
A Narrative Review of Immersive Technology Enhanced Learning in Healthcare Education
Abstract
:1. Introduction
- What are the trends in medical education research on immersive technology?
- What are the disciplines in healthcare (within the scope of the review) in which immersive technology has been studied?
- What is the quality of the medical education research on immersive technology, including a formal assessment of instrument validity?
- What are the pedagogical concepts used to understand learning and user experience in the studies reviewed?
2. Literature Review
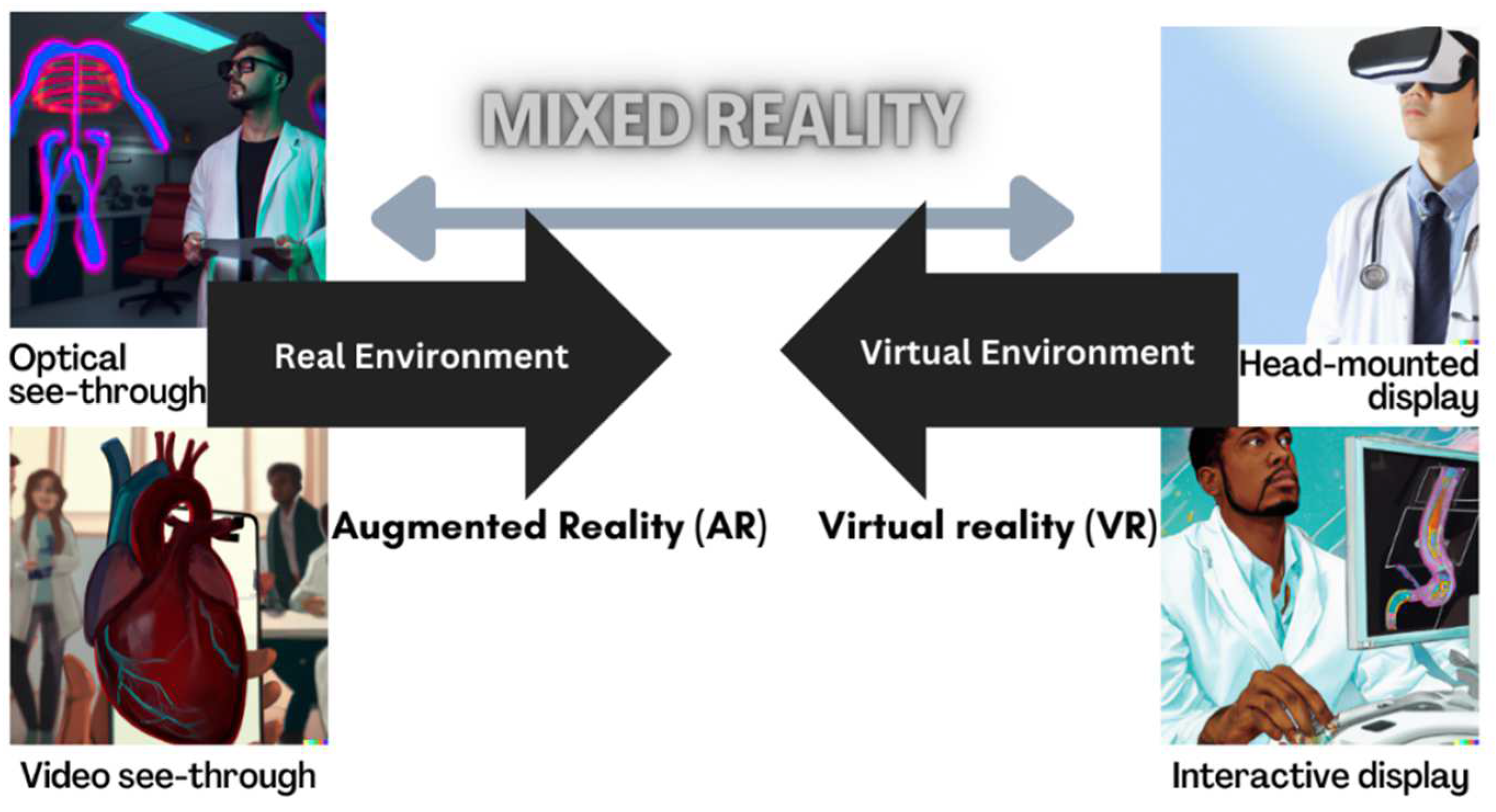
2.1. Definitions Relating to Immersive Technology
2.2. Related Literature of Medical Education, Theories of Learning, and Immersive Technology
3. Methods
3.1. Purpose and Reporting
3.2. Search Methods
3.3. Eligibility Criteria
3.4. Search Terms
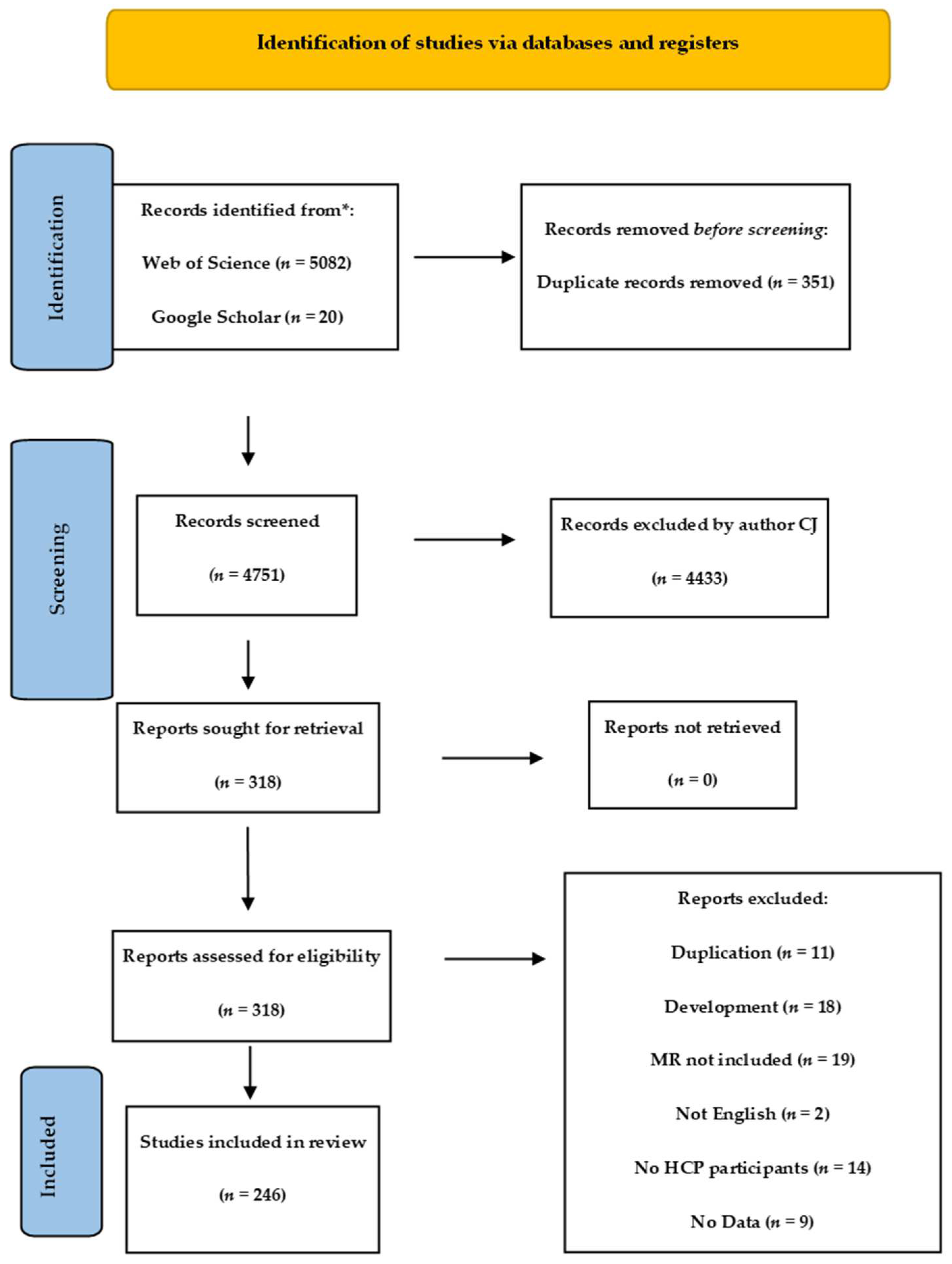
3.5. Selection Processing
3.6. Paper Quality Assessment Instrument
3.7. Charting the Data
3.8. Data Analysis
4. Results
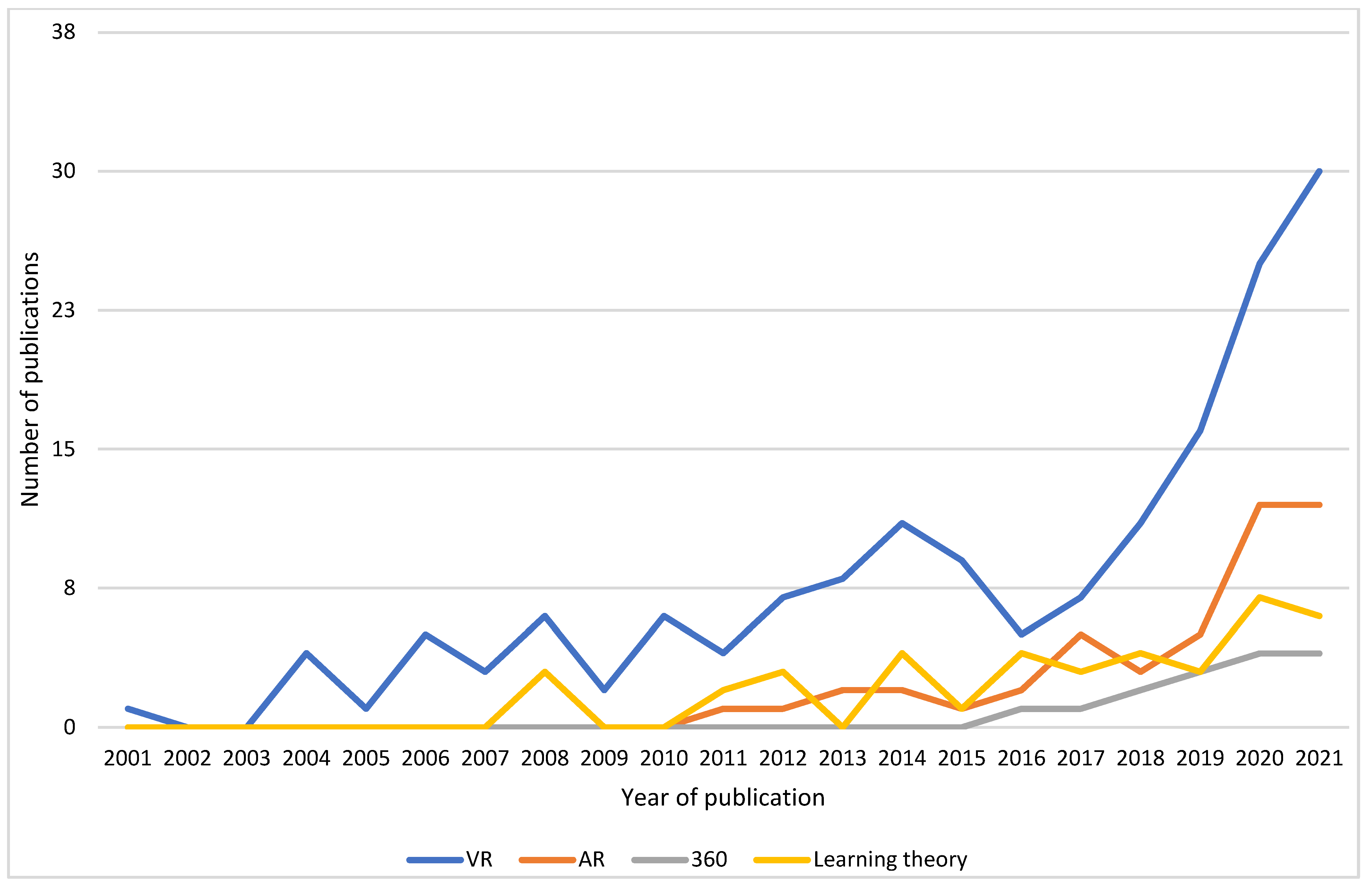
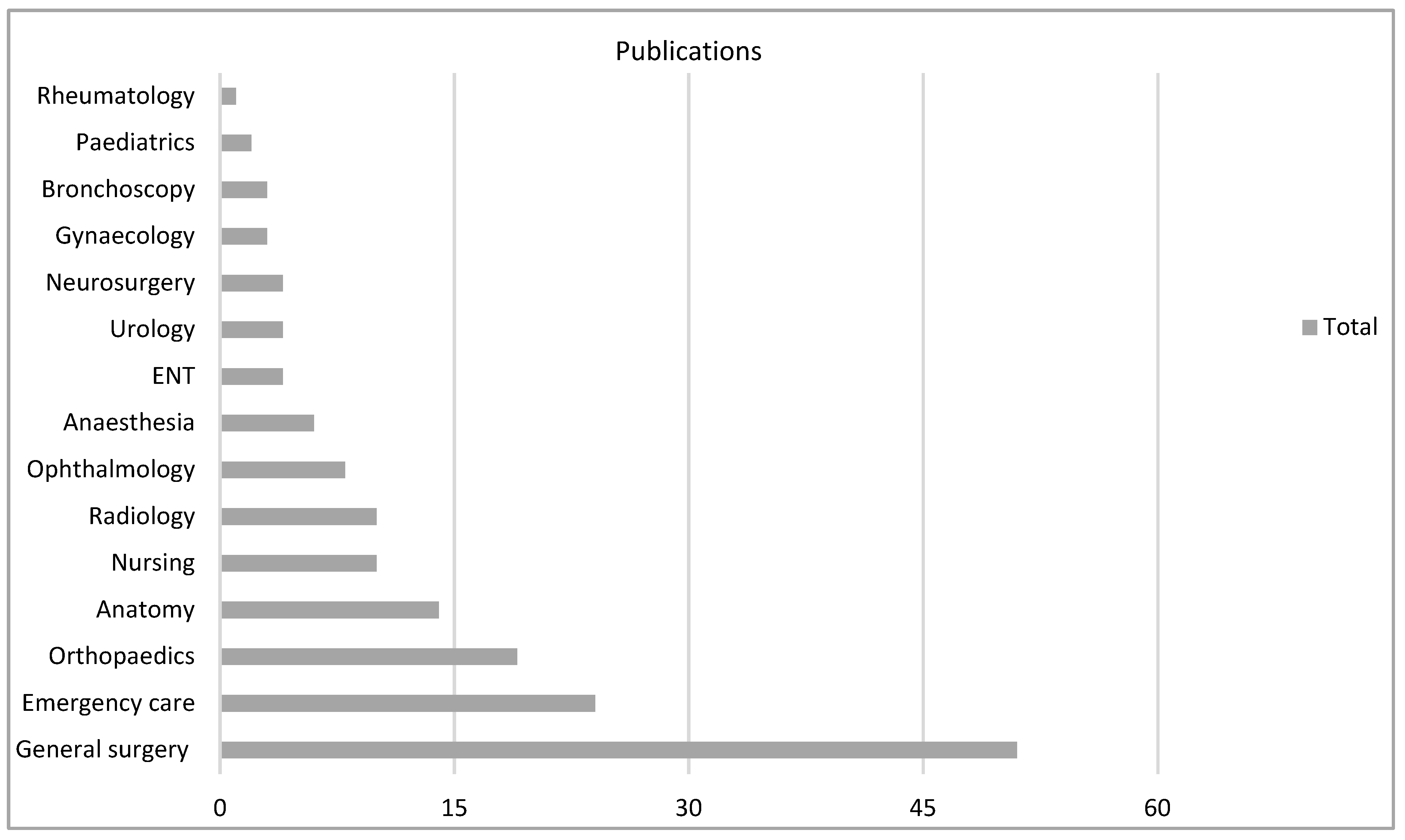
4.1. Study Characteristics—Research Questions 1 and 2
4.2. MERSQI Evaluation—Research Question 3
4.3. Instruments in VR
4.4. Instruments in AR
4.5. Instruments in 360
5. Synthesis of Main Study Findings—Research Question 4
5.1. VR Group
5.2. AR Group
5.3. 360 Group
5.4. Learning Theory
6. Discussion
- Apply a methodology that is grounded in learning theory and literature.
- Avoid basing conclusions on a newly created instrument but consider existing validated measures for further analysis.
- Do not assume a novice versus expert investigation equates to a thorough study of validity.
- Reframe the position on evidencing the superiority of TEL over traditional teaching methods and apply a non-inferior mindset.
- Technology is a tool, and the way technology is used to supplement learning is varied. MR may help some learning environments but not others.
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kotsis, S.V.; Chung, K.C. Application of the “See One, Do One, Teach One” Concept in Surgical Training. Plast. Reconstr. Surg. 2013, 131, 1194–1201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tang, K.S.; Cheng, D.L.; Mi, E.; Greenberg, P.B. Augmented reality in medical education: A systematic review. Can. Med. Educ. J. 2020, 11, e81–e96. [Google Scholar] [CrossRef] [PubMed]
- Baxendale, B.; Shinn, S.; Munsch, C.; Ralph, N. Enhancing Education, Clinical Practice and Staff Wellbeing. A National Vision for the Role of Simulation and Immersive Learning Technologies in Health and Care; Health Education England: Leeds, UK, 2020; Available online: https://www.hee.nhs.uk/ (accessed on 20 February 2022).
- Blair, C.; Walsh, C.; Best, P. Immersive 360° videos in health and social care education: A scoping review. BMC Med. Educ. 2021, 21, 590. [Google Scholar] [CrossRef]
- Suh, A.; Prophet, J. The state of immersive technology research: A literature analysis. Comput. Hum. Behav. 2018, 86, 77–90. [Google Scholar] [CrossRef]
- Swann, G.; Jacobs, C. Augmented reality medical student teaching within primary care. Future Healthc. J. 2021, 8, 15–16. [Google Scholar] [CrossRef]
- Kuhn, S.; Huettl, F.; Deutsch, K.; Kirchgassner, E.; Huber, T.; Kneist, W.; Kuhn, S.; Huettl, F.; Deutsch, K.; Kirchgaessner, E.; et al. Surgical Education in the Digital Age—Virtual Reality, Augmented Reality and Robotics in the Medical School. Zent. Fur Chir. 2021, 146, 37–43. [Google Scholar] [CrossRef]
- Moro, C.; Phelps, C.; Redmond, P.; Stromberga, Z.; Moro, C.; Phelps, C.; Redmond, P.; Stromberga, Z. HoloLens and mobile augmented reality in medical and health science education: A randomised controlled trial. Br. J. Educ. Technol. 2021, 52, 680–694. [Google Scholar] [CrossRef]
- Bala, L.; Kinross, J.; Martin, G.; Koizia, L.J.; Kooner, A.S.; Shimshon, G.J.; Hurkxkens, T.J.; Pratt, P.J.; Sam, A.H.; Bala, L.; et al. A remote access mixed reality teaching ward round. Clin. Teach. 2021, 18, 386–390. [Google Scholar] [CrossRef]
- Fukuta, J.; Gill, N.; Rooney, R.; Coombs, A.; Murphy, D.; Fukuta, J.; Gill, N.; Rooney, R.; Coombs, A.; Murphy, D. Use of 360 degrees Video for a Virtual Operating Theatre Orientation for Medical Students. J. Surg. Educ. 2021, 78, 391–393. [Google Scholar] [CrossRef] [PubMed]
- Sommer, G.M.; Broschewitz, J.; Huppert, S.; Sommer, C.G.; Jahn, N.; Jansen-Winkeln, B.; Gockel, I.; Hau, H.M.; Sommer, G.M.; Broschewitz, J.; et al. The role of virtual reality simulation in surgical training in the light of COVID-19 pandemic Visual spatial ability as a predictor for improved surgical performance: A randomized trial. Medicine 2021, 100, e27844. [Google Scholar] [CrossRef]
- Chan, V.; Larson, N.D.; Moody, D.A.; Moyer, D.G.; Shah, N.L.; Chan, V.; Larson, N.D.; Moody, D.A.; Moyer, D.G.; Shah, N.L. Impact of 360 degrees vs 2D Videos on Engagement in Anatomy Education. Cureus 2021, 13, e14260. [Google Scholar]
- Tang, Y.M.; Chau, K.Y.; Kwok, A.P.K.; Zhu, T.; Ma, X. A systematic review of immersive technology applications for medical practice and education—Trends, application areas, recipients, teaching contents, evaluation methods, and performance. Educ. Res. Rev. 2022, 35, 100429. [Google Scholar] [CrossRef]
- Chavez, O.L.; Rodriguez, L.F.; Gutierrez-Garcia, J.O.; Lopez Chavez, O.; Rodriguez, L.-F.; Octavio Gutierrez-Garcia, J. A comparative case study of 2D, 3D and immersive-virtual-reality applications for healthcare education. Int. J. Med. Inform. 2020, 141, 104226. [Google Scholar] [CrossRef]
- Munn, Z.; Peters, M.D.J.; Stern, C.; Tufanaru, C.; McArthur, A.; Aromataris, E. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med. Res. Methodol. 2018, 18, 143. [Google Scholar] [CrossRef]
- Slater, M. Place illusion and plausibility can lead to realistic behaviour in immersive virtual environments. Philos. Trans. R. Soc. B Biol. Sci. 2009, 364, 3549–3557. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ochs, M.; Mestre, D.; de Montcheuil, G.; Pergandi, J.M.; Saubesty, J.; Lombardo, E.; Francon, D.; Blache, P.; Ochs, M.; Mestre, D.; et al. Training doctors’ social skills to break bad news: Evaluation of the impact of virtual environment displays on the sense of presence. J. Multimodal User Interfaces 2019, 13, 41–51. [Google Scholar] [CrossRef] [Green Version]
- Sutherland, I. The ultimate display. In Proceedings of the Congress of the Internation Federation of Information Processing (IFIP), New York, NY, USA, 24–29 May 1965; Volume 2, pp. 506–508. [Google Scholar]
- Forrest, K.; McKimm, J. Healthcare Simulation at A Glance; John Wiley & Sons: Hoboken, NJ, USA, 2019. [Google Scholar]
- Milgram, P.; Kishino, F. A taxonomy of mixed reality visual displays. IEICE Trans. Inf. Syst. 1994, 77, 1321–1329. [Google Scholar]
- Lee, H.-G.; Chung, S.; Lee, W.-H. Presence in virtual golf simulators: The effects of presence on perceived enjoyment, perceived value, and behavioral intention. New Media Soc. 2013, 15, 930–946. [Google Scholar] [CrossRef]
- Zackoff, M.W.; Real, F.J.; Cruse, B.; Davis, D.; Klein, M.; Zackoff, M.W.; Real, F.J.; Cruse, B.; Davis, D.; Klein, M. Medical Student Perspectives on the Use of Immersive Virtual Reality for Clinical Assessment Training. Acad. Pediatr. 2019, 19, 849–851. [Google Scholar] [CrossRef]
- Kim, S.K.; Lee, Y.; Yoon, H.; Choi, J.; Kim, S.K.; Lee, Y.; Yoon, H.; Choi, J. Adaptation of Extended Reality Smart Glasses for Core Nursing Skill Training Among Undergraduate Nursing Students: Usability and Feasibility Study. J. Med. Internet Res. 2021, 23, e24313. [Google Scholar] [CrossRef]
- Lampropoulos, G.; Barkoukis, V.; Burden, K.; Anastasiadis, T. 360-degree video in education: An overview and a comparative social media data analysis of the last decade. Smart Learn. Environ. 2021, 8, 20. [Google Scholar] [CrossRef]
- Chuan, A.; Zhou, J.J.; Hou, R.M.; Stevens, C.J.; Bogdanovych, A. Virtual reality for acute and chronic pain management in adult patients: A narrative review. Anaesthesia 2021, 76, 695–704. [Google Scholar] [CrossRef]
- Hoffman, H.G.; Patterson, D.R.; Carrougher, G.J.; Sharar, S.R. Effectiveness of Virtual Reality—Based Pain Control With Multiple Treatments. Clin. J. Pain 2001, 17, 229–235. [Google Scholar] [CrossRef]
- Fong, K.N.K.; Tang, Y.M.; Sie, K.; Yu, A.K.H.; Lo, C.C.W.; Ma, Y.W.T. Task-specific virtual reality training on hemiparetic upper extremity in patients with stroke. Virtual Real. 2022, 26, 453–464. [Google Scholar] [CrossRef]
- Cortés-Pérez, I.; Nieto-Escamez, F.A.; Obrero-Gaitán, E. Immersive Virtual Reality in Stroke Patients as a New Approach for Reducing Postural Disabilities and Falls Risk: A Case Series. Brain Sci. 2020, 10, 296. [Google Scholar] [CrossRef] [PubMed]
- Scapin, S.; Echevarría-Guanilo, M.E.; Boeira Fuculo Junior, P.R.; Gonçalves, N.; Rocha, P.K.; Coimbra, R. Virtual Reality in the treatment of burn patients: A systematic review. Burns 2018, 44, 1403–1416. [Google Scholar] [CrossRef] [PubMed]
- Reilly, C.A.; Greeley, A.B.; Jevsevar, D.S.; Gitajn, I.L. Virtual reality-based physical therapy for patients with lower extremity injuries: Feasibility and acceptability. OTA Int. 2021, 4, e132. [Google Scholar] [CrossRef] [PubMed]
- Freitas, J.R.S.; Velosa, V.H.S.; Abreu, L.T.N.; Jardim, R.L.; Santos, J.A.V.; Peres, B.; Campos, P.A.-O. Virtual Reality Exposure Treatment in Phobias: A Systematic Review. Psychiatr. Q. 2021, 92, 1685–1710. [Google Scholar] [CrossRef]
- Matamala-Gomez, M.; Bottiroli, S.; Realdon, O.; Riva, G.; Galvagni, L.; Platz, T.; Sandrini, G.; De Icco, R.; Tassorelli, C. Telemedicine and Virtual Reality at Time of COVID-19 Pandemic: An Overview for Future Perspectives in Neurorehabilitation. Front. Neurol. 2021, 12, 646902. [Google Scholar] [CrossRef]
- Park, S.; Bokijonov, S.; Choi, Y. Review of microsoft hololens applications over the past five years. Appl. Sci. 2021, 11, 7259. [Google Scholar] [CrossRef]
- Kourouthanassis, P.; Boletsis, C.; Bardaki, C.; Chasanidou, D. Tourists responses to mobile augmented reality travel guides: The role of emotions on adoption behavior. Pervasive Mob. Comput. 2015, 18, 71–87. [Google Scholar] [CrossRef]
- Kolb, D. Experiential Learning: Experience as the Source of Learning and Development; Prentice-Hall: Hoboken, NJ, USA, 1984. [Google Scholar]
- Fauconnier, G. Conceptual blending and analogy. In The Analogical Mind: Perspectives from Cognitive Science; Bradford Books: Cambridge, UK, 2001; pp. 255–286. [Google Scholar]
- Sweller, J. Cognitive load theory. In Psychology of Learning and Motivation; Elsevier: Amsterdam, The Netherlands, 2011; Volume 55, pp. 37–76. [Google Scholar]
- Vermunt, J.D. The regulation of constructive learning processes. Br. J. Educ. Psychol. 1998, 68, 149–171. [Google Scholar] [CrossRef]
- Dweck, C.S. Motivational processes affecting learning. Am. Psychol. 1986, 41, 1040–1048. [Google Scholar] [CrossRef]
- Dengel, A.; Mägdefrau, J. Presence Is the Key to Understanding Immersive Learning; Springer: Berlin/Heidelberg, Germany, 2019; pp. 185–198. [Google Scholar]
- Dale, E. Audio-Visual Methods in Teaching; Dryden Press: Fort Worth, TX, USA, 1969. [Google Scholar]
- Keller, J.M. Motivation, learning, and technology: Applying the ARCS-V motivation model. Particip. Educ. Res. 2016, 3, 1–15. [Google Scholar] [CrossRef]
- Mayer, R.E. Incorporating motivation into multimedia learning. Learn. Instr. 2014, 29, 171–173. [Google Scholar] [CrossRef]
- Kyaw, B.M.; Saxena, N.; Posadzki, P.; Vseteckova, J.; Nikolaou, C.K.; George, P.P.; Divakar, U.; Masiello, I.; Kononowicz, A.A.; Zary, N.; et al. Virtual Reality for Health Professions Education: Systematic Review and Meta-Analysis by the Digital Health Education Collaboration. J. Med. Internet Res. 2019, 21, e12959. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bracq, M.-S.; Michinov, E.; Jannin, P. Virtual Reality Simulation in Nontechnical Skills Training for Healthcare Professionals: A Systematic Review. Simul. Healthc. 2019, 14, 188–194. [Google Scholar] [CrossRef]
- Mäkinen, H.; Haavisto, E.; Havola, S.; Koivisto, J.-M. User experiences of virtual reality technologies for healthcare in learning: An integrative review. Behav. Inf. Technol. 2022, 41, 1–17. [Google Scholar] [CrossRef]
- Gilmour, J.; Huntington, A.; Bogossian, F.; Leadbitter, B.; Turner, C. Medical education and informal teaching by nurses and midwives. Int. J. Med. Educ. 2014, 5, 171–175. [Google Scholar] [CrossRef] [Green Version]
- Jacobs, C. Immersive Technology in Healthcare Education: A Scoping Review. Available online: https://osf.io/tpjyw/ (accessed on 17 January 2022).
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maggio, L.A.; Costello, J.A.; Norton, C.; Driessen, E.W.; Artino, A.R., Jr. Knowledge syntheses in medical education: A bibliometric analysis. Perspect. Med. Educ. 2021, 10, 79–87. [Google Scholar] [CrossRef] [PubMed]
- Pei, L.; Wu, H. Does online learning work better than offline learning in undergraduate medical education? A systematic review and meta-analysis. Med. Educ. Online 2019, 24, 1666538. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reed, D.A.; Cook, D.A.; Beckman, T.J.; Levine, R.B.; Kern, D.E.; Wright, S.M. Association Between Funding and Quality of Published Medical Education Research. JAMA 2007, 298, 1002–1009. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reed, D.A.; Beckman, T.J.; Wright, S.M.; Levine, R.B.; Kern, D.E.; Cook, D.A. Predictive Validity Evidence for Medical Education Research Study Quality Instrument Scores: Quality of Submissions to JGIM’s Medical Education Special Issue. J. Gen. Intern. Med. 2008, 23, 903–907. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Debes, A.J.; Aggarwal, R.; Balasundaram, I.; Jacobsen, M.B.; Debes, A.J.; Aggarwal, R.; Balasundaram, I.; Jacobsen, M.B. A tale of two trainers: Virtual reality versus a video trainer for acquisition of basic laparoscopic skills. Am. J. Surg. 2010, 199, 840–845. [Google Scholar] [CrossRef] [PubMed]
- Elessawy, M.; Wewer, A.; Guenther, V.; Heilmann, T.; Eckmann-Scholz, C.; Schem, C.; Maass, N.; Noe, K.G.; Mettler, L.; Alkatout, I.; et al. Validation of psychomotor tasks by Simbionix LAP Mentor simulator and identifying the target group. Minim. Invasive Ther. Allied Technol. 2017, 26, 262–268. [Google Scholar] [CrossRef] [PubMed]
- Fiedler, M.J.; Chen, S.J.; Judkins, T.N.; Oleynikov, D.; Stergiou, N. Virtual Reality for Robotic Laparoscopic Surgical Training. In Studies in Health Technology and Informatics, Proceedings of 15th Conference on Medicine Meets Virtual Reality, Long Beach, CA, USA, 6–9 February 2007; IOS Press: Amsterdam, The Netherlands, 2007; Volume 125, pp. 127–129. [Google Scholar]
- Bartlett, J.D.; Lawrence, J.E.; Yan, M.; Guevel, B.; Stewart, M.E.; Audenaert, E.; Khanduja, V.; Bartlett, J.D.; Lawrence, J.E.; Yan, M.; et al. The learning curves of a validated virtual reality hip arthroscopy simulator. Arch. Orthop. Trauma Surg. 2020, 140, 761–767. [Google Scholar] [CrossRef] [Green Version]
- Gelinas-Phaneuf, N.; Choudhury, N.; Al-Habib, A.R.; Cabral, A.; Nadeau, E.; Mora, V.; Pazos, V.; Debergue, P.; DiRaddo, R.; Del Maestro, R.F.; et al. Assessing performance in brain tumor resection using a novel virtual reality simulator. Int. J. Comput. Assist. Radiol. Surg. 2014, 9, 1–9. [Google Scholar] [CrossRef]
- Sandy, N.S.; da Cruz, J.A.S.; Passerotti, C.C.; Nguyen, H.; dos Reis, S.T.; Gouveia, E.M.; Duarte, R.J.; Bruschini, H.; Srougi, M.; Sandy, N.S.; et al. Can the learning of laparoscopic skills be quantified by the measurements of skill parameters performed in a virtual reality simulator? Int. Braz. J. Urol. 2013, 39, 371–376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cychosz, C.C.; Tofte, J.N.; Johnson, A.; Gao, Y.B.; Phisitkul, P.; Cychosz, C.C.; Tofte, J.N.; Johnson, A.; Gao, Y.; Phisitkul, P. Fundamentals of Arthroscopic Surgery Training Program Improves Knee Arthroscopy Simulator Performance in Arthroscopic Trainees. Arthrosc.-J. Arthrosc. Relat. Surg. 2018, 34, 1543–1549. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, A.G.; Lederman, A.B.; McGlade, K.; Satava, R.M.; Smith, C.D.; Gallagher, A.G.; Lederman, A.B.; McGlade, K.; Satava, R.M.; Smith, C.D. Discriminative validity of the Minimally Invasive Surgical Trainer in Virtual Reality (MIST-VR) using criteria levels based on expert performance. Surg. Endosc. Other Interv. Tech. 2004, 18, 660–665. [Google Scholar] [CrossRef] [PubMed]
- Banaszek, D.; You, D.; Chang, J.; Pickell, M.; Hesse, D.; Hopman, W.M.; Borschneck, D.; Bardana, D. Virtual Reality Compared with Bench-Top Simulation in the Acquisition of Arthroscopic Skill A Randomized Controlled Trial. J. Bone Jt. Surg.-Am. Vol. 2017, 99, e34. [Google Scholar] [CrossRef] [PubMed]
- Chien, J.H.; Suh, I.H.; Park, S.H.; Mukherjee, M.; Oleynikov, D.; Siu, K.C. Enhancing Fundamental Robot-Assisted Surgical Proficiency by Using a Portable Virtual Simulator. Surg. Innov. 2013, 20, 198–203. [Google Scholar] [CrossRef] [PubMed]
- Gandhi, M.J.; Anderton, M.J.; Funk, L.; Gandhi, M.J.; Anderton, M.J.; Funk, L. Arthroscopic Skills Acquisition Tools: An Online Simulator for Arthroscopy Training. Arthrosc.-J. Arthrosc. Relat. Surg. 2015, 31, 1671–1679. [Google Scholar] [CrossRef] [PubMed]
- Gasco, J.; Patel, A.; Ortega-Barnett, J.; Branch, D.; Desai, S.; Kuo, Y.F.; Luciano, C.; Rizzi, S.; Kania, P.; Matuyauskas, M.; et al. Virtual reality spine surgery simulation: An empirical study of its usefulness. Neurol. Res. 2014, 36, 968–973. [Google Scholar] [CrossRef]
- Hart, R.; Doherty, D.A.; Karthigasu, K.; Garry, R.; Hart, R.; Doherty, D.A.; Karthigasu, K.; Garry, R. The value of virtual reality-simulator training in the development of laparoscopic surgical skills. J. Minim. Invasive Gynecol. 2006, 13, 126–133. [Google Scholar] [CrossRef] [PubMed]
- Hudak, S.J.; Landt, C.L.; Hernandez, J.; Soderdahl, D.W.; Hudak, S.J.; Landt, C.L.; Hernandez, J.; Soderdahl, D.W. External Validation of a Virtual Reality Transurethral Resection of the Prostate Simulator. J. Urol. 2010, 184, 2018–2022. [Google Scholar] [CrossRef] [PubMed]
- Johnston, T.J.; Tang, B.; Alijani, A.; Tait, I.; Steele, R.J.; Ker, J.; Nabi, G. Laparoscopic Surgical Skills are Significantly Improved by the Use of a Portable Laparoscopic Simulator: Results of a Randomized Controlled Trial. World J. Surg. 2013, 37, 957–964. [Google Scholar] [CrossRef] [PubMed]
- Kanumuri, P.; Ganai, S.; Wohaibi, E.M.; Bush, R.W.; Grow, D.R.; Seymour, N.E. Virtual reality and computer-enhanced training devices equally improve laparoscopic surgical skill in novices. Jsls-J. Soc. Laparoendosc. Surg. 2008, 12, 219–226. [Google Scholar]
- Le, T.D.B.; Adatia, F.A.; Lam, W.-C. Virtual reality ophthalmic surgical simulation as a feasible training and assessment tool: Results of a multicentre study. Can. J. Ophthalmol.-J. Can. D Ophtalmol. 2011, 46, 56–60. [Google Scholar] [CrossRef] [PubMed]
- LeBel, M.-E.; Haverstock, J.; Cristancho, S.; van Eimeren, L.; Buckingham, G. Observational Learning During Simulation-Based Training in Arthroscopy: Is It Useful to Novices? J. Surg. Educ. 2018, 75, 222–230. [Google Scholar] [CrossRef] [PubMed]
- Matzke, J.; Ziegler, C.; Martin, K.; Crawford, S.; Sutton, E. Usefulness of virtual reality in assessment of medical student laparoscopic skill. J. Surg. Res. 2017, 211, 191–195. [Google Scholar] [CrossRef] [PubMed]
- McClusky, D.A.; Ritter, E.M.; Lederman, A.B.; Gallagher, A.G.; Smith, C.D. Correlation between perceptual, visuo-spatial, and psychomotor aptitude to duration of training required to reach performance goals on the MIST-VR surgical simulator. Am. Surg. 2005, 71, 13–20. [Google Scholar] [CrossRef] [PubMed]
- Moore, A.K.; Grow, D.R.; Bush, R.W.; Seymour, N.E. Novices Outperform Experienced Laparoscopists on Virtual Reality Laparoscopy Simulator. JSLS-J. Soc. Laparoendosc. Surg. 2008, 12, 358–362. [Google Scholar]
- Mulla, M.; Sharma, D.; Moghul, M.; Kailani, O.; Dockery, J.; Ayis, S.; Grange, P. Learning Basic Laparoscopic Skills: A Randomized Controlled Study Comparing Box Trainer, Virtual Reality Simulator, and Mental Training. J. Surg. Educ. 2012, 69, 190–195. [Google Scholar] [CrossRef] [PubMed]
- Neumann, E.; Mayer, J.; Russo, G.I.; Amend, B.; Rausch, S.; Deininger, S.; Harland, N.; da Costa, I.A.; Hennenlotter, J.; Stenzl, A.; et al. Transurethral Resection of Bladder Tumors: Next-generation Virtual Reality Training for Surgeons. Eur. Urol. Focus 2019, 5, 906–911. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Newmark, J.; Dandolu, V.; Milner, R.; Grewal, H.; Harbison, S.; Hernandez, E. Correlating virtual reality and box trainer tasks in the assessment of laparoscopic surgical skills. Am. J. Obstet. Gynecol. 2007, 197, e1–e4. [Google Scholar] [CrossRef]
- Nielsen, M.R.; Kristensen, E.Q.; Jensen, R.O.; Mollerup, A.M.; Pfeiffer, T.; Graumann, O. Clinical Ultrasound Education for Medical Students Virtual Reality Versus e-Learning, a Randomized Controlled Pilot Trial. Ultrasound Q. 2021, 37, 292–296. [Google Scholar] [CrossRef] [PubMed]
- Nomura, T.; Mamada, Y.; Nakamura, Y.; Matsutani, T.; Hagiwara, N.; Fujita, I.; Mizuguchi, Y.; Fujikura, T.; Miyashita, M.; Uchida, E.; et al. Laparoscopic skill improvement after virtual reality simulator training in medical students as assessed by augmented reality simulator. Asian J. Endosc. Surg. 2015, 8, 408–412. [Google Scholar] [CrossRef] [PubMed]
- Orland, M.D.; Patetta, M.J.; Wieser, M.; Kayupov, E.; Gonzalez, M.H. Does Virtual Reality Improve Procedural Completion and Accuracy in an Intramedullary Tibial Nail Procedure? A Randomized Control Trial. Clin. Orthop. Relat. Res. 2020, 478, 2170–2177. [Google Scholar] [CrossRef] [PubMed]
- Paschold, M.; Huber, T.; Maedge, S.; Zeissig, S.R.; Lang, H.; Kneist, W. Laparoscopic assistance by operating room nurses: Results of a virtual-reality study. Nurse Educ. Today 2017, 51, 68–72. [Google Scholar] [CrossRef]
- Paschold, M.; Huber, T.; Zeissig, S.R.; Kauff, D.W.; Lang, H.; Kneist, W. Man versus machine: Is verbal instructor feedback in virtual-reality laparoscopic simulation dispensable? Results of a prospective randomised study. Biomed. Eng.-Biomed. Tech. 2014, 59, S1213–S1215. [Google Scholar]
- Paschold, M.; Huber, T.; Zeissig, S.R.; Lang, H.; Kneist, W. Tailored instructor feedback leads to more effective virtual-reality laparoscopic training. Surg. Endosc. Other Interv. Tech. 2014, 28, 967–973. [Google Scholar] [CrossRef] [PubMed]
- Peng, C.; Ng, K.M.; Roszczynialski, K.N.; Warrington, S.J.; Schertzer, K. Rapid Cycle Deliberate Practice in Virtual Reality: Teaching Transvenous Pacemaker Insertion to Emergency Medicine Residents. Cureus 2021, 13, e18503. [Google Scholar] [CrossRef] [PubMed]
- Pereferrer, F.S.; Gonzalez, M.H.; Garcia, A.M.; Vilanova, A.C.; Dejardin, D.D. Evaluation of surgical skills in medical students using a virtual simulator. Cir. Esp. 2013, 91, 177–183. [Google Scholar]
- Perez-Gutierrez, B.; Uribe-Quevedo, A.; Vega-Medina, L.; Salgado, J.S.; Jaimes, N.; Perez, O. Immersive and Non-Immersive VR Percutaneous Coronary Intervention Simulation for Acute Myocardial Infarction. In Proceedings of the 2020 IEEE 8th International Conference On Serious Games and Applications for Health (Segah 20), Vancouver, BC, Canada, 12–14 August 2020. [Google Scholar]
- Rivard, J.D.; Vergis, A.S.; Unger, B.J.; Hardy, K.M.; Andrew, C.G.; Gillman, L.M.; Park, J. Construct validity of individual and summary performance metrics associated with a computer-based laparoscopic simulator. Surg. Endosc. Other Interv. Tech. 2014, 28, 1921–1928. [Google Scholar] [CrossRef] [PubMed]
- Roehr, M.; Wu, T.; Maykowski, P.; Munter, B.; Hoebee, S.; Daas, E.; Kang, P. The Feasibility of Virtual Reality and Student-Led Simulation Training as Methods of Lumbar Puncture Instruction. Med. Sci. Educ. 2021, 31, 117–124. [Google Scholar] [CrossRef]
- Roitberg, B.Z.; Kania, P.; Luciano, C.; Dharmavaram, N.; Banerjee, P. Evaluation of Sensory and Motor Skills in Neurosurgery Applicants Using a Virtual Reality Neurosurgical Simulator: The Sensory-Motor Quotient. J. Surg. Educ. 2015, 72, 1165–1171. [Google Scholar] [CrossRef]
- Rose, K.; Pedowitz, R. Fundamental Arthroscopic Skill Differentiation With Virtual Reality Simulation. Arthrosc.-J. Arthrosc. Relat. Surg. 2015, 31, 299–305. [Google Scholar] [CrossRef]
- Rosenthal, R.; Gantert, W.A.; Scheidegger, D.; Oertli, D. Can skills assessment on a virtual reality trainer predict a surgical trainee’s talent in laparoscopic surgery? Surg. Endosc. Other Interv. Tech. 2006, 20, 1286–1290. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Peralta, L.F.; Sanchez-Margallo, F.M.; Moyano-Cuevas, J.L.; Pagador, J.B.; Enciso, S.; Gomez-Aguilera, E.J.; Uson-Gargallo, J. Learning curves of basic laparoscopic psychomotor skills in SINERGIA VR simulator. Int. J. Comput. Assist. Radiol. Surg. 2012, 7, 881–889. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Savran, M.M.; Nielsen, A.B.; Poulsen, B.B.; Thorsen, P.B.; Konge, L. Using virtual-reality simulation to ensure basic competence in hysteroscopy. Surg. Endosc. Other Interv. Tech. 2019, 33, 2162–2168. [Google Scholar] [CrossRef]
- Scerbo, M.W.; Bliss, J.P.; Schmidt, E.A.; Thompson, S.N. The efficacy of a medical virtual reality simulator for training phlebotomy. Hum. Factors 2006, 48, 72–84. [Google Scholar] [CrossRef]
- Seixas-Mikelus, S.A.; Adal, A.; Kesavadas, T.; Baheti, A.; Srimathveeravalli, G.; Hussain, A.; Chandrasekhar, R.; Wilding, G.E.; Guru, K.A. Can Image-Based Virtual Reality Help Teach Anatomy? J. Endourol. 2010, 24, 629–634. [Google Scholar] [CrossRef]
- Sheth, S.S.; Fader, A.N.; Tergas, A.I.; Kushnir, C.L.; Green, I.C. Virtual Reality Robotic Surgical Simulation: An Analysis of Gynecology Trainees. J. Surg. Educ. 2014, 71, 125–132. [Google Scholar] [CrossRef] [PubMed]
- Shetty, S.; Panait, L.; Baranoski, J.; Dudrick, S.J.; Bell, R.L.; Roberts, K.E.; Duffy, A.J. Construct and face validity of a virtual reality-based camera navigation curriculum. J. Surg. Res. 2012, 177, 191–195. [Google Scholar] [CrossRef] [PubMed]
- Snyder, C.W.; Vandromme, M.J.; Tyra, S.L.; Hawn, M.T. Proficiency-Based Laparoscopic and Endoscopic Training With Virtual Reality, Simulators: A Comparison of Proctored and Independent Approaches. J. Surg. Educ. 2009, 66, 201–207. [Google Scholar] [CrossRef]
- Sugand, K.; Wescott, R.A.; Carrington, R.; Hart, A.; van Duren, B.H. Training and Transfer Effect of FluoroSim, an Augmented Reality Fluoroscopic Simulator for Dynamic Hip Screw Guidewire Insertion A Single-Blinded Randomized Controlled Trial. J. Bone Jt. Surg.-Am. Vol. 2019, 101, e88. [Google Scholar] [CrossRef]
- Tanoue, K.; Ieiri, S.; Konishi, K.; Yasunaga, T.; Okazaki, K.; Yamaguchi, S.; Yoshida, D.; Kakeji, Y.; Hashizume, M. Effectiveness of endoscopic surgery training for medical students using a virtual reality simulator versus a box trainer: A randomized controlled trial. Surg. Endosc. Other Interv. Tech. 2008, 22, 985–990. [Google Scholar] [CrossRef]
- Van Ginkel, M.P.H.; Schijven, M.P.; van Grevenstein, W.M.U.; Schreuder, H.W.R. Bimanual Fundamentals: Validation of a New Curriculum for Virtual Reality Training of Laparoscopic Skills. Surg. Innov. 2020, 27, 523–533. [Google Scholar] [CrossRef] [PubMed]
- Vergmann, A.S.; Vestergaard, A.H.; Grauslund, J. Virtual vitreoretinal surgery: Validation of a training programme. Acta Ophthalmol. 2017, 95, 60–65. [Google Scholar] [CrossRef] [PubMed]
- Connolly, M.; Seligman, J.; Kastenmeier, A.; Goldblatt, M.; Gould, J.C. Validation of a virtual reality-based robotic surgical skills curriculum. Surg. Endosc. Other Interv. Tech. 2014, 28, 1691–1694. [Google Scholar] [CrossRef]
- Fiedler, M.J.; Chen, S.-J.; Judkins, T.N.; Oleynikov, D.; Stergiou, N. Virtual Reality for Robotic Laparoscopic Surgical Training. In Medicine Meets Virtual Reality 15: In Vivo, In Vitro, In Silico: Designing The Next In Medicine; IOS Press: Amsterdam, The Netherlands, 2007; Volume 125, pp. 127–129. [Google Scholar]
- Van Gestel, F.; Frantz, T.; Vannerom, C.; Verhellen, A.; Gallagher, A.G.; Elprama, S.A.; Jacobs, A.; Buyl, R.; Bruneau, M.; Jansen, B.; et al. The effect of augmented reality on the accuracy and learning curve of external ventricular drain placement. Neurosurg. Focus 2021, 51, E8. [Google Scholar] [CrossRef]
- Phe, V.; Cattarino, S.; Parra, J.; Bitker, M.O.; Ambrogi, V.; Vaessen, C.; Roupret, M. Outcomes of a virtual-reality simulator-training programme on basic surgical skills in robot-assisted laparoscopic surgery. Int. J. Med. Robot. Comput. Assist. Surg. 2017, 13, 183–202. [Google Scholar] [CrossRef]
- Hardon, S.F.; Kooijmans, A.; Horeman, R.; van der Elst, M.; Bloemendaal, A.L.A.; Horeman, T. Validation of the portable virtual reality training system for robotic surgery (PoLaRS): A randomized controlled trial. Surg. Endosc. Other Interv. Techniques. 2022, 36, 5282–5292. [Google Scholar] [CrossRef] [PubMed]
- Issleib, M.; Kromer, A.; Pinnschmidt, H.O.; Suss-Havemann, C.; Kubitz, J.C. Virtual reality as a teaching method for resuscitation training in undergraduate first year medical students: A randomized controlled trial. Scand. J. Trauma Resusc. Emerg. Med. 2021, 29, 27. [Google Scholar] [CrossRef]
- Berg, H.; Steinsbekk, A. Is individual practice in an immersive and interactive virtual reality application non-inferior to practicing with traditional equipment in learning systematic clinical observation? A randomized controlled trial. BMC Med. Educ. 2020, 20, 123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bishop, M.E.; Ode, G.E.; Hurwit, D.J.; Zmugg, S.; Rauck, R.C.; Nguyen, J.T.; Ranawat, A.S. The Arthroscopic Surgery Skill Evaluation Tool Global Rating Scale is a Valid and Reliable Adjunct Measure of Performance on a Virtual Reality Simulator for Hip Arthroscopy. Arthrosc.-J. Arthrosc. Relat. Surg. 2021, 37, 1856–1866. [Google Scholar] [CrossRef] [PubMed]
- Chang, J.; Banaszek, D.C.; Gambrel, J.; Bardana, D. Global Rating Scales and Motion Analysis Are Valid Proficiency Metrics in Virtual and Benchtop Knee Arthroscopy Simulators. Clin. Orthop. Relat. Res. 2016, 474, 956–964. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mulligan, A.; Vaghela, K.R.; Jeyaseelan, L.; Lee, J.; Akhtar, K. Transferable Global Rating Scales in the Validation of the ArthroSim (TM) Virtual Reality Arthroscopy Simulator. Surg. Technol. Int.-Int. Dev. Surg. Surg. Res. 2020, 37, 306–311. [Google Scholar]
- Wong, D.T.; Mehta, A.; Singh, K.P.; Leong, S.M.; Ooi, A.; Niazi, A.; You-Ten, E.; Okrainec, A.; Patel, R.; Singh, M.; et al. The effect of virtual reality bronchoscopy simulator training on performance of bronchoscopic-guided intubation in patients A randomised controlled trial. Eur. J. Anaesthesiol. 2019, 36, 227–233. [Google Scholar] [CrossRef] [PubMed]
- Chidambaram, S.; Erridge, S.; Leff, D.; Purkayastha, S. A Randomized Controlled Trial of Skills Transfer: From Touch Surgery to Laparoscopic Cholecystectomy. J. Surg. Res. 2019, 234, 217–223. [Google Scholar] [CrossRef]
- Hoogenes, J.; Wong, N.; Al-Harbi, B.; Kim, K.S.; Vij, S.; Bolognone, E.; Quantz, M.; Guo, Y.B.; Shayegan, B.; Matsumoto, E.D.; et al. A Randomized Comparison of 2 Robotic Virtual Reality Simulators and Evaluation of Trainees’ Skills Transfer to a Simulated Robotic Urethrovesical Anastomosis Task. Urology 2018, 111, 110–115. [Google Scholar] [CrossRef] [PubMed]
- Janse, J.A.; Goedegebuure, R.S.A.; Veersema, S.; Broekmans, F.J.M.; Schreuder, H.W.R. Hysteroscopic Sterilization Using a Virtual Reality Simulator: Assessment of Learning Curve. J. Minim. Invasive Gynecol. 2013, 20, 775–782. [Google Scholar] [CrossRef]
- Kulcsar, Z.; O’Mahony, E.; Lovquist, E.; Aboulafia, A.; Sabova, D.; Ghori, K.; Iohom, G.; Shorten, G. Preliminary evaluation of a virtual reality-based simulator for learning spinal anesthesia. J. Clin. Anesth. 2013, 25, 98–105. [Google Scholar] [CrossRef] [PubMed]
- Mok, T.-N.; Chen, J.Y.; Pan, J.H.; Ming, W.K.; He, Q.Y.; Sin, T.H.; Deng, J.L.; Li, J.R.; Zha, Z.Z. Use of a Virtual Reality Simulator for Tendon Repair Training: Randomized Controlled Trial. JMIR Serious Games 2021, 9, e27544. [Google Scholar] [CrossRef] [PubMed]
- Brady, A.-M. Assessment of learning with multiple-choice questions. Nurse Educ. Pract. 2005, 5, 238–242. [Google Scholar] [CrossRef] [PubMed]
- Gutierrez, F.; Pierce, J.; Vergara, V.; Coulter, R.; Saland, L.; Caudell, T.; Goldsmith, T.; Alverson, D. The impact of the degree of immersion upon learning performance in virtual reality simulations for medical education. J. Investig. Med. 2007, 55, S91. [Google Scholar] [CrossRef] [Green Version]
- Ebert, J.; Tutschek, B. Virtual reality objects improve learning efficiency and retention of diagnostic ability in fetal ultrasound. Ultrasound Obstet. Gynecol. 2019, 53, 525–528. [Google Scholar] [CrossRef] [PubMed]
- Lesch, H.; Johnson, E.; Peters, J.; Cendan, J.C. VR Simulation Leads to Enhanced Procedural Confidence for Surgical Trainees. J. Surg. Educ. 2020, 77, 213–218. [Google Scholar] [CrossRef] [PubMed]
- Galvez, R.; Wallon, R.C.; Shackelford, L.; Amos, J.R.; Rowen, J.L. Use of Virtual Reality to Educate Undergraduate Medical Students on Cardiac Peripheral and Collateral Circulation. Med. Sci. Educ. 2021, 31, 19–22. [Google Scholar] [CrossRef] [PubMed]
- Maresky, H.S.; Oikonomou, A.; Ali, I.; Ditkofsky, N.; Pakkal, M.; Ballyk, B. Virtual Reality and Cardiac Anatomy: Exploring Immersive Three-Dimensional Cardiac Imaging, A Pilot Study in Undergraduate Medical Anatomy Education. Clin. Anat. 2019, 32, 238–243. [Google Scholar] [CrossRef]
- Zackoff, M.W.; Real, F.J.; Sahay, R.D.; Fei, L.; Guiot, A.; Lehmann, C.; Tegtmeyer, K.; Klein, M. Impact of an Immersive Virtual Reality Curriculum on Medical Students’ Clinical Assessment of Infants With Respiratory Distress*. Pediatr. Crit. Care Med. 2020, 21, 477–485. [Google Scholar] [CrossRef] [PubMed]
- Gopal, M.; Skobodzinski, A.A.; Sterbling, H.M.; Rao, S.R.; LaChapelle, C.; Suzuki, K.; Litle, V.R. Bronchoscopy Simulation Training as a Tool in Medical School Education. Ann. Thorac. Surg. 2018, 106, 280–286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Connor, M.; Stowe, J.; Potocnik, J.; Giannotti, N.; Murphy, S.; Rainford, L. 3D virtual reality simulation in radiography education: The students’ experience. Radiography 2021, 27, 208–214. [Google Scholar] [CrossRef] [PubMed]
- Atli, K.; Selman, W.; Ray, A. A Comprehensive Multicomponent Neurosurgical Course with use of Virtual Reality: Modernizing the Medical Classroom. J. Surg. Educ. 2021, 78, 1350–1356. [Google Scholar] [CrossRef] [PubMed]
- Zackoff, M.W.; Young, D.; Sahay, R.D.; Fei, L.; Real, F.J.; Guiot, A.; Lehmann, C.; Klein, M. Establishing Objective Measures of Clinical Competence in Undergraduate Medical Education Through Immersive Virtual Reality. Acad. Pediatr. 2020, 21, 575–579. [Google Scholar] [CrossRef] [PubMed]
- Wilson, G.F.; Russell, C.A. Real-time assessment of mental workload using psychophysiological measures and artificial neural networks. Hum. Factors 2003, 45, 635–644. [Google Scholar] [CrossRef] [PubMed]
- Yu, P.; Pan, J.J.; Wang, Z.X.; Shen, Y.; Wang, L.L.; Li, J.L.; Hao, A.M.; Wang, H.P. Cognitive Load/flow and Performance in Virtual Reality Simulation Training of Laparoscopic Surgery. In Proceedings of the 2021 IEEE Conference on Virtual Reality and 3D User Interfaces Abstracts and Workshops (VRW 2021), Lisbon, Portugal, 27 March–1 April 2021; pp. 468–469. [Google Scholar]
- Mariana, F.P.; Damian, E.T.; Antonio, N.F.P.; Nuria, P.A.; Joaquin, C.M.J.; Rafael, M.R.; Joaquin, G.C.A.; Manuel, P.R.; Laura, J.R. Comparative study of a simulated incident with multiple victims and immersive virtual reality. Nurse Educ. Today 2018, 71, 48–53. [Google Scholar] [CrossRef]
- Mills, B.; Dyks, P.; Hansen, S.; Miles, A.; Rankin, T.; Hopper, L.; Brook, L.; Bartlett, D. Virtual Reality Triage Training Can Provide Comparable Simulation Efficacy for Paramedicine Students Compared to Live Simulation-Based Scenarios. Prehospital Emerg. Care 2020, 24, 525–536. [Google Scholar] [CrossRef]
- Kotranza, A.; Lind, D.S.; Lok, B. Real-Time Evaluation and Visualization of Learner Performance in a Mixed-Reality Environment for Clinical Breast Examination. IEEE Trans. Vis. Comput. Graph. 2012, 18, 1101–1114. [Google Scholar] [CrossRef]
- Gierwialo, R.; Witkowski, M.; Kosieradzki, M.; Lisik, W.; Groszkowski, L.; Sitnik, R. Medical Augmented-Reality Visualizer for Surgical Training and Education in Medicine. Appl. Sci.-Basel 2019, 9, 2732. [Google Scholar] [CrossRef] [Green Version]
- Peden, R.G.; Mercer, R.; Tatham, A.J. The use of head-mounted display eyeglasses for teaching surgical skills: A prospective randomised study. Int. J. Surg. 2016, 34, 169–173. [Google Scholar] [CrossRef] [PubMed]
- Choueib, S.; McGarry, C.; Jaeger, M.; Ungi, T.; Janssen, N.; Fichtinger, G.; Patterson, L. Assessment of skill translation of intrathecal needle insertion using real-time needle tracking with an augmented reality display. In Proceedings of the Medical Imaging Conference—Image-Guided Procedures, Robotic Interventions, and Modeling, Houston, TX, USA, 16–19 February 2020. [Google Scholar]
- Weeks, J.K.; Pakpoor, J.; Park, B.J.; Robinson, N.J.; Rubinstein, N.A.; Prouty, S.M.; Nachiappan, A.C. Harnessing Augmented Reality and CT to Teach First-Year Medical Students Head and Neck Anatomy. Acad. Radiol. 2021, 28, 871–876. [Google Scholar] [CrossRef] [PubMed]
- Pickering, J.D.; Panagiotis, A.; Ntakakis, G.; Athanassiou, A.; Babatsikos, E.; Bamidis, P.D. Assessing the difference in learning gain between a mixed reality application and drawing screencasts in neuroanatomy. Anat. Sci. Educ. 2022, 15, 628–635. [Google Scholar] [CrossRef] [PubMed]
- Robinson, B.L.; Mitchell, T.R.; Brenseke, B.M. Evaluating the Use of Mixed Reality to Teach Gross and Microscopic Respiratory Anatomy. Med. Sci. Educ. 2020, 30, 1745–1748. [Google Scholar] [CrossRef] [PubMed]
- Bangor, A.; Kortum, P.T.; Miller, J.T. An Empirical Evaluation of the System Usability Scale. Int. J. Hum.-Comput. Interact. 2008, 24, 574–594. [Google Scholar] [CrossRef]
- Vlachogianni, P.; Tselios, N. Perceived usability evaluation of educational technology using the System Usability Scale (SUS): A systematic review. J. Res. Technol. Educ. 2021, 54, 1–18. [Google Scholar] [CrossRef]
- Schoeb, D.S.; Schwarz, J.; Hein, S.; Schlager, D.; Pohlmann, P.F.; Frankenschmidt, A.; Gratzke, C.; Miernik, A. Mixed reality for teaching catheter placement to medical students: A randomized single-blinded, prospective trial. BMC Med. Educ. 2020, 20, 510. [Google Scholar] [CrossRef]
- Anderson, M.; Guido-Sanz, F.; Diaz, D.A.; Lok, B.; Stuart, J.; Akinnola, I.; Welch, G. Augmented Reality in Nurse Practitioner Education: Using a Triage Scenario to Pilot Technology Usability and Effectiveness. Clin. Simul. Nurs. 2021, 54, 105–112. [Google Scholar] [CrossRef]
- Wang, C.; Daniel, B.K.; Asil, M.; Khwaounjoo, P.; Cakmak, Y.O. A Randomised Control Trial and Comparative Analysis of Multi-Dimensional Learning Tools in Anatomy. Sci. Rep. 2020, 10, 6120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoganathan, S.; Finch, D.A.; Parkin, E.; Pollard, J. 360° virtual reality video for the acquisition of knot tying skills: A randomised controlled trial. Int. J. Surg. 2018, 54, 24–27. [Google Scholar] [CrossRef] [PubMed]
- Lowe, J.; Peng, C.; Winstead-Derlega, C.; Curtis, H. 360 virtual reality pediatric mass casualty incident: A cross sectional observational study of triage and out-of-hospital intervention accuracy at a national conference. J. Am. Coll. Emerg. Physicians Open 2020, 1, 974–980. [Google Scholar] [CrossRef] [PubMed]
- Sultan, L.; Abuznadah, W.; Al-Jifree, H.; Khan, M.A.; Alsaywid, B.; Ashour, F. An Experimental Study On Usefulness Of Virtual Reality 360 degrees In Undergraduate Medical Education. Adv. Med. Educ. Pract. 2019, 10, 907–916. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McLaughlin, N.; Rogers, J.; D’Arcy, J.; Gormley, G. ‘Sorry doctor …. I didn’t hear that …. ’: Phenomenological analysis of medical students’ experiences of simulated hearing impairment through virtual reality. BMJ Simul. Technol. Enhanc. Learn. 2021, 7, 207–215. [Google Scholar] [CrossRef] [PubMed]
- Giordano, N.A.; Whitney, C.E.; Axson, S.A.; Cassidy, K.; Rosado, E.; Hoyt-Brennan, A.M. A pilot study to compare virtual reality to hybrid simulation for opioid-related overdose and naloxone training. Nurse Educ. Today 2020, 88, 104365. [Google Scholar] [CrossRef]
- Arents, V.; de Groot, P.C.M.; Struben, V.M.D.; van Stralen, K.J. Use of 360 degrees virtual reality video in medical obstetrical education: A quasi-experimental design. BMC Med. Educ. 2021, 21, 202. [Google Scholar] [CrossRef]
- Sankaran, N.K.; Nisar, H.J.; Zhang, J.; Formella, K.; Amos, J.; Barker, L.T.; Vozenilek, J.A.; LaValle, S.M.; Kesavadas, T. Efficacy Study on Interactive Mixed Reality (IMR) Software with Sepsis Prevention Medical Education. In Proceedings of the 26th IEEE Conference on Virtual Reality and 3D User Interfaces (VR), Osaka, Japan, 23–27 March 2019; pp. 664–670. [Google Scholar]
- Birbara, N.S.; Pather, N. Instructional Design of Virtual Learning Resources for Anatomy Education. In Biomedical Visualisation; Springer: Berlin/Heidelberg, Germany, 2021; Volume 9, pp. 75–110. [Google Scholar]
- Aebersold, M.; Tschannen, D.; Bathish, A. Innovative Simulation Strategies in Education. Nurs. Res. Pract. 2012, 2012, 765212. [Google Scholar] [CrossRef] [Green Version]
- Andersen, S.A.W.; Mikkelsen, P.T.; Konge, L.; Caye-Thomasen, P.; Sorensen, M.S. Cognitive load in distributed and massed practice in virtual reality mastoidectomy simulation. Laryngoscope 2016, 126, E74–E79. [Google Scholar] [CrossRef]
- Chiu, H.-Y.; Kang, Y.-N.; Wang, W.-L.; Chen, C.-C.; Hsu, W.; Tseng, M.-F.; Wei, P.-L. The Role of Active Engagement of Peer Observation in the Acquisition of Surgical Skills in Virtual Reality Tasks for Novices. J. Surg. Educ. 2019, 76, 1655–1662. [Google Scholar] [CrossRef] [PubMed]
- Cone, D.C.; Serra, J.; Kurland, L. Comparison of the SALT and Smart triage systems using a virtual reality simulator with paramedic students. Eur. J. Emerg. Med. 2011, 18, 314–321. [Google Scholar] [CrossRef]
- De Faria, J.W.V.; Teixeira, M.J.; Sousa Junior, L.d.M.; Otoch, J.P.; Figueiredo, E.G. Virtual and stereoscopic anatomy: When virtual reality meets medical education. J. Neurosurg. 2016, 125, 1105–1111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Du, Y.-C.; Fan, S.-C.; Yang, L.-C. The impact of multi-person virtual reality competitive learning on anatomy education: A randomized controlled study. BMC Med. Educ. 2020, 20, 343. [Google Scholar] [CrossRef]
- Gockel, I.; Hakman, P.; Beardi, J.; Schutz, M.; Heinrichs, W.; Messow, C.M.; Junginger, T. New perspectives in laparoscopic simulation: From Students’ Skills Lab to stress evaluation. Zent. Fur Chir. 2008, 133, 244–249. [Google Scholar] [CrossRef] [PubMed]
- Henssen, D.J.H.A.; van den Heuvel, L.; De Jong, G.; Vorstenbosch, M.; Van Walsum, A.M.V.; Van den Hurk, M.M.; Kooloos, J.G.M.; Bartels, R. Neuroanatomy Learning: Augmented Reality vs. Cross-Sections. Anat. Sci. Educ. 2020, 13, 350–362. [Google Scholar] [CrossRef] [PubMed]
- Hu, K.-C.; Salcedo, D.; Kang, Y.-N.; Lin, C.-W.; Hsu, C.-W.; Cheng, C.-Y.; Suk, F.-M.; Huang, W.-C. Impact of virtual reality anatomy training on ultrasound competency development: A randomized controlled trial. PLoS ONE 2020, 15, e0242731. [Google Scholar] [CrossRef] [PubMed]
- Ijgosse, W.M.; van Goor, H.; Luursema, J.-M. Saving robots improves laparoscopic performance: Transfer of skills from a serious game to a virtual reality simulator. Surg. Endosc. Other Interv. Tech. 2018, 32, 3192–3199. [Google Scholar] [CrossRef]
- Johannesson, E.; Silen, C.; Kvist, J.; Hult, H. Students’ experiences of learning manual clinical skills through simulation. Adv. Health Sci. Educ. 2013, 18, 99–114. [Google Scholar] [CrossRef] [Green Version]
- Jungmann, E.; Gockel, I.; Hecht, H.; Kuhr, K.; Rasanen, J.; Sihvo, E.; Lang, H. Impact of Perceptual Ability and Mental Imagery Training on Simulated Laparoscopic Knot-Tying in Surgical Novices Using a Nissen Fundoplication Model. Scand. J. Surg. 2011, 100, 78–85. [Google Scholar] [CrossRef] [Green Version]
- Keskitalo, T. Students’ expectations of the learning process in virtual reality and simulation-based learning environments. Australas. J. Educ. Technol. 2012, 28, 841–856. [Google Scholar] [CrossRef] [Green Version]
- Kowalewski, K.-F.; Hendrie, J.D.; Schmidt, M.W.; Proctor, T.; Paul, S.; Garrow, C.R.; Kenngott, H.G.; Muller-Stich, B.P.; Nickel, F. Validation of the mobile serious game application Touch Surgery (TM) for cognitive training and assessment of laparoscopic cholecystectomy. Surg. Endosc. Other Interv. Tech. 2017, 31, 4058–4066. [Google Scholar] [CrossRef] [PubMed]
- Kucuk, S.; Kapakin, S.; Goktas, Y. Learning Anatomy via Mobile Augmented Reality: Effects on Achievement and Cognitive Load. Anat. Sci. Educ. 2016, 9, 411–421. [Google Scholar] [CrossRef]
- Liaw, S.Y.; Ooi, S.W.; Bin Rusli, K.D.; Lau, T.C.; San Tam, W.W.; Chua, W.L. Nurse-Physician Communication Team Training in Virtual Reality Versus Live Simulations: Randomized Controlled Trial on Team Communication and Teamwork Attitudes. J. Med. Internet Res. 2020, 22, e17279. [Google Scholar] [CrossRef] [PubMed]
- Macnamara, A.F.; Bird, K.; Rigby, A.; Sathyapalan, T.; Hepburn, D. High-fidelity simulation and virtual reality: An evaluation of medical students’ experiences. BMJ Simul. Technol. Enhanc. Learn. 2021, 7, 528–535. [Google Scholar] [CrossRef]
- Makransky, G.; Petersen, G.B. Investigating the process of learning with desktop virtual reality: A structural equation modeling approach. Comput. Educ. 2019, 134, 15–30. [Google Scholar] [CrossRef]
- Noll, C.; von Jan, U.; Raap, U.; Albrecht, U.-V. Mobile Augmented Reality as a Feature for Self-Oriented, Blended Learning in Medicine: Randomized Controlled Trial. JMIR Mhealth Uhealth 2017, 5, e139. [Google Scholar] [CrossRef]
- Rahm, S.; Wieser, K.; Wicki, I.; Holenstein, L.; Fucentese, S.F.; Gerber, C. Performance of medical students on a virtual reality simulator for knee arthroscopy: An analysis of learning curves and predictors of performance. BMC Surg. 2016, 16, 14. [Google Scholar] [CrossRef] [Green Version]
- Rim, D.; Shin, H. Development and Assessment of a Multi-User Virtual Environment Nursing Simulation Program: A Mixed Methods Research Study. Clin. Simul. Nurs. 2022, 62, 31–41. [Google Scholar] [CrossRef]
- Rosas-Paredes, K.; Esquicha-Tejada, J.; Manrique Morante, H.; del Carpio Toia, A.M. Usability and Learning Environment of a Virtual Reality Simulator for Laparoscopic Surgery Training. Int. J. Adv. Comput. Sci. Appl. 2021, 12, 760–768. [Google Scholar] [CrossRef]
- Samosorn, A.B.; Gilbert, G.E.; Bauman, E.B.; Khine, J.; McGonigle, D. Teaching Airway Insertion Skills to Nursing Faculty and Students Using Virtual Reality: A Pilot Study. Clin. Simul. Nurs. 2020, 39, 18–26. [Google Scholar] [CrossRef]
- Stepan, K.; Zeiger, J.; Hanchuk, S.; Del Signore, A.; Shrivastava, R.; Govindaraj, S.; Iloreta, A. Immersive virtual reality as a teaching tool for neuroanatomy. Int. Forum Allergy Rhinol. 2017, 7, 1006–1013. [Google Scholar] [CrossRef]
- Uemura, M.; Tomikawa, M.; Nagao, Y.; Yamashita, N.; Kumashiro, R.; Tsutsumi, N.; Ohuchida, K.; Ieiri, S.; Ohdaira, T.; Hashizume, M.; et al. Significance of metacognitive skills in laparoscopic surgery assessed by essential task simulation. Minim. Invasive Ther. Allied Technol. 2014, 23, 165–172. [Google Scholar] [CrossRef] [PubMed]
- Vincent, D.S.; Sherstyuk, A.; Burgess, L.; Connolly, K.K. Teaching Mass Casualty Triage Skills Using Immersive Three-dimensional Virtual Reality. Acad. Emerg. Med. 2008, 15, 1160–1165. [Google Scholar] [CrossRef] [PubMed]
- Windsor, J.A.; Diener, S.; Zoha, F. Learning style and laparoscopic experience in psychomotor skill performance using a virtual reality surgical simulator. Am. J. Surg. 2008, 195, 837–842. [Google Scholar] [CrossRef] [PubMed]
- Wainman, B.; Pukas, G.; Wolak, L.; Mohanraj, S.; Lamb, J.; Norman, G.R. The Critical Role of Stereopsis in Virtual and Mixed Reality Learning Environments. Anat. Sci. Educ. 2020, 13, 398–405. [Google Scholar] [CrossRef] [PubMed]
- Wainman, B.; Aggarwal, A.; Birk, S.K.; Gill, J.S.; Hass, K.S.; Fenesi, B. Virtual Dissection: An Interactive Anatomy Learning Tool. Anat. Sci. Educ. 2021, 14, 788–798. [Google Scholar] [CrossRef] [PubMed]
- Bric, J.; Connolly, M.; Kastenmeier, A.; Goldblatt, M.; Gould, J.C. Proficiency training on a virtual reality robotic surgical skills curriculum. Surg. Endosc. Other Interv. Tech. 2014, 28, 3343–3348. [Google Scholar] [CrossRef] [PubMed]
- Simpson, E.J. The Classification of Educational Objectives, Psychomotor Domain; University of Illinois: Champaign, IL, USA, 1966. [Google Scholar]
- Cierniak, G.; Scheiter, K.; Gerjets, P. Explaining the split-attention effect: Is the reduction of extraneous cognitive load accompanied by an increase in germane cognitive load? Comput. Hum. Behav. 2009, 25, 315–324. [Google Scholar] [CrossRef]
- Ryan, R.M.; Mims, V.; Koestner, R. Relation of reward contingency and interpersonal context to intrinsic motivation: A review and test using cognitive evaluation theory. J. Personal. Soc. Psychol. 1983, 45, 736–750. [Google Scholar] [CrossRef]
- Witmer, B.G.; Singer, M.J. Measuring Presence in Virtual Environments: A Presence Questionnaire. Presence: Teleoperators Virtual Environ. 1998, 7, 225–240. [Google Scholar] [CrossRef]
- Makransky, G.; Lilleholt, L.; Aaby, A. Development and validation of the Multimodal Presence Scale for virtual reality environments: A confirmatory factor analysis and item response theory approach. Comput. Hum. Behav. 2017, 72, 276–285. [Google Scholar] [CrossRef]
- Servotte, J.-C.; Goosse, M.; Campbell, S.H.; Dardenne, N.; Pilote, B.; Simoneau, I.L.; Guillaume, M.; Bragard, I.; Ghuysen, A. Virtual Reality Experience: Immersion, Sense of Presence, and Cybersickness. Clin. Simul. Nurs. 2020, 38, 35–43. [Google Scholar] [CrossRef] [Green Version]
- Anders Ericsson, K. Deliberate Practice and Acquisition of Expert Performance: A General Overview. Acad. Emerg. Med. 2008, 15, 988–994. [Google Scholar] [CrossRef]
- Petrosoniak, A.; Lu, M.; Gray, S.; Hicks, C.; Sherbino, J.; McGowan, M.; Monteiro, S. Perfecting practice: A protocol for assessing simulation-based mastery learning and deliberate practice versus self-guided practice for bougie-assisted cricothyroidotomy performance. BMC Med. Educ. 2019, 19, 100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andersen, S.A.; Konge, L.; Caye-Thomasen, P.; Sorensen, M.S.; Andersen, S.A.; Konge, L.; Caye-Thomasen, P.; Sorensen, M.S. Learning Curves of Virtual Mastoidectomy in Distributed and Massed Practice. JAMA Otolaryngol.-Head Neck Surg. 2015, 141, 913–918. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cisse, C.; Angioi, K.; Luc, A.; Berrod, J.-P.; Conart, J.-B. EYESI surgical simulator: Validity evidence of the vitreoretinal modules. ACTA Ophthalmol. 2019, 97, E277–E282. [Google Scholar] [CrossRef] [PubMed]
- Lia, H.; Paulin, G.; Yeo, C.T.; Andrews, J.; Yi, N.; Haq, H.; Emmanue, S.; Ludig, K.; Keri, Z.; Lasso, A.; et al. HoloLens in Suturing Training. In Proceedings of the Medical Imaging 2018: Image-Guided Procedures, Robotic Interventions, and Modeling, Houston, TX, USA, 10–15 February 2018; p. 10576. [Google Scholar]
- Berg, H.; Steinsbekk, A. The effect of self-practicing systematic clinical observations in a multiplayer, immersive, interactive virtual reality application versus physical equipment: A randomized controlled trial. Adv. Health Sci. Educ. 2021, 26, 667–682. [Google Scholar] [CrossRef]
- Pears, M.; Konstantinidis, S. The Future of Immersive Technology in Global Surgery Education. Indian J. Surg. 2022, 84, 281–285. [Google Scholar] [CrossRef] [PubMed]
- Ryan, G.V.; Callaghan, S.; Rafferty, A.; Higgins, M.F.; Mangina, E.; McAuliffe, F. Learning Outcomes of Immersive Technologies in Health Care Student Education: Systematic Review of the Literature. J Med. Internet Res. 2022, 24, e30082. [Google Scholar] [CrossRef] [PubMed]
- Carney, P.A.; Nierenberg, D.W.; Pipas, C.F.; Brooks, W.B.; Stukel, T.A.; Keller, A.M. Educational EpidemiologyApplying Population-Based Design and Analytic Approaches to Study Medical Education. JAMA 2004, 292, 1044–1050. [Google Scholar] [CrossRef] [PubMed]
- Barrie, M.; Socha, J.J.; Mansour, L.; Patterson, E.S. Mixed Reality in Medical Education: A Narrative Literature Review. In Proceedings of the International Symposium on Human Factors and Ergonomics in Health Care, Chicago, IL, USA, 24–27 March 2019; Volume 8, pp. 28–32. [Google Scholar] [CrossRef]
- Beckman, T.J.; Cook, D.A.; Mandrekar, J.N. What is the validity evidence for assessments of clinical teaching? J. Gen. Intern. Med. 2005, 20, 1159–1164. [Google Scholar] [CrossRef] [PubMed]
- Golnari, P.; Sodagari, F.; Baradaran, H.R. Quality of published Iranian medical education research studies: A systematic review. Med. J. Islam. Repub. Iran 2014, 28, 79. [Google Scholar] [PubMed]
- All, A.; Castellar, E.P.N.; Van Looy, J. Assessing the effectiveness of digital game-based learning: Best practices. Comput. Educ. 2016, 92, 90–103. [Google Scholar] [CrossRef]
- Gorbanev, I.; Agudelo-Londoño, S.; González, R.A.; Cortes, A.; Pomares, A.; Delgadillo, V.; Yepes, F.J.; Muñoz, Ó. A systematic review of serious games in medical education: Quality of evidence and pedagogical strategy. Med. Educ. Online 2018, 23, 1438718. [Google Scholar] [CrossRef] [Green Version]
- McGaghie, W.C.; Issenberg, S.B.; Petrusa, E.R.; Scalese, R.J. Effect of practice on standardised learning outcomes in simulation-based medical education. Med. Educ. 2006, 40, 792–797. [Google Scholar] [CrossRef] [PubMed]
- Kirkpatrick, D.L.; Kirkpatrick, J.D. Implementing the Four Levels: A Practical Guide for Effective Evaluation of Training Programs; ReadHowYouWant.com, Limited: Sydney, Australia, 2009. [Google Scholar]
- Ritter, E.M.; McClusky, D.A.; Gallagher, A.G.; Enochsson, L.; Smith, C.D. Perceptual, visuospatial, and psychomotor abilities correlate with duration of training required on a virtual-reality flexible endoscopy simulator. Am. J. Surg. 2006, 192, 379–384. [Google Scholar] [CrossRef] [PubMed]
- Taubert, M.; Webber, L.; Hamilton, T.; Carr, M.; Harvey, M. Virtual reality videos used in undergraduate palliative and oncology medical teaching: Results of a pilot study. BMJ Support. Palliat. Care 2019, 9, 281–285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Messick, S. Validity of psychological assessment: Validation of inferences from persons’ responses and performances as scientific inquiry into score meaning. Am. Psychol. 1995, 50, 741–749. [Google Scholar] [CrossRef]
- Cook, D.A.; Hatala, R. Validation of educational assessments: A primer for simulation and beyond. Adv. Simul. 2016, 1, 31. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Exclusion Criteria | Rationale |
|---|---|
| Patient education | Study aims to explore HCP education |
| Use of new prototypes/designs/haptics | These papers focus on technological development |
| Reviews | Prior material was considered in background |
| Virtual patients or virtual learning environment studies | Falls outside MR scope for this study |
| VR or AR without user interaction | This review aimed to focus on immersive environments |
| Animal studies | Human participants only are relevant |
| Gamification without medical content | Serious gaming is within MR domain, however, there needs to be a medical focus for purpose of review |
| Non-medical | By definition this excluded vets, dentists, pharmacists, and optometrists |
| Theme Subtype | Number of Studies | Total Participants (Number of Qualified HCP) | Sample Size Range | Average Sample Size |
|---|---|---|---|---|
| VR | 163 | 7879 (568) | 5–289 | 98 |
| AR | 68 | 2520 (10) | 10–292 | 55 |
| 360 | 15 | 1028 (48) | 34–207 | 69 |
| Learning theory | 44 | 2342 (115) | 10–200 | 56 |
| Variables | Score VR | Score AR | Score 360 | Score Learning Theory | Instrument Validity Score VR | Instrument Validity Score AR | Instrument Validity Score 360 | Instrument Validity Score Learning Theory |
|---|---|---|---|---|---|---|---|---|
| Mean | 10.57 | 9.58 | 8.86 | 10.85 | 1.26 | 1.30 | 1.29 | 1.88 |
| Standard deviation | 2.33 | 3.17 | 2.66 | 2.03 | 1.42 | 1.50 | 1.54 | 1.40 |
| Standard error of mean | 0.18 | 0.47 | 0.71 | 0.31 | 0.11 | 0.22 | 0.41 | 0.22 |
| Upper 95% CL of mean | 10.93 | 10.52 | 10.39 | 11.48 | 1.48 | 1.75 | 2.18 | 2.32 |
| Lower 95% CL of mean | 10.21 | 8.63 | 7.32 | 10.21 | 1.03 | 0.86 | 0.40 | 1.44 |
| Maximum | 15.50 | 14.50 | 13.00 | 14.50 | 3.00 | 3.00 | 3.00 | 3.00 |
| Procedure/Objective Tool | No. | Learning Assessment Tool | No. | Subjective Measure | No. | Physical Measure | No. |
|---|---|---|---|---|---|---|---|
| Task performance | 72 | MCQ | 20 | User experience questionnaire | 4 | Heart rate | 2 |
| Global rating scale (GRS) | 12 | NASA TLX | 4 | System usability scale (SUS) | 3 | Cortisol levels | 1 |
| OSCE | 7 | Visual-spatial ability | 3 | Confidence rating | 3 | EEG | 1 |
| Objective score by an assessor | 4 | Cube subtest of standard intelligence test | 1 | Presence questionnaire | 3 | ||
| Objective structured assessment of technical skills (OSATS) | 3 | Intrinsic motivation inventory | 1 | Difficulty rating | 1 | ||
| Arthroscopic surgery skill evaluation tool (ASSET) | 2 | Learner evaluation questionnaire (LEQ) | 1 | Instructional materials motivation survey (IMMS) | 1 | ||
| Reaction time | 2 | Lasater clinical judgment rubric | 1 | Interprofessional socialization and valuing scale (ISVS) | 1 | ||
| Procedure checklist | 2 | Learning survey | 1 | iGroup presence questionnaire (IPQ) | 1 | ||
| Basic life support | 2 | Mental rotation test | 2 | Scale of experience | 1 | ||
| Bronchoscopy skills and tasks assessment tool (BSTAT) | 2 | Learning style (MIDAS) | 1 | Nursing anxiety and self-confidence | 1 | ||
| Cannulation score | 1 | Pictorial surface orientation test (PicSOr) | 1 | Serious gaming usability scale (SGUS) | 1 | ||
| Xray procedure score | 1 | Social validity questionnaire | 1 | Simulation design questionnaire | 1 | ||
| Neurological exam | 1 | Spatial orientation test | 1 | Student satisfaction | 1 | ||
| Cochlear implant assessment (CISAT) | 1 | Stress mental readiness form | 1 | VR experience survey | 1 | ||
| Score of communication | 1 | Students’ engagement in school four-dimensional scale | 1 | ||||
| Emergency medicine crisis resource management (EMCRM) | 1 | Technology acceptance questionnaire | 1 | ||||
| Modified Welling score | 1 | ||||||
| Total measures | 115 | 41 | 23 | 4 |
| Procedure/Objective Tool | No. | Learning Assessment Tool | No. | Subjective Measure | No. | Physical Measure | No. |
|---|---|---|---|---|---|---|---|
| Task performance | 7 | MCQ | 13 | System usability scale | 6 | EEG | 1 |
| OSCE | 3 | Mental rotation test | 2 | Usability questionnaire | 2 | ||
| Anesthetist non-technical skills (ANTS) | 1 | NASA TLX | 1 | AttrakDiff 2 usability score | 2 | ||
| Angle of hip surgery | 1 | Cambridge brain psychomotor test | 1 | Profile of mood states (POMs) | 2 | ||
| Global rating scale | 1 | The nine-point cognitive load scale | 1 | Subjective rating | 2 | ||
| Kakarla scale of EVD insertion | 1 | Simulation effectiveness Tool | 1 | Experience survey | 2 | ||
| Skill competency checklist | 1 | Overall perception of headset score | 1 | ||||
| Evaluating technology-enhanced learning materials (ETELM) | 1 | ||||||
| Attention/confidence with scale | 1 | ||||||
| Written feedback | 1 | ||||||
| Instructional measure of motivation survey | 1 | ||||||
| Total | 15 | 19 | 21 | 2 |
| Procedure/Objective Tool | No. | Learning Assessment Tool | No. | Subjective Measure | No. |
|---|---|---|---|---|---|
| Task performance | 1 | MCQ | 5 | System usability scale | 1 |
| Simple triage and rapid treatment protocol (START) | 1 | Communication accuracy | 1 | Engagement scores | 1 |
| NASA TLX | 1 | ||||
| Ease to learn | 1 | ||||
| Motivation and learning | 1 | ||||
| Task unrelated images of thoughts | 1 | ||||
| Total | 2 | 10 | 2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jacobs, C.; Foote, G.; Joiner, R.; Williams, M. A Narrative Review of Immersive Technology Enhanced Learning in Healthcare Education. Int. Med. Educ. 2022, 1, 43-72. https://doi.org/10.3390/ime1020008
Jacobs C, Foote G, Joiner R, Williams M. A Narrative Review of Immersive Technology Enhanced Learning in Healthcare Education. International Medical Education. 2022; 1(2):43-72. https://doi.org/10.3390/ime1020008
Chicago/Turabian StyleJacobs, Chris, Georgia Foote, Richard Joiner, and Michael Williams. 2022. "A Narrative Review of Immersive Technology Enhanced Learning in Healthcare Education" International Medical Education 1, no. 2: 43-72. https://doi.org/10.3390/ime1020008