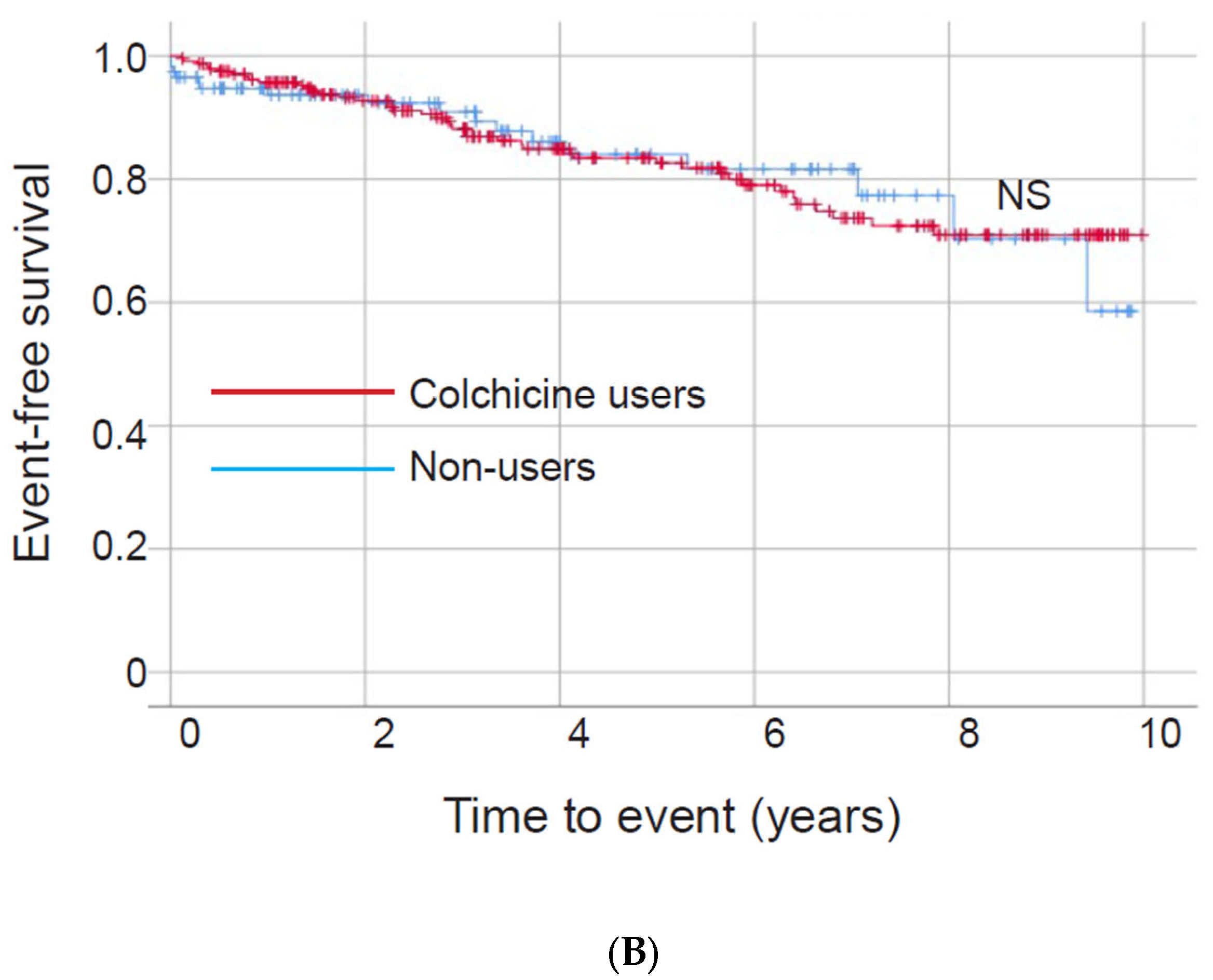
3.2. Part I: Colchicine Nonusers versus Users
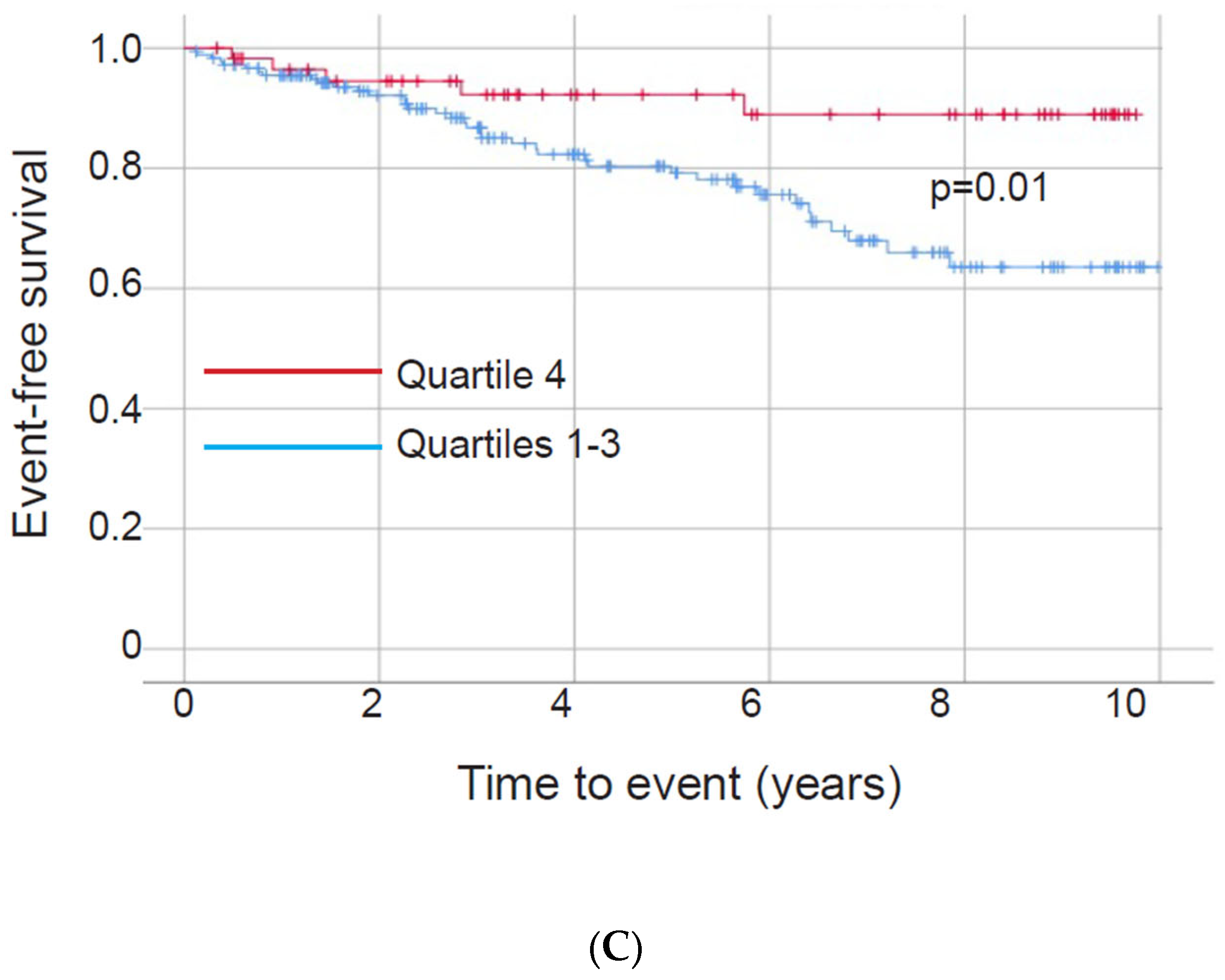
3.3. Part II: Colchicine Group—Consistency of Colchicine Use
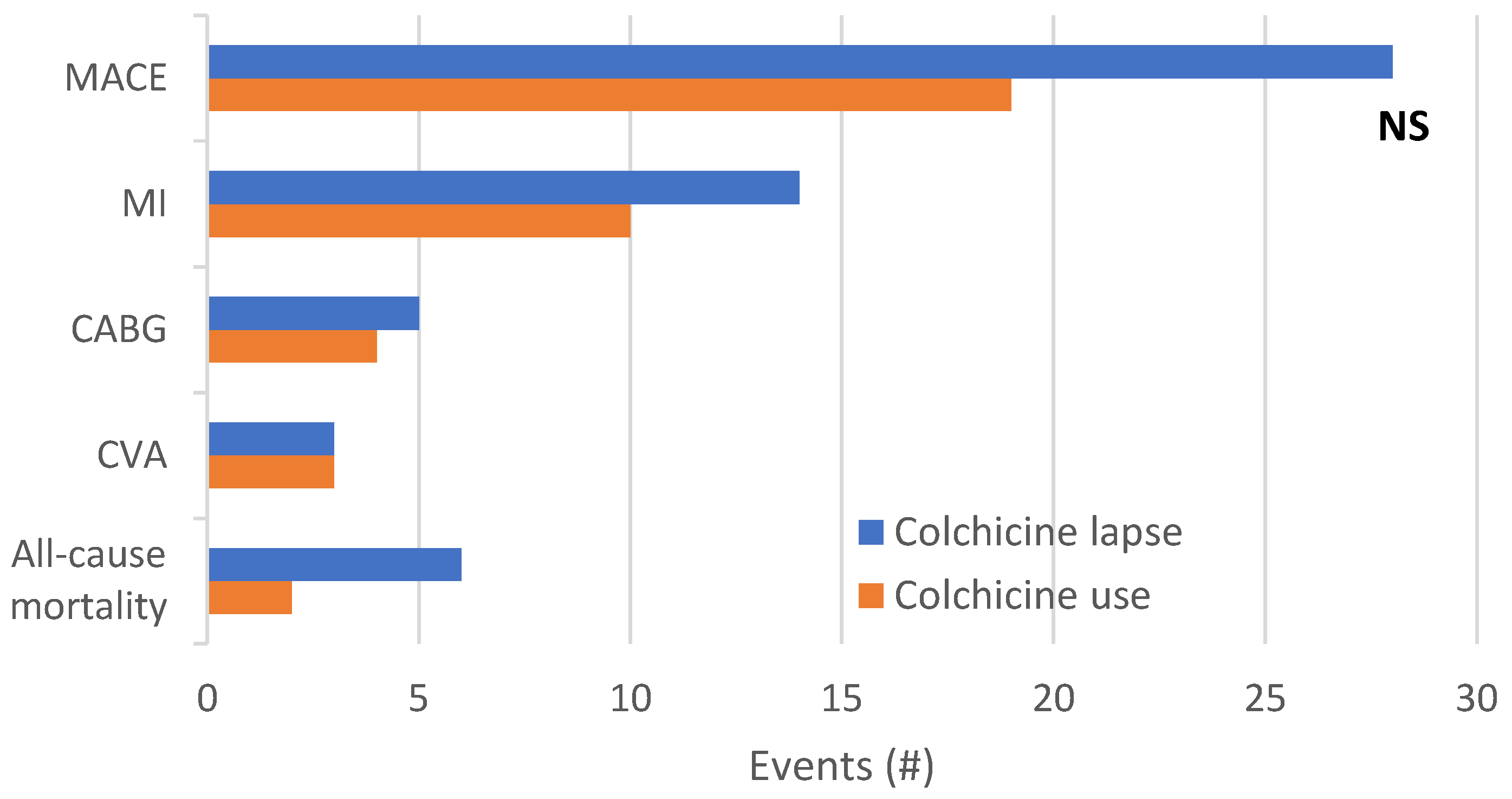
3.4. Exploratory Outcome: Major Adverse Cardiovascular Events during Active Colchicine Use versus Lapse
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Singh, G.; Lingala, B.; Mithal, A. Gout and hyperuricaemia in the USA: Prevalence and trends. Rheumatology 2019, 58, 2177–2180. [Google Scholar] [CrossRef] [PubMed]
- Singh, J.A.; Gaffo, A. Gout epidemiology and comorbidities. Semin. Arthritis Rheum. 2020, 50, S11–S16. [Google Scholar] [CrossRef] [PubMed]
- Pagidipati, N.J.; Clare, R.M.; Keenan, R.T.; Chiswell, K.; Roe, M.T.; Hess, C.N. Association of Gout with Long-Term Cardiovascular Outcomes Among Patients with Obstructive Coronary Artery Disease. J. Am. Heart Assoc. 2018, 7, e009328. [Google Scholar] [CrossRef] [PubMed]
- Kienhorst, L.B.; van Lochem, E.; Kievit, W.; Dalbeth, N.; Merriman, M.E.; Phipps-Green, A.; Loof, A.; van Heerde, W.; Vermeulen, S.; Stamp, L.K.; et al. Gout Is a Chronic Inflammatory Disease in Which High Levels of Interleukin-8 (CXCL8), Myeloid-Related Protein 8/Myeloid-Related Protein 14 Complex, and an Altered Proteome Are Associated with Diabetes Mellitus and Cardiovascular Disease. Arthritis Rheumatol. 2015, 67, 3303–3313. [Google Scholar] [CrossRef] [Green Version]
- Hansildaar, R.; Vedder, D.; Baniaamam, M.; Tausche, A.K.; Gerritsen, M.; Nurmohamed, M.T. Cardiovascular risk in inflammatory arthritis: Rheumatoid arthritis and gout. Lancet Rheumatol. 2021, 3, e58–e70. [Google Scholar] [CrossRef]
- FitzGerald, J.D.; Dalbeth, N.; Mikuls, T.; Brignardello-Petersen, R.; Guyatt, G.; Abeles, A.M.; Gelber, A.C.; Harrold, L.R.; Khanna, D.; King, C.; et al. 2020 American College of Rheumatology Guideline for the Management of Gout. Arthritis Care Res. 2020, 72, 744–760, Erratum in Arthritis Care Res. 2020, 72, 1187; Arthritis Care Res. 2021, 73, 458. [Google Scholar] [CrossRef]
- Tardif, J.C.; Kouz, S.; Waters, D.D.; Bertrand, O.F.; Diaz, R.; Maggioni, A.P.; Pinto, F.J.; Ibrahim, R.; Gamra, H.; Kiwan, G.S.; et al. Efficacy and Safety of Low-Dose Colchicine after Myocardial Infarction. N. Engl. J. Med. 2019, 381, 2497–2505. [Google Scholar] [CrossRef]
- Nidorf, S.M.; Fiolet, A.T.; Mosterd, A.; Eikelboom, J.W.; Schut, A.; Opstal, T.S.; The, S.H.; Xu, X.F.; Ireland, M.A.; Lenderink, T.; et al. Colchicine in Patients with Chronic Coronary Disease. N. Engl. J. Med. 2020, 383, 1838–1847. [Google Scholar] [CrossRef]
- Myinfla Product Information. Health Canada. Updated 3 November 2021. Available online: https://health-products.canada.ca/dpd-bdpp/dispatch-repartition.do (accessed on 1 February 2022).
- Robinson, P.C.; Terkeltaub, R.; Pillinger, M.H.; Shah, B.; Karalis, V.; Karatza, E.; Liew, D.; Imazio, M.; Cornel, J.H.; Thompson, P.L.; et al. Consensus Statement Regarding the Efficacy and Safety of Long-Term Low-Dose Colchicine in Gout and Cardiovascular Disease. Am. J. Med. 2022, 135, 32–38. [Google Scholar] [CrossRef]
- Ben-Chetrit, E.; Levy, M. Colchicine prophylaxis in familial Mediterranean fever: Reappraisal after 15 years. Semin. Arthritis Rheum. 1991, 20, 241–246. [Google Scholar] [CrossRef]
- Andreis, A.; Imazio, M.; Avondo, S.; Casula, M.; Paneva, E.; Piroli, F.; De Ferrari, G.M. Adverse events of colchicine for cardiovascular diseases: A comprehensive meta-analysis of 14,188 patients from 21 randomized controlled trials. J. Cardiovasc. Med. 2021, 22, 637–644. [Google Scholar] [CrossRef]
- Cronstein, B.N.; Molad, Y.; Reibman, J.; Balakhane, E.; Levin, R.I.; Weissmann, G. Colchicine alters the quantitative and qualitative display of selectins on endothelial cells and neutrophils. J. Clin. Investig. 1995, 96, 994–1002. [Google Scholar] [CrossRef]
- Asahina, A.; Tada, Y.; Nakamura, K.; Tamaki, K. Colchicine and griseofulvin inhibit VCAM-1 expression on human vascular endothelial cells—Evidence for the association of VCAM-1 expression with microtubules. J. Dermatol. Sci. 2001, 25, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Zhang, F.S.; He, Q.Z.; Qin, C.H.; Little, P.J.; Weng, J.P.; Xu, S.W. Therapeutic potential of colchicine in cardiovascular medicine: A pharmacological review. Acta Pharmacol. Sin. 2022, 43, 2173–2190. [Google Scholar] [CrossRef]
- Shah, B.; Allen, N.; Harchandani, B.; Pillinger, M.; Katz, S.; Sedlis, S.P.; Echagarruga, C.; Samuels, S.K.; Morina, P.; Singh, P.; et al. Effect of Colchicine on Platelet-Platelet and Platelet-Leukocyte Interactions: A Pilot Study in Healthy Subjects. Inflammation 2016, 39, 182–189, Erratum in Inflammation 2016, 39, 501. [Google Scholar] [CrossRef] [Green Version]
- Ridker, P.M.; Everett, B.M.; Thuren, T.; MacFayden, J.G.; Chang, W.H.; Ballantyne, C.; Fonseca, F.; Nicolau, J.; Koenig, W.; Anker, S.D.; et al. Antiinflammatory Therapy with Canakinumab for Atherosclerotic Disease. N. Engl. J. Med. 2017, 377, 1119–1131. [Google Scholar] [CrossRef]
- Shah, B.; Pillinger, M.; Zhong, H.; Cronstein, B.; Xia, Y.; Lorin, J.D.; Smilowitz, N.R.; Feit, F.; Ratnapala, N.; Keller, N.M.; et al. Effects of Acute Colchicine Administration Prior to Percutaneous Coronary Intervention: COLCHICINE-PCI Randomized Trial. Circ. Cardiovasc. Interv. 2020, 13, e008717. [Google Scholar] [CrossRef]
- Cole, J.; Htun, N.; Lew, R.; Freilich, M.; Quinn, S.; Layland, J. Colchicine to Prevent Periprocedural Myocardial Injury in Percutaneous Coronary Intervention: The COPE-PCI Pilot Trial. Circ. Cardiovasc. Interv. 2021, 14, e009992. [Google Scholar] [CrossRef]
- Crittenden, D.B.; Lehmann, R.A.; Schneck, L.; Keenan, R.T.; Shah, B.; Greenberg, J.D.; Cronstein, B.N.; Sedlis, S.P.; Pillinger, M.H. Colchicine use is associated with decreased prevalence of myocardial infarction in patients with gout. J. Rheumatol. 2012, 39, 1458–1464. [Google Scholar] [CrossRef] [Green Version]
- Solomon, D.H.; Liu, C.C.; Kuo, I.H.; Zak, A.; Kim, S.C. Effects of colchicine on risk of cardiovascular events and mortality among patients with gout: A cohort study using electronic medical records linked with Medicare claims. Ann. Rheum. Dis. 2016, 75, 1674–1679. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shah, B.; Toprover, M.; Crittenden, D.B.; Jeurling, S.; Pike, V.C.; Krasnokutsky, S.; Xia, Y.; Fisher, M.C.; Slobodnick, A.; Tenner, C.T.; et al. Colchicine Use and Incident Coronary Artery Disease in Male Patients with Gout. Can. J. Cardiol. 2020, 36, 1722–1728. [Google Scholar] [CrossRef] [PubMed]
- Souverein, P.C.; Berard, A.; Van Staa, T.P.; Cooper, C.; Egberts, A.C.; Leufkens, H.G.; Walker, B.R. Use of oral glucocorticoids and risk of cardiovascular and cerebrovascular disease in a population based case-control study. Heart 2004, 90, 859–865. [Google Scholar] [CrossRef] [Green Version]
- Bhala, N.; Emberson, J.; Merhi, A.; Abramson, S.; Arber, N.; Baron, J.A.; Bombardier, C.; Cannon, C.; Farkouh, M.E.; FitzGerald, G.A.; et al. Vascular and upper gastrointestinal effects of non-steroidal anti-inflammatory drugs: Meta-analyses of individual participant data from randomised trials. Lancet 2013, 382, 769–779. [Google Scholar]
- Toprover, M.; Shah, B.; Oh, C.; Igel, T.F.; Romero, A.G.; Pike, V.C.; Curovic, F.; Bang, D.; Lazaro, D.; Krasnokutsky, S.; et al. Initiating guideline-concordant gout treatment improves arterial endothelial function and reduces intercritical inflammation: A prospective observational study. Arthritis Res. Ther. 2020, 22, 169. [Google Scholar] [CrossRef]
- Xia, M.; Yang, X.; Qian, C. Meta-analysis Evaluating the Utility of Colchicine in Secondary Prevention of Coronary Artery Disease. Am. J. Cardiol. 2021, 140, 33–38. [Google Scholar] [CrossRef]
- Singh, J.A. Veterans Affairs databases are accurate for gout-related health care utilization: A validation study. Arthritis Res. Ther. 2013, 15, R224. [Google Scholar] [CrossRef] [Green Version]
- Ho, G.H.; Pillinger, M.H.; Toprover, M. Adherence to gout guidelines: Where do we stand? Curr. Opin. Rheumatol. 2021, 33, 128–134. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Nonusers (n = 116) | Colchicine Users (n = 239) | p Value |
|---|---|---|---|
| Age, years ± SD | 77 ± 10 | 78 ± 9 | 0.24 |
| Race | 0.16 | ||
| White | 64.0% | 55.6% | |
| Black | 26.1% | 34.9% | |
| Asian-Pacific Islander | 4.5% | 2.6% | |
| Ethnicity | 0.23 | ||
| Not Hispanic | 91.9% | 84.3% | |
| Hispanic | 6.3% | 10.6% | |
| Body mass index, kg/m2 ± SD | 31.4 ± 5.1 | 30.8 ± 4.3 | 0.62 |
| Diabetes mellitus | 37.1% | 42.7% | 0.30 |
| Hypertension | 89.7% | 87.9% | 0.58 |
| Systolic blood pressure, mmHg ± SD | 139 ± 21 | 131 ± 21 | <0.01 |
| Diastolic blood pressure, mmHg ± SD | 74 ± 13 | 74 ± 13 | 1.00 |
| Dyslipidemia | 65.5% | 76.2% | 0.07 |
| LDL cholesterol, mg/dL ± SD | 91 ± 31 | 102 ± 37 | 0.03 |
| Prior myocardial infarction | 34.5% | 45.6% | 0.04 |
| Prior coronary artery bypass graft | 31.0% | 28.0% | 0.62 |
| Prior percutaneous coronary intervention | 22.4% | 34.3% | 0.03 |
| Chronic kidney disease | 42.2% | 42.3% | 0.91 |
| Serum creatinine, mg/dL ± SD | 1.6 ± 1.2 | 1.6 ± 1.1 | 1.00 |
| Glomerular filtration rate, mL/min ± SD | 59 ± 21 | 54 ± 22 | 0.05 |
| History of tobacco use | 81.0% | 81.2% | 1.00 |
| Current tobacco use | 18.1% | 14.6% | 0.44 |
| Allopurinol use | 16.4% | 27.2% | 0.03 |
| Serum uric acid, mg/dL ± SD | 8.8 ± 2.4 | 8.7 ± 2.1 | 0.79 |
| NSAID use | 19.0% | 30.1% | 0.03 |
| Aspirin use | 50.0% | 59.8% | 0.11 |
| Statin use | 62.9% | 64.9% | 0.81 |
| ACE inhibitor use | 62.9% | 52.3% | 0.05 |
| β-blocker use | 62.9% | 71.1% | 0.18 |
| Any antihypertensive use | 69.8% | 66.1% | 0.47 |
| Mean daily colchicine dose, mg ± SD | 0.0 ± 0.0 | 0.71 ± 0.25 | – |
| Time on Colchicine, % of observation period ± SD | 0 ± 0 | 46.8 ± 29.8 | – |
| Variable | Quartiles 1–3 (n = 180) | Quartile 4 (n = 59) | p Value |
|---|---|---|---|
| Age, years ± SD | 78 ± 10 | 76 ± 9 | 0.17 |
| Race | 0.93 | ||
| White | 54.6% | 58.6% | |
| Black | 33.9% | 37.9% | |
| Asian-Pacific Islander | 2.3% | 3.4% | |
| Ethnicity | 0.81 | ||
| Not Hispanic | 83.1% | 88.1% | |
| Hispanic | 10.2% | 11.9% | |
| Body mass index, kg/m2 ± SD | 30.9 ± 5.8 | 31.0 ± 5.1 | 0.92 |
| Diabetes mellitus | 43.9% | 39.0% | 0.55 |
| Hypertension | 88.9% | 84.7% | 0.34 |
| Systolic blood pressure, mmHg ± SD | 132 ± 22 | 129 ± 20 | 0.43 |
| Diastolic blood pressure, mmHg ± SD | 74 ± 13 | 73 ± 12 | 0.40 |
| Dyslipidemia | 74.4% | 81.4% | 0.38 |
| LDL cholesterol, mg/dL ± SD | 104 ± 40 | 94 ± 26 | 0.37 |
| Prior myocardial infarction | 44.4% | 49.2% | 0.55 |
| Prior coronary artery bypass graft | 29.4% | 23.7% | 0.50 |
| Prior percutaneous coronary intervention | 33.9% | 35.6% | 0.75 |
| Chronic kidney disease | 41.7% | 44.1% | 0.76 |
| Serum creatinine, mg/dL ± SD | 1.6 ± 1.3 | 1.4 ± 0.5 | 0.88 |
| Glomerular filtration rate, mL/min ± SD | 53 ± 24 | 55 ± 18 | 0.76 |
| History of tobacco use | 81.1% | 81.4% | 1.00 |
| Current tobacco use | 13.3% | 18.6% | 0.40 |
| Allopurinol use | 30.0% | 18.6% | 0.09 |
| Serum uric acid, mg/dL ± SD | 8.6 ± 2.1 | 8.9 ± 2.0 | 0.50 |
| NSAID use | 32.2% | 23.7% | 0.25 |
| Aspirin use | 58.9% | 62.7% | 0.65 |
| Statin use | 61.7% | 74.6% | 0.08 |
| ACE inhibitor use | 51.1% | 55.9% | 0.55 |
| β-blocker use | 70.9% | 72.9% | 0.90 |
| Any antihypertensive use | 65.0% | 69.5% | 0.64 |
| Mean daily colchicine dose, mg ± SD | 0.72 ± 0.26 | 0.69 ± 0.22 | 0.43 |
| Time on colchicine, % of observation period ± SD | 33.1 ± 19.8 | 88.5 ± 9.9 | <0.01 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ho, G.H.; Toprover, M.; Crittenden, D.B.; Shah, B.; Pillinger, M.H. Colchicine Use and Major Adverse Cardiovascular Events in Male Patients with Gout and Established Coronary Artery Disease: A Veterans Affairs Nested Retrospective Cohort Study. Gout Urate Cryst. Depos. Dis. 2023, 1, 11-24. https://doi.org/10.3390/gucdd1010003
Ho GH, Toprover M, Crittenden DB, Shah B, Pillinger MH. Colchicine Use and Major Adverse Cardiovascular Events in Male Patients with Gout and Established Coronary Artery Disease: A Veterans Affairs Nested Retrospective Cohort Study. Gout, Urate, and Crystal Deposition Disease. 2023; 1(1):11-24. https://doi.org/10.3390/gucdd1010003
Chicago/Turabian StyleHo, Gary H., Michael Toprover, Daria B. Crittenden, Binita Shah, and Michael H. Pillinger. 2023. "Colchicine Use and Major Adverse Cardiovascular Events in Male Patients with Gout and Established Coronary Artery Disease: A Veterans Affairs Nested Retrospective Cohort Study" Gout, Urate, and Crystal Deposition Disease 1, no. 1: 11-24. https://doi.org/10.3390/gucdd1010003