
Using a Portable Autostereoscopic Screen to Improve Anatomy Teaching and Learning

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
1.1. Issues Facing Current Implementation of Practical Anatomy
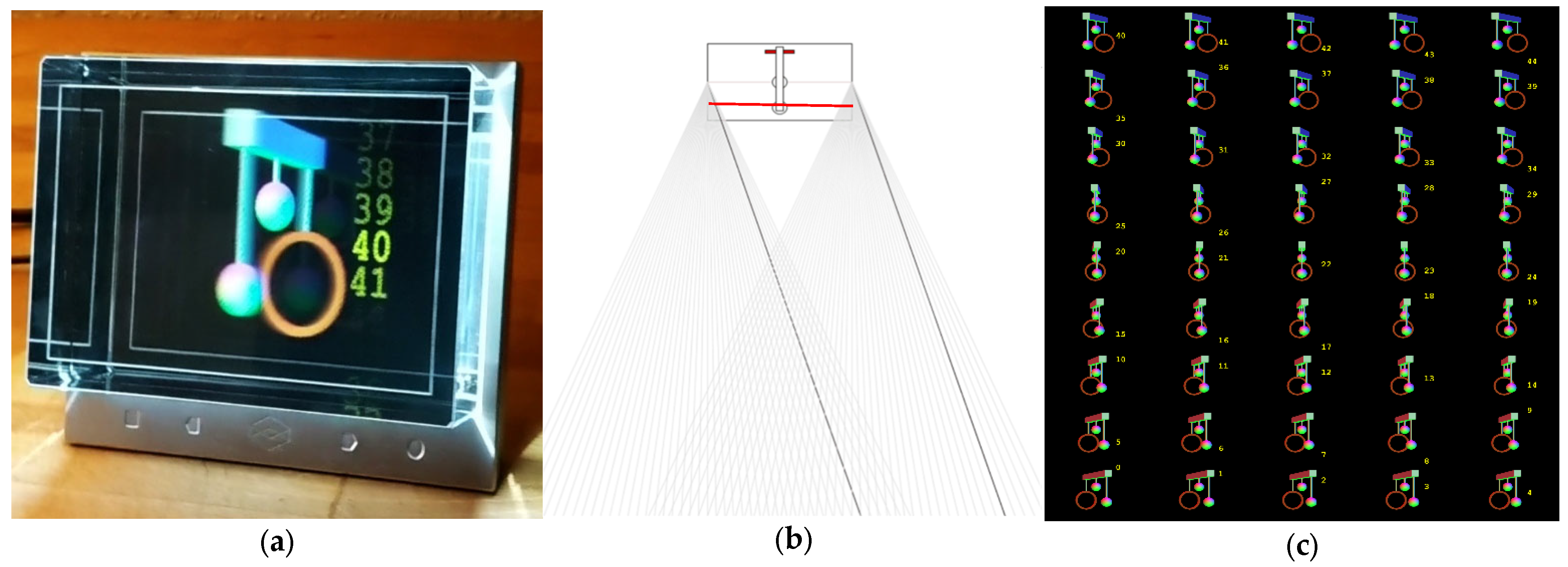
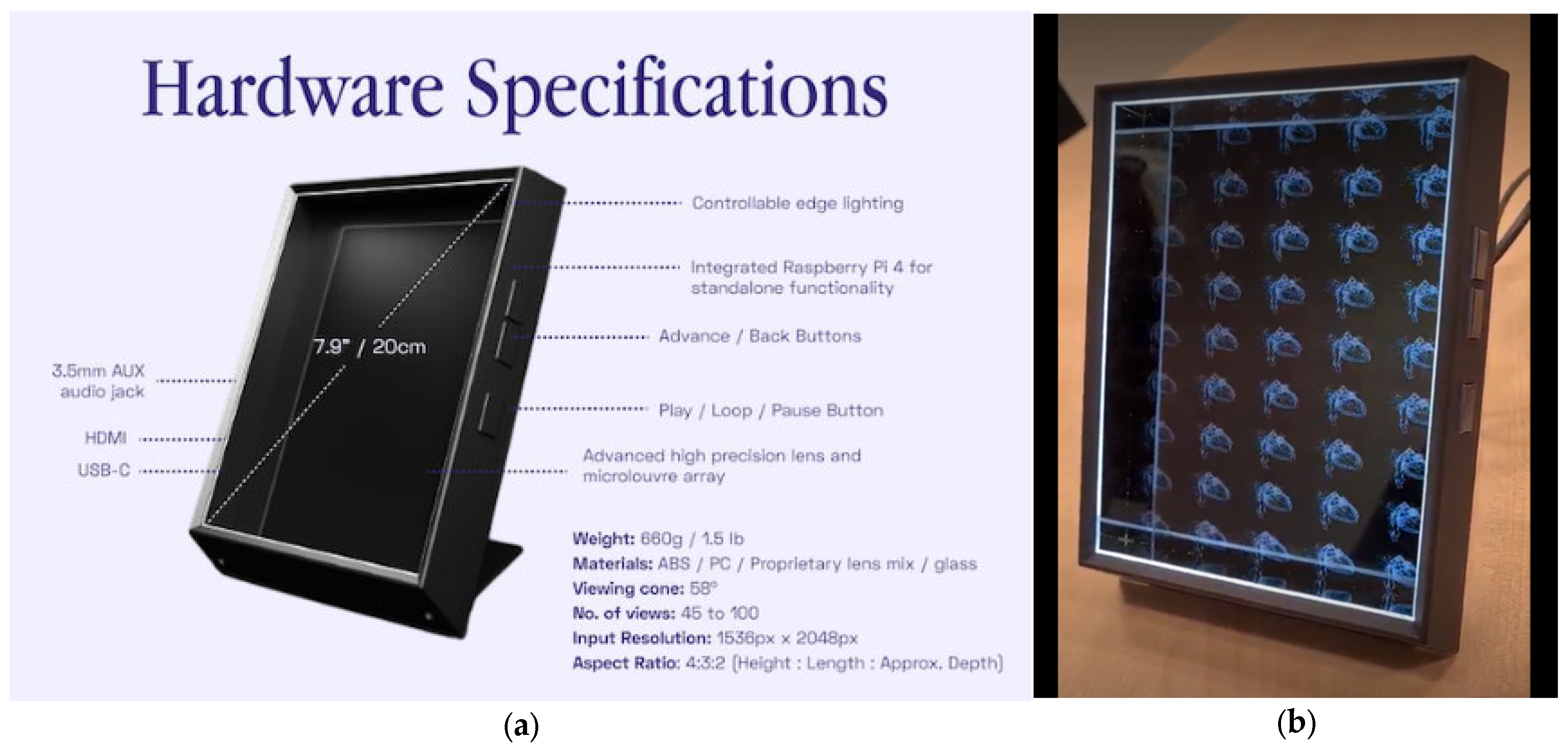
1.2. 3D Displays
1.3. 3D Displays in Anatomical Education
2. Materials and Methods
2.1. System Overview
2.2. Study Design
2.2.1. Participants
2.2.2. Procedure
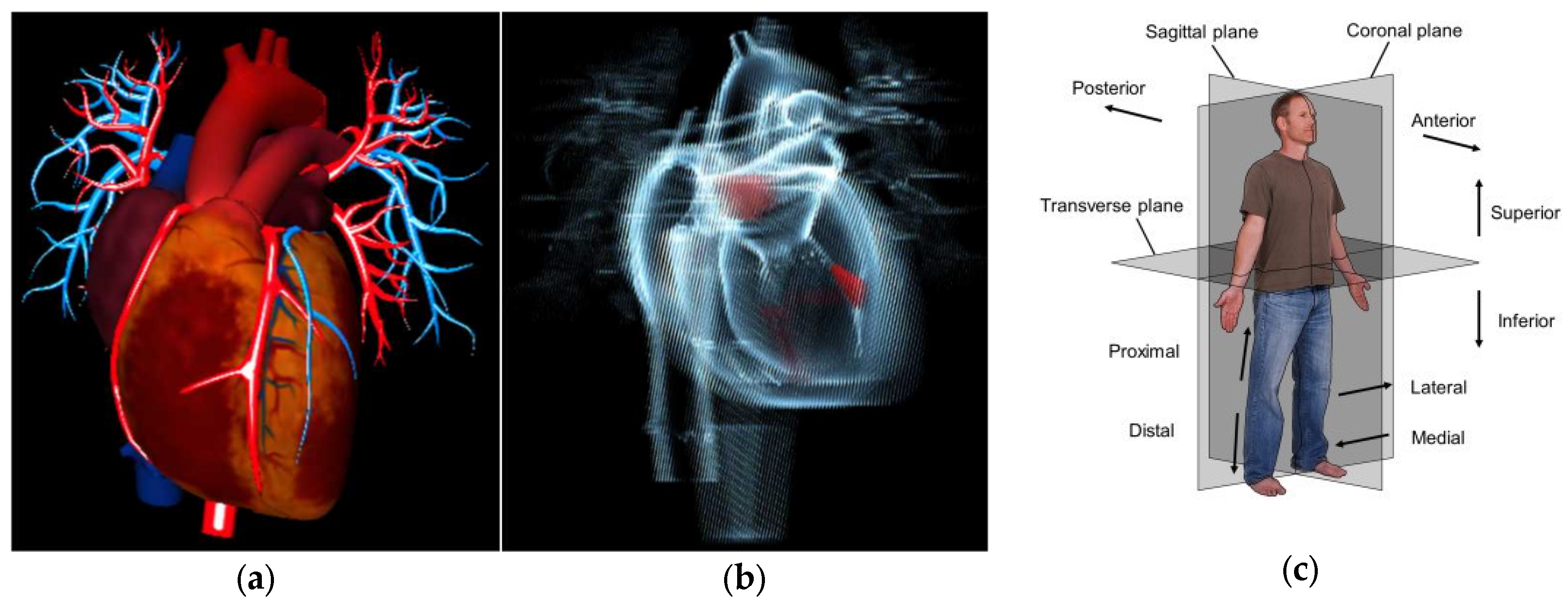
- Superior or inferior or in the same transversal plane;
- Anterior or posterior or in the same coronal plane;
- Left or right or in the same sagittal plane;
- Proximal and distal or lateral and medial or on the same medial line.

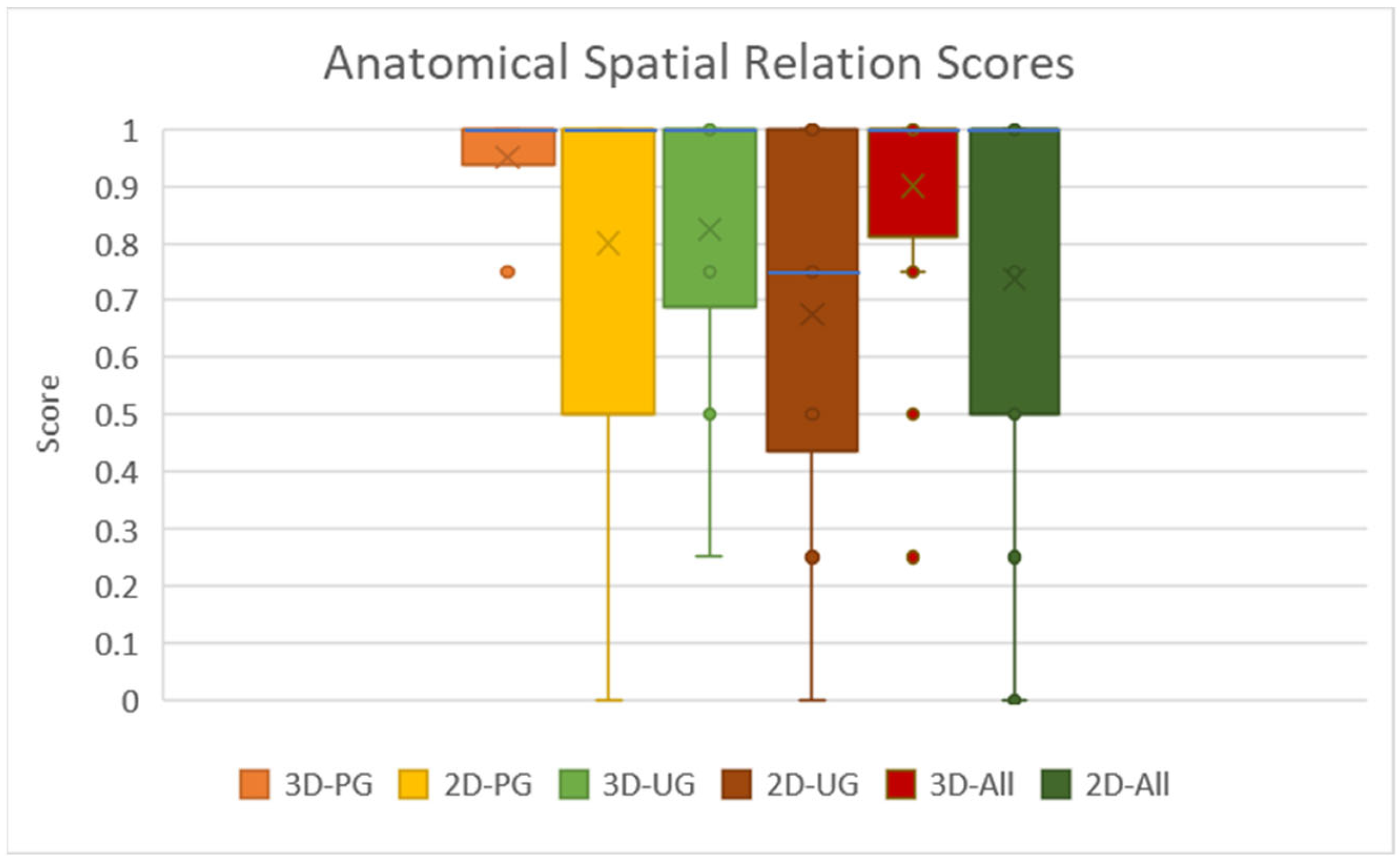
3. Results
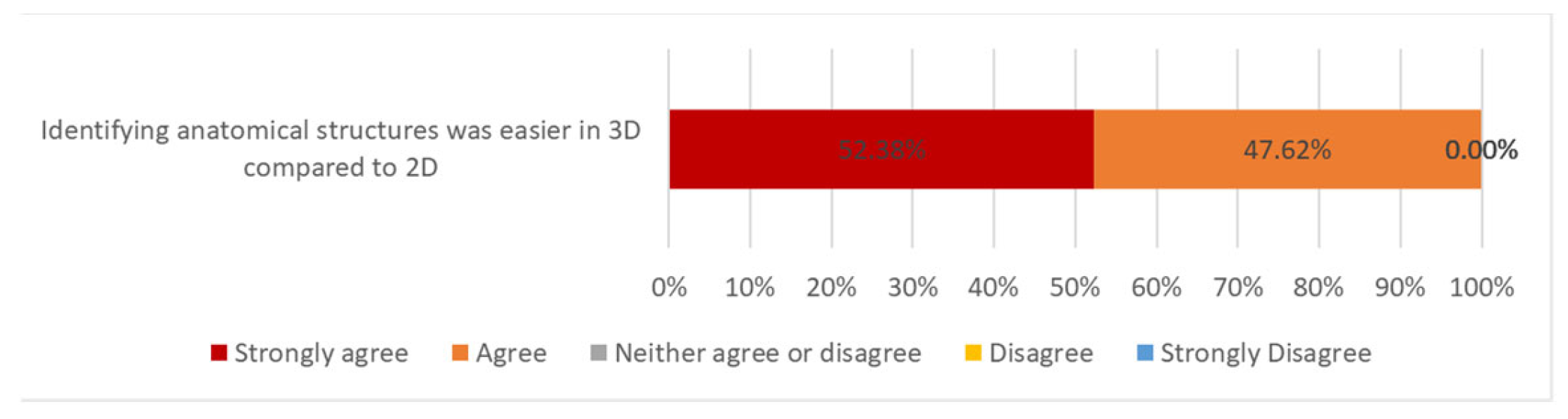
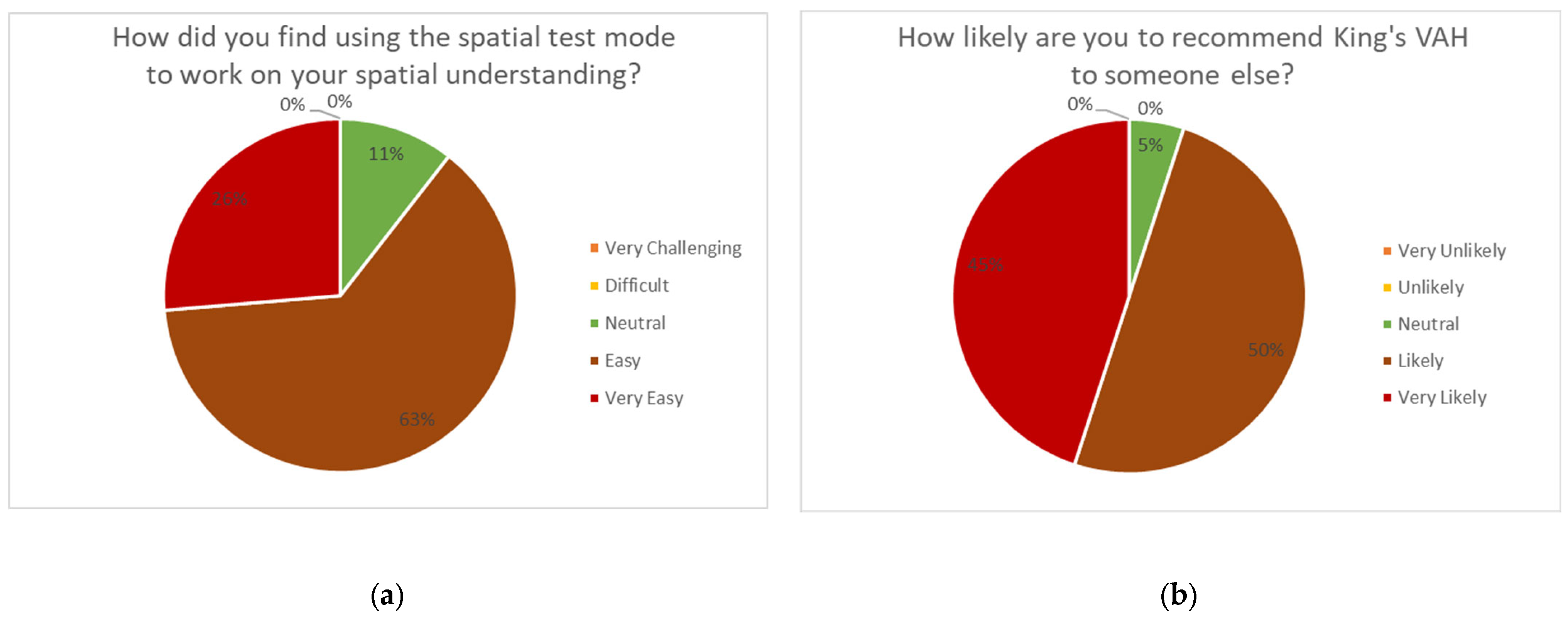
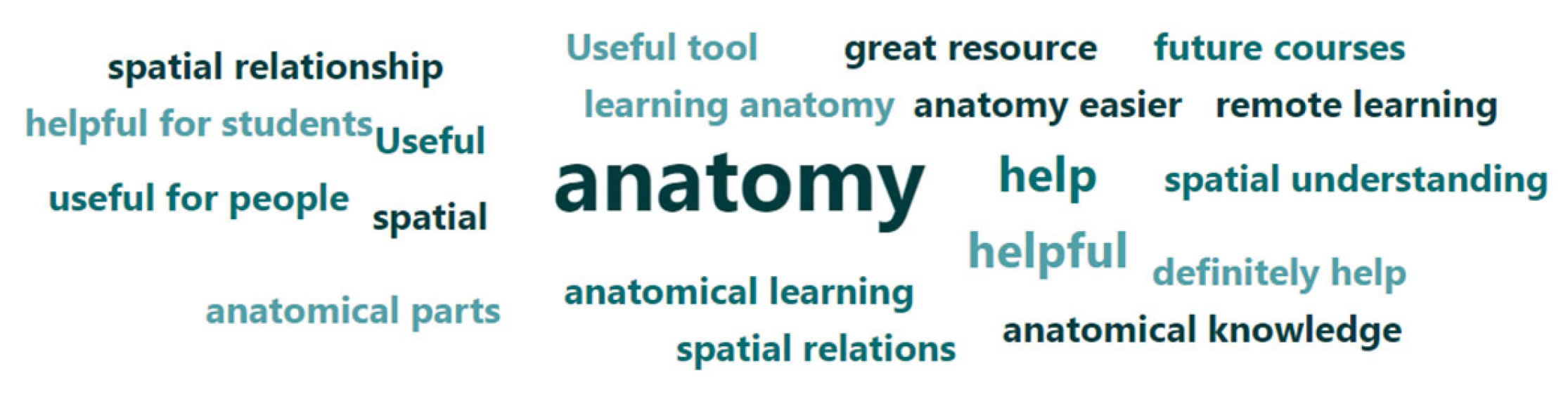
Qualitative Results
4. Discussion and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Böckers, A.; Jerg-Bretzke, L.; Lamp, C.; Brinkmann, A.; Traue, H.C.; Böckers, T.M. The Gross Anatomy Course: An Analysis of Its Importance. Anat. Sci. Educ. 2010, 3, 3–11. [Google Scholar] [CrossRef] [PubMed]
- McCuskey, R.S.; Carmichael, S.W.; Kirch, D.G. The Importance of Anatomy in Health Professions Education and the Shortage of Qualified Educators. Acad. Med. 2005, 80, 349–351. [Google Scholar] [CrossRef] [PubMed]
- Rowland, S.; Ahmed, K.; Davies, D.C.; Ashrafian, H.; Patel, V.; Darzi, A.; Paraskeva, P.A.; Athanasiou, T. Assessment of Anatomical Knowledge for Clinical Practice: Perceptions of Clinicians and Students. Surg. Radiol. Anat. 2011, 33, 263–269. [Google Scholar] [CrossRef] [PubMed]
- Azer, S.A.; Eizenberg, N. Do We Need Dissection in an Integrated Problem-Based Learning Medical Course? Perceptions of First- and Second-Year Students. Surg. Radiol. Anat. 2007, 29, 173–180. [Google Scholar] [CrossRef] [PubMed]
- The Expansion of Medical Student Numbers in the United Kingdom Medical Schools Council Position Paper; Medical Schools Council: London, UK, 2021; Available online: https://www.medschools.ac.uk/media/2899/the-expansion-of-medical-student-numbers-in-the-united-kingdom-msc-position-paper-october-2021.pdf (accessed on 29 November 2022).
- AAMC. U.S. Medical School Enrollment Rises 30%. Available online: https://www.aamc.org/news-insights/us-medical-school-enrollment-rises-30 (accessed on 12 January 2023).
- Habicht, J.L.; Kiessling, C.; Winkelmann, A. Bodies for Anatomy Education in Medical Schools: An Overview of the Sources of Cadavers Worldwide. Acad. Med. 2018, 93, 1293–1300. [Google Scholar] [CrossRef] [PubMed]
- Singh, V.; Kharb, P. A Paradigm Shift from Teaching to Learning Gross Anatomy: Meta-Analysis of Implications for Instructional Methods. J. Anat. Soc. India 2013, 62, 84–89. [Google Scholar] [CrossRef]
- In the U.S. Market for Human Bodies, Anyone Can Sell the Donated Dead. Available online: https://www.reuters.com/investigates/special-report/usa-bodies-brokers/ (accessed on 12 January 2023).
- Heizenrader. Why Virtual Cadavers Are a Wise Investment for Medical Schools. Available online: https://heizenrader.com/why-virtual-cadavers-are-a-wise-investment-for-medical-schools/ (accessed on 12 January 2023).
- Ayittey, F.K.; Ayittey, M.K.; Chiwero, N.B.; Kamasah, J.S.; Dzuvor, C. Economic Impacts of Wuhan 2019-NCoV on China and the World. J. Med. Virol. 2020, 92, 473–475. [Google Scholar] [CrossRef] [PubMed]
- UNESCO’s Education Response to COVID-19. Available online: https://en.unesco.org/covid19/educationresponse/support (accessed on 8 August 2022).
- Tóth, Á.; Pentelényi, P.; Tóth, P. Virtual Learning Aspects of Curriculum Development in Technical Teacher Training. In Proceedings of the 2006 International Conference on Intelligent Engineering Systems, London, UK, 26–28 June 2006; pp. 308–313. [Google Scholar] [CrossRef]
- Berney, S.; Bétrancourt, M.; Molinari, G.; Hoyek, N. How Spatial Abilities and Dynamic Visualizations Interplay When Learning Functional Anatomy with 3D Anatomical Models. Anat. Sci. Educ. 2015, 8, 452–462. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, K. Supporting Students with Varied Spatial Reasoning Abilities in the Anatomy Classroom. Teach. Innov. Proj. 2012, 2. Available online: https://ojs.lib.uwo.ca/index.php/tips/article/view/3576 (accessed on 29 November 2022).
- Bogomolova, K.; Hierck, B.P.; van der Hage, J.A.; Hovius, S.E.R. Anatomy Dissection Course Improves the Initially Lower Levels of Visual-Spatial Abilities of Medical Undergraduates. Anat. Sci. Educ. 2020, 13, 333–342. [Google Scholar] [CrossRef] [PubMed]
- Gonzales, R.A.; Ferns, G.; Vorstenbosch, M.A.T.M.; Smith, C.F. Does Spatial Awareness Training Affect Anatomy Learning in Medical Students? Anat. Sci. Educ. 2020, 13, 707–720. [Google Scholar] [CrossRef] [PubMed]
- Hegarty, M.; Waller, D. A Dissociation between Mental Rotation and Perspective-Taking Spatial Abilities. Intelligence 2004, 32, 175–191. [Google Scholar] [CrossRef]
- Preece, D.; Williams, S.B.; Lam, R.; Weller, R. “Let’s Get Physical”: Advantages of a Physical Model over 3D Computer Models and Textbooks in Learning Imaging Anatomy. Anat. Sci. Educ. 2013, 6, 216–224. [Google Scholar] [CrossRef] [PubMed]
- Marks, S.C., Jr. The Role of Three-Dimensional Information in Health Care and Medical Education: The Implications for Anatomy and Dissection. Clin. Anat. 2000, 13, 448–452. [Google Scholar] [CrossRef] [PubMed]
- Alioscopy. How Does It Work? Available online: https://www.alioscopy.com/en/principles.php (accessed on 30 September 2022).
- Looking Glass Documentation. How the Looking Glass Works. Available online: https://docs.lookingglassfactory.com/keyconcepts/how-it-works (accessed on 30 September 2022).
- Looking Glass Portrait. Available online: https://lookingglassfactory.com/looking-glass-portrait (accessed on 4 November 2022).
- CNET. Lume Pad Brings Back Glasses-Free 3D—This Time on an Android Tablet. Available online: https://www.cnet.com/tech/computing/lume-pad-brings-glasses-free-3d-back-again-on-an-android-tablet/ (accessed on 4 November 2022).
- Kickstarter. Looking Glass Portrait by Looking Glass. Available online: https://www.kickstarter.com/projects/lookingglass/looking-glass-portrait/description (accessed on 30 September 2022).
- Narita, Y.; Tsukagoshi, S.; Suzuki, M.; Miyakita, Y.; Ohno, M.; Arita, H.; Saito, Y.; Kokojima, Y.; Watanabe, N.; Moriyama, N.; et al. Usefulness of a Glass-Free Medical Three-Dimensional Autostereoscopic Display in Neurosurgery. Int. J. Comput. Assist. Radiol. Surg. 2014, 9, 905–911. [Google Scholar] [CrossRef] [PubMed]
- Silvestri, M.; Ranzani, T.; Argiolas, A.; Vatteroni, M.; Menciassi, A. A Multi-Point of View 3D Camera System for Minimally Invasive Surgery. Procedia Eng. 2012, 47, 1211–1214. [Google Scholar] [CrossRef]
- Luursema, J.-M.; Verwey, W.B.; Editor, A.; Kumar Tripathi, A. The Contribution of Dynamic Exploration to Virtual Anatomical Learning. Adv. Hum. Comput. Interact. 2011, 2011, 965342. [Google Scholar] [CrossRef]
- Di Natale, A.F.; Repetto, C.; Riva, G.; Villani, D. Immersive Virtual Reality in K-12 and Higher Education: A 10-Year Systematic Review of Empirical Research. Br. J. Educ. Technol. 2020, 51, 2006–2033. [Google Scholar] [CrossRef]
- Sinha, S.; DeYoung, V.; Chan, S.; Ives, R.; Lohit, S.; Reis, I.; Touliopoulos, E.; Nehru, A.; Mitchell, J.P.; Brewer-Deluce, D.; et al. Evaluating Autostereoscopy (AlioscopyTM) Use for Anatomy Education. FASEB J. 2022, 36. [Google Scholar] [CrossRef]
- Quizlet. Directional Terms Anatomy and Physiology Diagram. Available online: https://quizlet.com/424696628/directional-terms-anatomy-and-physiology-diagram/ (accessed on 27 November 2022).







Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Otoo, E.-M.A.; Leibowitz, H.; Wong, O.; Rhode, K. Using a Portable Autostereoscopic Screen to Improve Anatomy Teaching and Learning. Anatomia 2023, 2, 88-98. https://doi.org/10.3390/anatomia2010008
Otoo E-MA, Leibowitz H, Wong O, Rhode K. Using a Portable Autostereoscopic Screen to Improve Anatomy Teaching and Learning. Anatomia. 2023; 2(1):88-98. https://doi.org/10.3390/anatomia2010008
Chicago/Turabian StyleOtoo, Elsa-Marie A., Hannah Leibowitz, Oliver Wong, and Kawal Rhode. 2023. "Using a Portable Autostereoscopic Screen to Improve Anatomy Teaching and Learning" Anatomia 2, no. 1: 88-98. https://doi.org/10.3390/anatomia2010008