Undergraduate Interprofessional Education in the European Higher Education Area: A Systematic Review

Abstract
:1. Introduction
- What are the theoretical backgrounds of IPE interventions in EHEA?
- What are the disciplines included in the IPE interventions?
- What are the key outcomes of IPE experiences?
- What are the key limitations of IPE experiences?
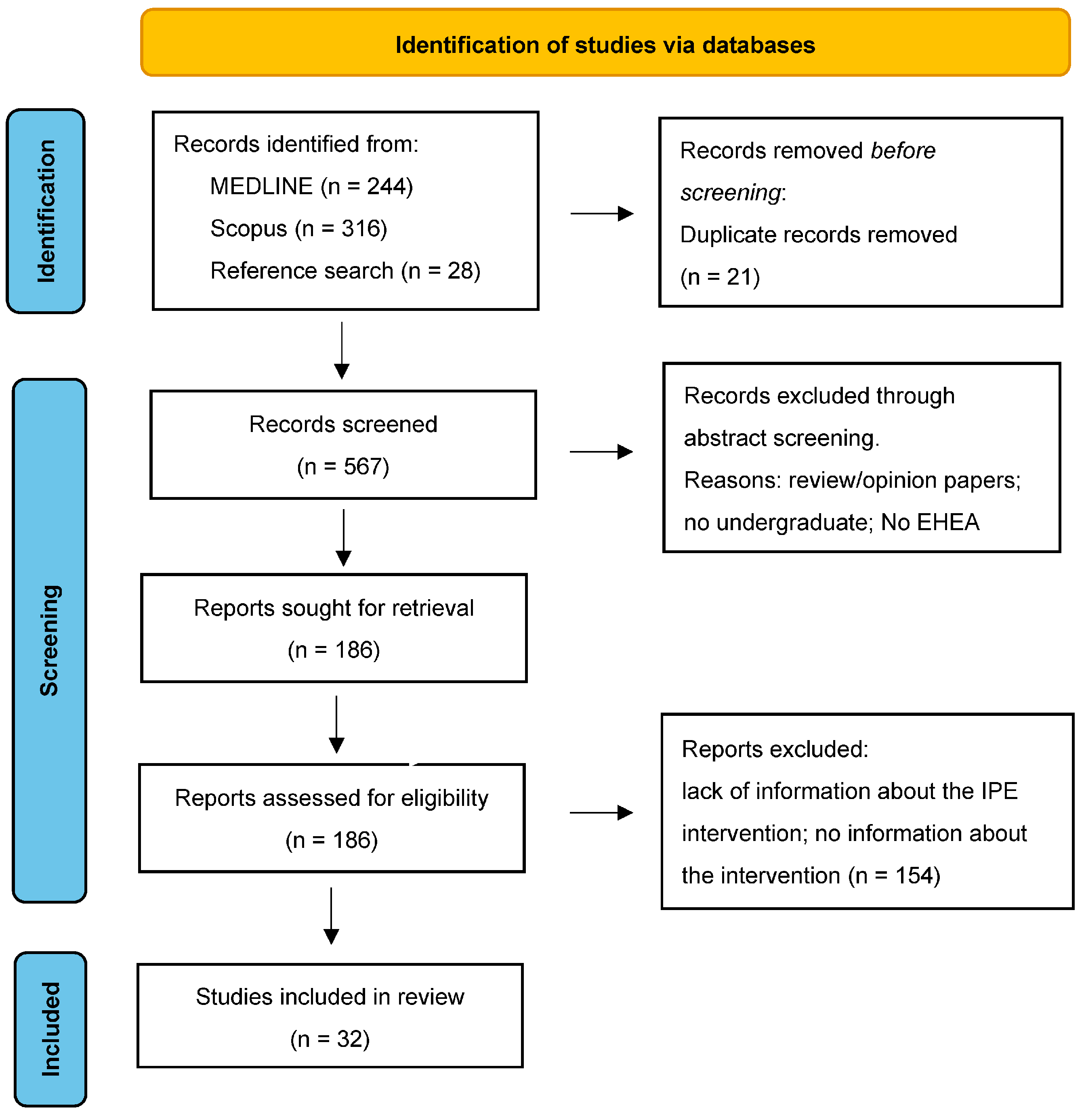
2. Materials and Methods
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
References
- World Health Organization. Framework for Action on Interprofessional Education and Collaborative Practice; No. WHO/HRH/HPN/10.3; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Spaulding, E.M.; Marvel, F.A.; Jacob, E.; Rahman, A.; Hansen, B.R.; Hanyok, L.A.; Han, H.R. Interprofessional education and collaboration among healthcare students and professionals: A systematic review and call for action. J. Interprof. Care 2021, 35, 612–621. [Google Scholar] [CrossRef]
- Irajpour, A.; Farzi, S.; Saghaei, M.; Ravaghi, H. Effect of interprofessional education of medication safety program on the medication error of physicians and nurses in the intensive care units. J. Edu. Health Promot. 2019, 8, 196. [Google Scholar]
- Reeves, S.; Perrier, L.; Goldman, J.; Freeth, D.; Zwarenstein, M. Interprofessional education: Effects on professional practice and healthcare outcomes. Cochrane Database Syst. Rev. 2013, 3, CD002213. [Google Scholar] [CrossRef]
- Zwarenstein, M.; Reeves, S.; Barr, H.; Hammick, M.; Koppel, I.; Atkins, J. Interprofessional education: Effects on professional practice and health care outcomes. Cochrane Database Syst. Rev. 2001, 1, CD002213. [Google Scholar]
- Smeets, H.W.H.; Sluijsmans, D.; Moser, A.; van Merriënboer, J.J. Design guidelines for assessing students’ interprofessional competencies in healthcare education: A consensus study. Perspect. Med. Educ. 2022, 11, 316–324. [Google Scholar] [CrossRef]
- Homberg, A.; Krug, K.; Klafke, N.; Glasse, K.; Mahler, C.; Loukanova, S. Consensus views on competencies and teaching methods for an interprofessional curriculum on complementary and integrative medicine: A Delphi study. J. Integr. Med. 2021, 19, 282–290. [Google Scholar] [CrossRef]
- Buring, S.M.; Bhushan, A.; Broeseker, A.; Conway, S.; Duncan-Hewitt, W.; Hansen, L.; Westberg, S. Interprofessional education: Definitions, student competencies, and guidelines for implementation. Am. J. Pharm. Educ. 2009, 73, 59. [Google Scholar] [CrossRef] [Green Version]
- Bologna Process Committee. Joint Declaration of the European Ministers of Education Convened in Bologna on 19 June 1999. 1999. Available online: http://www.ehea.info/page-ministerial-conference-bologna-1999 (accessed on 3 September 2022).
- Bologna Process. Sorbonne Declaration. 1998. Available online: http://www.ehea.info/page-sorbonne-declaration-1998 (accessed on 3 September 2022).
- Colonnello, V.; Mattarozzi, K.; Russo, P.M. Promoting a curriculum focused on the affective dimension of learning in medical education. In Bologna Process Beyond 2020: Fundamental Values of the EHEA; Noorda, S., Scott, P., Vukasoviċ, M., Eds.; Bononia University Press: Bologna, Italy, 2019; Volume 2019, pp. 177–182. [Google Scholar]
- Cumming, A. The Bologna process, medical education and integrated learning. Med. Teach. 2010, 32, 316–318. [Google Scholar] [CrossRef]
- Snelgrove, H.; Familiari, G.; Gallo, P.; Gaudio, E.; Lenzi, A.; Ziparo, V.; Frati, L. The challenge of reform: 10 years of curricula change in Italian medical schools. Med. Teach. 2009, 3, 1047–1055. [Google Scholar] [CrossRef]
- Christensen, L. The Bologna Process and medical education. Med. Teach. 2004, 26, 625–629. [Google Scholar] [CrossRef]
- Reeves, S.; Fletcher, S.; Barr, H.; Birch, I.; Boet, S.; Davies, N.; McFadyen, A.; Rivera, J.; Kitto, S. A BEME systematic review of the effects of interprofessional education: BEME Guide No. 39. Med. Teach. 2016, 38, 656–668. [Google Scholar] [CrossRef] [Green Version]
- Homberg, A.; Klafke, N.; Glassen, K.; Loukanova, S.; Mahler, C. Role competencies in interprofessional undergraduate education in complementary and integrative medicine: A delphi study. Complement. Ther. Med. 2020, 54, 102542. [Google Scholar] [CrossRef]
- Abu-Rish, E.; Kim, S.; Choe, L.; Varpio, L.; Malik, E.; White, A.A.; Zierler, B. Current trends in interprofessional education of health sciences students: A literature review. J. Interprof. Care 2012, 26, 444–451. [Google Scholar] [CrossRef]
- Thistlethwaite, J. Interprofessional education: A review of context, learning and the research agenda. Med. Educ. 2012, 46, 58–70. [Google Scholar] [CrossRef]
- Spada, F.; Caruso, R.; De Maria, M.; Karma, E.; Oseku, A.; Pata, X.; Stievano, A. Italian Translation and Validation of the Readiness for Interprofessional Learning Scale (RIPLS) in an Undergraduate Healthcare Student Context. Healthcare 2022, 10, 1698. [Google Scholar] [CrossRef]
- Villagrán, I.; Jeldez, P.; Calvo, F.; Fuentes, J.; Moya, J.; Barañao, P.; Fuentes-López, E. Spanish version of the readiness for interprofessional learning scale (RIPLS) in an undergraduate health sciences student context. J. Interprof. Care 2022, 36, 318–326. [Google Scholar] [CrossRef]
- Pedersen, T.H.; Cignacco, E.; Meuli, J.; Habermann, F.; Berger-Estilita, J.; Greif, R. The German interprofessional attitudes scale: Translation, cultural adaptation, and validation. GMS J. Med. Educ. 2020, 37, Doc:32. [Google Scholar]
- Bachmann, C.; Kiessling, C.; Härtl, A.; Haak, R. Communication in health professions: A European consensus on inter-and multi-professional learning objectives in German. GMS J. Med. Educ. 2016, 33, Doc:23. [Google Scholar]
- Shaw, E.; Walpole, S.; McLean, M.; Alvarez-Nieto, C.; Barna, S.; Bazin, K.; Woollard, R. AMEE consensus statement: Planetary health and education for sustainable healthcare. Med. Teach. 2021, 43, 272–286. [Google Scholar] [CrossRef]
- Witti, M.J.; Hartmann, D.; Wershofen, B.; Zottmann, J.M. Building interprofessional and interinstitutional bridges in health care education. Med. Educ. 2021, 55, 1309–1310. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Int. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [Green Version]
- Reed, D.A.; Cook, D.A.; Beckman, T.J.; Levine, R.B.; Kern, D.E.; Wright, S.M. Association Between Funding and Quality of Published Medical Education Research. JAMA 2007, 298, 1002–1009. [Google Scholar] [CrossRef] [Green Version]
- Reed, D.A.; Beckman, T.J.; Wright, S.M.; Levine, R.B.; Kern, D.E.; Cook, D.A. Predictive Validity Evidence for Medical Education Research Study Quality Instrument Scores: Quality of Submissions to JGIM’s Medical Education Special Issue. J. Gen. Intern. Med. 2008, 23, 903–907. [Google Scholar] [CrossRef] [Green Version]
- O’Brien, B.C.; Harris, I.B.; Beckman, T.J.; Reed, D.A.; Cook, D.A. Standards for reporting qualitative research: A synthesis of recommendations. Acad. Med. 2014, 89, 1245–1251. [Google Scholar] [CrossRef]
- Blum, C.G.; Richter, R.; Fuchs, R.; Sandeck, F.; Kunz, K.; Heermann, S. Interprofessional education in medical and physiotherapy studies for future collaboration. Ann. Anat. 2022, 240, 151850. [Google Scholar] [CrossRef]
- Homberg, A.; Ziegler, S.; Mahler, C.; Schultz, J.H.; Loukanova, S.; Hundertmark, J. Opening up a tailored tutor qualification program for medical students to other healthcare students—A mixed-method study. BMC Med. Educ. 2022, 22, 251. [Google Scholar] [CrossRef]
- Bergendahl, L.; Werner, F.; Schmidt, A.; Ronicke, M.; Renner, R.; Erfurt-Berge, C. Development and evaluation of an interprofessional teaching concept for modern wound management. JDDG 2020, 18, 977–982. [Google Scholar] [CrossRef]
- Mink, J.; Mitzkat, A.; Krug, K.; Mihaljevic, A.; Trierweiler-Hauke, B.; Götsch, B.; Mahler, C. Impact of an interprofessional training ward on interprofessional competencies—A quantitative longitudinal study. J. Interprof. Care 2020, 35, 751–759. [Google Scholar] [CrossRef]
- Scheide, L.; Huber, T.; Bette, S.; Nest, A.; Zimmer, C.; Berberat, P.O.; Kreiser, K. Imagine Neuro-Oncology-a one week course with medical and technical students: Students’ reflections about multidisciplinarity and its practical relevance. J. Interprof. Care 2020, 34, 202–210. [Google Scholar] [CrossRef]
- Straub, C.; Kruger, M.; Bode, S. Interprofessional education in pediatrics-Child protection and family ervices as a teaching example. Ann. Anat. 2017, 213, 62–68. [Google Scholar] [CrossRef]
- Balzer, K.; Schröder, R.; Junghans, A.; Stahl, U.; Träder, J.M.; Köpke, S. Improving competencies in evidence-based dementia care: Results from a pilot study on a novel inter-professional training course (the KOMPIDEM project). GMS J. Med. Educ. 2016, 33, Doc35. [Google Scholar]
- Reichel, K.; Dietsche, S.; Hölzer, H.; Ewers, M. Interprofessional peer-assisted learning as a low-threshold course for joint learning: Evaluation results of the interTUT Project. GMS J. Med. Educ. 2016, 33, Doc:30. [Google Scholar]
- Jebara, T.; Thomas, I.; Cunningham, S.; Rushworth, G.F. Pharmacy and medical student interprofessional education placement week. Clin. Teach. 2022, 19, 143–149. [Google Scholar] [CrossRef]
- Gupta, S.; Howden, S. Context and mechanisms of interprofessional learning during a Longitudinal Integrated Clerkship. J. Interprof. Care 2022, 36, 413–418. [Google Scholar] [CrossRef]
- Leadbeater, W.; Pallett, R.; Dunn, E.; Bashir, A. A virtual approach to promote inter-professional learning (IPL) between biomedical science and medicine in higher education for the benefit of patient care. Public Health Front. 2021, 9, 747751. [Google Scholar] [CrossRef]
- Thompson, S.; Metcalfe, K.; Boncey, K.; Merriman, C.; Flynn, L.C.; Alg, G.S.; Bothwell, H.; Johnston, C.F.; Puffett, E.; Hardy, C.; et al. Interprofessional education in geriatric medicine: Towards best practice. A controlled before-after study of medical and nursing students. BMJ Open 2019, 10, e018041. [Google Scholar] [CrossRef] [Green Version]
- Attoe, C.; Lavelle, M.; Sherwali, S.; Rimes, K.A.; Jabur, Z. Student interprofessional mental health simulation (SIMHS): Evaluating the impact on medical and nursing students, and clinical psychology trainees. J. Ment. Health Train. Educ. Pract. 2018, 14, 46–58. [Google Scholar] [CrossRef]
- Morse, J.C.; Brown, C.W.; Morrison, I.; Wood, C. Interprofessional learning in immediate life support training does effect TEAM performance during simulated resuscitation. BMJ Simul. Technol. Enhanc. Learn. 2019, 54, 204–209. [Google Scholar] [CrossRef]
- Young, M.; Wilkinson, T. Near-peer interprofessional simulation training in an undergraduate setting. BMJ Simul. Technol. Enhanc. Learn. 2018, 5, 111–113. [Google Scholar] [CrossRef]
- Nasir, J.; Goldie, J.; Little, A.; Banerjee, D.; Reeves, S. Case-based interprofessional learning for undergraduate healthcare professionals in the clinical setting. J. Interprof. Care 2017, 31, 125–128. [Google Scholar] [CrossRef]
- Edelbring, S.; Broberger, E.; Sandelius, S.; Norberg, J.; Wiegleb Edström, D. Flexible interprofessional student encounters based on virtual patients: A contribution to an interprofessional strategy. J. Interprof. Care 2022, 36, 310–317. [Google Scholar] [CrossRef]
- Kiessling, A.; Amiri, C.; Arhammar, J.; Lundbäck, M.; Wallingstam, C.; Wikner, J.; Kuhl, J. Interprofessional simulation-based team-training and self-efficacy in emergency medicine situations. J. Interprof. Care 2022, 36, 873–881. [Google Scholar] [CrossRef]
- Pelling, S.; Kalén, A.; Hammar, M.; Wahlström, O. Preparation for becoming members of health care teams: Findings from a 5-year evaluation of a student interprofessional training ward. J. Interprof. Care 2011, 25, 328–332. [Google Scholar] [CrossRef] [Green Version]
- Fagerdahl, A.M.; Torbjörnsson, E.; Sondén, A. An Interprofessional E-Learning Resource to Prepare Students for Clinical Practice in the Operating Room—A Mixed Method Study from the Students’ Perspective. Healthcare 2021, 9, 1028. [Google Scholar]
- Hallin, K.; Kiessling, A.; Waldner, A.; Henriksson, P. Active interprofessional education in a patient -based setting increases perceived collaborative and professional competence. Med. Teach. 2009, 31, 151–157. [Google Scholar]
- Swinnen, E.; Fobelets, M.; Adriaenssens, N.; Vandyck, E.; Goelen, G.; Moortgat, E.; Laforge, D.; Peersman, W. Effectiveness of an Interprofessional Education Model to Influence Students’ Perceptions on Interdisciplinary Work. J. Nurs. Educ. 2021, 60, 494–499. [Google Scholar]
- Račić, M.; Joksimović, B.N.; Cicmil, S.; Kusmuk, S.; Ivković, N.; Hadživuković, N.; Dubravac, M. The effects of interprofessional diabetes education on the knowledge of medical, dentistry and nursing students. Acta Med. Acad. 2017, 46, 145–154. [Google Scholar] [CrossRef]
- Perisin, A.S.; Mestrovic, A.; Bozic, J.; Kacic, J.; Bukic, J.; Leskur, D.; Rusic, D.; Zekan, L.; Stipic, M.; Modun, D. Interprofessional pharmacotherapy workshop: Intervention to improve health professionals’ and students’ attitudes towards collaboration between physicians and pharmacists. J. Interprof. Care 2018, 33, 456–463. [Google Scholar] [CrossRef]
- Hansen, T.B.; Pape, B.; Thiesen, P.S.; Jakobsen, F. Interprofessional versus uniprofessional dyad learning for medical students in a clinical setting. Int. J. Med. Educ. 2020, 2020, 191–200. [Google Scholar] [CrossRef]
- Kangas, S.; Rintala, T.M.; Hannula, P.; Jamsen, E.; Kannisto, R.; Paavilainen, E.; Jaatinen, P. The impact of interprofessional education on students’ current and desired competence in diabetes care. Nurs. Open 2023, 10, 264–277. [Google Scholar] [CrossRef]
- Busca, E.; Airoldi, C.; Caristia, S.; Rinaldi, C.; Gambaro, E.; Barisone, M.; Ingrassia, P.L.; Marzullo, P.; Prodam, F.; Surico, D.; et al. The Impact of an Interprofessional Simulation-Based Education Intervention in Healthy Ageing: A Quasi-Experimental Study. Clin. Simul. Nurs. 2022, 64, 1–9. [Google Scholar]
- Teuwen, C.; van der Burgt, S.; Kusurkar, R.; Schreurs, H.; Daelmans, H.; Peerdeman, S. How does interprofessional education influence students’ perceptions of collaboration in the clinical setting? A qualitative study. BMC Med. Educ. 2022, 22, 325. [Google Scholar] [CrossRef]
- Jakobsen, R.B.; Gran, S.F.; Grimsmo, B.; Arntzen, K.; Fosse, E.; Frich, J.C.; Hjortdahl, P. Examining participant perceptions of an interprofessional simulation-based trauma team training for medical and nursing students. J. Interprof. Care 2018, 32, 80–88. [Google Scholar] [CrossRef] [Green Version]
- Neumann-Podczaska, A.; Seostianin, M.; Madejczyk, K.; Merks, P.; Religioni, U.; Tomczak, Z.; Wieczorowska-Tobis, K. An experimental education project for consultations of older adults during the pandemic and healthcare lockdown. Healthcare 2021, 9, 425. [Google Scholar] [CrossRef]
- Breckwoldt, J.; Knecht, M.; Massée, R.; Flach, B.; Hofmann-Huber, C.; Kaap-Fröhlich, S.; Witt, C.M.; Aeberhard, R.; Sax, H. Operating room technician trainees teach medical students—An inter-professional peer teaching approach for infection prevention strategies in the operation room. Antimicrob. Resist. Infect. Control 2019, 8, 75. [Google Scholar] [CrossRef]
- Uslu-Sahan, F.; Terzioglu, F. Interprofessional simulation-based training in gynecologic oncology palliative care for students in the healthcare profession: A comparative randomized controlled trial. Nurse Educ. Today 2020, 95, 104588. [Google Scholar] [CrossRef]
- Kirkpatrick, D.L. Evaluating Training Programs: The Four Levels, 2nd ed.; Berrett-Koehler Publishers: San Francisco, CA, USA, 1998. [Google Scholar]
- Hean, S.; Craddock, D.; Hammick, M.; Hammick, M. Theoretical insights into interprofessional education: AMEE Guide No. 62. Med. Teach. 2012, 34, e78–e101. [Google Scholar] [CrossRef]
- Knowles, M.S. Androgogy in Action: Applying Modern Principles of Adult Learning; Jossey-Bass: San Francisco, CA, USA, 1984. [Google Scholar]
- Knowles, M. The Adult Learner: A Neglected Species; Gulf Publishing: Houston, TX, USA, 1990. [Google Scholar]
- Hammick, M.; Freeth, D.; Koppel, I.; Reeves, S.; Barr, H. A best evidence systematic review of interprofessional education (Best Evidence Medical Education Guide No 9). Med. Teach. 2007, 29, 735–751. [Google Scholar] [CrossRef]
- Deci, E.L.; Ryan, R.M. Self-determination theory: A macrotheory of human motivation, development, and health. Can. Psychol. 2008, 49, 182–185. [Google Scholar] [CrossRef] [Green Version]
- Ten Cate, T.J.; Kusurkar, R.A.; Williams, G.C. How self-determination theory can assist our understanding of the teaching and learning processes in medical education. AMEE Guide No. 59. Med. Teach. 2011, 33, 961–973. [Google Scholar] [CrossRef]
- Hutchins, E. Cognition in the Wild; MIT Press: Cambridge, MA, USA, 1995. [Google Scholar]
- Hutchins, E. The role of cultural practices in the emergence of modern human intelligence. Philos. Trans. R. Soc. B 2008, 363, 2011–2019. [Google Scholar] [CrossRef] [Green Version]
- Boyle, J.G.; Walters, M.R.; Jamieson, S.; Durning, S.J. Distributed cognition: Theoretical insights and practical applications to health professions education: AMEE Guide No. 159. Med. Teach. 2023, 1–11. [Google Scholar] [CrossRef]
- World Health Organization. Framework for Action on Interprofessional Education & Collaborative Practice by the Health Professions Network Nursing and Midwifery Office within the Department of Human Resources for Health. Available online: http://www.who.int/hrh/nursing_midwifery/en/ (accessed on 16 April 2023).
- Artino, A.R., Jr.; Holmboe, E.S.; Durning, S.J. Control-value theory: Using achievement emotions to improve understanding of motivation, learning, and performance in medical education: AMEE Guide No. 64. Med. Teach. 2012, 34, e148–e160. [Google Scholar] [CrossRef]
- Colonnello, V. Enhancing remediation by focusing on affective experience. Med. Educ. 2021, 55, 1338. [Google Scholar] [CrossRef]
- Dadich, A.; Olson, R.E. How and why emotions matter in interprofessional healthcare. Int. J. Work Organ. Emot. 2017, 8, 59–79. [Google Scholar] [CrossRef]
- Colonnello, V.; Mattarozzi, K.; Agostini, A.; Russo, P.M. Emotionally salient patient information enhances the educational value of surgical videos. Adv. Health Sci. Educ. 2020, 25, 799–808. [Google Scholar] [CrossRef]
- Colonnello, V.; Leonardi, G.; Farinelli, M.; Russo, P.M. The relationship of psychological health and primary emotional traits in medical students. Med. Teach. 2022, 1–7. [Google Scholar] [CrossRef]
- Colonnello, V.; Fino, E.; Russo, P.M. Attachment anxiety and depressive symptoms in undergraduate medical students: The mediating role of emotion regulation strategies. Perspect. Med. Educ. 2022, 11, 207–212. [Google Scholar] [CrossRef]
- Colonnello, V.; Mattarozzi, K.; Russo, P.M. Emotion recognition in medical students: Effects of facial appearance and care schema activation. Med. Educ. 2019, 53, 195–205. [Google Scholar] [CrossRef]


{kind=link}
| Country | Target Population | Key Outcome | Key Limitation | Reference |
|---|---|---|---|---|
| Germany | Medicine; physiotherapy | Increased students’ attitudes and perceptions towards IPE in anatomy and understanding of professional roles and teamwork | Selection bias | [29] |
| Medicine; nursing; allied healthcare | Satisfaction with an interprofessional tutor qualification program | No pre-post-survey; single site study; no control group; results are based on self-assessments; no study of mechanisms underlying students’ satisfaction | [30] | |
| Medicine; nursing | Increased subjective level of knowledge about wound management | Selection bias | [31] | |
| Medicine; nursing | Positive short-term effects in participants’ perception of interprofessional competencies; positive long-term effects on socialization and collaboration | Single center; small sample size; no control group; no instruments for objective assessments | [32] | |
| Medicine and STEM (physics, engineering, computer science, and biomedical computing) | Students’ positive evaluation of course content and learning methods | Small sample size; short observation; selection bias; no objective assessment | [33] | |
| Medicine; psychology; social work; clinical education; educational science | Students’ positive evaluation of course structure, content, and multidisciplinary setting; students’ perception of an “artificial dividing line” between professions | Not reported | [34] | |
| Medicine; nursing | Feasibility of the program; students’ positive evaluation of course scope and learning methods and need of improvement of practical learning outcomes | Small sample size; no objective measurements of learning outcomes | [35] | |
| Medicine; nursing; physiotherapy; not specified | Students’ positive evaluation of course content, atmosphere, and learning activities | Selection bias; limited knowledge gain | [36] | |
| UK | Medicine; pharmacy | students’ positive perception of IPE program and increased subjective level of knowledge | Not reported | [37] |
| Medicine | Students’ positive perception of IP practice setting, interprofessional relationships, and engagement in clinical teams | Small sample size; selection-bias | [38] | |
| Medicine; biomedical science | Students’ perception of increased understanding of roles in IPC; students’ positive evaluation of course format | Selection bias; complexity of the planning; poor internet connectivity; small-sample size | [39] | |
| Medicine; nursing | students’ positive evaluation of course content and learning of teamwork and professional identity | Students’ unequal levels of clinical experience; no actual clinical practice cases; use of a standardized questionnaire with limited validity | [40] | |
| Medicine; mental health nursing; clinical psychology | increase in students’ self-reported knowledge, confidence, and attitudes | No comparison of educational interventions; small sample size; no validated measures of learning outcomes | [41] | |
| Medicine; nursing | increase in team performance, as evaluated by instructors | Possible influences between control and experimental groups | [42] | |
| Medicine; nursing | students’ self-reported increase of care knowledge of professional roles and limitations within the team | Selection bias; small sample size; no control group | [43] | |
| Medicine; nursing; pharmacy; physician associate; physiotherapy; midwifery; occupational therapy; speech and language therapy | Students’ positive perception of interaction with other professionals and multidisciplinary teams; students’ self-reported increased knowledge about professional roles | Trainers’ lack of awareness of the sessions | [44] | |
| Sweden | Medicine; nursing | Students’ self-reported gain in understanding of other profession’s roles, competences and in awareness about holistic patient care | Not reported | [45] |
| Medicine; nursing; graduate healthcare providers | Students’ satisfaction with the course and increase in confidence in interprofessional communication; perceived self-efficacy over a six-month period | No objective measures | [46] | |
| Medicine; nursing; occupational therapy; physiotherapy; biomedical laboratory science; medical biology; speech and language pathology | Students’ self-reported increase in knowledge about professional roles and the value of teamwork | Evaluation instrument was not a validated and contained only three questions | [47] | |
| Medicine; nursing | Students’ satisfaction with course and perceived gain in preparedness for their clinical placement | Small sample size; selection bias; no standardized measures | [48] | |
| Medicine; nursing; physiotherapy; occupational therapy | Students’ self-reported increased knowledge of IPC, communication, and teamwork | No gender specific results; no control group | [49] | |
| Belgium | Medicine; physiotherapy; nursing; nutrition | Students’ self-reported increase positive attitude toward IPC and perception of competence | Inadequate reliability of the scales; participants were not blinded to the intervention | [50] |
| Bosnia and Herzegovina | Medicine; dentistry; nursing | Students’ positive self-assessment of communication and teamwork skills | Single-site study; assessment at one point in time; self-assessment | [51] |
| Croatia | Medicine; pharmacy | Students’ reported increase in positive attitude towards IPC | single site setting; convenience sampling; small sample size; low response rate; reliability of measures | [52] |
| Denmark | Medicine; nursing | Students’ positive evaluation of IP training | No objective measures; single site setting; small sample size | [53] |
| Finland | Medicine; nursing | Students’ self-assessed increase of knowledge and competence | Small sample size; selection bias; no standardized measures | [54] |
| Italy | Medicine; nursing | Students reported positive attitudes toward communication skills; high levels of self-confidence and attitude toward learning in simulation | Selection bias; no objective measures; limited transferability of simulations | [55] |
| Netherland | Medicine; nursing. | Students’ positive self-assessment of knowledge gain in roles and responsibilities, improvement in patient care | Single site setting; interviewer was the teacher (social desirability bias); lack of long-term assessment | [56] |
| Norway | Medicine; nursing. | Students’ satisfaction with course material and self-reported increased insight ins about communication, teamwork and leadership Facilitators reported students’ knowledge gain in non-technical skills | No objective measures | [57] |
| Poland | Medicine; pharmacy | Students’ self-reported strengthening of their self-confidence and understanding of patient care skills | Small sample size | [58] |
| Switzerland | Medicine; healthcare tecniques | Students’ satisfaction with course; students reported a better understanding of roles | Selection bias; no objective measures; no assessment of learning | [59] |
| Turkey | Medicine; nursing; nutrition-dietetics; social work | Students’ self-reported gain in interdisciplinary education, perception, and teamwork attitude | Difficulties in IPE program planning; no objective changes of students’ behavior | [60] |
| Practical Recommendations for Future Research and Educational Programs | |
|---|---|
| Theoretical background |
|
| Methods |
|
| Evaluation and effectiveness |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Colonnello, V.; Kinoshita, Y.; Yoshida, N.; Bustos Villalobos, I. Undergraduate Interprofessional Education in the European Higher Education Area: A Systematic Review. Int. Med. Educ. 2023, 2, 100-112. https://doi.org/10.3390/ime2020010
Colonnello V, Kinoshita Y, Yoshida N, Bustos Villalobos I. Undergraduate Interprofessional Education in the European Higher Education Area: A Systematic Review. International Medical Education. 2023; 2(2):100-112. https://doi.org/10.3390/ime2020010
Chicago/Turabian StyleColonnello, Valentina, Yukako Kinoshita, Nao Yoshida, and Itzel Bustos Villalobos. 2023. "Undergraduate Interprofessional Education in the European Higher Education Area: A Systematic Review" International Medical Education 2, no. 2: 100-112. https://doi.org/10.3390/ime2020010