

Pulse Pressure Independent of Mean Arterial Pressure Is Associated with Cardiovascular and All-Cause Mortality in Normotensive Elders: Findings from National Health and Nutrition Examination Survey III 1999–2014
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants and Data Collection
2.2. Statistical Analysis
3. Results
3.1. The Baseline Characteristics of All Subjects
3.2. Associations between PP and Mortality in All Subjects
3.3. The Baseline Characteristics of the Study Subjects after PSM
3.4. Survival Analysis before and after PSM
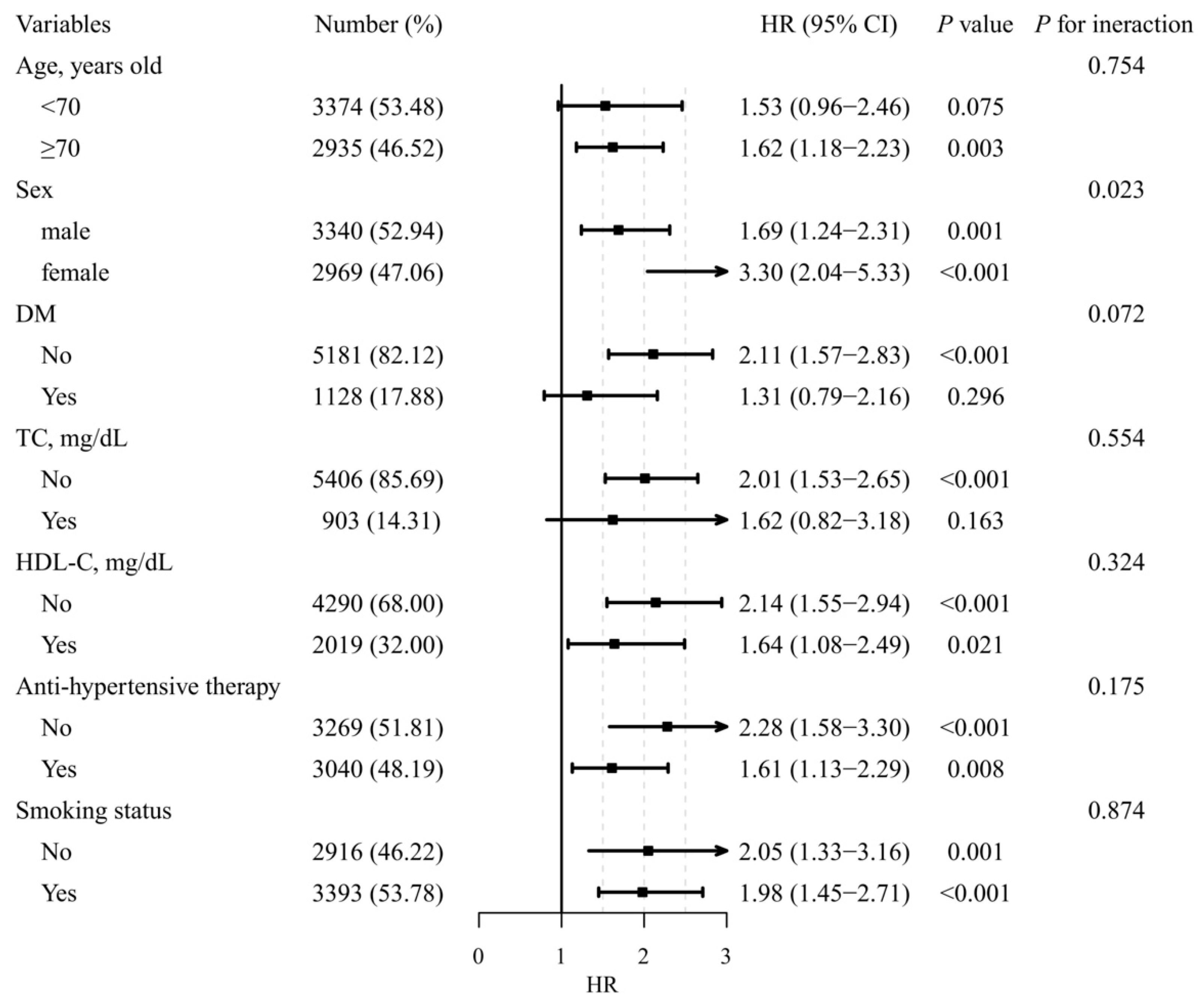
3.5. Subgroup Analysis Stratified by Traditional Cardiovascular Risk Factors
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Warren, J.; Nanayakkara, S.; Andrianopoulos, N.; Brennan, A.; Dinh, D.; Yudi, M.; Clark, D.; Ajani, A.E.; Reid, C.M.; Selkrig, L.; et al. Impact of Pre-Procedural Blood Pressure on Long-Term Outcomes Following Percutaneous Coronary Intervention. J. Am. Coll. Cardiol. 2019, 73, 2846–2855. [Google Scholar] [CrossRef] [PubMed]
- Georgakis, M.K.; Gill, D.; Malik, R.; Protogerou, A.D.; Webb, A.J.S.; Dichgans, M. Genetically Predicted Blood Pressure across the Lifespan: Differential Effects of Mean and Pulse Pressure on Stroke Risk. Hypertension 2020, 76, 953–961. [Google Scholar] [CrossRef] [PubMed]
- Vlachopoulos, C.; Aznaouridis, K.; O’Rourke, M.F.; Safar, M.E.; Baou, K.; Stefanadis, C. Prediction of cardiovascular events and all-cause mortality with central haemodynamics: A systematic review and meta-analysis. Eur. Heart J. 2010, 31, 1865–1871. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Melgarejo, J.D.; Thijs, L.; Wei, D.-M.; Bursztyn, M.; Yang, W.-Y.; Li, Y.; Asayama, K.; Hansen, T.W.; Kikuya, M.; Ohkubo, T.; et al. Relative and Absolute Risk to Guide the Management of Pulse Pressure, an Age-Related Cardiovascular Risk Factor. Am. J. Hypertens. 2021, 34, 929–938. [Google Scholar] [CrossRef] [PubMed]
- Pareek, M.; Vaduganathan, M.; Biering-Sørensen, T.; Byrne, C.; Qamar, A.; Almarzooq, Z.; Pandey, A.; Olsen, M.H.; Bhatt, D.L. Pulse Pressure, Cardiovascular Events, and Intensive Blood-Pressure Lowering in the Systolic Blood Pressure Intervention Trial (SPRINT). Am. J. Med. 2019, 132, 733–739. [Google Scholar] [CrossRef] [PubMed]
- Wei, H.; Hongwei, L.; Ying, S.; Dai, Z.; Man, W. The U-shape relationship between pulse pressure level on inpatient ad-mission and long-term mortality in acute coronary syndrome patients undergoing percutaneous coronary intervention. J. Clin. Hypertens. 2021, 24, 58–66. [Google Scholar] [CrossRef] [PubMed]
- Wei, F.-F.; Wu, Y.; Xue, R.; Liu, X.; He, X.; Dong, B.; Zhen, Z.; Chen, X.; Liang, W.; Zhao, J.; et al. Clinical Significance of Mean and Pulse Pressure in Patients with Heart Failure with Preserved Ejection Fraction. Hypertension 2022, 79, 241–250. [Google Scholar] [CrossRef] [PubMed]
- Selvaraj, S.; Steg, P.G.; Elbez, Y.; Sorbets, E.; Feldman, L.J.; Eagle, K.A.; Ohman, E.M.; Blacher, J.; Bhatt, D.L.; on behalf of the REACH Registry Investigators. Pulse Pressure and Risk for Cardiovascular Events in Patients with Atherothrombosis: From the REACH Registry. J. Am. Coll. Cardiol. 2016, 67, 392–403. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Darne, B.; Girerd, X.; Safar, M.; Cambien, F.; Guize, L. Pulsatile versus steady component of blood pressure: A cross-sectional analysis and a prospective analysis on cardiovascular mortality. Hypertension 1989, 13, 392–400. [Google Scholar] [CrossRef] [PubMed]
- Burt, V.L.; Whelton, P.; Roccella, E.J.; Brown, C.; Cutler, J.A.; Higgins, M.; Horan, M.J.; Labarthe, D. Prevalence of hypertension in the US adult population. Results from the Third National Health and Nutrition Examination Survey, 1988–1991. Hypertension 1995, 25, 305–313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chirinos, J.A.; Segers, P.; Hughes, T.; Townsend, R. Large-Artery Stiffness in Health and Disease: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2019, 74, 1237–1263. [Google Scholar] [CrossRef] [PubMed]
- Laurent, S.; Boutouyrie, P. Arterial Stiffness and Hypertension in the Elderly. Front. Cardiovasc. Med. 2020, 7, 544302. [Google Scholar] [CrossRef] [PubMed]
- Niiranen, T.J.; Kalesan, B.; Hamburg, N.M.; Benjamin, E.J.; Mitchell, G.F.; Vasan, R.S. Relative Contributions of Arterial Stiffness and Hypertension to Cardiovascular Disease: The Framingham Heart Study. J. Am. Heart Assoc. 2016, 5, e004271. [Google Scholar] [CrossRef] [PubMed]
- Webb, A.J.; Lawson, A.; Wartolowska, K.; Mazzucco, S.; Rothwell, P.M.; on behalf of the OXVASC Study Cohort. Aortic Stiffness, Pulse Pressure, and Cerebral Pulsatility Progress despite Best Medical Management: The OXVASC Cohort. Stroke 2022, 53, 1310–1317. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.-Y.; Meng, Q.; Yang, C.; Wang, Y.; Kong, G.; Zhao, Y.; Wang, F.; Zhang, L. Association between pulse pressure, systolic blood pressure and the risk of rapid decline of kidney function among general population without hypertension: Results from the China health and retirement longitudinal study (CHARLS). J. Transl. Med. 2021, 19, 512. [Google Scholar] [CrossRef] [PubMed]
- Jackson, C.E.; Castagno, D.; Maggioni, A.P.; Køber, L.; Squire, I.B.; Swedberg, K.; Andersson, B.; Richards, A.M.; Bayes-Genis, A.; Tribouilloy, C.; et al. Differing prognostic value of pulse pressure in patients with heart failure with reduced or preserved ejection fraction: Results from the MAGGIC individual patient meta-analysis. Eur. Heart J. 2015, 36, 1106–1114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laugesen, E.; Knudsen, S.T.; Hansen, K.W.; Rossen, N.B.; Jensen, L.O.; Hansen, M.S.; Andersen, L.K.; Thomsen, K.K.; Søndergaard, H.; Böttcher, M.; et al. Invasive aortic purvival Analysis Before and Afterflse pressure is not superior to cuff pulse pressure in cardiovascular risk prediction. J. Hypertens. 2020, 39, 607–613. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | Total n = 6309 | Normal PP n = 4294 | Widening PP n = 2015 | p-Value |
|---|---|---|---|---|
| Age, years | 69 (63, 75) | 67 (63, 73) | 73 (66, 80) | <0.001 |
| Male, n (%) | 3340 (52.9) | 2354 (54.8) | 986 (48.9) | <0.001 |
| BMI, Kg/m2 | 28.13 (24.95, 32.03) | 28.1 (25.00, 31.94) | 28.26 (24.90, 32.30) | 0.336 |
| DM, n (%) | 1128 (17.9) | 634 (14.8) | 494 (24.5) | <0.001 |
| TC ≥ 240 mg/dL, n (%) | 903 (14.3) | 658 (15.3) | 245 (12.2) | <0.001 |
| HDL-C < 40 mg/dL (male) or 50 mg/dL (female), n (%) | 2019 (32.0) | 1332 (31.0) | 687 (34.1) | 0.016 |
| Smoker, n (%) | 3393 (53.8) | 2326 (54.2) | 1067 (53.0) | 0.381 |
| Anti-hypertensive therapy, n (%) | 3040 (48.2) | 1896 (44.2) | 1144 (56.8) | <0.001 |
| PP, mmHg | 56.00 (47.33, 65.33) | 50.67 (44.00, 56.00) | 69.33 (65.33, 76.67) | <0.001 |
| MAP, mmHg | 85.56 (79.33, 91.11) | 86.67 (80.67, 92.44) | 82.89 (76.67, 88.22) | <0.001 |
| All-cause mortality, n (%) | 1391 (22.1) | 817 (19.0) | 574 (28.5) | <0.001 |
| Cardiovascular mortality, n (%) | 242 (3.8) | 135 (3.1) | 107 (5.3) | <0.001 |
| Median follow-up, months | 74 (42, 114) | 77 (44, 120) | 69 (39, 101) | <0.001 |
| Variable | Total n = 3710 | Normal PP n = 1855 | Widening PP n = 1855 | p-Value |
|---|---|---|---|---|
| Age, years | 72 (66, 78) | 72 (66, 78) | 72 (66, 78) | 0.940 |
| Male, n (%) | 1877 (50.6) | 932 (50.2) | 945 (50.9) | 0.695 |
| BMI, Kg/m2 | 28.20 (25.00, 32.20) | 28.16 (25.11, 32.09) | 28.28 (24.89, 32.34) | 0.969 |
| DM, n (%) | 792 (21.4) | 393 (21.2) | 399 (21.5) | 0.841 |
| TC ≥ 240 mg/dL, n (%) | 468 (12.6) | 239 (12.9) | 229 (12.4) | 0.656 |
| HDL-C < 40 mg/dL (male) or 50 mg/dL (female), n (%) | 1260 (34.0) | 628 (33.9) | 632 (34.1) | 0.917 |
| Smoker, n (%) | 1984 (53.5) | 984 (53.1) | 1000 (53.9) | 0.623 |
| Anti-hypertensive therapy, n (%) | 2047 (55.2) | 1023 (55.2) | 1024 (55.2) | 1.000 |
| PP, mmHg | 62.34 (52.00, 69.33) | 52.00 (46.00, 57.33) | 69.33 (65.33, 76.00) | <0.001 |
| MAP, mmHg | 84.22 (78.00, 89.78) | 85.56 (79.11, 91.33) | 83.11 (76.89, 88.44) | <0.001 |
| All-cause mortality, n (%) | 966 (26.0) | 461 (24.9) | 505 (27.2) | 0.108 |
| Cardiovascular mortality, n (%) | 163 (4.4) | 68 (3.7) | 95 (5.1) | 0.037 |
| Median follow-up, months | 71 (39, 105) | 73 (38, 107) | 70 (39, 101) | 0.124 |
| Variable | Before PSM | After PSM | ||
|---|---|---|---|---|
| Univariate | Multivariate | Univariate | Multivariate | |
| HR (95% CI) | HR (95% CI) | HR (95% CI) | HR (95% CI) | |
| Cardiovascular mortality | ||||
| Age, years | 1.09 (1.07–1.11) *** | 1.09 (1.07–1.11) *** | 1.09 (1.06–1.12) *** | 1.09 (1.06–1.11) *** |
| Male | 0.44 (0.33–0.58) *** | 0.48 (0.36–0.64) *** | 0.44 (0.32–0.61) *** | 0.53 (0.38–0.75) *** |
| BMI, Kg/m2 | 0.98 (0.96–1.01) | – | 0.99 (0.96–1.01) | – |
| DM | 1.75 (1.31–2.34) *** | 1.72 (1.28–2.31) *** | 1.29 (0.91–1.85) | – |
| TC ≥ 240 mg/dL | 0.91 (0.64–1.29) | – | 0.76 (0.47–1.23) | – |
| HDL-C < 40 mg/dL (male) or 50 mg/dL (female) | 1.22 (0.94–1.59) | – | 1.21 (0.89–1.66) | – |
| Smoker | 1.69 (1.30–2.21) *** | 1.52 (1.15–2.00) ** | 1.74 (1.26–2.40) *** | 1.55 (1.11–2.16) * |
| MAP, mmHg | 0.97 (0.96–0.98) *** | 0.99 (0.97–1.00) | 0.98 (0.97–1.00) * | 1.00 (0.98–1.01) |
| SBP, mmHg | 1.00 (0.99–1.01) | – | 1.00 (0.99–1.02) | – |
| Anti-hypertensive therapy | 1.38 (1.07–1.78) * | 1.25 (0.97–1.61) | 1.05 (0.77–1.43) | – |
| Widening PP | 1.96 (1.52–2.52) *** | 1.32 (1.01–1.74) * | 1.47 (1.07–2.00) * | 1.44 (1.05–1.98) * |
| All-cause mortality | ||||
| Age, y | 1.11 (1.10–1.12) *** | 1.11 (1.10–1.12) *** | 1.11 (1.10–1.12) *** | 1.11 (1.09–1.12) *** |
| Male | 0.62 (0.56–0.69) *** | 0.68 (0.60–0.76) *** | 0.57 (0.50–0.65) *** | 0.69 (0.60–0.79) *** |
| BMI, Kg/m2 | 0.97 (0.96–0.98) *** | 0.98 (0.97–1.00) ** | 0.97 (0.95–0.98) *** | 1.00 (0.98–1.01) |
| DM | 1.44 (1.26–1.63) *** | 1.54 (1.34–1.76) *** | 1.12 (0.96–1.30) | – |
| TC ≥ 240 mg/dL | 0.82 (0.70–0.95) ** | 1.05 (0.90–1.23) | 0.78 (0.64–0.95) * | 0.93 (0.76–1.13) |
| HDL-C < 40 mg/dL (male) or 50 mg/dL (female) | 1.13 (1.02–1.27) * | 1.23 (1.09–1.37) *** | 1.07 (0.93–1.22) | – |
| Smoker | 1.50 (1.35–1.68) *** | 1.47 (1.31–1.65) *** | 1.53 (1.34–1.74) *** | 1.44 (1.26–1.65) *** |
| MAP, mmHg | 0.97 (0.97–0.98) *** | 0.99 (0.98–0.99) *** | 0.98 (0.97–0.98) *** | 0.99 (0.98–1.00) ** |
| SBP, mmHg | 1.00 (1.00–1.00) | – | 0.99 (0.99–1.00) ** | 1.00 (0.99–1.01) |
| Anti-hypertensive therapy | 1.21 (1.09–1.34) *** | 1.11 (0.99–1.23) | 0.93 (0.82–1.05) | – |
| Widening PP | 1.74 (1.57–1.94) *** | 1.11 (0.99–1.24) | 1.15 (1.01–1.31) * | 1.10 (0.91–1.33) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jiang, Y.; Zhang, H.; Yang, Y.; Sun, Y.; Tian, W. Pulse Pressure Independent of Mean Arterial Pressure Is Associated with Cardiovascular and All-Cause Mortality in Normotensive Elders: Findings from National Health and Nutrition Examination Survey III 1999–2014. J. Vasc. Dis. 2022, 1, 113-122. https://doi.org/10.3390/jvd1020013
Jiang Y, Zhang H, Yang Y, Sun Y, Tian W. Pulse Pressure Independent of Mean Arterial Pressure Is Associated with Cardiovascular and All-Cause Mortality in Normotensive Elders: Findings from National Health and Nutrition Examination Survey III 1999–2014. Journal of Vascular Diseases. 2022; 1(2):113-122. https://doi.org/10.3390/jvd1020013
Chicago/Turabian StyleJiang, Yuqi, Huanrui Zhang, Yu Yang, Yujiao Sun, and Wen Tian. 2022. "Pulse Pressure Independent of Mean Arterial Pressure Is Associated with Cardiovascular and All-Cause Mortality in Normotensive Elders: Findings from National Health and Nutrition Examination Survey III 1999–2014" Journal of Vascular Diseases 1, no. 2: 113-122. https://doi.org/10.3390/jvd1020013