
The Role of Sentinel Node Mapping and Lymphadenectomies in Veterinary Surgical Oncology

Abstract
:1. Introduction
2. Comparative Anatomy of the Canine and Human Lymphatic System
3. SLN Mapping in Companion Animals
3.1. Preoperative SLN Mapping Techniques Available in Veterinary Medicine
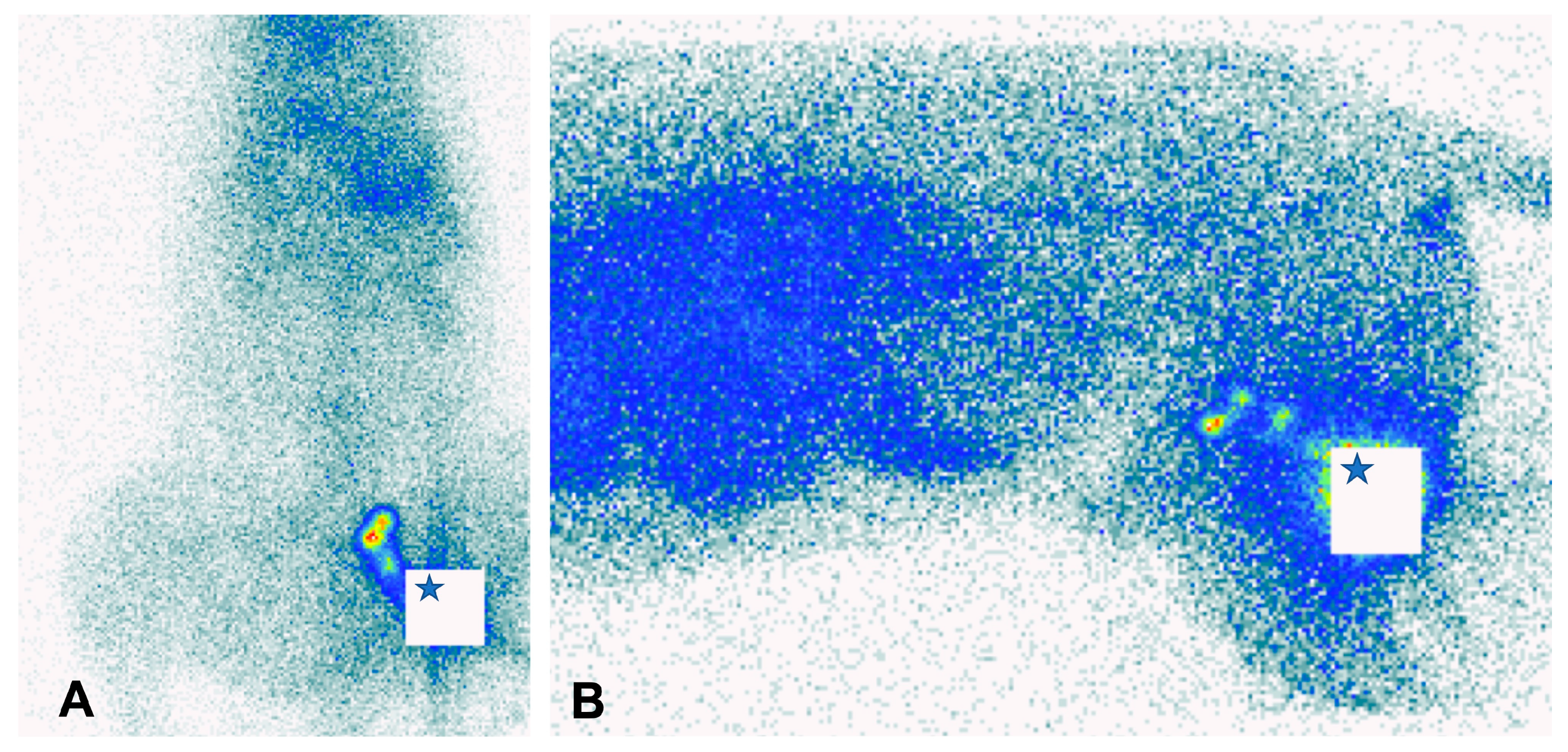
3.1.1. Lymphoscintigraphy
3.1.2. Indirect Radiographic Lymphography
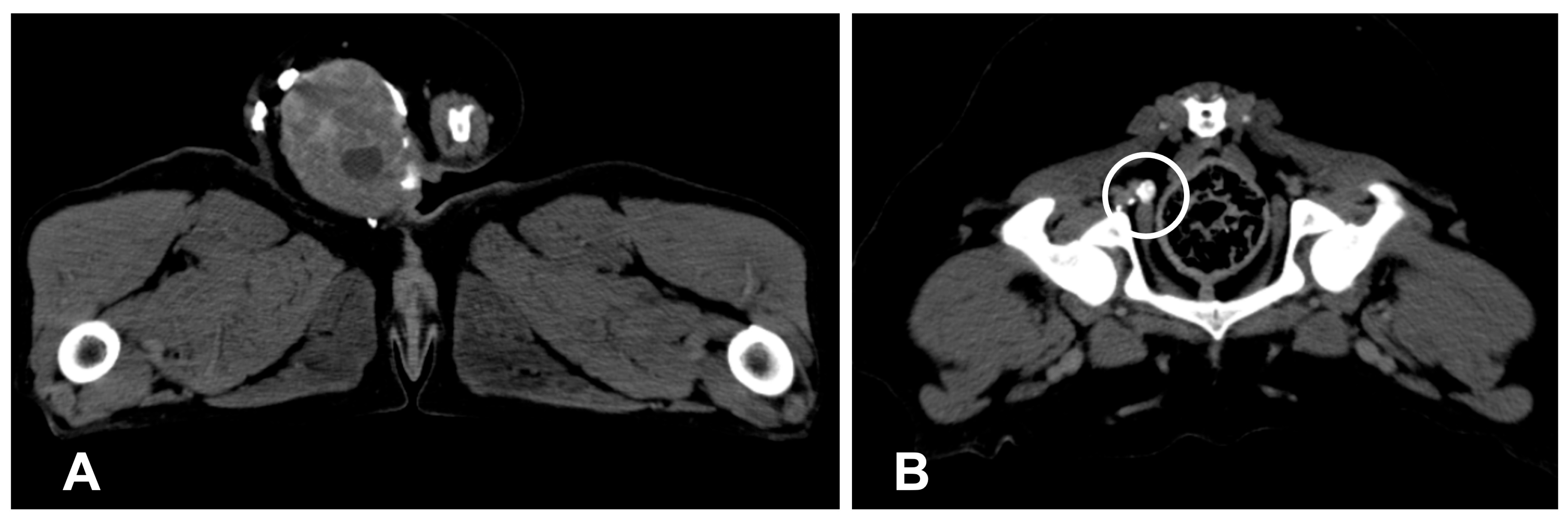
3.1.3. Computed Tomography Lymphography
3.1.4. Contrast-Enhanced Ultrasound (CEUS)
3.2. Intraoperative SLN Mapping Techniques
3.2.1. Colorimetric SLN Mapping Using Blue Dye
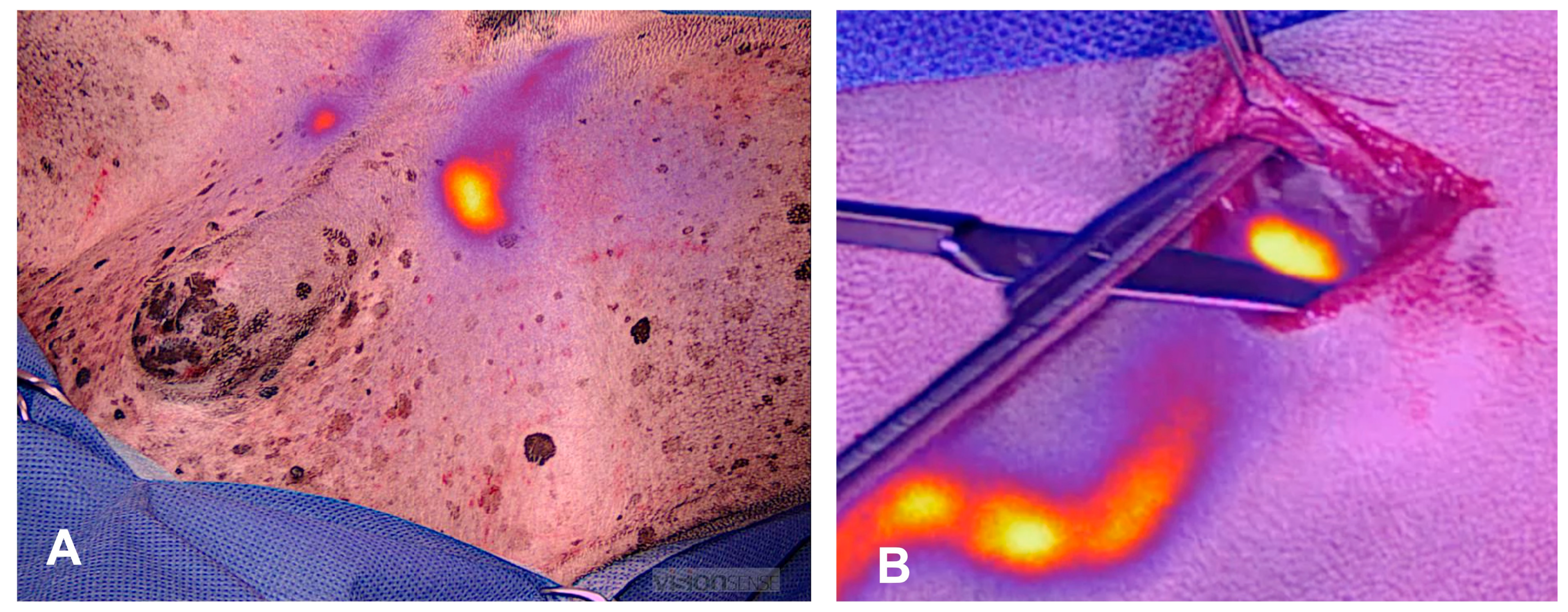
3.2.2. Near-Infrared Lymphography
4. Role of Lymphadenectomies and SLN Mapping in Selected Cancer Types in Dogs and Cats
4.1. Mammary Carcinoma
4.2. Apocrine Gland Anal Sac Adenocarcinoma (AGASAC)
4.3. Mast Cell Tumor
4.4. Cancers of the Head and Neck
5. Future Perspectives
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
List of Abbreviations
| AGASAC | Apocrine gland anal sac adenocarcinoma |
| CEUS | Contrast-enhanced ultrasound |
| CT | Computed tomography |
| END | Elective neck dissection |
| ICG | Indocyanine green |
| LN | Lymph node |
| MCT | Mast cell tumor |
| NIR | Near-infrared |
| NIR-L | Near-infrared fluorescent lymphography |
| RLN | Regional lymph node |
| SLN | Sentinel lymph node |
| Tc-99m | Technetium-99m |
References
- Liptak, J.M.; Boston, S.E. Nonselective Lymph Node Dissection and Sentinel Lymph Node Mapping and Biopsy. Vet. Clin. N. Am. Small Anim. Pract. 2019, 49, 793–807. [Google Scholar] [CrossRef] [PubMed]
- Beer, P.; Pozzi, A.; Rohrer Bley, C.; Bacon, N.; Pfammatter, N.S.; Venzin, C. The role of sentinel lymph node mapping in small animal veterinary medicine: A comparison with current approaches in human medicine. Vet. Comp. Oncol. 2018, 16, 178–187. [Google Scholar] [CrossRef] [PubMed]
- Chalfon, C.; Sabattini, S.; Finotello, R.; Faroni, E.; Guerra, D.; Pisoni, L.; Ciammaichella, L.; Vasconi, M.E.; Annoni, M.; Marconato, L. Lymphadenectomy improves outcome in dogs with resected Kiupel high-grade cutaneous mast cell tumours and overtly metastatic regional lymph nodes. J. Small Anim. Pract. 2022, 63, 661–669. [Google Scholar] [CrossRef]
- Marconato, L.; Polton, G.; Stefanello, D.; Morello, E.; Ferrari, R.; Henriques, J.; Tortorella, G.; Benali, S.L.; Bergottini, R.; Vasconi, M.E.; et al. Therapeutic impact of regional lymphadenectomy in canine stage II cutaneous mast cell tumours. Vet. Comp. Oncol. 2018, 16, 580–589. [Google Scholar] [CrossRef] [PubMed]
- Marconato, L.; Stefanello, D.; Kiupel, M.; Finotello, R.; Polton, G.; Massari, F.; Ferrari, R.; Agnoli, C.; Capitani, O.; Giudice, C.; et al. Adjuvant medical therapy provides no therapeutic benefit in the treatment of dogs with low-grade mast cell tumours and early nodal metastasis undergoing surgery. Vet. Comp. Oncol. 2020, 18, 409–415. [Google Scholar] [CrossRef] [PubMed]
- Mendez, S.E.; Drobatz, K.J.; Duda, L.E.; White, P.; Kubicek, L.; Sorenmo, K.U. Treating the locoregional lymph nodes with radiation and/or surgery significantly improves outcome in dogs with high-grade mast cell tumours. Vet. Comp. Oncol. 2020, 18, 239–246. [Google Scholar] [CrossRef]
- Halsted, W.S.I. The Results of Operations for the Cure of Cancer of the Breast Performed at the Johns Hopkins Hospital from June 1889, to January 1894. Ann. Surg. 1894, 20, 497–555. [Google Scholar] [CrossRef]
- Loukas, M.; Bellary, S.S.; Kuklinski, M.; Ferrauiola, J.; Yadav, A.; Shoja, M.M.; Shaffer, K.; Tubbs, R.S. The lymphatic system: A historical perspective. Clin. Anat. 2011, 24, 807–816. [Google Scholar] [CrossRef]
- Dogan, N.U.; Dogan, S.; Favero, G.; Kohler, C.; Dursun, P. The Basics of Sentinel Lymph Node Biopsy: Anatomical and Pathophysiological Considerations and Clinical Aspects. J. Oncol. 2019, 2019, 3415630. [Google Scholar] [CrossRef] [Green Version]
- Liptak, J.M. Histologic margins and the residual tumour classification scheme: Is it time to use a validated scheme in human oncology to standardise margin assessment in veterinary oncology? Vet. Comp. Oncol. 2020, 18, 25–35. [Google Scholar] [CrossRef]
- Barnes, D.C.; Demetriou, J.L. Surgical management of primary, metastatic and recurrent anal sac adenocarcinoma in the dog: 52 cases. J. Small Anim. Pract. 2017, 58, 263–268. [Google Scholar] [CrossRef] [PubMed]
- Repasy, A.B.; Selmic, L.E.; Kisseberth, W.C. Canine Apocrine Gland Anal Sac Adenocarcinoma: A Review. Top. Companion Anim. Med. 2022, 50, 100682. [Google Scholar] [CrossRef] [PubMed]
- Chiti, L.E.; Stefanello, D.; Manfredi, M.; Zani, D.D.; De Zani, D.; Boracchi, P.; Giudice, C.; Grieco, V.; Di Giancamillo, M.; Ferrari, R. To map or not to map the cN0 neck: Impact of sentinel lymph node biopsy in canine head and neck tumours. Vet. Comp. Oncol. 2021, 19, 661–670. [Google Scholar] [CrossRef] [PubMed]
- Beer, P.; Rohrer Bley, C.; Nolff, M.C. Near-infrared fluorescent image-guided lymph node dissection compared with locoregional lymphadenectomies in dogs with mast cell tumours. JSAP 2022, 63, 670–678. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, R.; Boracchi, P.; Chiti, L.E.; Manfredi, M.; Giudice, C.; De Zani, D.; Spediacci, C.; Recordati, C.; Grieco, V.; Gariboldi, E.M.; et al. Assessing the Risk of Nodal Metastases in Canine Integumentary Mast Cell Tumors: Is Sentinel Lymph Node Biopsy Always Necessary? Animals 2021, 11, 2373. [Google Scholar] [CrossRef]
- Haley, P.J. The lymphoid system: A review of species differences. J. Toxicol. Pathol. 2017, 30, 111–123. [Google Scholar] [CrossRef] [Green Version]
- Baum, H. Das Lymphgefäßsystem des Hundes; Hirschwald: Berlin, Germnay, 1918. [Google Scholar]
- Suami, H.; Yamashita, S.; Soto-Miranda, M.A.; Chang, D.W. Lymphatic territories (lymphosomes) in a canine: An animal model for investigation of postoperative lymphatic alterations. PLoS ONE 2013, 8, e69222. [Google Scholar] [CrossRef] [Green Version]
- Suami, H.; Shin, D.; Chang, D.W. Mapping of lymphosomes in the canine forelimb: Comparative anatomy between canines and humans. Plast. Reconstr. Surg. 2012, 129, 612–620. [Google Scholar] [CrossRef]
- Worley, D.R. Incorporation of sentinel lymph node mapping in dogs with mast cell tumours: 20 consecutive procedures. Vet. Comp. Oncol. 2014, 12, 215–226. [Google Scholar] [CrossRef]
- Linden, D.S.; Cole, R.; Tillson, D.M.; Boothe, H.W.; Matz, B.M. Sentinel lymph node mapping of the canine anal sac using lymphoscintigraphy: A pilot study. Vet. Radiol. Ultrasound Off. J. Am. Coll. Vet. Radiol. Int. Vet. Radiol. Assoc. 2019, 60, 346–350. [Google Scholar] [CrossRef]
- Skinner, O.T.; Boston, S.E.; Souza, C.H.M. Patterns of lymph node metastasis identified following bilateral mandibular and medial retropharyngeal lymphadenectomy in 31 dogs with malignancies of the head. Vet. Comp. Oncol. 2017, 15, 881–889. [Google Scholar] [CrossRef] [PubMed]
- Morton, D.L.; Wen, D.R.; Wong, J.H.; Economou, J.S.; Cagle, L.A.; Storm, F.K.; Foshag, L.J.; Cochran, A.J. Technical details of intraoperative lymphatic mapping for early-stage melanoma. Arch. Surg. 1992, 127, 392–399. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, R.; Chiti, L.E.; Manfredi, M.; Ravasio, G.; De Zani, D.; Zani, D.D.; Giudice, C.; Gambini, M.; Stefanello, D. Biopsy of sentinel lymph nodes after injection of methylene blue and lymphoscintigraphic guidance in 30 dogs with mast cell tumors. Vet. Surg. 2020, 49, 1099–1108. [Google Scholar] [CrossRef]
- Fournier, Q.; Thierry, F.; Longo, M.; Malbon, A.; Cazzini, P.; Bisson, J.; Woods, S.; Liuti, T.; Bavcar, S. Contrast-enhanced ultrasound for sentinel lymph node mapping in the routine staging of canine mast cell tumours: A feasibility study. Vet. Comp. Oncol. 2021, 19, 451–462. [Google Scholar] [CrossRef] [PubMed]
- Chiti, L.E.; Gariboldi, E.M.; Stefanello, D.; De Zani, D.; Grieco, V.; Nolff, M.C. Sentinel Lymph Node Mapping and Biopsy in Cats with Solid Malignancies: An Explorative Study. Animals 2022, 12, 3116. [Google Scholar] [CrossRef] [PubMed]
- Ashikaga, T.; Krag, D.N.; Land, S.R.; Julian, T.B.; Anderson, S.J.; Brown, A.M.; Skelly, J.M.; Harlow, S.P.; Weaver, D.L.; Mamounas, E.P.; et al. Morbidity results from the NSABP B-32 trial comparing sentinel lymph node dissection versus axillary dissection. J. Surg. Oncol. 2010, 102, 111–118. [Google Scholar] [CrossRef] [Green Version]
- Schrenk, P.; Rieger, R.; Shamiyeh, A.; Wayand, W. Morbidity following sentinel lymph node biopsy versus axillary lymph node dissection for patients with breast carcinoma. Cancer 2000, 88, 608–614. [Google Scholar] [CrossRef]
- Cabanas, R.M. An approach for the treatment of penile carcinoma. Cancer 1977, 39, 456–466. [Google Scholar] [CrossRef]
- Hayashi, H.; Tangoku, A.; Suga, K.; Shimizu, K.; Ueda, K.; Yoshino, S.; Abe, T.; Sato, T.; Matsunaga, N.; Oka, M. CT lymphography-navigated sentinel lymph node biopsy in patients with superficial esophageal cancer. Surgery 2006, 139, 224–235. [Google Scholar] [CrossRef]
- Motomura, K.; Sumino, H.; Noguchi, A.; Horinouchi, T.; Nakanishi, K. Sentinel nodes identified by computed tomography-lymphography accurately stage the axilla in patients with breast cancer. BMC Med. Imaging 2013, 13, 42. [Google Scholar] [CrossRef]
- Sever, A.; Jones, S.; Cox, K.; Weeks, J.; Mills, P.; Jones, P. Preoperative localization of sentinel lymph nodes using intradermal microbubbles and contrast-enhanced ultrasonography in patients with breast cancer. Br. J. Surg. 2009, 96, 1295–1299. [Google Scholar] [CrossRef] [PubMed]
- Naaman, Y.; Pinkas, L.; Roitman, S.; Ikher, S.; Oustinov, N.; Vaisbuch, E.; Yachnin, A.; Ben-Arie, A. The Added Value of SPECT/CT in Sentinel Lymph Nodes Mapping for Endometrial Carcinoma. Ann. Surg. Oncol. 2016, 23, 450–455. [Google Scholar] [CrossRef] [PubMed]
- Heusner, T.A.; Kuemmel, S.; Hahn, S.; Koeninger, A.; Otterbach, F.; Hamami, M.E.; Kimmig, K.R.; Forsting, M.; Bockisch, A.; Antoch, G.; et al. Diagnostic value of full-dose FDG PET/CT for axillary lymph node staging in breast cancer patients. Eur. J. Nucl. Med. Mol. Imaging 2009, 36, 1543–1550. [Google Scholar] [CrossRef] [PubMed]
- Jeremiasse, B.; van den Bosch, C.H.; Wijnen, M.; Terwisscha van Scheltinga, C.E.J.; Fiocco, M.F.; van der Steeg, A.F.W. Systematic review and meta-analysis concerning near-infrared imaging with fluorescent agents to identify the sentinel lymph node in oncology patients. Eur. J. Surg. Oncol. 2020, 46, 2011–2022. [Google Scholar] [CrossRef]
- Brissot, H.N.; Edery, E.G. Use of indirect lymphography to identify sentinel lymph node in dogs: A pilot study in 30 tumours. Vet. Comp. Oncol. 2016, 15, 740–753. [Google Scholar] [CrossRef]
- Hlusko, K.C.; Cole, R.; Tillson, D.M.; Boothe, H.W.; Almond, G.; Coggeshall, W.S.; Matz, B.M. Sentinel lymph node detection differs when comparing lymphoscintigraphy to lymphography using water soluble iodinated contrast medium and digital radiography in dogs. Vet. Radiol. Ultrasound 2020, 61, 659–666. [Google Scholar] [CrossRef]
- Mayer, M.N.; Silver, T.I.; Lowe, C.K.; Anthony, J.M. Radiographic lymphangiography in the dog using iodized oil. Vet. Comp. Oncol. 2013, 11, 151–161. [Google Scholar] [CrossRef]
- Grimes, J.A.; Secrest, S.A.; Northrup, N.C.; Saba, C.F.; Schmiedt, C.W. Indirect computed tomography lymphangiography with aqueous contrast for evaluation of sentinel lymph nodes in dogs with tumors of the head. Vet. Radiol. Ultrasound Off. J. Am. Coll. Vet. Radiol. Int. Vet. Radiol. Assoc. 2017, 58, 559–564. [Google Scholar] [CrossRef]
- Majeski, S.A.; Steffey, M.A.; Fuller, M.; Hunt, G.B.; Mayhew, P.D.; Pollard, R.E. Indirect Computed Tomographic Lymphography for Iliosacral Lymphatic Mapping in a Cohort of Dogs with Anal Sac Gland Adenocarcinoma: Technique Description. Vet. Radiol. Ultrasound Off. J. Am. Coll. Vet. Radiol. Int. Vet. Radiol. Assoc. 2017, 58, 295–303. [Google Scholar] [CrossRef]
- Rossi, F.; Korner, M.; Suarez, J.; Carozzi, G.; Meier, V.S.; Roos, M.; Rohrer Bley, C. Computed tomographic-lymphography as a complementary technique for lymph node staging in dogs with malignant tumors of various sites. Vet. Radiol. Ultrasound Off. J. Am. Coll. Vet. Radiol. Int. Vet. Radiol. Assoc. 2018, 59, 155–162. [Google Scholar] [CrossRef]
- Soultani, C.; Patsikas, M.N.; Karayannopoulou, M.; Jakovljevic, S.; Chryssogonidis, I.; Papazoglou, L.; Papaioannou, N.; Papadopoulou, P.; Pavlidou, K.; Ilia, G.M.; et al. Assessment of Sentinel Lymph Node Metastasis in Canine Mammary Gland Tumors Using Computed Tomographic Indirect Lymphography. Vet. Radiol. Ultrasound Off. J. Am. Coll. Vet. Radiol. Int. Vet. Radiol. Assoc. 2017, 58, 186–196. [Google Scholar] [CrossRef] [PubMed]
- Balogh, L.; Thuroczy, J.; Andocs, G.; Mathe, D.; Chaudhari, P.; Perge, E.; Biksi, I.; Polyak, A.; Kiraly, R.; Janoki, G.A. Sentinel lymph node detection in canine oncological patients. Nucl. Med. Rev. Cent. East. Eur. 2002, 5, 139–144. [Google Scholar] [PubMed]
- Pereira, C.T.; Luiz Navarro Marques, F.; Williams, J.; Wlademir De Martin, B.; Primo Bombonato, P. 99mTc-labeled dextran for mammary lymphoscintigraphy in dogs. Vet. Radiol. Ultrasound Off. J. Am. Coll. Vet. Radiol. Int. Vet. Radiol. Assoc. 2008, 49, 487–491. [Google Scholar] [CrossRef]
- Tuohy, J.L.; Worley, D.R. Pulmonary lymph node charting in normal dogs with blue dye and scintigraphic lymphatic mapping. Res. Vet. Sci. 2014, 97, 148–155. [Google Scholar] [CrossRef]
- Hlusko, K.C.; Cole, R.; Tillson, D.M.; Boothe, H.W.; Almond, G.T.; Coggeshall, W.S.; Matz, B.M. The effect of surgery on lymphoscintigraphy drainage patterns from the canine brachium in a simulated tumor model. Vet. Surg. 2020, 49, 1118–1124. [Google Scholar] [CrossRef]
- Wan, J.; Oblak, M.L.; Ram, A.; Singh, A.; Nykamp, S. Determining agreement between preoperative computed tomography lymphography and indocyanine green near infrared fluorescence intraoperative imaging for sentinel lymph node mapping in dogs with oral tumours. Vet. Comp. Oncol. 2021, 19, 295–303. [Google Scholar] [CrossRef]
- Lurie, D.M.; Seguin, B.; Schneider, P.D.; Verstraete, F.J.; Wisner, E.R. Contrast-assisted ultrasound for sentinel lymph node detection in spontaneously arising canine head and neck tumors. Investig. Radiol. 2006, 41, 415–421. [Google Scholar] [CrossRef] [PubMed]
- Gariboldi, E.M.; Stefanello, D.; Nolff, M.C.; De Zani, D.; Zani, D.; Grieco, V.; Giudice, C.; Recordati, C.; Ferrari, F.; Ferrari, R.; et al. Sentinel Lymph Node Biopsy Is Feasible in Dogs with Scars from Prior Local Excision of Solid Malignancies. Animals 2022, 12, 2195. [Google Scholar] [CrossRef] [PubMed]
- Knapp, D.W.; Adams, L.G.; Degrand, A.M.; Niles, J.D.; Ramos-Vara, J.A.; Weil, A.B.; O’Donnell, M.A.; Lucroy, M.D.; Frangioni, J.V. Sentinel lymph node mapping of invasive urinary bladder cancer in animal models using invisible light. Eur. Urol. 2007, 52, 1700–1708. [Google Scholar] [CrossRef] [Green Version]
- Townsend, K.L.; Milovancev, M.; Bracha, S. Feasibility of near-infrared fluorescence imaging for sentinel lymph node evaluation of the oral cavity in healthy dogs. Am. J. Vet. Res. 2018, 79, 995–1000. [Google Scholar] [CrossRef]
- Arz, R.; Seehusen, F.; Meier, V.S.; Nolff, M.C. Indocyanine-based near-infrared lymphography for real-time detection of lymphatics in a cat with multiple mast cell tumours. JFMS Open Rep. 2022, 8, 20551169221074961. [Google Scholar] [CrossRef]
- Niebling, M.G.; Pleijhuis, R.G.; Bastiaannet, E.; Brouwers, A.H.; van Dam, G.M.; Hoekstra, H.J. A systematic review and meta-analyses of sentinel lymph node identification in breast cancer and melanoma, a plea for tracer mapping. Eur. J. Surg. Oncol. 2016, 42, 466–473. [Google Scholar] [CrossRef] [PubMed]
- Manfredi, M.; De Zani, D.; Chiti, L.E.; Ferrari, R.; Stefanello, D.; Giudice, C.; Pettinato, V.; Longo, M.; Di Giancamillo, M.; Zani, D.D. Preoperative planar lymphoscintigraphy allows for sentinel lymph node detection in 51 dogs improving staging accuracy: Feasibility and pitfalls. Vet. Radiol. Ultrasound Off. J. Am. Coll. Vet. Radiol. Int. Vet. Radiol. Assoc. 2021, 62, 602–609. [Google Scholar] [CrossRef] [PubMed]
- Wawroschek, F.; Wengenmair, H.; Senekowitsch-Schmidtke, R.; Hamm, M.; Henke, J.; Schonberger, T.; Hauser, A.; Erhardt, W.; Harzmann, R. Prostate lymphoscintigraphy for sentinel lymph node identification in canines: Reproducibility, uptake, and biokinetics depending on different injection strategies. Urol. Res. 2003, 31, 152–158. [Google Scholar] [CrossRef] [PubMed]
- Alex, J.C.; Krag, D.N. Gamma-probe guided localization of lymph nodes. Surg. Oncol. 1993, 2, 137–143. [Google Scholar] [CrossRef]
- Patsikas, M.N.; Karayannopoulou, M.; Kaldrymidoy, E.; Papazoglou, L.G.; Papadopoulou, P.L.; Tzegas, S.I.; Tziris, N.E.; Kaitzis, D.G.; Dimitriadis, A.S.; Dessiris, A.K. The lymph drainage of the neoplastic mammary glands in the bitch: A lymphographic study. Anat. Histol. Embryol. 2006, 35, 228–234. [Google Scholar] [CrossRef]
- Papadopoulou, P.L.; Patsikas, M.N.; Charitanti, A.; Kazakos, G.M.; Papazoglou, L.G.; Karayannopoulou, M.; Chrisogonidis, I.; Tziris, N.; Dimitriadis, A. The lymph drainage pattern of the mammary glands in the cat: A lymphographic and computerized tomography lymphographic study. Anat. Histol. Embryol. 2009, 38, 292–299. [Google Scholar] [CrossRef] [PubMed]
- Collivignarelli, F.; Tamburro, R.; Aste, G.; Falerno, I.; Del Signore, F.; Simeoni, F.; Patsikas, M.; Gianfelici, J.; Terragni, R.; Attorri, V.; et al. Lymphatic Drainage Mapping with Indirect Lymphography for Canine Mammary Tumors. Animals 2021, 11, 115. [Google Scholar] [CrossRef] [PubMed]
- Patsikas, M.N.; Papadopoulou, P.L.; Charitanti, A.; Kazakos, G.M.; Soultani, C.B.; Tziris, N.E.; Tzegas, S.I.; Jakovljevic, S.; Savas, I.; Stamoulas, K.G. Computed tomography and radiographic indirect lymphography for visualization of mammary lymphatic vessels and the sentinel lymph node in normal cats. Vet. Radiol. Ultrasound Off. J. Am. Coll. Vet. Radiol. Int. Vet. Radiol. Assoc. 2010, 51, 299–304. [Google Scholar] [CrossRef]
- Randall, E.K.; Jones, M.D.; Kraft, S.L.; Worley, D.R. The development of an indirect computed tomography lymphography protocol for sentinel lymph node detection in head and neck cancer and comparison to other sentinel lymph node mapping techniques. Vet. Comp. Oncol. 2020, 18, 634–644. [Google Scholar] [CrossRef]
- Haers, H.; Saunders, J.H. Review of clinical characteristics and applications of contrast-enhanced ultrasonography in dogs. J. Am. Vet. Med. Assoc. 2009, 234, 460–470. [Google Scholar] [CrossRef] [PubMed]
- Seiler, G.S.; Brown, J.C.; Reetz, J.A.; Taeymans, O.; Bucknoff, M.; Rossi, F.; Ohlerth, S.; Alder, D.; Rademacher, N.; Drost, W.T.; et al. Safety of contrast-enhanced ultrasonography in dogs and cats: 488 cases (2002–2011). J. Am. Vet. Med. Assoc. 2013, 242, 1255–1259. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, B.B.; Merton, D.A.; Liu, J.B.; Murphy, G.; Forsberg, F. Contrast-enhanced sonographic imaging of lymphatic channels and sentinel lymph nodes. J. Ultrasound Med. 2005, 24, 953–965. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Cheng, Z.; Li, J.; Tang, J. Gray-scale contrast-enhanced ultrasonography in detecting sentinel lymph nodes: An animal study. Eur. J. Radiol. 2010, 74, e55–e59. [Google Scholar] [CrossRef]
- Wisner, E.R.; Ferrara, K.W.; Short, R.E.; Ottoboni, T.B.; Gabe, J.D.; Patel, D. Sentinel node detection using contrast-enhanced power Doppler ultrasound lymphography. Investig. Radiol. 2003, 38, 358–365. [Google Scholar] [CrossRef]
- Blomley, M.J.; Cooke, J.C.; Unger, E.C.; Monaghan, M.J.; Cosgrove, D.O. Microbubble contrast agents: A new era in ultrasound. BMJ 2001, 322, 1222–1225. [Google Scholar] [CrossRef] [PubMed]
- Sever, A.R.; Mills, P.; Jones, S.E.; Cox, K.; Weeks, J.; Fish, D.; Jones, P.A. Preoperative sentinel node identification with ultrasound using microbubbles in patients with breast cancer. AJR Am. J. Roentgenol. 2011, 196, 251–256. [Google Scholar] [CrossRef]
- Rossanese, M.; Pierini, A.; Pisani, G.; Freeman, A.; Burrow, R.; Booth, M.; Marchetti, V.; Finotello, R. Ultrasound-guided placement of an anchor wire or injection of methylene blue to aid in the intraoperative localization and excision of peripheral lymph nodes in dogs and cats. J. Am. Vet. Med. Assoc. 2021, 260, S75–S82. [Google Scholar] [CrossRef]
- Qiu, S.Q.; Zhang, G.J.; Jansen, L.; de Vries, J.; Schroder, C.P.; de Vries, E.G.E.; van Dam, G.M. Evolution in sentinel lymph node biopsy in breast cancer. Crit. Rev. Oncol. Hematol. 2018, 123, 83–94. [Google Scholar] [CrossRef]
- Troyan, S.L.; Kianzad, V.; Gibbs-Strauss, S.L.; Gioux, S.; Matsui, A.; Oketokoun, R.; Ngo, L.; Khamene, A.; Azar, F.; Frangioni, J.V. The FLARE intraoperative near-infrared fluorescence imaging system: A first-in-human clinical trial in breast cancer sentinel lymph node mapping. Ann. Surg. Oncol. 2009, 16, 2943–2952. [Google Scholar] [CrossRef]
- Schaafsma, B.E.; Mieog, J.S.; Hutteman, M.; van der Vorst, J.R.; Kuppen, P.J.; Lowik, C.W.; Frangioni, J.V.; van de Velde, C.J.; Vahrmeijer, A.L. The clinical use of indocyanine green as a near-infrared fluorescent contrast agent for image-guided oncologic surgery. J. Surg. Oncol. 2011, 104, 323–332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sevick-Muraca, E.M. Translation of near-infrared fluorescence imaging technologies: Emerging clinical applications. Annu. Rev. Med. 2012, 63, 217–231. [Google Scholar] [CrossRef] [PubMed]
- Fujisawa, Y.; Nakamura, Y.; Kawachi, Y.; Otsuka, F. Indocyanine green fluorescence-navigated sentinel node biopsy showed higher sensitivity than the radioisotope or blue dye method, which may help to reduce false-negative cases in skin cancer. J. Surg. Oncol. 2012, 106, 41–45. [Google Scholar] [CrossRef] [PubMed]
- Sugie, T.; Kinoshita, T.; Masuda, N.; Sawada, T.; Yamauchi, A.; Kuroi, K.; Taguchi, T.; Bando, H.; Yamashiro, H.; Lee, T.; et al. Evaluation of the Clinical Utility of the ICG Fluorescence Method Compared with the Radioisotope Method for Sentinel Lymph Node Biopsy in Breast Cancer. Ann. Surg. Oncol. 2016, 23, 44–50. [Google Scholar] [CrossRef] [PubMed]
- Jewell, E.L.; Huang, J.J.; Abu-Rustum, N.R.; Gardner, G.J.; Brown, C.L.; Sonoda, Y.; Barakat, R.R.; Levine, D.A.; Leitao, M.M., Jr. Detection of sentinel lymph nodes in minimally invasive surgery using indocyanine green and near-infrared fluorescence imaging for uterine and cervical malignancies. Gynecol. Oncol. 2014, 133, 274–277. [Google Scholar] [CrossRef] [Green Version]
- Van Heumen, S.; Riksen, J.J.M.; Bramer, W.M.; van Soest, G.; Vasilic, D. Imaging of the Lymphatic Vessels for Surgical Planning: A Systematic Review. Ann. Surg. Oncol. 2022, 2022, 1–18. [Google Scholar] [CrossRef]
- Hirche, C.; Murawa, D.; Mohr, Z.; Kneif, S.; Hunerbein, M. ICG fluorescence-guided sentinel node biopsy for axillary nodal staging in breast cancer. Breast Cancer Res. Treat. 2010, 121, 373–378. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.; Lee, S.K.; Kim, Y.M.; Lee, E.H.; Lim, S.J.; Kim, S.H.; Yang, J.; Lim, J.S.; Hyung, W.J. Fluorescent iodized emulsion for pre- and intraoperative sentinel lymph node imaging: Validation in a preclinical model. Radiology 2015, 275, 196–204. [Google Scholar] [CrossRef]
- Lapsley, J.; Hayes, G.M.; Janvier, V.; Newman, A.W.; Peters-Kennedy, J.; Balkman, C.; Sumner, J.P.; Johnson, P. Influence of locoregional lymph node aspiration cytology vs sentinel lymph node mapping and biopsy on disease stage assignment in dogs with integumentary mast cell tumors. Vet. Surg. 2021, 50, 133–141. [Google Scholar] [CrossRef]
- De Bonis, A.; Collivignarelli, F.; Paolini, A.; Falerno, I.; Rinaldi, V.; Tamburro, R.; Bianchi, A.; Terragni, R.; Gianfelici, J.; Frescura, P.; et al. Sentinel Lymph Node Mapping with Indirect Lymphangiography for Canine Mast Cell Tumour. Vet. Sci. 2022, 9, 484. [Google Scholar] [CrossRef]
- Stratmann, N.; Failing, K.; Richter, A.; Wehrend, A. Mammary tumor recurrence in bitches after regional mastectomy. Vet. Surg. 2008, 37, 82–86. [Google Scholar] [CrossRef]
- Polton, G.A.; Brearley, M.J. Clinical stage, therapy, and prognosis in canine anal sac gland carcinoma. J. Vet. Intern. Med. 2007, 21, 274–280. [Google Scholar] [CrossRef]
- Williams, L.E.; Gliatto, J.M.; Dodge, R.K.; Johnson, J.L.; Gamblin, R.M.; Thamm, D.H.; Lana, S.E.; Szymkowski, M.; Moore, A.S.; Veterinary Cooperative Oncology, G. Carcinoma of the apocrine glands of the anal sac in dogs: 113 cases (1985–1995). J. Am. Vet. Med. Assoc. 2003, 223, 825–831. [Google Scholar] [CrossRef] [PubMed]
- Wong, H.; Byrne, S.; Rasotto, R.; Drees, R.; Taylor, A.; Priestnall, S.L.; Leo, C. A Retrospective Study of Clinical and Histopathological Features of 81 Cases of Canine Apocrine Gland Adenocarcinoma of the Anal Sac: Independent Clinical and Histopathological Risk Factors Associated with Outcome. Animals 2021, 11, 3327. [Google Scholar] [CrossRef] [PubMed]
- Chambers, A.R.; Skinner, O.T.; Mickelson, M.A.; Schlag, A.N.; Butler, J.R.; Wallace, M.L.; Moyer, A.L.; Vinayak, A.; Samuel, N.; Kennedy, K.C.; et al. Adherence to follow-up recommendations for dogs with apocrine gland anal sac adenocarcinoma: A multicentre retrospective study. Vet. Comp. Oncol. 2020, 18, 683–688. [Google Scholar] [CrossRef] [PubMed]
- Graf, R.; Pospischil, A.; Guscetti, F.; Meier, D.; Welle, M.; Dettwiler, M. Cutaneous Tumors in Swiss Dogs: Retrospective Data from the Swiss Canine Cancer Registry, 2008–2013. Vet. Pathol. 2018, 55, 809–820. [Google Scholar] [CrossRef]
- Miller, M.A.; Nelson, S.L.; Turk, J.R.; Pace, L.W.; Brown, T.P.; Shaw, D.P.; Fischer, J.R.; Gosser, H.S. Cutaneous neoplasia in 340 cats. Vet. Pathol. 1991, 28, 389–395. [Google Scholar] [CrossRef] [Green Version]
- Sabattini, S.; Bettini, G. Grading Cutaneous Mast Cell Tumors in Cats. Vet. Pathol. 2019, 56, 43–49. [Google Scholar] [CrossRef]
- Fournier, Q.; Cazzini, P.; Bavcar, S.; Pecceu, E.; Ballber, C.; Elders, R. Investigation of the utility of lymph node fine-needle aspiration cytology for the staging of malignant solid tumors in dogs. Vet. Clin. Pathol. 2018, 47, 489–500. [Google Scholar] [CrossRef]
- Weishaar, K.M.; Thamm, D.H.; Worley, D.R.; Kamstock, D.A. Correlation of nodal mast cells with clinical outcome in dogs with mast cell tumour and a proposed classification system for the evaluation of node metastasis. J. Comp. Pathol. 2014, 151, 329–338. [Google Scholar] [CrossRef]
- Hume, C.T.; Kiupel, M.; Rigatti, L.; Shofer, F.S.; Skorupski, K.A.; Sorenmo, K.U. Outcomes of dogs with grade 3 mast cell tumors: 43 cases (1997–2007). J. Am. Anim. Hosp. Assoc. 2011, 47, 37–44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sabattini, S.; Kiupel, M.; Finotello, R.; Stefanello, D.; Faroni, E.; Bertazzolo, W.; Bonfanti, U.; Rigillo, A.; Del Magno, S.; Foglia, A.; et al. A retrospective study on prophylactic regional lymphadenectomy versus nodal observation only in the management of dogs with stage I, completely resected, low-grade cutaneous mast cell tumors. BMC Vet. Res. 2021, 17, 331. [Google Scholar] [CrossRef] [PubMed]
- Herring, E.S.; Smith, M.M.; Robertson, J.L. Lymph node staging of oral and maxillofacial neoplasms in 31 dogs and cats. J. Vet. Dent. 2002, 19, 122–126. [Google Scholar] [CrossRef] [PubMed]
- Rodrigo, J.P.; Grilli, G.; Shah, J.P.; Medina, J.E.; Robbins, K.T.; Takes, R.P.; Hamoir, M.; Kowalski, L.P.; Suarez, C.; Lopez, F.; et al. Selective neck dissection in surgically treated head and neck squamous cell carcinoma patients with a clinically positive neck: Systematic review. Eur. J. Surg. Oncol. 2018, 44, 395–403. [Google Scholar] [CrossRef]
- Congiusta, M.; Lawrence, J.; Rendahl, A.; Goldschmidt, S. Variability in Recommendations for Cervical Lymph Node Pathology for Staging of Canine Oral Neoplasia: A Survey Study. Front. Vet. Sci. 2020, 7, 506. [Google Scholar] [CrossRef]
- Ren, Z.H.; Xu, J.L.; Li, B.; Fan, T.F.; Ji, T.; Zhang, C.P. Elective versus therapeutic neck dissection in node-negative oral cancer: Evidence from five randomized controlled trials. Oral Oncol. 2015, 51, 976–981. [Google Scholar] [CrossRef]
- Costantino, A.; Canali, L.; Festa, B.M.; Spriano, G.; Mercante, G.; De Virgilio, A. Sentinel lymph node biopsy in high-risk cutaneous squamous cell carcinoma of the head and neck: Systematic review and meta-analysis. Head Neck 2022, 44, 2288–2300. [Google Scholar] [CrossRef]
- Den Toom, I.J.; Boeve, K.; Lobeek, D.; Bloemena, E.; Donswijk, M.L.; de Keizer, B.; Klop, W.M.C.; Leemans, C.R.; Willems, S.M.; Takes, R.P.; et al. Elective Neck Dissection or Sentinel Lymph Node Biopsy in Early Stage Oral Cavity Cancer Patients: The Dutch Experience. Cancers 2020, 12, 1783. [Google Scholar] [CrossRef]
- Smith, M.M. Surgical approach for lymph node staging of oral and maxillofacial neoplasms in dogs. J. Vet. Dent. 2002, 19, 170–174. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Study | Technique | Detection Rate | Tumor Type | Species |
|---|---|---|---|---|
| Balogh et al. 2002 [43] * | Lymphoscintigraphy | 89% | various | dog |
| Methylene Blue | 77% | |||
| Gamma probe and Methylene Blue | 97% | |||
| Brissot et al. 2016 [36] * | Radiographic lymphography | 96% | various | dog |
| Blue dye | 86% | |||
| Correspondence rate between techniques | 84% | |||
| Rossi et al. 2018 [41] | CT Lymphography | 60% | various | dog |
| Manfredi et al. 2021 [54] | Lymphoscintigraphy | 95% | various | dog |
| Chiti et al. 2022 [26] | Lymphoscintigraphy + gamma probe + Methylene Blue | 100% | various | cat |
| NIR Lymphography | 100% | |||
| Gariboldi et al. 2022 [49] | Lymphoscintigraphy and Methylene Blue | 87% | various scar revisions | dog |
| NIR Lymphography | 100% | |||
| Lurie et al. 2006 [48] | CEUS | 80% | head and neck | dog |
| Grimes et al. 2017 [39] | CT lymphography | 89% | head and neck | dog |
| Randall et al. 2020 [61] * | Lymphoscintigraphy | 100% | head and neck | dog |
| Methylene Blue | 94% | |||
| CT Lymphography | 55% | |||
| Wan et al. [47] | CT Lymphography | 42% | Head and neck (oral) | dog |
| Methylene Blue | 50% | |||
| NIR Lymphography | 91% | |||
| CT and Methylene Blue | 100% | |||
| Chiti et al. 2021 [13] | Lymphoscintigraphy | 83% | various head and neck | dog |
| Lurie et al. 2006 [48] | CEUS | 80% | head and neck | dog |
| Collivignarelli et al. 2021 [59] | Radiographic lymphography | 100% | mamma | dog |
| Majeski et al. 2017 [40] | CT lymphography | 92% | AGASAC | dog |
| Worley et al. 2014 [20] * | Lymphoscintigraphy and Methylene Blue | 95% | MCT | dog |
| Gamma probe | 100% | |||
| Lapsley et al. 2020 [80] | CT Lymphography | 90% | MCT | dog |
| Ferrari et al. 2020 [24] | Lymphoscintigraphy and Methylene Blue | 91% | MCT | dog |
| Fournier et al. 2021 [25] | CEUS | 95% | MCT | dog |
| De Bonis et al. 2022 [81] | Radiographic lymphography | 90% | MCT | dog |
| Beer et al. 2022 [14] | NIR Lymphography | 100% | MCT | dog |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Beer, P.; Chiti, L.E.; Nolff, M.C. The Role of Sentinel Node Mapping and Lymphadenectomies in Veterinary Surgical Oncology. Lymphatics 2023, 1, 2-18. https://doi.org/10.3390/lymphatics1010002
Beer P, Chiti LE, Nolff MC. The Role of Sentinel Node Mapping and Lymphadenectomies in Veterinary Surgical Oncology. Lymphatics. 2023; 1(1):2-18. https://doi.org/10.3390/lymphatics1010002
Chicago/Turabian StyleBeer, Patricia, Lavinia E. Chiti, and Mirja C. Nolff. 2023. "The Role of Sentinel Node Mapping and Lymphadenectomies in Veterinary Surgical Oncology" Lymphatics 1, no. 1: 2-18. https://doi.org/10.3390/lymphatics1010002