
Feasibility of Using Oncology-Specific Electronic Health Record (EHR) Data to Emulate Clinical Trial Eligibility Criteria †
 ,
,
Abstract
:1. Introduction
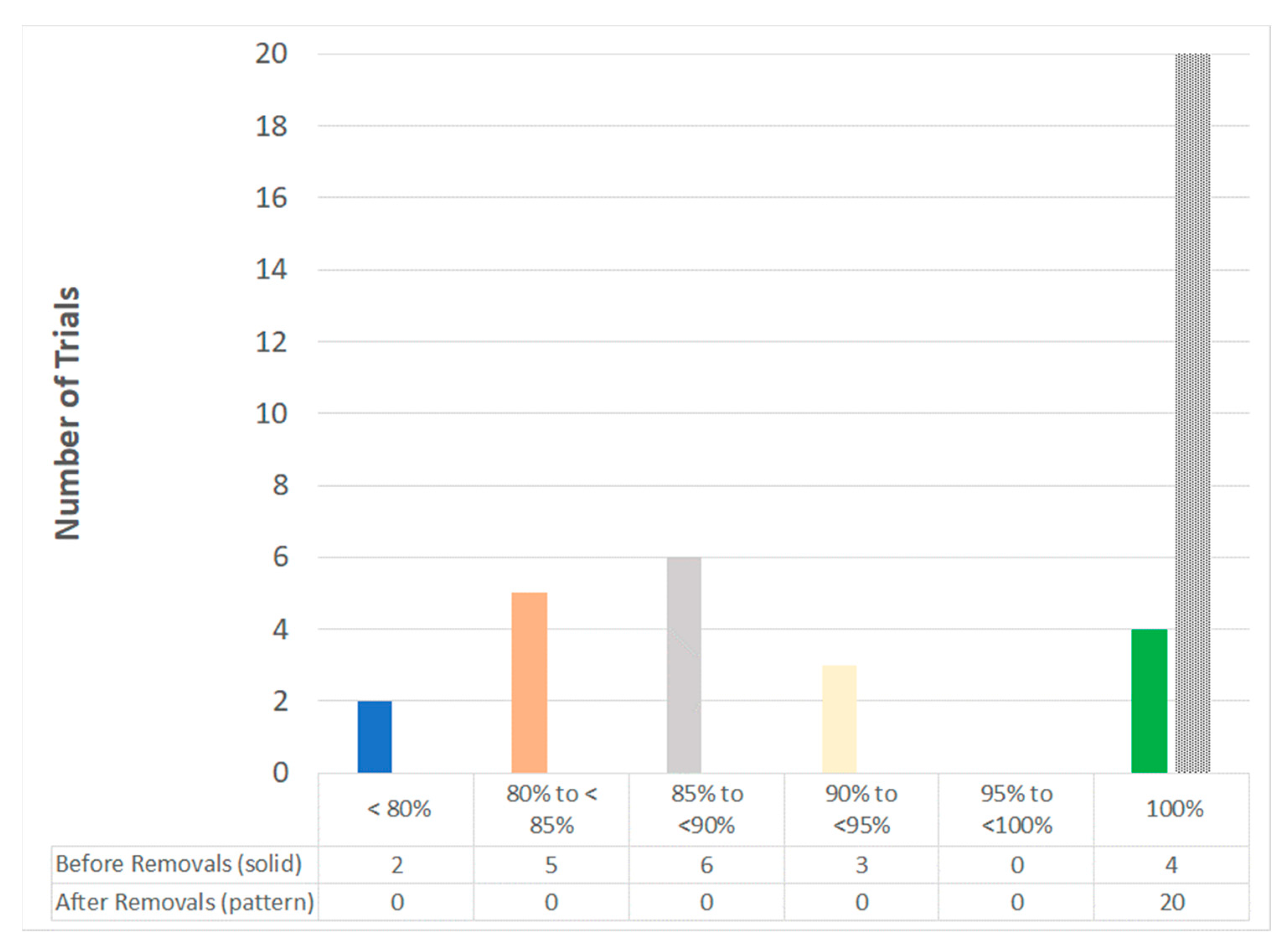
2. Results
3. Discussion
4. Methods
- Cancer-Related:
- ○
- Biomarker or Genetic Marker, Cancer Stage, Cancer Type, Measurable Disease, Metastasis, Other Cancer, Prior Cancer Treatments/Procedures, Progressive Disease.
- Comorbidity-Related:
- ○
- Cardiovascular Status, Comorbidity, Concomitant Medications, Contraindication, Drug–Drug/Food Interaction, Organ Function, Pulmonary Status.
- Demographic:
- ○
- Age and Sex.
- Functional Status:
- ○
- Hematological Status, Hepatic Status, HIV Status, Hypersensitivity, Immune Status, Infection, Ocular Status, Performance Status, Renal Status, Reproductive Status.
- Trial-Specific:
- ○
- Donor Status, Life Expectancy, Trial Operations.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- US Food and Drug Administration. Real-World Evidence. Real-World Data (RWD) and Real-World Evidence (RWE) Are Playing an Increasing Role in Health Care Decisions. Available online: https://www.fda.gov/science-research/science-and-research-special-topics/real-world-evidence (accessed on 5 July 2022).
- International Society for Pharmacoeconomics and Outcomes Research. Top 10 HEOR Trends. Available online: https://www.ispor.org/heor-resources/about-heor/top-10-heor-trends/ (accessed on 5 July 2022).
- Thorlund, K.; Dron, L.; Park, J.J.H.; Mills, E.J. Synthetic and external controls in clinical trials-a primer for researchers. Clin. Epidemiol. 2020, 12, 457–467. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7218288/ (accessed on 5 July 2022). [CrossRef] [PubMed]
- Wallach, J.D.; Zhang, A.D.; Skydel, J.J.; Bartlett, V.L.; Dhuva, S.S.; Shah, N.D.; Ross, J.S. Feasibility of using real-world data to emulate post-approval confirmatory clinical trials of therapeutic agents granted US Food and Drug Administration accelerated approval. JAMA Netw. Open 2021, 4, e2133667. Available online: https://pubmed.ncbi.nlm.nih.gov/34751763/ (accessed on 5 July 2022). [CrossRef] [PubMed]
- American Society of Clinical Oncology. The ASCO Post. 2020 FDA Approvals of Drugs for Cancer Treatment. 2020. Available online: https://ascopost.com/issues/december-25-2020/2020-fda-approvals-of-drugs-for-cancer-treatment/ (accessed on 5 July 2022).
- Clinical Trials Transformation Initiative. Download AACT. Available online: https://aact.ctti-clinicaltrials.org/download (accessed on 17 December 2021).
- US Food and Drug Administration. Enhancing the Diversity of Clinical Trial Populations—Eligibility Criteria, Enrollment Practices, and Trial Designs Guidance for Industry. 2020. Available online: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/enhancing-diversity-clinical-trial-populations-eligibility-criteria-enrollment-practices-and-trial (accessed on 28 January 2023).
- Riner, A.N.; Girma, S.; Vudatha, V.; Mukhopadhyay, N.; Skoro, N.; Gal, T.S.; Freudenberger, D.C.; Herremans, K.M.; George, T.J.; Trevino, J.G. Eligibility criteria perpetuate disparities in enrollment and participation of Black patients in pancreatic cancer clinical trials. J. Clin. Oncol. 2022, 40, 2193–2202. Available online: https://pubmed.ncbi.nlm.nih.gov/35316089/ (accessed on 28 January 2023). [CrossRef] [PubMed]
- Von Lucadou, M.; Ganslandt, T.; Prokosch, H.U.; Toddenroth, D. Feasibility analysis of conducting observational studies with the electronic health record. BMC Med. Inform. Decis. Mak. 2019, 19, 202. Available online: https://pubmed.ncbi.nlm.nih.gov/31660955/ (accessed on 2 May 2023). [CrossRef] [PubMed]
- Ontada. Available online: https://www.ontada.com/ (accessed on 1 May 2023).


{kind=link}
| Example Verbatim Trial Criteria a | Inclusion (I) orExclusion (E) b | Category c | Subcategory d | Likelihood of Presence in EHR |
|---|---|---|---|---|
| Participants must have PD-L1 IHC testing with results performed by a central laboratory during the screening period | I | Cancer-Related | Biomarker or Genetic Marker | Yes |
| Histologically confirmed MBC, current stage IV | I | Cancer-Related | Cancer Stage | Yes |
| Newly diagnosed acute myeloid leukemia (AML) | I | Cancer-Related | Cancer Type | Yes |
| At least one measurable untreated lesion | I | Cancer-Related | Measurable Disease | Yes |
| Active or untreated central nervous system (CNS) metastases as determined by computed tomography (CT) or magnetic resonance imaging (MRI) evaluation | E | Cancer-Related | Metastasis | Yes |
| Isolated myeloid sarcoma (i.e., myeloblastoma or chloroma) allowed regardless of bone marrow results | I | Cancer-Related | Other Cancer | Yes |
| Intrathecal [drug name] e given at diagnosis allowed | I | Cancer-Related | Prior Cancer Treatments/Procedures | Yes |
| Progression of disease after 1 or 2 prior regimens in the metastatic setting | I | Cancer-Related | Progressive Disease | Yes |
| Significant history of cardiovascular disease | E | Comorbidity-Related | Cardiovascular Status | Yes |
| Patients with Down syndrome over 4 years of age are eligible | I | Comorbidity-Related | Comorbidity | Yes |
| Topical or inhalation steroids for other conditions allowed | I | Comorbidity-Related | Concomitant Medications | Yes |
| Known contraindication to receive [drug name]e at the planned doses | E | Comorbidity-Related | Contraindication | Yes |
| Participant has received strong or moderate cytochrome P450 3A4 (CYP3A) inducers 7 days prior to the initiation of study treatment | E | Comorbidity-Related | Drug–Drug/Food Interaction | Yes |
| Have adequate organ function, as defined by the study protocol | I | Comorbidity-Related | Organ Function | Yes |
| History of idiopathic pulmonary fibrosis, organizing pneumonia, drug induced pneumonitis, idiopathic pneumonitis, or evidence of active pneumonitis on screening chest CT scan. History of radiation pneumonitis in the radiation field (fibrosis) is permitted | E | Comorbidity-Related | Pulmonary Status | Yes |
| Male or female participants ≥ 55 years of age | I | Demographic | Demographic | Yes |
| Adequate hematologic and end-organ function | I | Functional Status | Hematologic Status | Yes |
| History of hepatic encephalopathy | I | Functional Status | Hepatic Status | Yes |
| Positive test for Human Immunodeficiency Virus (HIV) | E | Functional Status | HIV Status | Yes |
| Participant has a known hypersensitivity to the components of [drug name] e or its excipients | E | Functional Status | Hypersensitivity | Yes |
| Active or history of autoimmune disease or immune deficiency | E | Functional Status | Immune Status | Yes |
| Active hepatitis B or hepatitis C | E | Functional Status | Infection | Yes |
| The participant has any known significant ophthalmologic abnormalities of the surface of the eye | E | Functional Status | Ocular Status | Yes |
| Eastern Cooperative Oncology Group (ECOG) performance status—0, 1, 2, 3 | I | Functional Status | Performance Status | Yes |
| Creatinine clearance inferior to 30 mL per minute (Modification of Diet in Renal Disease (MDRD) Formula) | E | Functional Status | Renal Status | Yes |
| Not pregnant or nursing | I | Functional Status | Reproductive Status | Yes |
| Matched family donor criteria (for patients with intermediate-risk or high-risk disease) | I | Trial-Specific | Donor Matching | No |
| Life expectancy of at least 3 months | I | Trial-Specific | Life Expectancy | No |
| Negative pregnancy test | I | Trial-Specific | Trial Operations | No |
| Criteria Category | Criteria Subcategory | ||||
|---|---|---|---|---|---|
| Name | n of Criteria Found across all 20 Trials | % of the Total Criteria across All 20 Trials | Name | n | % |
| Cancer-Related | 212 | 46 | Biomarker or Genetic Marker | 21 | 10 |
| Cancer Stage | 10 | 5 | |||
| Cancer Type | 35 | 17 | |||
| Measurable Disease | 12 | 6 | |||
| Metastasis | 7 | 3 | |||
| Other Cancer | 51 | 24 | |||
| Prior Cancer Treatments/Procedures | 71 | 33 | |||
| Progressive Disease | 5 | 2 | |||
| Comorbidity-Related | 92 | 20 | Cardiovascular Status | 14 | 15 |
| Comorbidity | 48 | 52 | |||
| Concomitant Medications | 4 | 4 | |||
| Contraindication | 1 | 1 | |||
| Drug–Drug/Food Interaction | 5 | 5 | |||
| Organ Function | 15 | 16 | |||
| Pulmonary Status | 5 | 5 | |||
| Demographic | 11 | 2 | Age and Sex | 11 | 100 |
| Functional Status | 82 | 18 | Hematological Status | 19 | 23 |
| Hepatic Status | 6 | 7 | |||
| HIV Status | 6 | 7 | |||
| Hypersensitivity | 7 | 9 | |||
| Immune Status | 4 | 5 | |||
| Infection | 12 | 15 | |||
| Ocular Status | 3 | 4 | |||
| Performance Status | 17 | 21 | |||
| Renal Status | 3 | 4 | |||
| Reproductive Status | 5 | 6 | |||
| Trial-Specific | 66 | 14 | Donor Status | 8 | 12 |
| Life Expectancy | 4 | 6 | |||
| Trial Operations | 54 | 82 | |||
| Total | 463 | 100 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wilson, T.W.; Dye, J.T.; Spark, S.; Robert, N.J.; Espirito, J.L.; Amirian, E.S. Feasibility of Using Oncology-Specific Electronic Health Record (EHR) Data to Emulate Clinical Trial Eligibility Criteria. Pharmacoepidemiology 2023, 2, 140-147. https://doi.org/10.3390/pharma2020013
Wilson TW, Dye JT, Spark S, Robert NJ, Espirito JL, Amirian ES. Feasibility of Using Oncology-Specific Electronic Health Record (EHR) Data to Emulate Clinical Trial Eligibility Criteria. Pharmacoepidemiology. 2023; 2(2):140-147. https://doi.org/10.3390/pharma2020013
Chicago/Turabian StyleWilson, Thomas W., Joseph T. Dye, Sarah Spark, Nicholas J. Robert, Janet L. Espirito, and E. Susan Amirian. 2023. "Feasibility of Using Oncology-Specific Electronic Health Record (EHR) Data to Emulate Clinical Trial Eligibility Criteria" Pharmacoepidemiology 2, no. 2: 140-147. https://doi.org/10.3390/pharma2020013