1. Introduction
Endophthalmitis is a severe inflammation of the inner ocular tissues which could lead even to blindness. The causative agents (bacteria, fungi) enter to the eye from the environment (exogeneous origin, trauma-related or non-traumatic way i.e., medical intervention or keratitis) or spread hematogenously (endogenous endophthalmitis). [
1]. Bilateral endophthalmitis raises suspicion of endogenous origin. The well-known risk factors for hematogenous microbe spread include recent hospitalization, diabetes, uroinfection and long-indwelling catheter, liver or kidney failure, organ transplantation, immunosuppressive or immunodeficient conditions.
Fungal endophthalmitis severely threatens visual function. Its prognosis is worse than that from endophthalmitis of bacterial origin. Fungal endophthalmitis is more often reported from Asia, including India [
1,
2]. The incidence of fungal endophthalmitis is 8–18%, [
3]. High incidence (nearly 60%) has been reported in cases with intravenous drug abuse [
4]. Although the incidence of fungal endophthalmitis is lower than endophthalmitis of bacterial origin, its occurrence is probably underestimated and may increase due to the emerging use of multiple immunosuppressive agents, antibiotics and implants (such as indwelling catheters). The most common oculopathogenic fungi are aspergillus species (A. fumigatus, niger, nidulans, flavus), fusarium (F. equiseti, solani, moniliforme) and Candida (C. albicans) [
5].
Fungal endophthalmitis is often difficult to diagnose as the clinical picture is non-specific; it resembles chronic bacterial endophthalmitis. Fungi do not always grow in culture, histopathologic identification is challenging and fungal antibody tests may cross-react. Furthermore, in the absence of a global incidence report and randomized clinical trials, there are no universally accepted diagnostic and management protocols [
1,
2].
The aims of this report are to present a severe case of bilateral endogenous fungal endophthalmitis and to provide a short review of the current literature.
2. Case History
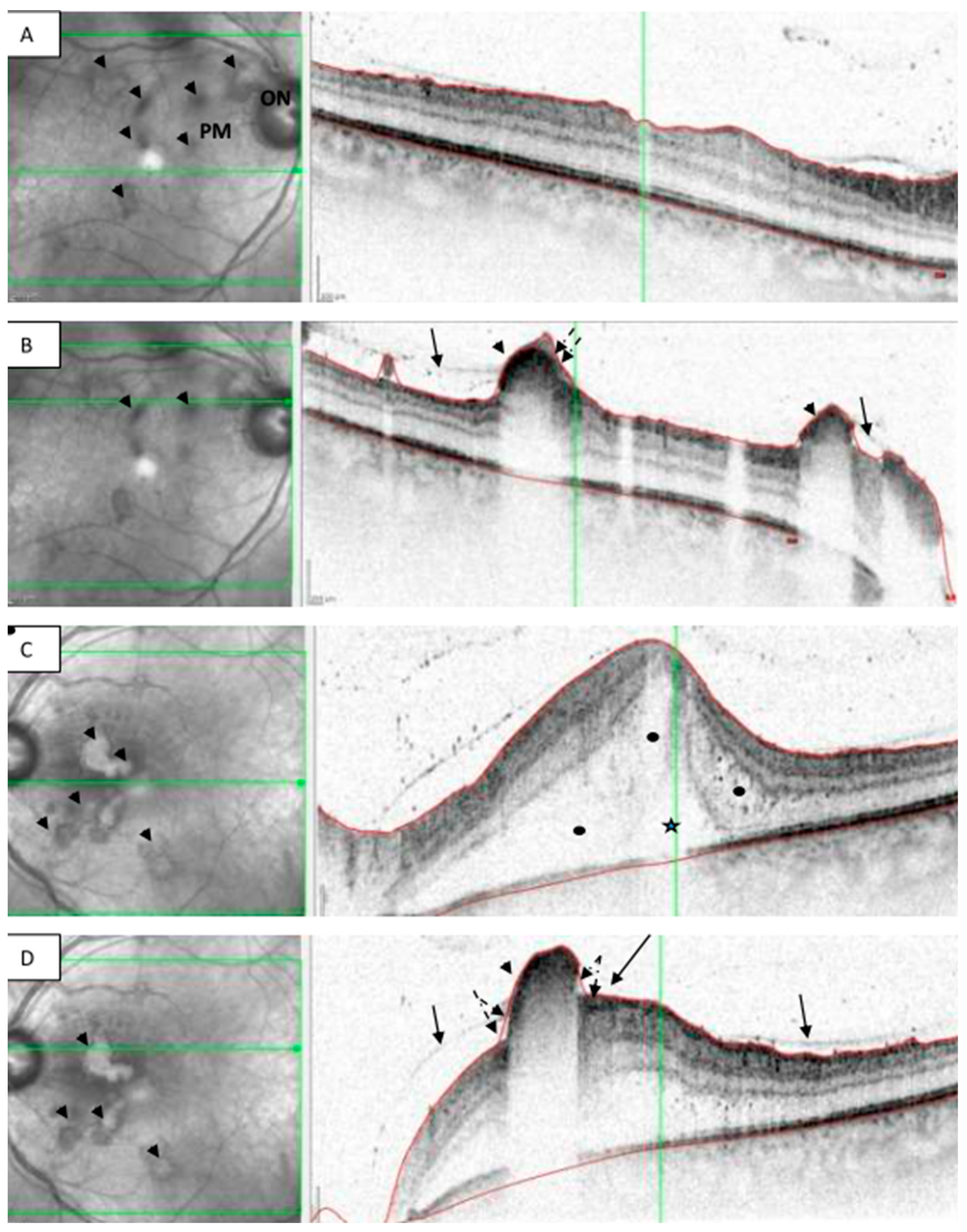
A 50-year-old male patient was referred to our department from a regional hospital due to bilateral blurred vision that had previously been diagnosed as panuveitis and a combined steroid-antibiotic eyedrop was initiated. On presentation, the best corrected visual acuity was 0.4 (Snellen chart) on the right eye and fingers counting at 1 m distance on the left eye. Slit-lamp examination showed mild conjunctival injection, tiny corneal precipitates and moderate flare in the anterior chambers. Fundus examination revealed faint red reflex with fluffy yellowish white vitreous and preretinal-retinal opacities in the papillomacular area. Ultrasonography B-scan showed hyperechoic vitreous debris and attached retina. Optical coherence scans suggested subhyaloidal or sub-ILM (internal limiting membrane) infiltrates in both eyes; no deep retinal invasion was detected. The macula was not involved in the right eye while in the left intra- and sub-retinal fluid were detected in the fovea (
Figure 1).
The patient’s general history included well-controlled type 2 diabetes and recurrent uroinfections due to urolithiasis. Eight months prior to the ocular symptoms, he received a double J catheter. After the catheter implantation he suffered from recurrent uroinfections with fever that were treated with broad spectrum antibiotics (cefuroxime and metronidazole). Fungal culture of urine revealed the presence of Candida albicans that showed resistance to azole derivates. Four weeks before the occurrence of endophthalmitis, the patient was hospitalized again in a urological unit due to high fever and increased inflammatory parameters (CRP 8.2 mg/L, ESR 61 mm/h). He received ciprofloxacin intravenously for 14 days and became afebrile and his general symptoms improved. At that time, microbiological urine tests did not yield any microorganisms.
We suspected fungal endophthalmitis of the endogenous origin in both eyes on the basis of the clinical picture and reviewing the patient’s medical reports on an infection with chronic indwelling J-catheter, the prolonged recurrent febrile condition and Candida albicans infection previously detected in the urine sample. We decided to perform a pars plana vitrectomy (PPV) on the left eye, that was in worst condition. The indications of a surgery were to collect a vitreous tap for microbiological tests, to eliminate the microbes and inflammatory cells from the vitreous and to administered empirically amphotericin-B and vancomycin intravitreal therapies. The patient was referred to the department of internal medicine for high dose intravenous antifungal and antibiotic treatment. Parenteral meropenem and anidulafungin were initiated.
After a few days, the patient’s best corrected visual acuity (BCVA) improved on the operated left eye to BCVA 0.2 and declined to BCVA 0.1 on the right eye. Therefore, we decided to also perform PPV on the right eye, with vitreous tapping, vancomycin infusion (1 mg in the BSS infusion) and intravitreal injection of amphotericin-B (5 μg/0.1 mL). During surgery, we realized that—fortunately—the whitish (presumably fungal) accumulations were only in the vitreous, no deep retinal infiltration was observed. We could separate and peel the posterior hyaloid from the macular area and the posterior pole easily. The investigation of the first vitreous tap from the left eye showed no microorganisms while Candida albicans was cultured from the second tap. Multiplex-PCR also excluded bacterial origin and toxoplasmosis. The flow cytometry of the vitreous sample showed a T-cell enriched reactive lymphoid infiltration. No malignant cells were detected. Hemoculture was negative. Meropenem therapy was continued until the repeated urine test proved persistent Candida albicans uroinfection with azole-susceptibility. The ongoing anidulafungin therapy was changed to oral fluconazole. The urologist explanted the catheters. The patient was admitted to an inpatient ward for 14 days.
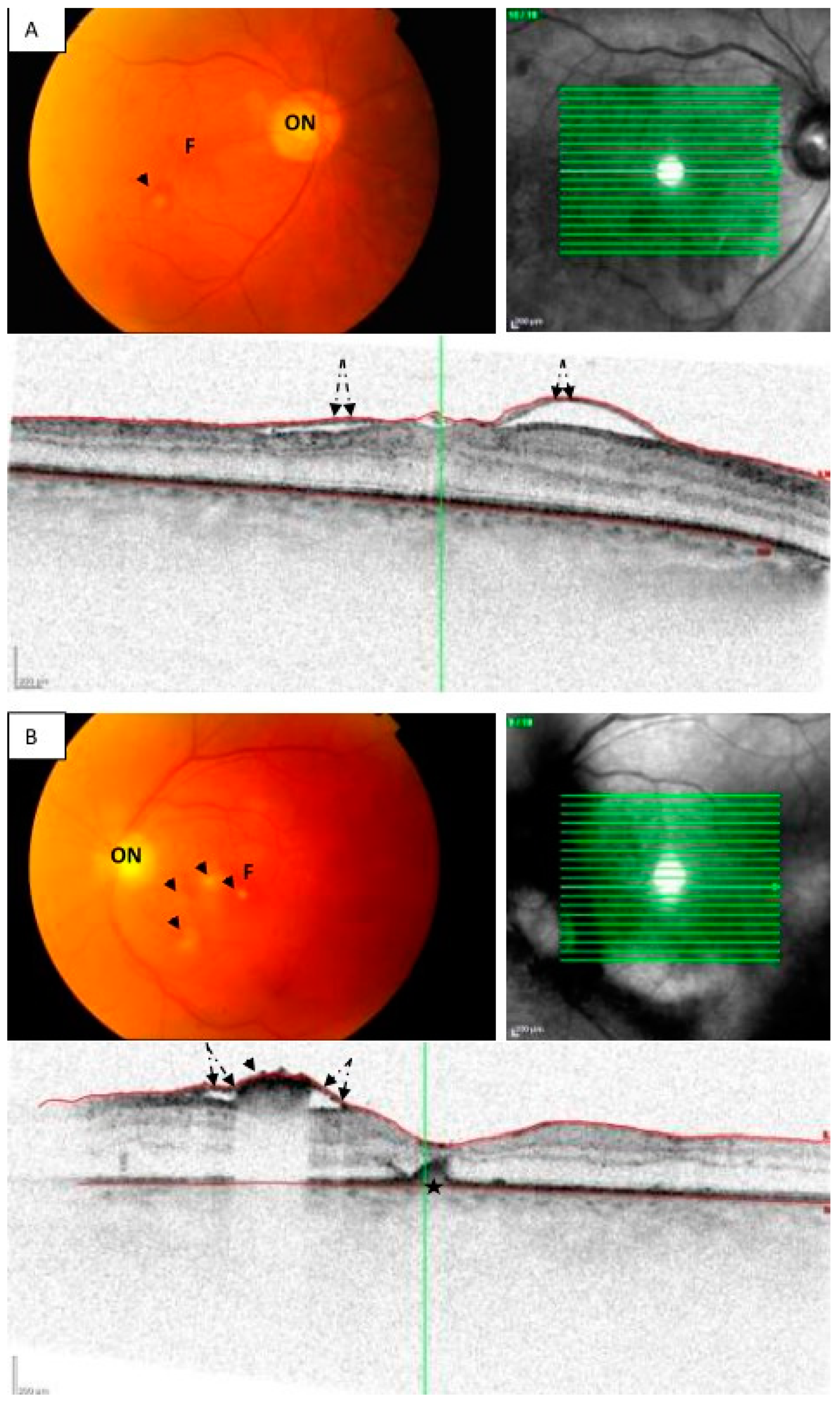
During the following 12 months, the patient’s visual acuity slowly improved on both eyes to 1.0 and the vitreous spaces resolved completely (
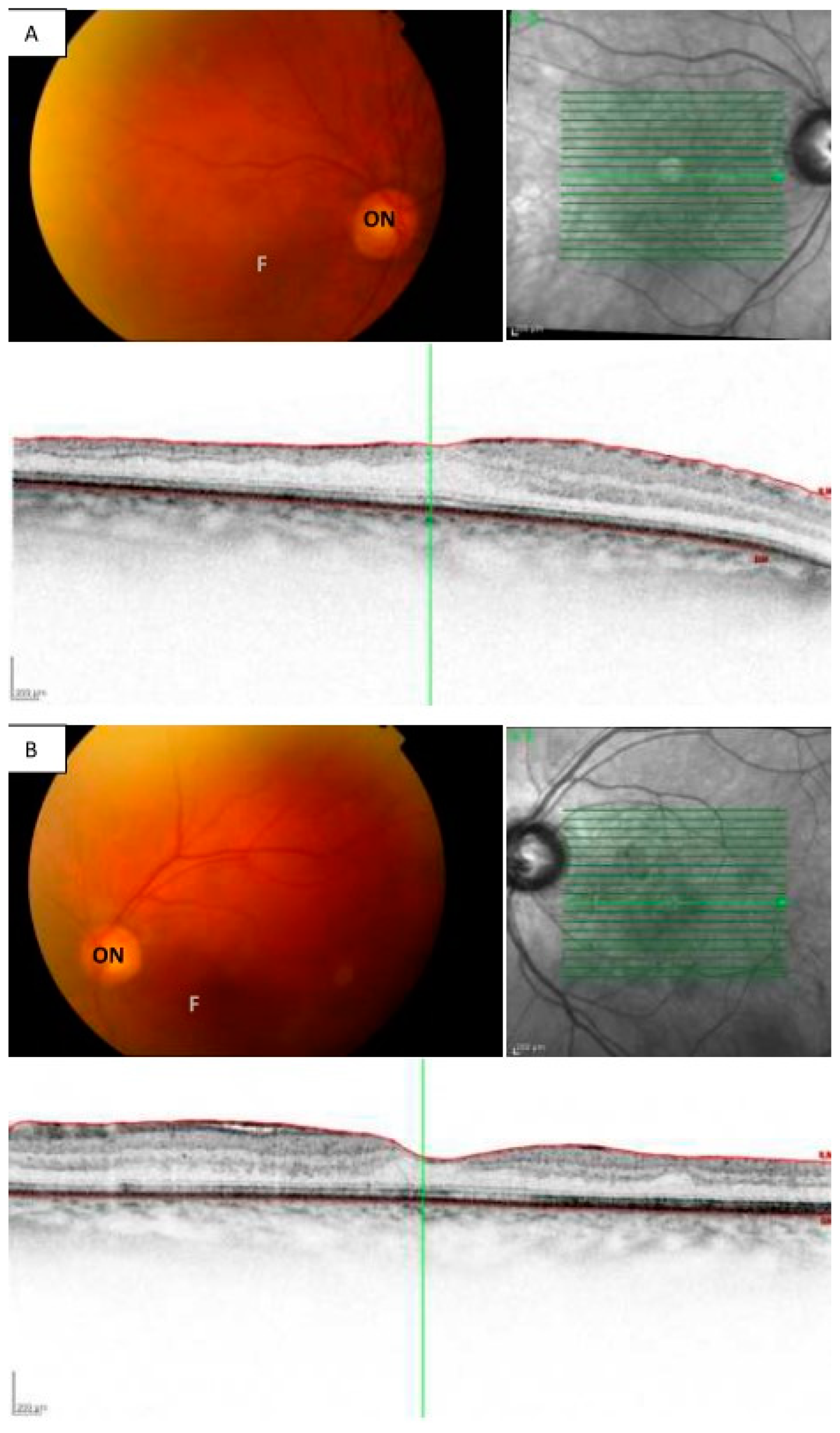
Figure 2). The follow-up occurred biweekly in the first month, and thereafter every 3 months. At the last visit the best corrected visual acuity of the right eye decreased to 0.7 due to nuclear cataract formation, the ocular slit lamp examination with fundus biomicroscopy did not show any signs of inflammation. No recurrent inflammation occurred and no additional intravitreal therapy was required (
Figure 3).
Patient’s medical records were analyzed retrospectively. Institutional Review Board approval and informed consent of the patient were obtained for all study protocols and publication (SE RKEB 194/2022).
3. Discussion
Fungal endophthalmitis is a potentially vision-threatening condition. Fungi are ubiquitous eukaryotic organisms. The pathogenesis of fungal disease involves an interplay between fungal virulence factors and host immune responses. Infection occurs when fungi accidentally penetrate barriers (such as intact skin and mucous membrane linings) or overcome the immunological defense mechanisms. Fungi also gain access to the host tissues by penetrating trauma or surgical interventions (cataract, glaucoma surgery, intravitreal injections). The severity of the disease depends on the size of the inoculum, the magnitude of tissue destruction, the ability of the fungi to multiply in tissues, and the immunologic status of the host [
2]. Both diagnosis and disease management can be challenging. In our case several risk factors could be identified, such as diabetes, urinary tract infection, prolonged and repeated use of broad-spectrum antibiotics and the presence of catheters within the body.
The clinical picture of fungal endophthalmitis has some particularity as it starts slowly with mild anterior segment signs resembling chronic bacterial endophthalmitis. Hematological disorders such as lymphomas or leukemias should also be considered due to a similar appearance. Hypopyon is observed less frequently than in bacterial infections. Fungal precipitates are usually whitish or slightly yellowish. Their localization could be characteristic for the mechanism of the infection as well as the type of the fungi. In postoperative cases, the infiltrates can surround the corneal wound. They can accumulate in the lens capsule and on the surface of the iris. With multimodal imaging such as optical coherence tomography (OCT), we can also localize their position according to the vitreous body, the retina or even the choroid. In endogenous Candida infection, some authors differentiate two forms based upon the OCT findings: one form covers intraretinal infiltration involving the internal retinal layers and vitreous/subhyaloidal infiltrates as the sites of invasion. The other type is a chorioretinal invasion, where the Candida penetrates through the pigment epithelium and causes large subretinal infiltrates [
6]. Others divide the cases into four groups: 1. subretinal macular type, 2. whole thickness retinitis with macular edema, 3. internal retinal layer affection, 4. infiltrates under the internal limiting membrane (ILM). In case of aspergillus infections mostly large subretinal infiltrates can be seen that are also called “aspergillomas” [
7,
8]. In our case the clinical picture also suggested an endogenous Candida infection as it was bilateral, there were only moderate signs of inflammation, no hypopyon was detected, and fluffy whitish infiltrates in the posterior part of the vitreous and in superficial retina layers were seen. The previous Candida positive urine culture in the patient’s medical report also supported the diagnosis.
Histopathology of formalin-fixed tissue and microbiology of ocular fluid are the two primary sources of laboratory confirmation. Histopathologically, the inflammatory cells are best seen by hematoxylin-eosin stains. The microbiological confirmation of fungi includes direct microscopy, culture, polymerase chain reaction (PCR) and DNA sequencing. Direct microscopy of the ocular specimen is rapid and is the most commonly used method. Culture prolonged testing sometimes takes 1–2 weeks. It should also be taken into account that a negative culture does not always exclude fungal infection. More recently, PCR detection of fungal species in vitreous specimens has shown high sensitivity and specificity, enabling the rapid diagnosis of fungal endophthalmitis [
9,
10]. Unfortunately, PCR does not provide resistance testing. In the absence of known fungemia, cultures of blood, catheter tips, wounds, and/or body fluids should be obtained. Cardiac imaging studies may be necessary to rule out the presence of septic emboli. Blood tests such as a QuantiFERON test for tuberculosis, special antibody tests for syphilis and toxoplasma, as well as angiotensin converting enzyme for sarcoidosis are helpful to rule out other uveitis entities. A critical review of the medical record is a crucial step. In our case, despite the negative direct microscopy and culture of the first vitreous tap and the unavailability of multiplex PCR for fungi at the time of surgery, the known risk factors (diabetes mellitus, J catheters), recurrent fever treated with broad spectrum antibiotics, a previous Candida positive urine culture helped us establish an accurate diagnosis and quickly initiate an adequate therapy.
Standard treatment protocols for fungal endophthalmitis are not available. Systemic antifungal drugs, vitrectomy and intravitreal antifungal injections are the three important interventions of proven efficacy. Maximum benefits are derived from the three interventions instituted together [
11,
12]. The continuation of systemic therapy is necessary for at least 4–6 weeks, depending on clinical signs with careful monitoring of liver and kidney functions. Traditionally, Candida infections are treated with azole-class drugs including fluconazole and voriconazole and non-azoles including amphotericin-B and caspofungin. Amphotericin-B has a well-studied side effect profile most notably nephrotoxicity, while voriconazole is associated with a greater risk of hepatotoxicity. Voriconazole or amphotericin-B can also be administered intravitreally. As a result of our experience with amphotericin-B, we preferred its usage during vitrectomy. We also considered voriconazole, which is reported safer, than amphotericin-B. The advantage of amphotericin-B is that it has a longer half-life after intravitreal injection [
13]. However, no fungi were collected from the first vitreous tap. On the basis of a previous resistance test from the urine culture, we started the systemic therapy with anidulafungin. The investigation of the second vitreous tap showed fluconazole-sensitive Candida albicans species. Fluconazole resistance is characteristic for non-Candida-albicans candida species [
14]. The previous resistance test was misleading and resulted in a difficult choice of therapy.
Early surgical intervention with pars plana vitrectomy is recommended for cases of fungal endophthalmitis with significant vitreous involvement if there is no significant improvement with intravitreal treatment [
11,
15,
16]. Sampling the vitreous at the time of vitrectomy can provide important culture and PCR data to identify the pathogen or rule out other inflammatory disorders such as intraocular lymphomas. Vitrectomy can be combined with the administration of the above-mentioned intravitreal agents. The outcome of early vitrectomy in combination with systemic antifungals could be favorable for cases of Candida and Aspergillus endophthalmitis [
16,
17,
18]. The half-life of antifungal agents administered directly into the vitreous at the time of vitrectomy is shortened and repeated administration may be necessary if there is evidence of persistent infection [
13,
18]. In our case, amphotericin-B was also administered intravitreously during the surgeries. Due to the favorable response with systemic therapy, we did not repeat it and only continued the oral antifungal therapy for 4 weeks. Intravitreal administration of amphotericin into both eyes at the same time could also have been an option but during the first surgery we applied it only empirically, and the retinotoxicity of amphotericin was also considered as a potential hazard.

{kind=link}
{kind=link}
{kind=link}


