
Clinical Indicators of Cardiovascular Risk in Adult Patients Undergoing Chemotherapy: A Protocol for Scoping Review


 ,
, 
Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Research Question
2.3. Searching for the Evidence
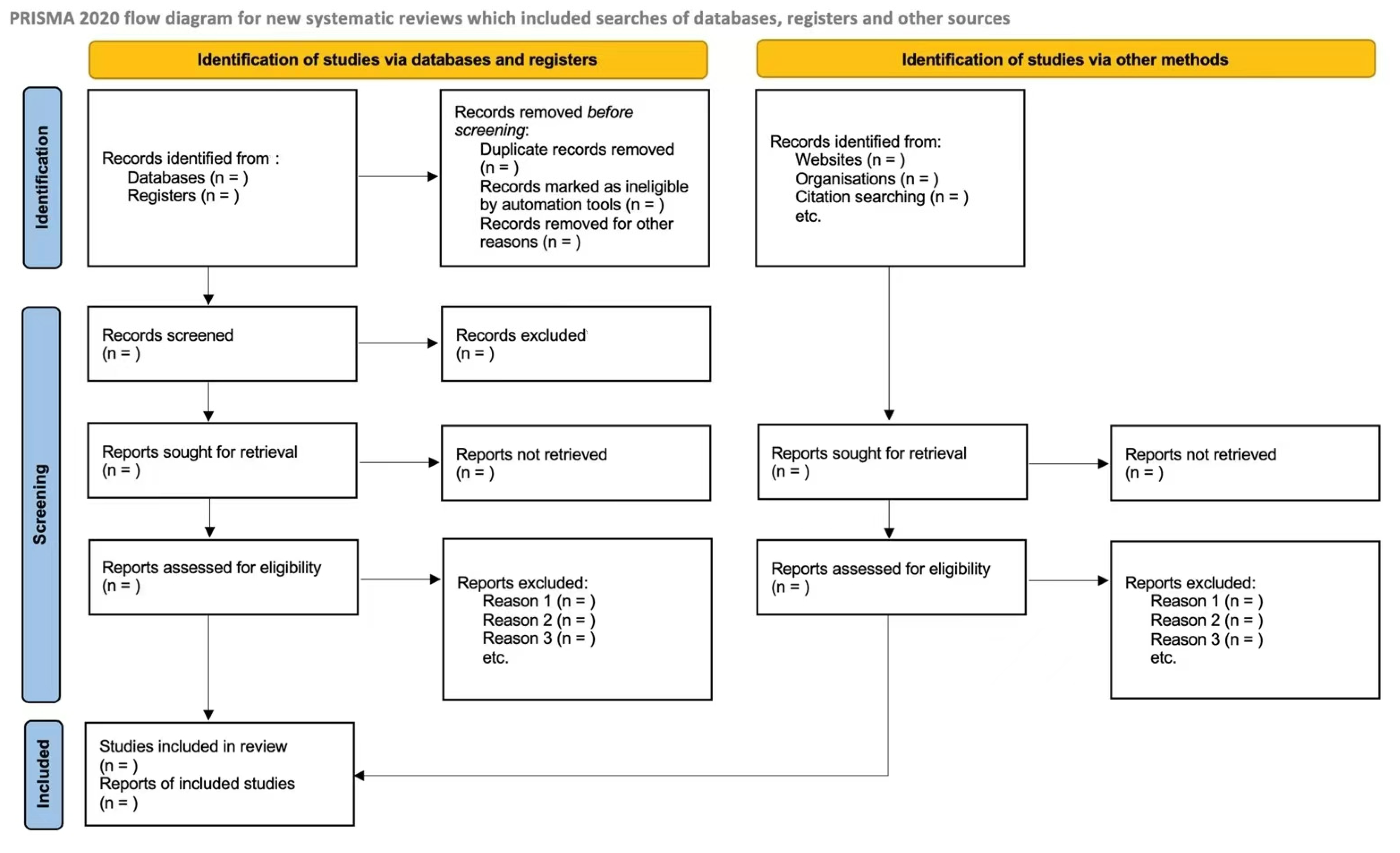
2.4. Selecting Evidence
2.5. Collating Evidence
2.6. Analyzing Evidence
2.7. Patient and Public Involvement
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fuster, V.; Voûte, J. MDGs: Chronic diseases are not on the agenda. Lancet 2005, 366, 1512–1514. [Google Scholar] [CrossRef] [PubMed]
- Miller, K.D.; Nogueira, L.; Devasia, T.; Mariotto, A.B.; Yabroff, K.R.; Jemal, A.; Kramer, J.; Siegel, R.L. Cancer treatment and survivorship statistics, 2022. CA Cancer J. Clin. 2022, 72, 409–436. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer statistics, 2022. CA Cancer J. Clin. 2022, 72, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Lopes-Júnior, L.C.; Lima, R.A.G. Cancer care and interdisciplinary practice. Cad. Saude Publica 2019, 35, e00193218. [Google Scholar] [CrossRef]
- Levis, B.E.; Binkley, P.F.; Shapiro, C.L. Cardiotoxic effects of anthracycline-based therapy: What is the evidence and what are the potential harms? Lancet Oncol. 2017, 18, e445–e456. [Google Scholar] [CrossRef]
- Colombo, A.; Cipolla, C.; Beggiato, M.; Cardinale, D. Cardiac toxicity of anticancer agents. Curr. Cardiol. Rep. 2013, 15, 362. [Google Scholar] [CrossRef]
- O’Hare, M.; Sharma, A.; Murphy, K.; Mookadam, F.; Lee, H. Cardio-oncology Part I: Chemotherapy and cardiovascular toxicity. Expert. Rev. Cardiovasc. Ther. 2015, 13, 511–518. [Google Scholar] [CrossRef]
- O’Hare, M.; Murphy, K.; Mookadam, F.; Sharma, A.; Lee, H. Cardio-oncology Part II: The monitoring, prevention, detection and treatment of chemotherapeutic cardiac toxicity. Expert. Rev. Cardiovasc. Ther. 2015, 13, 519–527. [Google Scholar] [CrossRef]
- Armstrong, G.T.; Oeffinger, K.C.; Chen, Y.; Kawashima, T.; Yasui, Y.; Leisenring, W.; Stovall, M.; Chow, E.J.; Sklar, C.A.; Mulrooney, D.A.; et al. Modifiable risk factors and major cardiac events among adult survivors of childhood cancer. J. Clin. Oncol. 2013, 31, 3673–3680. [Google Scholar] [CrossRef]
- Pan, J.; Garza, F.; Lyon, A.R. Cardio-oncology: Rationale, aims and future directions. Curr. Opin. Support. Palliat. Care 2021, 15, 134–140. [Google Scholar] [CrossRef] [PubMed]
- Kostakou, P.M.; Kouris, N.T.; Kostopoulos, V.S.; Damaskos, D.S.; Olympios, C.D. Cardio-oncology: A new and developing sector of research and therapy in the field of cardiology. Heart Fail. Rev. 2019, 24, 91–100. [Google Scholar] [CrossRef] [PubMed]
- Karlstaedt, A.; Barrett, M.; Hu, R.; Gammons, S.T.; Ky, B. Cardio-Oncology: Understanding the Intersections Between Cardiac Metabolism and Cancer Biology. JACC Basic Transl. Sci. 2021, 6, 705–718. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Health Statistics and Information Systems: Disease Burden and Mortality Estimates; WHO: Geneva, Switzerland, 2022; Available online: http://www.who.int/healthinfo/global_burden_disease/estimates/en/index1.html (accessed on 1 August 2022).
- Ewer, M.S.; Ewer, S.M. Cardiotoxicity of anticancer treatments: What the cardiologist needs to know. Nat. Rev. Cardiol. 2010, 7, 564–575. [Google Scholar] [CrossRef] [PubMed]
- Wu, A.H. Cardiotoxic drugs: Clinical monitoring and decision making. Heart 2008, 94, 1503–1509. [Google Scholar] [CrossRef] [PubMed]
- Monsuez, J.J.; Charniot, J.C.; Vignat, N.; Artigou, J.Y. Cardiac side-effects of cancer chemotherapy. Int. J. Cardiol. 2010, 144, 3–15. [Google Scholar] [CrossRef]
- Yeh, E.T.; Bickford, C.L. Cardiovascular complications of cancer therapy: Incidence, pathogenesis, diagnosis, and management. J. Am. Coll. Cardiol. 2009, 53, 2231–2247. [Google Scholar] [CrossRef]
- Peters, M.D.J.; Godfrey, C.; McInerney, P.; Munn, Z.; Tricco, A.C.; Khalil, H. Chapter 11: Scoping Reviews (2020 version). In JBI Manual for Evidence Synthesis; Aromataris, E., Munn, Z., Eds.; JBI: North Adelaide, Australia, 2020. [Google Scholar]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. Theory Pract. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Munn, Z.; Peters, M.D.; Stern, C.; Tufanaru, C.; McArthur, A.; Aromataris, E. Systematic review or scoping review? Guidance for authors when choosing be-tween a systematic or scoping review approach. BMC Med. Res. Methodol. 2018, 18, 143. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.; Colquhoun, H.; Kastner, M.; Levac, D.; Ng, C.; Sharpe, J.P.; Wilson, K.; et al. A scoping review on the conduct and reporting of scoping reviews. BMC Med. Res. Methodol. 2016, 16, 15. [Google Scholar] [CrossRef] [PubMed]
- Lotufo, P.A. O escore de risco de Framingham para doenças cardiovasculares. Rev. Med. 2008, 87, 232–237. [Google Scholar] [CrossRef]
- Lopes-Júnior, L.C.; Bomfim, E.; Olson, K.; Neves, E.T.; Silveira, D.S.C.; Nunes, M.D.R.; Nascimento, L.C.; Pereira-da-Silva, G.; Lima, R.A.G. Effectiveness of hospital clowns for symptom management in paediatrics: Systematic review of randomised and non-randomised controlled trials. BMJ 2020, 371, m4290. [Google Scholar] [CrossRef] [PubMed]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan-a web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef]
- Lopes-Júnior, L.C.; Lima, R.A.G.; Zonta, J.B.; Sulino, M.C.; Looman, W.S.; Correa, L.M.; Okido, A.C.C. Biomarkers of stress in caregivers of children with special health care needs: A protocol for systematic review. Medicine 2022, 101, e31448. [Google Scholar] [CrossRef]
- Da Silva Junior, F.J.G.; de Souza Monteiro, C.F.; Costa, A.P.C.; Campos, L.R.B.; Miranda, P.I.G.; de Souza Monteiro, T.A.; Lima, R.A.G.; Lopes-Junior, L.C. Impact of COVID-19 pandemic on mental health of young people and adults: A systematic review protocol of observational studies. BMJ Open 2020, 10, e039426. [Google Scholar] [CrossRef]
- Pessanha, R.M.; Schuab, S.I.P.D.C.; Nunes, K.Z.; Lopes-Júnior, L.C. Use of family history taking for hereditary neoplastic syndromes screening in primary health care: A systematic review protocol. PLoS ONE 2022, 17, e0271286. [Google Scholar] [CrossRef]
- Lopes-Júnior, L.C.; Ferrarini, T.; Pires, L.B.C.; Rodrigues, J.G.; Salaroli, L.B.; Nunes, K.Z. Cancer symptom clusters in adult patients undergoing chemotherapy: A systematic review and meta-analysis protocol. PLoS ONE 2022, 17, e0273411. [Google Scholar] [CrossRef]
- Centre for Evidence Based Medicine. Available online: http://www.cebm.net (accessed on 1 November 2021).
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Moslehi, J.J. Cardiovascular Toxic Effects of Targeted Cancer Therapies. N. Engl. J. Med. 2016, 375, 1457–1467. [Google Scholar] [CrossRef]
- Hajjar, L.A.; Costa, I.B.S.D.S.D.; Lopes, M.A.C.Q.; Hoff, P.M.G.; Diz, M.D.P.E.; Fonseca, S.M.R.; Bittar, C.S.; Rehder, M.H.H.D.S.; Rizk, S.I.; Almeida, D.R.; et al. Diretriz Brasileira de Cardio-oncologia—2020. Arq. Bras. Cardiol. 2020, 115, 1006–1043. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Barsevick, A.M.; Fang, C.Y.; Miaskowski, C. Common biological pathways underlying the psycho- neurological symptom cluster in cancer patients. Cancer Nurs. 2012, 35, E1–E20. [Google Scholar] [CrossRef] [PubMed]
- Dodd, M.J.; Miaskowski, C.; Lee, K.A. Occurrence of symptom clusters. J. Natl. Cancer Inst. Monogr. 2004, 2004, 76–78. [Google Scholar] [CrossRef] [PubMed]
- Lopes-Júnior, L.C. Cancer symptom clusters: From the lab bench to clinical practice. Rev. Bras. Enferm. 2022, 75, e2022v75n5inov. [Google Scholar] [CrossRef] [PubMed]
- Lopes-Júnior, L.C.; Tuma, M.C.; Amorim, M.H.C. Psychoneuroimmunology and oncology nursing: A theoretical study. Rev. Esc. Enferm. USP 2021, 55, e20210159. [Google Scholar] [CrossRef] [PubMed]
- Hull, M.C.; Morris, C.G.; Pepine, C.J.; Mendenhall, N.P. Valvular dysfunction and carotid, subclavian, and coronary artery disease in survivors of hodgkin lymphoma treated with radiation therapy. JAMA 2003, 290, 2831–2837. [Google Scholar] [CrossRef]
- Oeffinger, K.C.; Mertens, A.C.; Sklar, C.A.; Kawashima, T.; Hudson, M.M.; Meadows, A.T.; Friedman, D.L.; Marina, N.; Hobbie, W.; Kadan-Lottick, N.S.; et al. Childhood Cancer Survivor Study. Chronic health conditions in adult survivors of childhood cancer. N. Engl. J. Med. 2006, 355, 1572–1582. [Google Scholar] [CrossRef]
- Geenen, M.M.; Cardous-Ubbink, M.C.; Kremer, L.C.; van den Bos, C.; van der Pal, H.J.; Heinen, R.C.; Jaspers, M.W.; Koning, C.C.; Oldenburger, F.; Langeveld, N.E.; et al. Medical assessment of adverse health outcomes in long-term survivors of childhood cancer. JAMA 2007, 297, 2705–2715. [Google Scholar] [CrossRef]
- Reulen, R.C.; Winter, D.L.; Frobisher, C.; Lancashire, E.R.; Stiller, C.A.; Jenney, M.E.; Skinner, R.; Stevens, M.C.; Hawkins, M.M. British Childhood Cancer Survivor Study Steering Group. Long-term cause-specific mortality among survivors of childhood cancer. JAMA 2010, 304, 172–179. [Google Scholar] [CrossRef]
- Pinto, C.M.; Silva, D.C.; Pinto, G.H.; Santos, M.H.H. Quimioterapia e cardiotoxicidade. Rev. Soc. Cardiol. Estado São Paulo 2017, 27, 266–273. [Google Scholar] [CrossRef]
- Armenian, S.H.; Lacchetti, C.; Lenihan, D. Prevention and Monitoring of Cardiac Dysfunction in Survivors of Adult Cancers: American Society of Clinical Oncology Clinical Practice Guideline Summary. J. Oncol. Pract. 2017, 13, 270–275. [Google Scholar] [CrossRef] [PubMed]
- Da Costa, A.G.; Costa, M.S.C.R.; da Silva Ferreira, E.; de Sousa, P.C.; dos Santos, M.M.; Lima, D.E.D.O.B.; Ramos, A.M.P.C. Conhecimento dos Profissionais de Enfermagem sobre Segurança do Paciente Oncológico em Quimioterapia. Rev. Bras. Cancerol. 2019, 65, e04274. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| MEDLINE/PubMed | Search Strategy |
|---|---|
| (P)—Population | #1 ((“Young Adult” [MeSH Terms] OR “Adult” [MeSH Terms])) #2 ((“Neoplasms” [MeSH Terms] OR “Neoplasia” [All Fields] OR “Neoplasias” [All Fields] OR “Neoplasm” [All Fields] OR “Tumors” [All Fields] OR “Tumor” [All Fields] OR “Cancer” [All Fields] OR “Cancers” [All Fields] OR “Malignancy” [All Fields] OR “Malignancies” [All Fields] OR “Malignant Neoplasms” [All Fields] OR “Malignant Neoplasm” [All Fields] OR “Neoplasm, Malignant” [All Fields] OR “Neoplasms, Malignant” [All Fields])) #3 #1 AND #2 |
| (C)—Concept | #4 ((“Signs and Symptoms” [MeSH Terms] OR “Symptoms and Signs” [All Fields] OR “Heart Disease” [All Fields] OR “Cardiac Diseases” [All Fields] OR “Cardiac Disease” [All Fields] OR “Cardiac Disorders” [All Fields] OR “Cardiac Disorder” [All Fields] OR “Heart Disorders” [All Fields] OR “Heart Disorder” [All Fields])) #5 ((“Heart Disease Risk Factors” [MeSH Terms] OR “Cardiovascular Risk Factors” [All Fields] OR “Cardiovascular Risk Factor” [All Fields] OR “Factor, Cardiovascular Risk” [All Fields] OR “Risk Factor, Cardiovascular” [All Fields] OR “Risk Factors for Heart Disease” [All Fields] OR “Risk Factors for Cardiovascular Disease” [All Fields] OR “Cardiovascular Risk Score” [All Fields] OR “Cardiovascular Risk Scores” [All Fields] OR “Risk Score, Cardiovascular” [All Fields] OR “Score, Cardiovascular Risk” [All Fields] OR “Cardiovascular Risk” [All Fields] OR “Cardiovascular Risks” [All Fields] OR “Risk, Cardiovascular” [All Fields] OR “Residual Cardiovascular Risk” [All Fields] OR “Residual Cardiovascular Risks” [All Fields])) #6 #3 AND #4 AND #5 |
| (C)—Context | #7 ((“Chemotherapy” [All Fields] OR “Chemotherapy, Adjuvant” [MeSH Terms] OR “Induction Chemotherapy” [MeSH Terms] OR “Consolidation Chemotherapy” [MeSH Terms] OR “Maintenance Chemotherapy” [MeSH Terms])) NOT “Radiotherapy” [MeSH Terms] NOT “Surgery” [All Fields])) #8 #6 AND #7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nunes, K.Z.; Grassi, J.; Lopes, A.B.; Rezende, L.D.A.; Cavalcanti, J.A.; Gomes, K.N.; Silva, J.A.D.d.; Lopes-Júnior, L.C. Clinical Indicators of Cardiovascular Risk in Adult Patients Undergoing Chemotherapy: A Protocol for Scoping Review. Pharmacoepidemiology 2023, 2, 35-41. https://doi.org/10.3390/pharma2010004
Nunes KZ, Grassi J, Lopes AB, Rezende LDA, Cavalcanti JA, Gomes KN, Silva JADd, Lopes-Júnior LC. Clinical Indicators of Cardiovascular Risk in Adult Patients Undergoing Chemotherapy: A Protocol for Scoping Review. Pharmacoepidemiology. 2023; 2(1):35-41. https://doi.org/10.3390/pharma2010004
Chicago/Turabian StyleNunes, Karolini Zuqui, Jonathan Grassi, Andressa Bolsoni Lopes, Lucas Dalvi Armond Rezende, Julia Anhoque Cavalcanti, Karoline Neumann Gomes, Julia Antonietta Dantas da Silva, and Luís Carlos Lopes-Júnior. 2023. "Clinical Indicators of Cardiovascular Risk in Adult Patients Undergoing Chemotherapy: A Protocol for Scoping Review" Pharmacoepidemiology 2, no. 1: 35-41. https://doi.org/10.3390/pharma2010004