

Birth Outcomes of Anticancer Drug Prescriptions during Pregnancy: A Case Series from a Japanese Claims Database
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Data Source
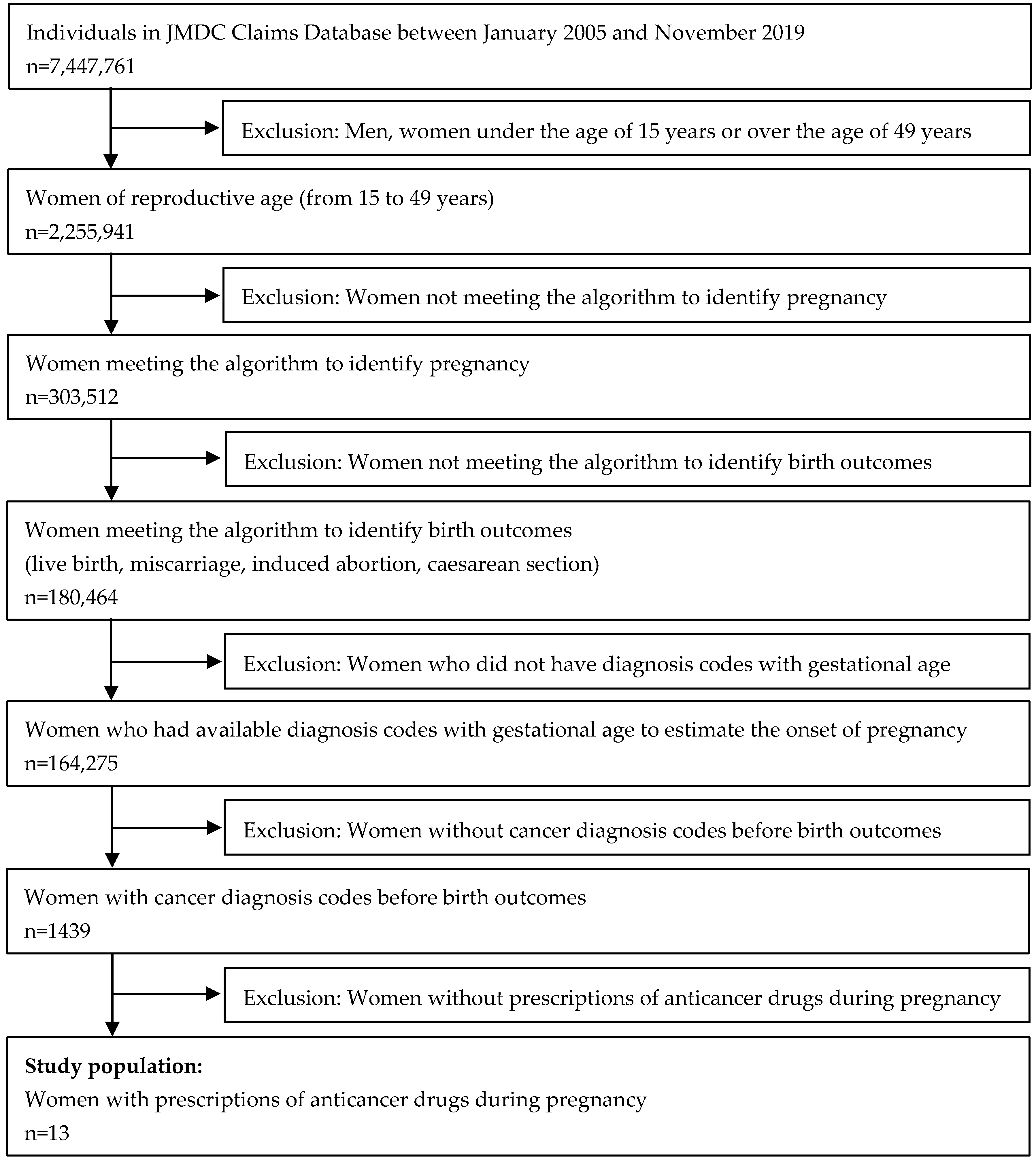
2.2. Eligible Study Population
2.3. Data Analysis
3. Results
3.1. Description of the Study Population
3.2. Causal Assessments between Anticancer Drugs and Adverse Birth Outcomes

{kind=link}
| Items of ’Evidence from Individual Cases’ Proposed by CIOMS Working Group VI | No. 1 (Miscarriage) Cyclophosphamide Cytarabine Daunorubicin l-Asparaginase Methotrexate Vincristine | No. 3 (Miscarriage) Imatinib | No. 7 (Atrial/Ventricular Septal Defect) Cyclophosphamide Doxorubicin | No. 11 (Miscarriage) Cisplatin Fluorouracil | |
|---|---|---|---|---|---|
| 2. | Definitive | Identified risk: Methotrexate [7,38,39] Potential risk: Cytarabine [40] Daunorubicin [40] Not definitive risk: cyclophosphamide l-asparaginase nelarabine vincristine | Potential risk: Imatinib [41,42] | Not definitive risk: cyclophosphamide doxorubicin | Not definitive risk: cisplatin fluorouracil |
| 3. | Time to onset plausible | Plausible: 12 days after nelarabine; 16 days after l-asparaginase; 34 days after other drugs | Plausible: 44 days after imatinib | Not plausible: Both drugs prescribed from week 17 of gestation | Plausible: 11 days after both drugs |
| 5. | Lack of confounding risk factors | Confounding risk factors: Diagnosis related with high-risk pregnancy (DIC, insomnia, sepsis, MDS); Medications (fluconazole, gentamicin, ketoprofen, loxoprofen); Radiation (CT scan) | Confounding risk factors: Medications (diclofenac, loxoprofen); Advanced age | Lack of confounding risk factors in this study | Confounding risk factors: Diagnosis related with high-risk pregnancy (epilepsy); Medications (loxoprofen, sodium valproate); Radiation (CT scan). |
| 6. | Amount and duration of exposure consistent/plausible with cause and effect (a) | Consistent/plausible: cyclophosphamide (once: 500 mg 5 vials); cytarabine (twice: 20 mg 2 vials); daunorubicin (twice: 20 mg 4 vials); l-asparaginase (twice: 5000 K unit 2 vials); methotrexate (twice: 5 mg 3 vials); nelarabine (three times: 250 mg 11 vials); vincristine (twice: 1 mg 2 vials). | Consistent/plausible: Imatinib (once (b): 400 mg 4 days, once: 400 mg 38 days, once: 400 mg 21 days). | Consistent/plausible: cyclophosphamide (five times: 500 mg 2 vials); doxorubicin (five times: 50 mg 2 vials). | Consistent/plausible: cisplatin (once: 50 mg 2 vials, 10 mg 2 vials); fluorouracil (four times: 250 mg 4 vials). |
| 9. | Co-medication unlikely to play a role | Likely based on item #5: Medications, radiation exposure. | Likely based on item #5: Medications, radiation exposure. | Unlikely based on item #5 | Likely based on item #5: Medications, radiation exposure. |
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ngu, S.F.; Ngan, H.Y. Chemotherapy in pregnancy. Best Pract. Res. Clin. Obstet. Gynaecol. 2016, 33, 86–101. [Google Scholar] [CrossRef]
- Pavlidis, N.A. Coexistence of pregnancy and malignancy. Oncologist 2002, 7, 279–287. [Google Scholar] [CrossRef] [Green Version]
- Ministry of Health, Labour and Welfare. Briefing of Birth Staatitics in 2021. Available online: https://www.mhlw.go.jp/toukei/saikin/hw/jinkou/tokusyu/syussyo07/index.html (accessed on 4 November 2022). (In Japanese)
- Stensheim, H.; Møller, B.; van Dijk, T.; Fosså, S.D. Cause-specific survival for women diagnosed with cancer during pregnancy or lactation: A registry-based cohort study. J. Clin. Oncol. 2009, 27, 45–51. [Google Scholar] [CrossRef]
- The Japanese Breast Cancer Society. Clinical Practice Guidelines for Breast Cancer 2018 [Supplement in 2019]; Kanehara & Co., LTD: Tokyo, Japan, 2019. (In Japanese) [Google Scholar]
- Japanese Society for Fertility Preservation. Clinical Practive Guidelines of Pregnancy, Delivery, and Reproductive Medicine for Patients with Breast Cancer in 2021; Kanehara & Co., LTD: Tokyo, Japan, 2021. (In Japanese) [Google Scholar]
- Japan Society of Obstetrics and Gynecology, Japan Association of Obstetricians and Gynecologists. Clinical guidelines for Obstetrics and Gynecology (Obstetrics part) in 2020. Available online: https://www.jsog.or.jp/activity/pdf/gl_sanka_2020.pdf (accessed on 4 November 2022). (In Japanese).
- Cardonick, E.; Iacobucci, A. Use of chemotherapy during human pregnancy. Lancet Oncol. 2004, 5, 283–291. [Google Scholar] [CrossRef]
- Loibl, S.; Han, S.N.; von Minckwitz, G.; Bontenbal, M.; Ring, A.; Giermek, J.; Fehm, T.; Van Calsteren, K.; Linn, S.C.; Schlehe, B.; et al. Treatment of breast cancer during pregnancy: An observational study. Lancet Oncol. 2012, 13, 887–896. [Google Scholar] [CrossRef]
- Lu, D.; Ludvigsson, J.F.; Smedby, K.E.; Fall, K.; Valdimarsdóttir, U.; Cnattingius, S.; Fang, F. Maternal Cancer During Pregnancy and Risks of Stillbirth and Infant Mortality. J. Clin. Oncol. 2017, 35, 1522–1529. [Google Scholar] [CrossRef]
- Cardonick, E.; Bhat, A.; Gilmandyar, D.; Somer, R. Maternal and fetal outcomes of taxane chemotherapy in breast and ovarian cancer during pregnancy: Case series and review of the literature. Ann. Oncol. 2012, 23, 3016–3023. [Google Scholar] [CrossRef]
- Momen, N.C.; Arendt, L.H.; Ernst, A.; Olsen, J.; Li, J.; Gissler, M.; Ramlau-Hansen, C.H. Pregnancy-associated cancers and birth outcomes in children: A Danish and Swedish population-based register study. BMJ Open 2018, 8, e022946. [Google Scholar] [CrossRef] [Green Version]
- de Haan, J.; Verheecke, M.; Van Calsteren, K.; Van Calster, B.; Shmakov, R.G.; Mhallem Gziri, M.; Halaska, M.J.; Fruscio, R.; Lok, C.A.R.; Boere, I.A.; et al. Oncological management and obstetric and neonatal outcomes for women diagnosed with cancer during pregnancy: A 20-year international cohort study of 1170 patients. Lancet Oncol. 2018, 19, 337–346. [Google Scholar] [CrossRef]
- Danet, C.; Araujo, M.; Bos-Thompson, M.A.; Portolan, G.; Gautier, S.; Vanlemmens, L.; Bonenfant, S.; Jonville-Béra, A.P.; Cottin, J.; Vial, T.; et al. Pregnancy outcomes in women exposed to cancer chemotherapy. Pharmacoepidemiol. Drug Saf. 2018, 27, 1302–1308. [Google Scholar] [CrossRef]
- Daw, J.R.; Hanley, G.E.; Greyson, D.L.; Morgan, S.G. Prescription drug use during pregnancy in developed countries: A systematic review. Pharmacoepidemiol. Drug Saf. 2011, 20, 895–902. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pisa, F.E.; Casetta, A.; Clagnan, E.; Michelesio, E.; Vecchi Brumatti, L.; Barbone, F. Medication use during pregnancy, gestational age and date of delivery: Agreement between maternal self-reports and health database information in a cohort. BMC Pregnancy Childbirth 2015, 15, 310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Japanese Society for Pharmacoepidemiology. Inventory of Japanese Databases for Clinical- and Pharmaco-Epidemiology Researches Ver.1.0_2020. Available online: https://sites.google.com/view/jspedatabaseindex/home (accessed on 4 November 2022).
- Ishikawa, T.; Obara, T.; Jin, K.; Nishigori, H.; Miyakoda, K.; Akazawa, M.; Nakasato, N.; Yaegashi, N.; Kuriyama, S.; Mano, N. Folic acid prescribed to prenatal and postpartum women who are also prescribed antiepileptic drugs in Japan: Data from a health administrative database. Birth Defects Res. 2020, 112, 1224–1233. [Google Scholar] [CrossRef] [PubMed]
- Ishikawa, T.; Obara, T.; Kikuchi, S.; Kobayashi, N.; Miyakoda, K.; Nishigori, H.; Tomita, H.; Akazawa, M.; Yaegashi, N.; Kuriyama, S.; et al. Antidepressant prescriptions for prenatal and postpartum women in Japan: A health administrative database study. J. Affect. Disord. 2020, 264, 295–303. [Google Scholar] [CrossRef]
- Ishikawa, T.; Obara, T.; Akazawa, M.; Noda, A.; Oyanagi, G.; Morishita, K.; Miyakoda, K.; Nishigori, H.; Kawame, H.; Yaegashi, N.; et al. Risk of major congenital malformations associated with first-trimester exposure to propulsives: A health administrative database study in Japan. Pharmacoepidemiol. Drug Saf. 2022, 31, 196–205. [Google Scholar] [CrossRef]
- Michihata, N.; Shigemi, D.; Yamana, H.; Matsui, H.; Jo, T.; Yasunaga, H. Safety of Japanese herbal Kampo medicines for the treatment of depression during pregnancy. Int. J. Gynaecol. Obstet. 2022. Epub ahead of print. [Google Scholar] [CrossRef]
- Yamamoto-Sasaki, M.; Yoshida, S.; Takeuchi, M.; Tanaka-Mizuno, S.; Kawakami, K. Association between antidepressant use during pregnancy and congenital anomalies in children: A retrospective cohort study based on Japanese claims data. Congenit. Anom. 2020, 60, 180–188. [Google Scholar] [CrossRef]
- Kimura, S.; Sato, T.; Ikeda, S.; Noda, M.; Nakayama, T. Development of a database of health insurance claims: Standardization of disease classifications and anonymous record linkage. J. Epidemiol. 2010, 20, 413–419. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. The Global Health Observatory-Indicator Metadata Registry List. Available online: https://www.who.int/data/gho/indicator-metadata-registry/imr-details/3199 (accessed on 4 November 2022).
- Tajima, K.; Ishikawa, T.; Matsuzaki, F.; Noda, A.; Morishita, K.; Inoue, R.; Iwama, N.; Nishigori, H.; Sugawara, J.; Saito, M.; et al. Validity of Administrative Data for Identifying Birth-Related Outcomes with the End Date of Pregnancy in a Japanese University Hospital. Int. J. Environ. Res. Public Health 2022, 19, 4864. [Google Scholar] [CrossRef]
- Tajima, K.; Ishikawa, T.; Noda, A.; Matsuzaki, F.; Morishita, K.; Inoue, R.; Iwama, N.; Nishigori, H.; Sugawara, J.; Saito, M.; et al. Development and validation of claims-based algorithms to identify pregnancy based on data from a university hospital in Japan. Curr. Med. Res. Opin. 2022, 38, 1651–1654. [Google Scholar] [CrossRef]
- Ishikawa, T.; Obara, T.; Nishigori, H.; Miyakoda, K.; Inoue, R.; Hoshiai, T.; Saito, M.; Yaegashi, N.; Mano, N. Development of algorithms to determine the onset of pregnancy and delivery date using health care administrative data in a university hospital in Japan. Pharmacoepidemiol. Drug Saf. 2018, 27, 751–762. [Google Scholar] [CrossRef] [PubMed]
- Minakami, H.; Maeda, T.; Fujii, T.; Hamada, H.; Iitsuka, Y.; Itakura, A.; Itoh, H.; Iwashita, M.; Kanagawa, T.; Kanai, M.; et al. Guidelines for obstetrical practice in Japan: Japan Society of Obstetrics and Gynecology (JSOG) and Japan Association of Obstetricians and Gynecologists (JAOG) 2014 edition. J. Obstet. Gynaecol. Res. 2014, 40, 1469–1499. [Google Scholar] [CrossRef] [PubMed]
- Ihira, H.; Goto, A.; Yamagishi, K.; Iso, H.; Iwasaki, M.; Sawada, N.; Tsugane, S.; JPHC-NEXT Study Group. Validity of claims data for identifying cancer incidence in the Japan public health center-based prospective study for the next generation. Pharmacoepidemiol. Drug Saf. 2022, 31, 972–982. [Google Scholar] [CrossRef] [PubMed]
- de Luise, C.; Sugiyama, N.; Morishima, T.; Higuchi, T.; Katayama, K.; Nakamura, S.; Chen, H.; Nonnenmacher, E.; Hase, R.; Jinno, S.; et al. Validity of claims-based algorithms for selected cancers in Japan: Results from the VALIDATE-J study. Pharmacoepidemiol. Drug Saf. 2021, 30, 1153–1161. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Preterm Birth. Available online: https://www.who.int/news-room/fact-sheets/detail/preterm-birth (accessed on 4 November 2022).
- Boothby, L.A.; Doering, P.L. FDA labeling system for drugs in pregnancy. Ann. Pharmacother. 2001, 35, 1485–1489. [Google Scholar] [CrossRef] [PubMed]
- Kao, W.H.; Kuo, C.F.; Chiou, M.J.; Liu, Y.C.; Wang, C.C.; Hong, J.H.; Hsu, J.T.; Chiang, Y.J.; Chuang, Y.F. Adverse birth outcomes in adolescent and young adult female cancer survivors: A nationwide population-based study. Br. J. Cancer 2020, 122, 918–924. [Google Scholar] [CrossRef]
- McCollough, C.H.; Schueler, B.A.; Atwell, T.D.; Braun, N.N.; Regner, D.M.; Brown, D.L.; LeRoy, A.J. Radiation exposure and pregnancy: When should we be concerned? Radiographics 2007, 27, 909–917; discussion 917–918. [Google Scholar] [CrossRef]
- Ministry of Health, Labour and Welfare. Health System for Pregnant Women. Available online: https://www.mhlw.go.jp/stf/shingi/other-hoken_553056_00007.html (accessed on 4 November 2022). (In Japanese)
- Ishikawa, T.; Oyanagi, G.; Obara, T.; Noda, A.; Morishita, K.; Takagi, S.; Inoue, R.; Kawame, H.; Mano, N. Validity of congenital malformation diagnoses in healthcare claims from a university hospital in Japan. Pharmacoepidemiol. Drug Saf. 2021, 30, 975–978. [Google Scholar] [CrossRef]
- CIOMS Working Group VI. Management of Safety Information from Clinical Trials. Available online: https://cioms.ch/wp-content/uploads/2017/01/Mgment_Safety_Info.pdf (accessed on 4 November 2022).
- Carbonell Esteve, J.L.; Varela, L.; Velazco, A.; Tanda, R.; Sánchez, C. 25 mg or 50 mg of oral methotrexate followed by vaginal misoprostol 7 days after for early abortion: A randomized trial. Gynecol. Obstet. Investig. 1999, 47, 182–187. [Google Scholar] [CrossRef]
- Kulier, R.; Kapp, N.; Gülmezoglu, A.M.; Hofmeyr, G.J.; Cheng, L.; Campana, A. Medical methods for first trimester abortion. Cochrane Database Syst. Rev. 2011, 2011, Cd002855. [Google Scholar] [CrossRef]
- Azim, H.A., Jr.; Pavlidis, N.; Peccatori, F.A. Treatment of the pregnant mother with cancer: A systematic review on the use of cytotoxic, endocrine, targeted agents and immunotherapy during pregnancy. Part II: Hematological tumors. Cancer Treat. Rev. 2010, 36, 110–121. [Google Scholar] [CrossRef] [PubMed]
- Pye, S.M.; Cortes, J.; Ault, P.; Hatfield, A.; Kantarjian, H.; Pilot, R.; Rosti, G.; Apperley, J.F. The effects of imatinib on pregnancy outcome. Blood 2008, 111, 5505–5508. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rambhatla, A.; Strug, M.R.; De Paredes, J.G.; Cordoba Munoz, M.I.; Thakur, M. Fertility considerations in targeted biologic therapy with tyrosine kinase inhibitors: A review. J. Assist. Reprod. Genet 2021, 38, 1897–1908. [Google Scholar] [CrossRef] [PubMed]
- Murthy, R.K.; Theriault, R.L.; Barnett, C.M.; Hodge, S.; Ramirez, M.M.; Milbourne, A.; Rimes, S.A.; Hortobagyi, G.N.; Valero, V.; Litton, J.K. Outcomes of children exposed in utero to chemotherapy for breast cancer. Breast Cancer Res. 2014, 16, 500. [Google Scholar] [CrossRef] [Green Version]
- Albright, C.M.; Wenstrom, K.D. Malignancies in pregnancy. Best Pract. Res. Clin. Obstet. Gynaecol. 2016, 33, 2–18. [Google Scholar] [CrossRef]
- Peccatori, F.A.; Azim, H.A., Jr.; Orecchia, R.; Hoekstra, H.J.; Pavlidis, N.; Kesic, V.; Pentheroudakis, G.; ESMO Guidelines Working Group. Cancer, pregnancy and fertility: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2013, 24, vi160–vi170. [Google Scholar] [CrossRef]
- Varghese, S.S.; Eekhoudt, C.R.; Jassal, D.S. Mechanisms of anthracycline-mediated cardiotoxicity and preventative strategies in women with breast cancer. Mol. Cell Biochem. 2021, 476, 3099–3109. [Google Scholar] [CrossRef]
- Ministry of Health, Labour and Welfare. Briefing of Survey of Medical Institutions (Static/Dynamic) and Horpital Report in 2020. Available online: https://www.mhlw.go.jp/toukei/saikin/hw/iryosd/20/ (accessed on 4 November 2022). (In Japanese)
- Kim, J.H.; Kim, H.S.; Sung, C.W.; Kim, K.J.; Kim, C.H.; Lee, K.Y. Docetaxel, gemcitabine, and cisplatin administered for non-small cell lung cancer during the first and second trimester of an unrecognized pregnancy. Lung Cancer 2008, 59, 270–273. [Google Scholar] [CrossRef]
- Zemlickis, D.; Lishner, M.; Degendorfer, P.; Panzarella, T.; Sutcliffe, S.B.; Koren, G. Fetal outcome after in utero exposure to cancer chemotherapy. Arch. Intern. Med. 1992, 152, 573–576. [Google Scholar] [CrossRef]
- Bando, H.; Kataoka, A.; Tamaki, K.; Kobayashi, M.; Tamura, N.; Ozawa, M.; Kawano, J.; Fukatsu, Y.; Kitano, A.; Shiota, K.; et al. Physician’s knowledge, attitudes and practice pattern for breast cancer diagnosed during pregnancy: A survey among breast care specialists in Japan. Breast Cancer 2020, 27, 796–802. [Google Scholar] [CrossRef]

| Age at the Time of Birth Outcomes, Year (Mean ± Standard Deviation) | 34.6 ± 5.0 | ||
|---|---|---|---|
| Anticancer drugs, n | Alkylating agent | Cyclophosphamide | 5 |
| Dacarbazine | 1 | ||
| Anticancer antibiotics | Doxorubicin | 4 | |
| Daunorubicin | 2 | ||
| Bleomycin | 1 | ||
| Vinca alkaloid | Vincristine | 3 | |
| Vinblastine | 1 | ||
| Tyrosine kinase inhibitor | Imatinib | 2 | |
| Dasatinib | 1 | ||
| Platinum | Carboplatin | 2 | |
| Cisplatin | 1 | ||
| Antimetabolic agent | Cytarabine | 1 | |
| Fluorouracil | 1 | ||
| Nelarabine | 1 | ||
| Methotrexate | 1 | ||
| Tegafur combination | 1 | ||
| Taxane | Docetaxel | 1 | |
| Paclitaxel | 1 | ||
| Monoclonal antibody | Rituximab | 1 | |
| Anticancer enzyme | L-asparaginase | 1 | |
| Timing of anticancer medications, n | First trimester | 6 | |
| Second trimester | 8 | ||
| Third trimester | 7 | ||
| Type of birth outcomes, n | Term live birth | 3 | |
| Preterm live birth | 7 | ||
| Miscarriage | 3 | ||
| Caesarean section | 6 | ||
| Types of cancers, n | Leukemia | 5 | |
| Breast cancer | 2 | ||
| Cervical cancer | 2 | ||
| Lymphoma | 2 | ||
| Gastric cancer | 1 | ||
| Ovarian cancer | 1 | ||
| No | Age | Cancer | Anticancer Drugs | Exposure Timing | Birth Outcome | Days (a) | Other Prescriptions/ Medical Practice | Medical History |
|---|---|---|---|---|---|---|---|---|
| 1 | 25 | ALL | Cyclophosphamide Cytarabine Daunorubicin L-asparaginase Methotrexate Nelarabine Vincristine | T1 (b) T1 (b) T1 (b) T1 T1 (b) T1 T1 (b) | Miscarriage | 65 | Fluconazole (T1) (c) Gentamicin (T1) (d) Ketoprofen (T1) (d) Loxoprofen (T1) (c) CT scan (T1) | DIC, insomnia, sepsis, MDS |
| 2 | 36 | ALL | Cyclophosphamide Daunorubicin Vincristine | T2 T2 T2/T3 | Preterm live birth by CS without CMs | 224 | Radiotherapy (T2) | DM, hypertension, threatened abortion, TPL, thrombocytopenia |
| 3 | 42 | CML | Imatinib (c) | T1 | Miscarriage | 48 | Diclofenac (T1) (d) Ketoprofen (T1) (d) | Renal dysfunction, hypothyroidism, uterine fibroid, HF |
| 4 | 34 | CML | Imatinib (c) | T1 (b) | Term live birth | 273 | Naproxen (T1) (c) | TPL |
| 5 | 40 | CML | Dasatinib (c) | T1 | Preterm live birth by CS (e) | 238 | Clindamycin (T1) (d) Loxoprofen (T1) (c) | Cervical cancer, threatened abortion, placenta previa with bleeding |
| 6 | 36 | Breast cancer | Cyclophosphamide Doxorubicin | T2/T3 T2/T3 | Term live birth without CMs | 266 | Medroxyprogesterone (T1) (c) | Threatened abortion, TPL, haemorrhage in the third stage of labour |
| 7 | 38 | Breast cancer | Cyclophosphamide Doxorubicin | T2/T3 T2/T3 | Preterm live birth by CS with atrial/ventricular septal defect | 247 | None | None |
| 8 | 37 | NHL | Cyclophosphamide Doxorubicin Rituximab Vincristine | T2/T3 (b) T2/T3 (b) T2/T3 (b) T2/T3 (b) | Term live birth by CS (e) | 260 | Etanercept (T1) Ketoprofen (T1/T3) (d) Ibuprofen (T2/T3) (c) Loxoprofen (T3) (c) CT scan (T2) | DM, RA, threatened abortion, hypothyroidism, abnormal uterine and vaginal bleeding |
| 9 | 28 | HL | Bleomycin Doxorubicin Dacarbazine Vinblastine | T2/T3 T2/T3 T2/T3 T2/T3 | Preterm live birth by CS without CMs | 231 | Fluconazole (T3) (c) | DM, MI, CHF, insomnia, TPL, Amniotic infection |
| 10 | 37 | Cervical cancer | Carboplatin | T2/T3 | Preterm live birth by CS (e) | 233 | Fradiomycin (T2) (d) Ibuprofen (T2) (d) CT scan (T2) | Threatened abortion |
| 11 | 28 | Cervical cancer | Cisplatin Fluorouracil | T1 T1 | Miscarriage | 56 | Loxoprofen (T1) (c) Sodium valproate (T1) (c) CT scan (T1) | Epilepsy |
| 12 | 32 | Gastric cancer | Docetaxel Tegafur combination (c,f) | T2/T3 T2/T3 | Preterm live birth without CMs | 234 | None | GAD, hypothyroidism, threatened abortion, TPL, arrhythmia |
| 13 | 37 | Ovarian cancer | Carboplatin Paclitaxel | T1 (b)/T2 T1/T2 | Preterm live birth(e) | 201 | Ketoprofen (T1) (d) Loxoprofen (T1) (c) Diclofenac (T1/T2) (d) Betamethasone/gentamicin (T2) (d) CT scan (T1/T2) | Schizophrenia, depression, parkinson’s disease, insomnia, autoimmune thyroiditis, asthma |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tajima, K.; Ishikawa, T.; Tsuchiya, M.; Kikuchi, M.; Obara, T.; Mano, N. Birth Outcomes of Anticancer Drug Prescriptions during Pregnancy: A Case Series from a Japanese Claims Database. Pharmacoepidemiology 2023, 2, 13-25. https://doi.org/10.3390/pharma2010002
Tajima K, Ishikawa T, Tsuchiya M, Kikuchi M, Obara T, Mano N. Birth Outcomes of Anticancer Drug Prescriptions during Pregnancy: A Case Series from a Japanese Claims Database. Pharmacoepidemiology. 2023; 2(1):13-25. https://doi.org/10.3390/pharma2010002
Chicago/Turabian StyleTajima, Kentaro, Tomofumi Ishikawa, Masami Tsuchiya, Masafumi Kikuchi, Taku Obara, and Nariyasu Mano. 2023. "Birth Outcomes of Anticancer Drug Prescriptions during Pregnancy: A Case Series from a Japanese Claims Database" Pharmacoepidemiology 2, no. 1: 13-25. https://doi.org/10.3390/pharma2010002