

Arterial Stiffness in Patients with Sarcoidosis and Obstructive Sleep Apnea
by
 , , ,
, , ,
Maurice Roeder
1,*,
Noriane A. Sievi
1,
Stefan Malesevic
1,
Thomas Gaisl
1,
Daniel Franzen
1 and
Malcolm Kohler
1,2 1
Department of Pulmonology, University Hospital Zurich, Rämistrasse 100, 8091 Zurich, Switzerland
2
Center for Interdisciplinary Sleep Research, University of Zurich, Rämistrasse 71, 8006 Zurich, Switzerland
*
Author to whom correspondence should be addressed.
J. Vasc. Dis. 2023, 2(1), 165-176; https://doi.org/10.3390/jvd2010011
Submission received: 19 December 2022
/
Revised: 6 January 2023
/
Accepted: 11 January 2023
/
Published: 16 February 2023
(This article belongs to the Topic Diagnosis, Management, and Prognostic Assessment of Chronic Disease)
Abstract
:Background: Obstructive sleep apnea (OSA) and sarcoidosis have both been implied to be risk factors for increased arterial stiffness. However, it is unclear whether an elevated apnea–hypopnea index (AHI) in sarcoidosis patients increases arterial stiffness and thus the cardiovascular risk. Methods: We performed non-invasive applanation tonometry in 57 adults with sarcoidosis. The participants underwent SphygmoCor to assess arterial stiffness using an aortic augmentation index with a heart rate of 75/min (AIx) and level-3 respiratory polygraphy. An AHI of ≥5/h, ≥15/h, and ≥30/h defined mild, moderate, and severe OSA, respectively. Multivariate regression analysis was used to investigate the association between AIx and AHI, adjusted for prespecified risk factors for AIx. Results: 23 (40%) sarcoidosis patients had at least mild OSA (AHI ≥ 5), while 7 (12%) patients showed AHI ≥ 15/h. AHI was significantly associated with AIx (coef. (95%CI) of 0.31 (0.09/0.52), p = 0.006) even after adjustment for known risk factors of arterial stiffness. While severe OSA was positively associated with increased AIx, mild and moderate OSA were not associated with increased AIx after adjusting for known risk factors. Conclusions: Increased AHI is independently associated with increased arterial stiffness in sarcoidosis patients. Further investigations are needed to underline the association between OSA severity and the magnitude of arterial stiffness.
1. Introduction
Cardiovascular disease (CVD) is one of the leading causes of death worldwide. Beside traditional risk factors such as diabetes, hypertension, and smoking, chronic inflammation has increasingly been recognized as a non-traditional risk factor for CVD. Several studies have described an increased incidence of atherosclerosis and cardiovascular risk in patients with inflammatory diseases, such as ankylosing spondylitis, vasculitis, and sarcoidosis [1,2,3,4]. Sarcoidosis is a granulomatous disease of an unknown etiology that typically affects the lungs, but can involve virtually any other organ [5]. Beside lymphadenopathy and the formation of non-ceasing granulomas, systemic inflammation is a hallmark of the disease [6]. Non-invasive assessment techniques such as the measurement of arterial stiffness, endothelial function, and carotid-intima media thickness have been investigated to improve the early detection of vascular dysfunction before it becomes clinically overt in the form of cardiovascular events [7]. Arterial stiffness assessed by pulse wave velocity (PWV) and the augmentation index (AIx) is a strong predictor of cardiovascular events and all-cause mortality in the general population [8]. There is growing proof that patients with sarcoidosis might be at higher risk for endothelial dysfunction and increased arterial stiffness [9]. Higher AIx values have been described in sarcoidosis patients with ocular and cardiac sarcoidosis, thereby supporting the hypothesis that AIx not only predicts cardiovascular risk in sarcoidosis patients, but also extra pulmonary involvement [10]. Hence, the understanding of the pathomechansim of increased arterial stiffness in sarcoidosis is of great importance. While disease-specific risk factors such as increased inflammation cytokines, direct granulomatous involvement of the vessels, and medication side effects have been under intense investigation, little is known about the role of classical risk factors in the development of arterial stiffness in this patient group [9,11]. We recently described an increased prevalence of obstructive sleep apnea (OSA) in sarcoidosis patients [12]. OSA is considered to be an independent cardiovascular risk factor in the general population [13]. It is the most common form of sleep-related breathing disorder (SDB) and is characterized by repetitive breathing cessation due to narrowing of the upper airways. Kohler et al. [14] reported that even patients with minimally symptomatic OSA show endothelial dysfunction and increased arterial stiffness. Several potential mechanisms have been discussed in the literature. Aside from arterial wall shear stress caused by rising blood pressure during apneic events, the suppression of endothelial nitric oxide (NO) synthase (due to increased oxidative stress), increased endothelial cell apoptosis, increased levels of coagulation factors, and cholesterol might orchestrate endothelial dysfunction and increased arterial stiffness in OSA patients [15,16,17,18].
Whether OSA is associated with an additional increase in arterial stiffness in sarcoidosis patients has so far not been investigated. This information would be of great interest as therapeutic options such as continuous positive airway therapy (CPAP) might be able to reverse pathological vascular changes in OSA patients [19]. The intent of this study was to assess the association between the apnea–hypopnea index (AHI) and arterial stiffness in patients with sarcoidosis.
2. Materials and Methods
2.1. Study Design and Participants
This study was part of a prospective cross-sectional study at the University Hospital Zurich, which our group conducted to assess the prevalence of OSA in sarcoidosis patients. For this purpose, 71 adult patients with sarcoidosis were matched one-to-one to 71 adult controls according to sex, age, and Body mass index (BMI). The study procedures included structured interviews, level-3 respiratory polygraphy, and arterial tonometry in all sarcoidosis patients.
Sarcoidosis patients were recruited via (1) visits to the University Hospital Zurich and (2) the sarcoidosis database of the University Hospital Zurich. Only sarcoidosis patients diagnosed according to international American thoracic society (ATS)/European respiratory society (ERS)/World Association of Sarcoidosis and other Granulomatous Disorders (WASOG) guidelines were included [20]. All of the inclusion and exclusion criteria can be viewed in the supplemental material (supplemental material). The study was conducted in accordance with the declaration of Helsinki and all subjects gave written informed consent to participate. The Ethics Committee of the Canton of Zurich approved the study (BASEC-Nr 2019-01604) and the study was registered at www.ClinicalTrials.gov, NCT04156789 on 11 August 2019.
2.2. Measurements
2.2.1. Pulse Wave Analysis
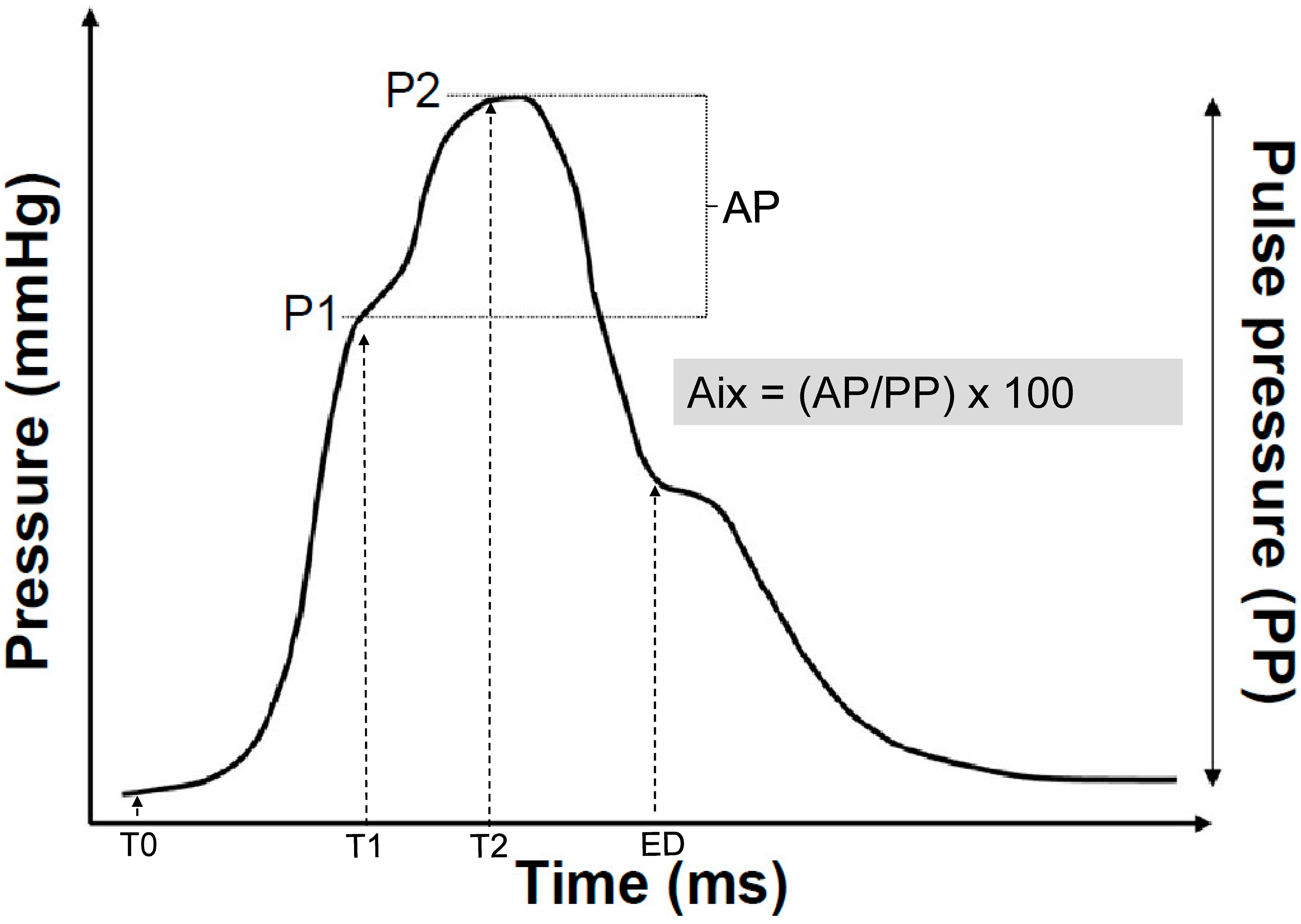
Subjects had to rest for 10 min in a supine position before the pulse wave analysis maneuver was performed. Afterwards, radial artery pulse waveforms were recorded using the SphygmoCor System (AtCor Medical, Sydney, NSW, Australia). Approximately 10 radial pulse waves were measured to generate a corresponding central aortic pressure waveform by using a validated mathematical transfer function [21]. The inflection point of the aortic pressure waveform was determined using an algorithm that divides the aortic pressure wave into an early and late systolic peak and corresponds to the onset of the reflected wave returning from the peripheral arteries (Figure 1).
The AIx quantifies the augmentation of the central aortic pressure, thereby representing a measure of the peripheral arterial wave reflection. AIx can be calculated as the difference between the second (P2) and the first systolic peak pressure (P1) and is expressed as a percentage of the central pulse pressure (PP):
AIx (%) = [(P2 − P1)/PP] × 100
As AIx is influenced by heart rate [22,23], the index is reported after being adjusted to a heart rate of 75 bpm, unless otherwise stated. SphygmoCor Px software adjusts the AIx at an inverse rate of 4.8% for each 10bpm increment. Only measurements with an operator index of 75 and above were accepted so as to ensure a high measurement quality.
2.2.2. Home-Based Sleep Study
Home sleep apnea testing (HSAT) was performed using the ApneaLinkTM Plus device (ResMed Corporation, Poway, Calif). This overnight respiratory polygraphy is a non-invasive medical examination technique, routinely applied to detect sleep-related breathing disorders. The study subjects were instructed in the usage of the device to install it on their own for the study night. The ApneaLinkTM Plus device records the nasal respiratory pressure signal as a surrogate of the nasal flow, respiratory movements by a thoracic impedance belt, and finger pulse oximetry. A blinded scorer, who was not involved in the organization and conduction of this study, scored the results of the sleep studies according to the current American Academy of Sleep Medicine (AASM) guidelines [24]. Apneas are defined as a cessation of airflow by ≥90% lasting >10 s, and hypopneas as a reduction in airflow of at least 30% lasting >10 s, associated with a drop in oxygen saturation of ≥3%. OSA severity was quantified as the number of apneas/hypopneas per hour (AHI) and oxygen desaturations ≥ 3% per hour (ODI) of sleep study. AHI thresholds according to the AASM Task Force of AHI ≥5, ≥15, and ≥30 were used to define mild, moderate, and severe OSA, respectively [25].
2.3. Data Analysis and Statistics
All data are presented as mean ± standard deviation (SD) or median (quartiles), unless otherwise stated. Multivariable regression analysis was used to investigate the association between AIx and AHI, adjusted for prespecified predictors for Aix, such as height, sex, current smoker, systolic blood pressure, antihypertensive drug, and corticosteroids. A residual analysis of the final model was performed to check the regression assumption. A two-sided p-value of <0.05 was considered to be statistically significant.
3. Results
3.1. Study Participants and Baseline Characteristics
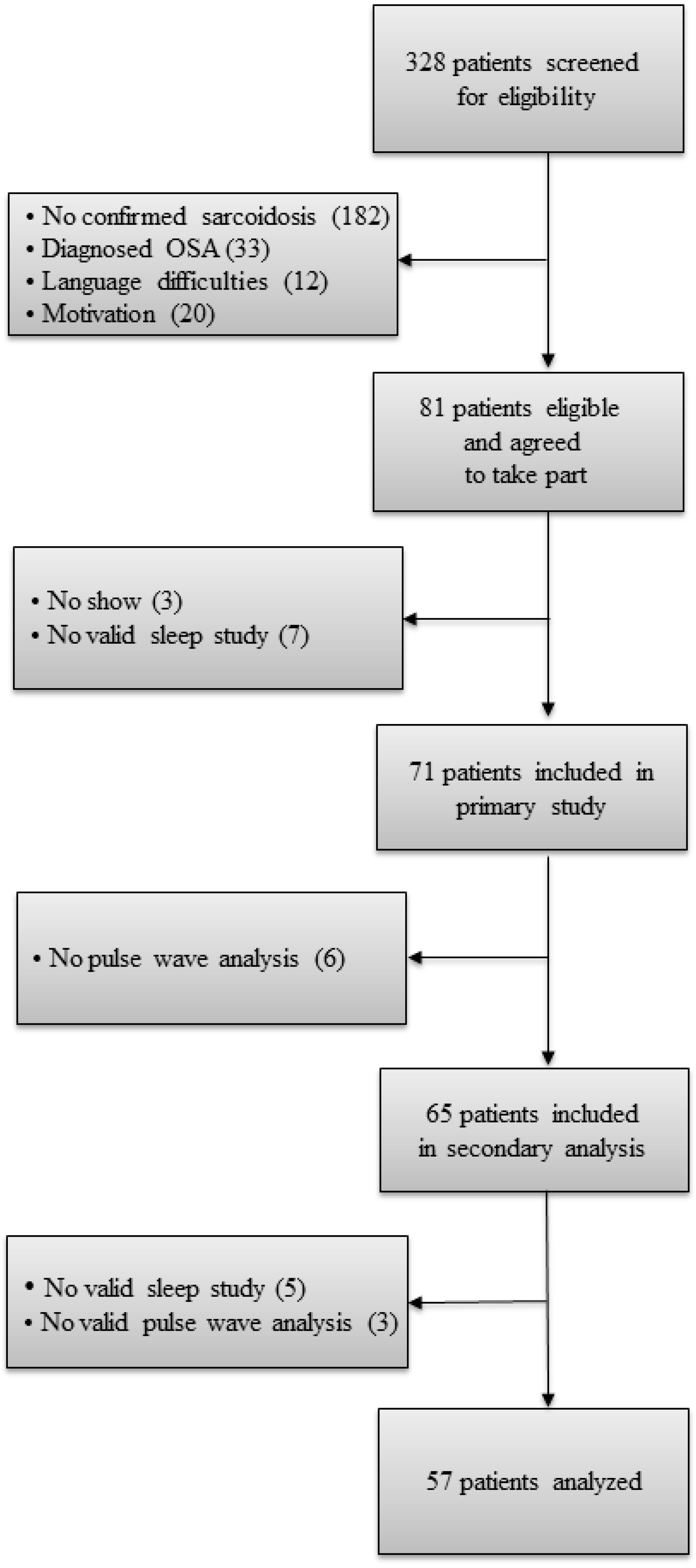
A total of 65 sarcoidosis patients underwent pulse wave analysis measurements. Because of an insufficient measurement quality, three sarcoidosis patients had to be excluded. Five sarcoidosis patients were excluded due to missing sleep studies. A total of 57 subjects entered the final analysis (Figure 2).
The mean (SD) age was 51 (11.9) years and 26 (46%) participants were female. Here, 11% of the sarcoidosis patients were current smokers. The detailed patients’ characteristics are shown in Table 1.
Serum inflammation markers (CRP, Soluble interleukin 2 receptor (sIL-2R) and neopterin) and angiotensin converting enzyme (ACE) were not elevated. The median (quartiles) AHI and ODI were 3.8 (1.2/7.5) events/h and 5.3 (1.7/13.4) events/h, respectively. Here, 23 (40%) sarcoidosis patients had at least mild OSA (AHI ≥ 5), while 7 (12%) patients showed an AHI ≥ 15/h.
3.2. Pulse Wave Analysis of Sarcoidosis Patients
The mean (SD) Aortic AIx was 20.5 (8.6)%. Further parameters for the pulse wave are shown in Table 2.
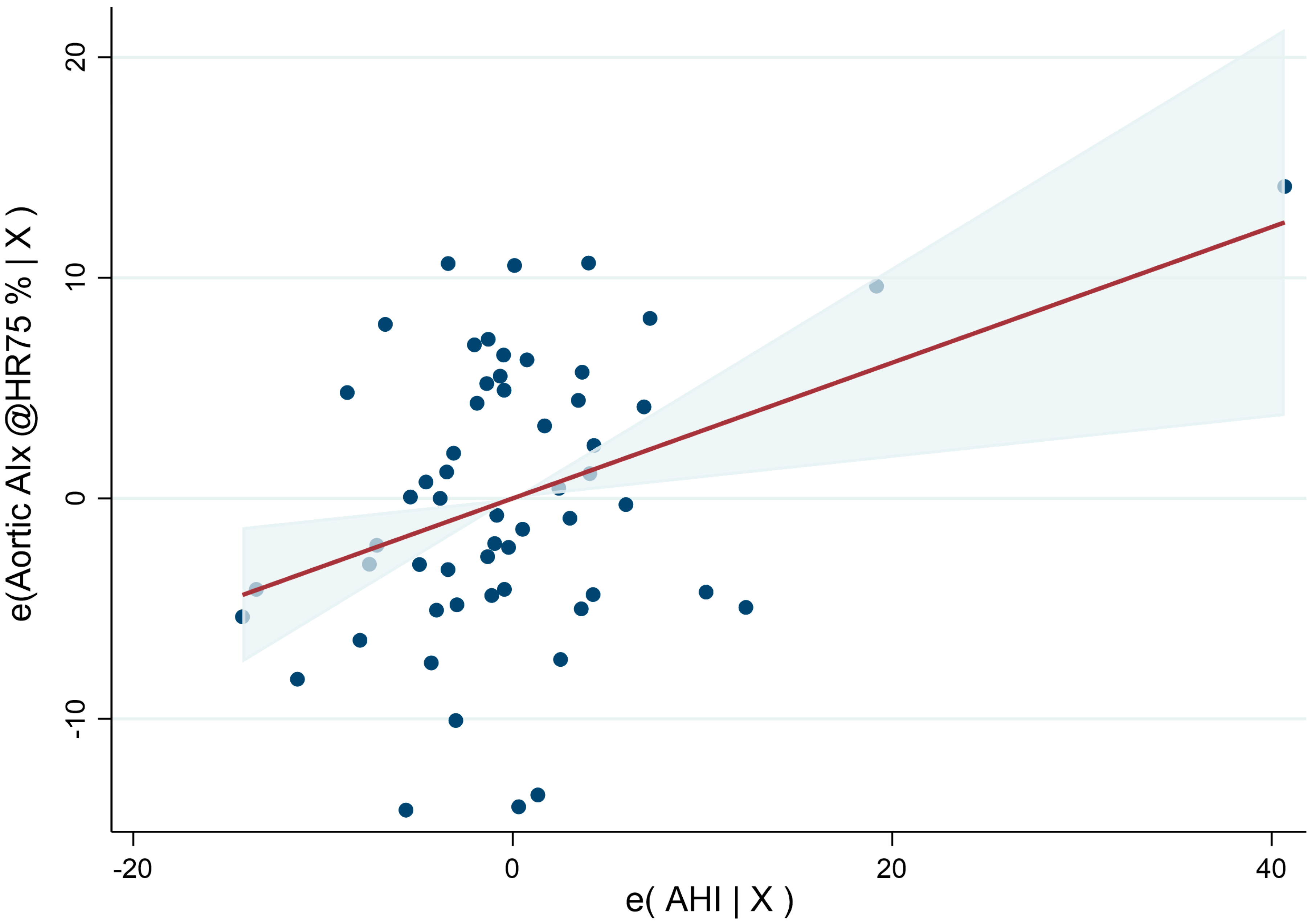
AHI was positively associated with a higher aortic AIx (coef. (95%CI) of 0.31 (0.09/0.52), p = 0.006) after adjusting for known modifying factors (age, sex, height, systolic blood pressure, current smoker, antihypertensive drugs, and steroids) (Figure 3 and Table 3).
Addressing the influence of OSA severity on AIx, severe OSA was independently associated with increased AIx (coef. (95%CI) of 16.04 (5.41/26.68), p = 0.004), while mild and moderate OSA showed no association with AIx (coef. (95%CI) of 0.21 (−4.22/4.36), p = 0.925, coef. (95%CI) of 3.83 (−3.38/11.05), p = 0.291) (Table 4). Sub-analyzing the influence of AHI ≥ 15 (n = 7) also revealed an independent influence on AIx (coef. (95%CI) of 7.31 (0.89/13.73), p = 0.026).
4. Discussion
This cross-sectional study investigated arterial stiffness in a well-characterized cohort of sarcoidosis patients with and without obstructive sleep apnea (OSA). We found that an increase in AHI was independently associated with increased arterial stiffness in sarcoidosis patients.
There is growing evidence that patients with sarcoidosis have a higher risk of cardiovascular disease (CVD). A population-based cohort study retrospectively assessed the medical records of 345 sarcoidosis patients and 1:1 sex- and age-matched controls without sarcoidosis between 1976 and 2013. They found significantly increased risk for cardiovascular endpoints including stroke, coronary artery disease congestive heart failure, atrial fibrillation, and cerebrovascular incidents, even after controlling for traditional cardiovascular risk factors [4]. Arterial stiffness and endothelial dysfunction play a central role in the initiation of atherosclerosis. The aortic AIx measured by the arterial tonometry is used as an indirect index of arterial stiffness derived from aortic pressure waveform analysis [26,27]. It represents the ratio of the ejection pressure from the heart and the reflection pressure from the arterial system (Figure 1). The augmentation index (AIx) has been shown to be an independent predictor of mortality and cardiovascular events in patients with hypertensive, cardiovascular, and renal disease in the general population [28]. Besides the prediction of cardiovascular risk, indirect measurement of arterial wall properties in sarcoidosis patients might even predict extra pulmonary involvement in sarcoidosis [10]. Saisos et al. described an increased augmentation index, increased pulse wave velocity (PWV), and reduced flow mediated dilation (FMD) in sarcoidosis patients with active disease. They reported even further deterioration of the endothelial function and arterial wall properties in sarcoidosis patients with ocular involvement, mainly uveitis, suggesting vascular dysfunction as a possible pathomechanism [10]. They reported FMD to be the strongest independent predictor for ocular involvement [10]. As a result, an understanding of increased arterial stiffness in sarcoidosis patients is of the utmost importance.
We found increased AIx values comparable to earlier studies investigating arterial stiffness in sarcoidosis patients [10]. There are several possible pathomechanisms discussed in the literature regarding increased arterial stiffness in sarcoidosis. Systemic inflammation might play a role, being a common feature of sarcoidosis and atherosclerosis [9,29,30]. Moreover, direct granulomatous involvement of the vessels and the infiltration of inflammation cells in the capillaries with consecutive microcirculatory disturbance have been described [11,31].
While sarcoidosis specific factors of arterial stiffness are under intensive investigation, there is little evidence regarding the effect of classical risk factors such as arterial hypertension, smoking status, or OSA in sarcoidosis patients. Our group found an increased prevalence of mild OSA in patients with sarcoidosis [12]. OSA is the most common form of sleep-related breathing disorder (SDB) and is characterized by repetitive breathing cessation due to narrowing of the upper airways. Endothelial dysfunction and increased arterial stiffness have been described in OSA, even in mildly symptomatic patients [14]. Our study suggests that increased respiratory event rates are associated with increased arterial stiffness in patients with sarcoidosis, even after adjusting for known modifying factors. While severe OSA was positively associated with increased AIx, mild and moderate OSA were not. This observation aligns with previous studies investigating the influence of OSA on arterial stiffness in the general population, showing a positive association between the severity of OSA and the magnitude of arterial stiffness [32]. Another reason for this observation might be shared pathomechanisms of both diseases leading to increased arterial stiffness. As a result, only severe forms of OSA might add an additional effect on the development of arterial stiffness. As such, increased arterial stiffness in OSA is considered to be a result of repetitive hypoxemia and reoxygenation resulting in oxidative stress and systemic inflammation [11]. Inflammation markers such as C-reactive protein, tumor necrosis factor-a, interleukin-6, and intercellular adhesion molecule-1 have been shown to be associated with arterial stiffness in sarcoidosis as well as in OSA patients [9,32]. It seems reasonable to assume that a lower number of apneas and hypopneas do not drive systemic inflammation to such an extent that it overrules sarcoidosis associated systemic inflammation. Oxidative stress not only triggers inflammation, but also reduces the activity of nitric oxide synthase and thus leads to a decreased production of nitric oxide increasing arterial stiffness [32]. Increased oxidative stress has also been described in patients with pulmonary sarcoidosis with even stable disease [33]. There might be no significant additional effect on the nitric oxide synthase in mild and moderate OSA. In addition, corticosteroids—the gold standard treatment of sarcoidosis—also reduce the function of nitric oxide synthetase, leading to reduced nitric oxide levels [34]. It seems noteworthy that one study showed decreased arterial stiffness in sarcoidosis patients receiving corticosteroids [9]. The authors emphasize the anti-inflammatory effect of corticosteroids inhibiting the release of inflammation mediators overruling negative medication associated vascular effects [9]. These findings were supported by studies showing preserved endothelial function in other inflammatory diseases such as Behçet’s disease treated with corticosteroids [35]. While corticosteroids might deteriorate OSA by increasing weight and oedema, the positive effect on the inflammation status might counteract the effect of oxidative stress triggered by OSA. Nevertheless, corticosteroids were not associated with an increased prevalence of OSA (not shown) nor with decreased arterial stiffness in our study. Furthermore, increased arterial stiffness in OSA is associated with a higher sympathetic activity, due to recurrent sleep fragmentation or intermittent hypoxia [19]. Measurements of single- and multi-unit muscle sympathetic nerve activity in OSA patients suggest a high sympathetic activity in patients with severe OSA, thereby supporting our finding of increased AIx in sarcoidosis patients with severe OSA. There is only limited evidence regarding autonomic dysfunction in sarcoidosis. A small prospective study with only 12 sarcoidosis patients and 12 healthy controls presented a reduced heart rate variability that might suggest reduced parasympathetic tone in sarcoidosis patients [36]. There are no data available connecting sympathetic activity and arterial stiffness in sarcoidosis patients so far. Both OSA and chronic inflammation are independently associated with insulin resistance [37,38]. Insulin resistance, measured by insulin resistance index based on the homeostasis model assessment method (HOMA-IR), was higher in patients with severe OSA compared with mild and moderate OSA [37].
The finding that increased AHI might lead to an additional increase in arterial stiffness in sarcoidosis patients is clinically relevant. First, sarcoidosis patients already have an increased cardiovascular risk, and untreated OSA might put sarcoidosis patients at even higher cardiovascular risk [4].
Second, once OSA is diagnosed, therapy options are available that could reduce cardiovascular risk in sarcoidosis patients. In 2019, the American College of Cardiology (ACC)/American Heart Association (AHA) Guideline for the Primary Prevention of cardiovascular disease named auto immune and inflammatory diseases a “risk enhancer”. The guidelines suggest statin initiation or intensification in primary prevention in those patients [39]. There is evidence that CPAP therapy might reverse endothelial dysfunction and thereby reduce cardiovascular risk in OSA patients [19]. Hence, sarcoidosis patients should be screened for OSA, particularly when they suffer increased daytime sleepiness or fatigue. It seems reasonable to assume that OSA treatment might improve the cardiovascular risk profile in sarcoidosis patients.
However, a recent meta-analysis pointed out that the majority of recent RCTs have failed to demonstrate convincing evidence for the benefits of CPAP on cardiovascular risk in the general population, except in patients with hypertension [40]. If CPAP therapy reduces endothelial dysfunction in sarcoidosis, patients should be evaluated in future randomized controlled trials.
There are some limitations to this study. Most of our sarcoidosis patients with OSA had only a mild form of the disease. Hence, the positive association found in severe OSA was based only on a few observations. Further investigations of arterial stiffness in sarcoidosis patients with severe OSA are needed to underline our results. Furthermore, there are several inflammation markers noted in the literature that are associated with increased arterial stiffness in OSA and sarcoidosis. We only investigated a limited amount of these markers due to the great number of included patients and limited resources.
5. Conclusions
This study showed evidence of an independent influence of increased AHI on arterial stiffness in sarcoidosis patients. These findings have important implications, given the importance of aortic stiffness for cardiovascular risk and the potential of therapeutic interventions such as CPAP therapy. These data underline the need for intensive screening efforts for OSA in sarcoidosis. Further studies should be conducted to confirm that severe OSA is an independent predictor of increased arterial stiffness in sarcoidosis.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/jvd2010011/s1, Section S1: Inclusion and Exclusion Criteria.
Author Contributions
Conceptualization, M.R., N.A.S., D.F. and M.K.; data curation, S.M. and T.G.; formal analysis, M.R., N.A.S., T.G. and M.K.; funding acquisition, M.R. and M.K.; investigation, M.R., N.A.S., S.M., T.G. and D.F.; methodology, N.A.S.; resources, M.R. and M.K.; supervision, M.R., D.F. and M.K.; writing—original draft, M.R.; writing—review and editing, N.A.S., S.M., T.G. and M.K. All authors have read and agreed to the published version of the manuscript.
Funding
The research was supported by grants from “Lunge Zürich, 2019-06”. Beside the financial support, the organization had no role in any study process.
Institutional Review Board Statement
All procedures were reviewed and approved by the Cantonal Ethics Committee Zurich (BASEC-Nr 2019-01604) and conformed to the Declaration of Helsinki.
Informed Consent Statement
All participants provided written informed consent to participate in the study.
Data Availability Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Conflicts of Interest
Malcolm Kohler reports grants and personal fees from Bayer, personal fees from Novartis, personal fees from Boehringer, personal fees from GSK, personal fees from Astra Zeneca, grants from Roche, personal fees from CSL Behring, and personal fees from Mundipharma, during the conduct of the study. The authors report no other conflicts of interest in this work. Thomas Gaisl reports personal fees from Bayer (outside the submitted work) during the conduct of this study.
Abbreviations
| AHI | Apnea-hypopnea index |
| AIx | Augmentation index |
| AP | Augmentation pressure |
| BMI | Body mass index |
| BP | Blood pressure |
| BSA | Body surface area |
| Coef. | Coefficient |
| CPAP | Continuous positive airway pressure |
| CVD | Cardiovascular disease |
| CRP | C-reactive protein |
| FMD | Flow mediated dilation |
| HR | Heart rate |
| IL-6 | interleukin-6 |
| Min | Minute |
| NSAID | Non-steroidal anti-inflammatory drug |
| OSA | Obstructive sleep apnea |
| ODI | Oxygen-desaturation index |
| PP | Pulse pressure |
| PWV | Pulse wave velocity |
| SD | Standard deviation |
| SDB | sleep-related breathing disorder |
| TNF-α | tumour necrosis factor-α |
References
- Sari, I.; Okan, T.; Akar, S.; Cece, H.; Altay, C.; Secil, M.; Birlik, M.; Onen, F.; Akkoc, N. Impaired endothelial function in patients with ankylosing spondylitis. Rheumatology 2006, 45, 283–286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Filer, A.D.; Gardner-Medwin, J.M.; Thambyrajah, J.; Raza, K.; Carruthers, D.M.; Stevens, R.J.; Liu, L.; Lowe, S.E.; Townend, J.N.; Bacon, P.A. Diffuse endothelial dysfunction is common to ANCA associated systemic vasculitis and polyarteritis nodosa. Ann. Rheum. Dis. 2003, 62, 162–167. [Google Scholar] [CrossRef]
- Margos, P.N.; Moyssakis, I.E.; Tzioufas, A.G.; Zintzaras, E.; Moutsopoulos, H.M. Impaired elastic properties of ascending aorta in patients with giant cell arteritis. Ann. Rheum. Dis. 2005, 64, 253–256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ungprasert, P.; Crowson, C.S.; Matteson, E.L. Risk of cardiovascular disease among patients with sarcoidosis: A population-based retrospective cohort study, 1976–2013. Eur. Respir. J. 2017, 49, 1601290. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Franzen, D.P.; Brutsche, M.; Nilsson, J.; Böni, C.; Daccord, C.; Distler, O.; Elsener, D.; Funke-Chambour, M.; Gruner, C.; Hayward-Könnecke, H.; et al. Sarcoidosis—A multisystem disease. Swiss Med. Wkly. 2022, 152, w30049. [Google Scholar] [CrossRef]
- Belperio, J.A.; Shaikh, F.; Abtin, F.G.; Fishbein, M.C.; Weigt, S.S.; Saggar, R.; Lynch, J.P., III. Diagnosis and Treatment of Pulmonary Sarcoidosis: A Review. JAMA 2022, 327, 856–867. [Google Scholar] [CrossRef]
- Vivodtzev, I.; Tamisier, R.; Baguet, J.P.; Borel, J.C.; Levy, P.; Pepin, J.L. Arterial stiffness in COPD. Chest 2014, 145, 861–875. [Google Scholar] [CrossRef]
- Vlachopoulos, C.; Aznaouridis, K.; Stefanadis, C. Prediction of cardiovascular events and all-cause mortality with arterial stiffness: A systematic review and meta-analysis. J. Am. Coll. Cardiol. 2010, 55, 1318–1327. [Google Scholar] [CrossRef] [Green Version]
- Siasos, G.; Tousoulis, D.; Gialafos, E.; Oikonomou, E.; Zaromitidou, M.; Aggeli, C.; Korompelis, P.; Kallianos, A.; Rapti, A.; Zisimos, K.; et al. Association of sarcoidosis with endothelial function, arterial wall properties, and biomarkers of inflammation. Am. J. Hypertens. 2011, 24, 647–653. [Google Scholar] [CrossRef] [Green Version]
- Siasos, G.; Paraskevopoulos, T.; Gialafos, E.; Rapti, A.; Oikonomou, E.; Zaromitidou, M.; Mourouzis, K.; Siasou, G.; Gouliopoulos, N.; Tsalamandris, S.; et al. Vascular function and ocular involvement in sarcoidosis. Microvasc. Res. 2015, 100, 54–58. [Google Scholar] [CrossRef]
- Takemura, T.; Shishiba, T.; Akiyama, O.; Oritsu, M.; Matsui, Y.; Eishi, Y. Vascular involvement in cutaneous sarcoidosis. Pathol. Int. 1997, 47, 84–89. [Google Scholar] [CrossRef] [PubMed]
- Roeder, M.; Sievi, N.A.; Schneider, A.; Osswald, M.; Malesevic, S.; Kolios, A.; Nilsson, J.; Kohler, M.; Franzen, D. The prevalence of obstructive sleep apnea in sarcoidosis and its impact on sleepiness, fatigue, and sleep-associated quality of life: A cross-sectional study with matched controls (the OSASA study). J. Clin. Sleep Med. 2022, 18, 2415–2422. [Google Scholar] [CrossRef] [PubMed]
- Yeghiazarians, Y.; Jneid, H.; Tietjens, J.R.; Redline, S.; Brown, D.L.; El-Sherif, N.; Mehra, R.; Bozkurt, B.; Ndumele, C.E.; Somers, V.K. Obstructive Sleep Apnea and Cardiovascular Disease: A Scientific Statement From the American Heart Association. Circulation 2021, 144, e56–e67. [Google Scholar] [CrossRef] [PubMed]
- Kohler, M.; Craig, S.; Nicoll, D.; Leeson, P.; Davies, R.J.; Stradling, J.R. Endothelial function and arterial stiffness in minimally symptomatic obstructive sleep apnea. Am. J. Respir. Crit. Care Med. 2008, 178, 984–988. [Google Scholar] [CrossRef] [PubMed]
- Gozal, D.; Kheirandish-Gozal, L. Cardiovascular morbidity in obstructive sleep apnea: Oxidative stress, inflammation, and much more. Am. J. Respir. Crit. Care Med. 2008, 177, 369–375. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Somers, V.K.; Dyken, M.E.; Clary, M.P.; Abboud, F.M. Sympathetic neural mechanisms in obstructive sleep apnea. J. Clin. Investig. 1995, 96, 1897–1904. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El Solh, A.A.; Akinnusi, M.E.; Baddoura, F.H.; Mankowski, C.R. Endothelial cell apoptosis in obstructive sleep apnea: A link to endothelial dysfunction. Am. J. Respir. Crit. Care Med. 2007, 175, 1186–1191. [Google Scholar] [CrossRef]
- Robinson, G.V.; Pepperell, J.C.; Segal, H.C.; Davies, R.J.; Stradling, J.R. Circulating cardiovascular risk factors in obstructive sleep apnoea: Data from randomised controlled trials. Thorax 2004, 59, 777–782. [Google Scholar] [CrossRef] [Green Version]
- Kohler, M.; Pepperell, J.C.T.; Casadei, B.; Craig, S.; Crosthwaite, N.; Stradling, J.R.; Davies, R.J.O. CPAP and measures of cardiovascular risk in males with OSAS. Eur. Respir. J. 2008, 32, 1488–1496. [Google Scholar] [CrossRef] [Green Version]
- Hunninghake, G.W.; Costabel, U.; Ando, M.; Baughman, R.; Cordier, J.F.; du Bois, R.; Eklund, A.; Kitaichi, M.; Lynch, J.; Rizzato, G.; et al. ATS/ERS/WASOG statement on sarcoidosis. American Thoracic Society/European Respiratory Society/World Association of Sarcoidosis and other Granulomatous Disorders. Sarcoidosis Vasc. Diffus. Lung Dis. Off. J. WASOG 1999, 16, 149–173. [Google Scholar]
- Pauca, A.L.; O’Rourke, M.F.; Kon, N.D. Prospective Evaluation of a Method for Estimating Ascending Aortic Pressure From the Radial Artery Pressure Waveform. Hypertension 2001, 38, 932–937. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilkinson, I.B.; MacCallum, H.; Flint, L.; Cockcroft, J.R.; Newby, D.E.; Webb, D.J. The influence of heart rate on augmentation index and central arterial pressure in humans. J. Physiol. 2000, 525 Pt 1, 263–270. [Google Scholar] [CrossRef] [PubMed]
- Wilkinson, I.B.; Mohammad, N.H.; Tyrrell, S.; Hall, I.R.; Webb, D.J.; Paul, V.E.; Levy, T.; Cockcroft, J.R. Heart rate dependency of pulse pressure amplification and arterial stiffness. Am. J. Hypertens. 2002, 15, 24–30. [Google Scholar] [CrossRef] [PubMed]
- Berry, R.B.; Budhiraja, R.; Gottlieb, D.J.; Gozal, D.; Iber, C.; Kapur, V.K.; Marcus, C.L.; Mehra, R.; Parthasarathy, S.; Quan, S.F.; et al. Rules for scoring respiratory events in sleep: Update of the 2007 AASM Manual for the Scoring of Sleep and Associated Events. Deliberations of the Sleep Apnea Definitions Task Force of the American Academy of Sleep Medicine. J. Clin. Sleep Med. 2012, 8, 597–619. [Google Scholar] [CrossRef] [Green Version]
- Kapur, V.K.; Auckley, D.H.; Chowdhuri, S.; Kuhlmann, D.C.; Mehra, R.; Ramar, K.; Harrod, C.G. Clinical Practice Guideline for Diagnostic Testing for Adult Obstructive Sleep Apnea: An American Academy of Sleep Medicine Clinical Practice Guideline. J. Clin. Sleep Med. 2017, 13, 479–504. [Google Scholar] [CrossRef]
- O’Rourke, M.F.; Mancia, G. Arterial stiffness. J. Hypertens. 1999, 17, 1065–1072. [Google Scholar] [CrossRef]
- O’Rourke, M.F.; Staessen, J.A.; Vlachopoulos, C.; Duprez, D.; Plante, G.E. Clinical applications of arterial stiffness; definitions and reference values. Am. J. Hypertens. 2002, 15, 426–444. [Google Scholar] [CrossRef]
- Laurent, S.; Cockcroft, J.; Van Bortel, L.; Boutouyrie, P.; Giannattasio, C.; Hayoz, D.; Pannier, B.; Vlachopoulos, C.; Wilkinson, I.; Struijker-Boudier, H. Expert consensus document on arterial stiffness: Methodological issues and clinical applications. Eur. Heart J. 2006, 27, 2588–2605. [Google Scholar] [CrossRef] [Green Version]
- Kaperonis, E.A.; Liapis, C.D.; Kakisis, J.D.; Dimitroulis, D.; Papavassiliou, V.G. Inflammation and atherosclerosis. Eur. J. Vasc. Endovasc. Surg. 2006, 31, 386–393. [Google Scholar] [CrossRef] [Green Version]
- Aciksari, G.; Kavas, M.; Atici, A.; Kul, S.; Erman, H.; Yilmaz, Y.; Demircioglu, K.; Yalcinkaya, E.; Kanbay, A.; Caliskan, M. Endocan Levels and Endothelial Dysfunction in Patients with Sarcoidosis. Angiology 2018, 69, 878–883. [Google Scholar] [CrossRef]
- Umazume, A.; Kezuka, T.; Okunuki, Y.; Ooshita, M.; Usui, Y.; Hirano, M.; Yamashina, A.; Goto, H. Prediction of severe cardiac involvement by fundus lesion in sarcoidosis. Jpn. J. Ophthalmol. 2014, 58, 81–85. [Google Scholar] [CrossRef] [PubMed]
- Doonan, R.J.; Scheffler, P.; Lalli, M.; Kimoff, R.J.; Petridou, E.T.; Daskalopoulos, M.E.; Daskalopoulou, S.S. Increased arterial stiffness in obstructive sleep apnea: A systematic review. Hypertens. Res. 2011, 34, 23–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koutsokera, A.; Papaioannou, A.I.; Malli, F.; Kiropoulos, T.S.; Katsabeki, A.; Kerenidi, T.; Gourgoulianis, K.I.; Daniil, Z.D. Systemic oxidative stress in patients with pulmonary sarcoidosis. Pulm. Pharmacol. Ther. 2009, 22, 603–607. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duckles, S.P.; Miller, V.M. Hormonal modulation of endothelial NO production. Pflügers Arch.-Eur. J. Physiol. 2010, 459, 841–851. [Google Scholar] [CrossRef] [Green Version]
- Protogerou, A.D.; Sfikakis, P.P.; Stamatelopoulos, K.S.; Papamichael, C.; Aznaouridis, K.; Karatzis, E.; Papaioannou, T.G.; Ikonomidis, I.; Kaklamanis, P.; Mavrikakis, M.; et al. Interrelated modulation of endothelial function in Behcet’s disease by clinical activity and corticosteroid treatment. Arthritis Res. Ther. 2007, 9, R90. [Google Scholar] [CrossRef] [Green Version]
- Hamaoka, T.; Murai, H.; Kaneko, S.; Usui, S.; Okabe, Y.; Tokuhisa, H.; Kato, T.; Furusho, H.; Sugiyama, Y.; Nakatsumi, Y.; et al. Single-Unit Muscle Sympathetic Nerve Activity Reflects Sleep Apnea Severity, Especially in Severe Obstructive Sleep Apnea Patients. Front. Physiol. 2016, 7, 66. [Google Scholar] [CrossRef] [Green Version]
- Ip, M.S.; Lam, B.; Ng, M.M.; Lam, W.K.; Tsang, K.W.; Lam, K.S. Obstructive sleep apnea is independently associated with insulin resistance. Am. J. Respir. Crit. Care Med. 2002, 165, 670–676. [Google Scholar] [CrossRef] [Green Version]
- Alfaddagh, A.; Martin, S.S.; Leucker, T.M.; Michos, E.D.; Blaha, M.J.; Lowenstein, C.J.; Jones, S.R.; Toth, P.P. Inflammation and cardiovascular disease: From mechanisms to therapeutics. Am. J. Prev. Cardiol. 2020, 4, 100130. [Google Scholar] [CrossRef]
- Arnett, D.K.; Blumenthal, R.S.; Albert, M.A.; Buroker, A.B.; Goldberger, Z.D.; Hahn, E.J.; Himmelfarb, C.D.; Khera, A.; Lloyd-Jones, D.; McEvoy, J.W.; et al. 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2019, 140, e596–e646. [Google Scholar] [CrossRef]
- Peker, Y.; Balcan, B. Cardiovascular outcomes of continuous positive airway pressure therapy for obstructive sleep apnea. J. Thorac. Dis. 2018, 10, S4262–S4279. [Google Scholar] [CrossRef] [Green Version]
Figure 1.
Schematic presentation of the pulse wave curve measured at the A. radialis. After the foot of the pulse (T0), indicating the onset of ejection, the pressure wave rises to an initial peak where it forms a shoulder (P1). This is the peak of the primary left ventricular ejection pressure. The second shoulder (P2) represents the peak of the arterial reflection wave. The difference between P2 and P1 is called augmentation pressure (AP). The end of ejection (ED) is the point of closure of the aortic valve and time of the end of systole. The augmentation index (AIx) is calculated as the difference between the second (P2) and first (P1) systolic peak pressure and is expressed as percentage of the central PP: AIx (%) = [(P2 − P1)/PP] × 100.
Figure 1.
Schematic presentation of the pulse wave curve measured at the A. radialis. After the foot of the pulse (T0), indicating the onset of ejection, the pressure wave rises to an initial peak where it forms a shoulder (P1). This is the peak of the primary left ventricular ejection pressure. The second shoulder (P2) represents the peak of the arterial reflection wave. The difference between P2 and P1 is called augmentation pressure (AP). The end of ejection (ED) is the point of closure of the aortic valve and time of the end of systole. The augmentation index (AIx) is calculated as the difference between the second (P2) and first (P1) systolic peak pressure and is expressed as percentage of the central PP: AIx (%) = [(P2 − P1)/PP] × 100.

Figure 2.
Study flow chart.

Figure 3.
Added-variable plot with a 95% confidence interval between the aortic augmentation index (AIx) and apnea–hypopnea index (AHI) to display the relationship between AIx and AHI in the multivariable regression model. A higher AHI is associated with a higher Aix, while the adjusted variables (age, sex, height, systolic blood pressure, smoker, antihypertensive drug, and steroids) remained constant (Coef. 0.31, p = 0.006).
Figure 3.
Added-variable plot with a 95% confidence interval between the aortic augmentation index (AIx) and apnea–hypopnea index (AHI) to display the relationship between AIx and AHI in the multivariable regression model. A higher AHI is associated with a higher Aix, while the adjusted variables (age, sex, height, systolic blood pressure, smoker, antihypertensive drug, and steroids) remained constant (Coef. 0.31, p = 0.006).


{kind=link}
{kind=link}
{kind=link}
Table 1.
Baseline characteristics.
| Total N = 57 | |
|---|---|
| Age, years | 51 (11.9) |
| Female/Male | 26/31 |
| Height, cm | 171.6 (9.2) |
| Weight, cm | 75.9 (14.1) |
| BMI, kg/m2 | 25.6 (3.6) |
| Pulmonary sarcoidosis, N (%) Scadding I, N (%) Scadding II, N (%) Scadding III, N (%) Scadding IV, N (%) Extrapulmonary sarcoidosis, N (%) Cardiac sarcoidosis, N (%) Ocular sarcoidosis, N (%) Cutaneous sarcoidosis, N (%) Current smoker, N (%) | 56 (98.2) 11 (19.3) 41 (71.9) 3 (5.3) 1 (1.8) 37 (64.9) 17 (29.8) 5 (8.8) 9 (15.8) 6 (11) |
| Pack years, N | 0 (0/9) |
| Blood pressure systolic (office), mmHg | 124 (17.6) |
| Blood pressure diastolic (office), mmHg | 82 (9.7) |
| Pulse, min−1 | 74 (11.7) |
| Arterial hypertension, N (%) | 7 (12) |
| Dyslipidemia, N (%) | 3 (5.3) |
| Diabetes, N (%) | 0 (0) |
| Coronary artery disease, N (%) | 3 (5.3) |
| Antihypertensive drugs, N (%) | 15 (26) |
| Corticosteroids, N (%) | 17 (29.8) |
| CRP, mg/L | 1.2 (0.6/2.3) |
| ACE, U/L | 41.1 (24.6/53.8) |
| Neopterin, ng/mL | 2.1 (1.6/2.9) |
| sIL-2R, pg/ml | 281.3 (211.9/382.1) |
| AHI, events/h | 3.8 (1.2/7.5) |
| ODI, events/h Mild OSA, N (%) Moderate OSA, N (%) Severe OSA, N (%) | 5.3 (1.7/13.4) 16 (28.1) 5 (8.8) 2 (3.5) |
BMI: body mass index; CRP: c-reactive protein; ACE: angiotensin converting enzyme; sIL-2R: soluble interleukin-2 receptor; AHI: apnea–hypopnea index; ODI: oxygen desaturation index; OSA: obstructive sleep apnea.
Table 2.
Pulse wave analysis parameters.
| Aortic AIx (AP/PP) @HR 75, %. | 20.5 (8.6) |
|---|---|
| P1 height, mmHg | 23 (20/27) |
| Aortic T1, ms | 113.1 (7.6) |
| Aortic T2, ms | 212.2 (22.8) |
| Peripheral AIx, % | 82.6 (13.8) |
| End systolic pressure, mmHg | 106.4 (12.4) |
| Ejection duration, ms | 293.9 (22.3) |
| Heart rate, min−1 | 71.9 (11.1) |
| Radial systolic pressure, mmHg | 123.3 (15.1) |
| Radial diastolic pressure, mmHg | 80.5 (9.1) |
Values are mean (SD) or median (quartiles). AIx: augmentation index; AP: augmented pressure; PP: pulse pressure; HR: heart rate; P1: first systolic peak pressure; T1: time to first peak; T2: time to second peak.
Table 3.
Multivariable linear regression analysis of aortic AIx (AP/PP) normalized for a heart rate of 75/min and AHI, adjusted for known risk factors.
Table 3.
Multivariable linear regression analysis of aortic AIx (AP/PP) normalized for a heart rate of 75/min and AHI, adjusted for known risk factors.
| Variable | Coefficient | 95% Confidence Interval | p-Value |
|---|---|---|---|
| AHI, events/h | 0.31 | 0.09/0.52 | 0.006 |
| Age, y | 0.10 | −0.09/0.29 | 0.314 |
| Male sex | −4.77 | −9.77/0.23 | 0.061 |
| Height, m | −0.42 | −0.67/−0.18 | 0.001 |
| Current smoker | 5.85 | −0.58/12.29 | 0.074 |
| Mean systolic blood pressure, mmHg | 0.16 | 0.03/0.28 | 0.014 |
| Antihypertensive drugs | 4.60 | −0.41/9.60 | 0.071 |
| Corticosteroids | −4.38 | −8.97/0.21 | 0.061 |
AIx: Augmentation index; AP: augmented pressure; PP: pulse pressure; AHI: apnea-hypopneaindex.
Table 4.
Multivariable linear regression analysis of the aortic AIx (AP/PP) normalized for a heart rate of 75/min and OSA severity groups, adjusted for known risk factors.
Table 4.
Multivariable linear regression analysis of the aortic AIx (AP/PP) normalized for a heart rate of 75/min and OSA severity groups, adjusted for known risk factors.
| Variable | Coefficient | 95% Confidence Interval | p-Value |
|---|---|---|---|
| OSA severity group (AHI < 5 as reference) | |||
| Mild (AHI ≥5–<15) | 0.21 | −4.22/4.63 | 0.925 |
| Moderate (AHI ≥15–<30) | 3.83 | −3.38/11.05 | 0.291 |
| Severe (AHI ≥ 30) | 16.04 | 5.41/26.68 | 0.004 |
| Age, y | 0.09 | −0.11/0.28 | 0.365 |
| Male sex | −4.24 | −9.48/0.99 | 0.110 |
| Height, m | −0.43 | −0.68/−0.18 | 0.001 |
| Current smoker | 4.87 | −1.83/11.57 | 0.150 |
| Mean systolic blood pressure, mmHg | 0.15 | 0.03/0.28 | 0.020 |
| Antihypertensive drugs | 5.00 | −0.10/10.04 | 0.055 |
| Corticosteroids | −4.94 | −10.09/0.21 | 0.060 |
OSA: obstructive sleep apnea; AIx: augmentation index; AP: augmented pressure; PP: pulse pressure; AHI: apnea-hypopnea index.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Roeder, M.; Sievi, N.A.; Malesevic, S.; Gaisl, T.; Franzen, D.; Kohler, M. Arterial Stiffness in Patients with Sarcoidosis and Obstructive Sleep Apnea. J. Vasc. Dis. 2023, 2, 165-176. https://doi.org/10.3390/jvd2010011
AMA Style
Roeder M, Sievi NA, Malesevic S, Gaisl T, Franzen D, Kohler M. Arterial Stiffness in Patients with Sarcoidosis and Obstructive Sleep Apnea. Journal of Vascular Diseases. 2023; 2(1):165-176. https://doi.org/10.3390/jvd2010011
Chicago/Turabian StyleRoeder, Maurice, Noriane A. Sievi, Stefan Malesevic, Thomas Gaisl, Daniel Franzen, and Malcolm Kohler. 2023. "Arterial Stiffness in Patients with Sarcoidosis and Obstructive Sleep Apnea" Journal of Vascular Diseases 2, no. 1: 165-176. https://doi.org/10.3390/jvd2010011