
Presumed Presence of Extensor Indicis et Digiti Medii Communis Muscle in a 70-Year-Old White Male Donor
by
 ,
,
Isabella Penkwitz
1 ,
,
Gary Wind
2,
Elizabeth Maynes
2,
Maria Ximena Leighton
2 and
Guinevere Granite
2,*
1
F. Edward Hebert School of Medicine, Uniformed Services University of the Health Sciences, Bethesda, MD 20814, USA
2
Department of Surgery, Uniformed Services University of the Health Sciences, Bethesda, MD 20814, USA
*
Author to whom correspondence should be addressed.
Anatomia 2023, 2(1), 109-116; https://doi.org/10.3390/anatomia2010010
Submission received: 11 January 2023
/
Revised: 24 February 2023
/
Accepted: 14 March 2023
/
Published: 16 March 2023
(This article belongs to the Special Issue Advances in Anatomy and Its History)
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:Forearm extensor muscle variations can be diverse and, in some instances, rare. During a routine anatomical dissection of human cadaveric donors during the 2021 first-year medical gross anatomy course and 2021 graduate nursing advanced anatomy course at the Uniformed Services University of the Health Sciences, bilateral agenesis of the extensor carpi ulnaris muscle was noted in one 70-year-old white male donor. This variation is described as extremely rare in the literature. The presence of an extensor indicis et digiti medii tendon, a variant of the extensor indicis tendon, appeared to be evident in post-dissection photographs on the left hand. The presence of a duplicated extensor indicis proprious tendon appears to be evident on the right hand. However, further inspection of this region was impeded as the body was sent for cremation prior to the variation being identified. The presence of various juncturae tendinum was also noted bilaterally. Reported prevalence of extensor indicis muscle variants ranges from 0.75% to 13%, depending on the specific type or grouping of variations observed. Knowledge of variations in the extensor compartment of the forearm and wrist is crucial for orthopedic surgeons and specialists. Alteration of surgical approaches may be necessary if such a variation is present. Such variations can be options for grafts, resulting in minimal functional change to the grafted area due to the continued existence of other muscles performing similar functions. Knowledge of such variations, and alternative, synonymous names for them, is also important for anatomy instructors, who may need to assist students in identifying these rare variations during anatomical dissection.
1. Introduction
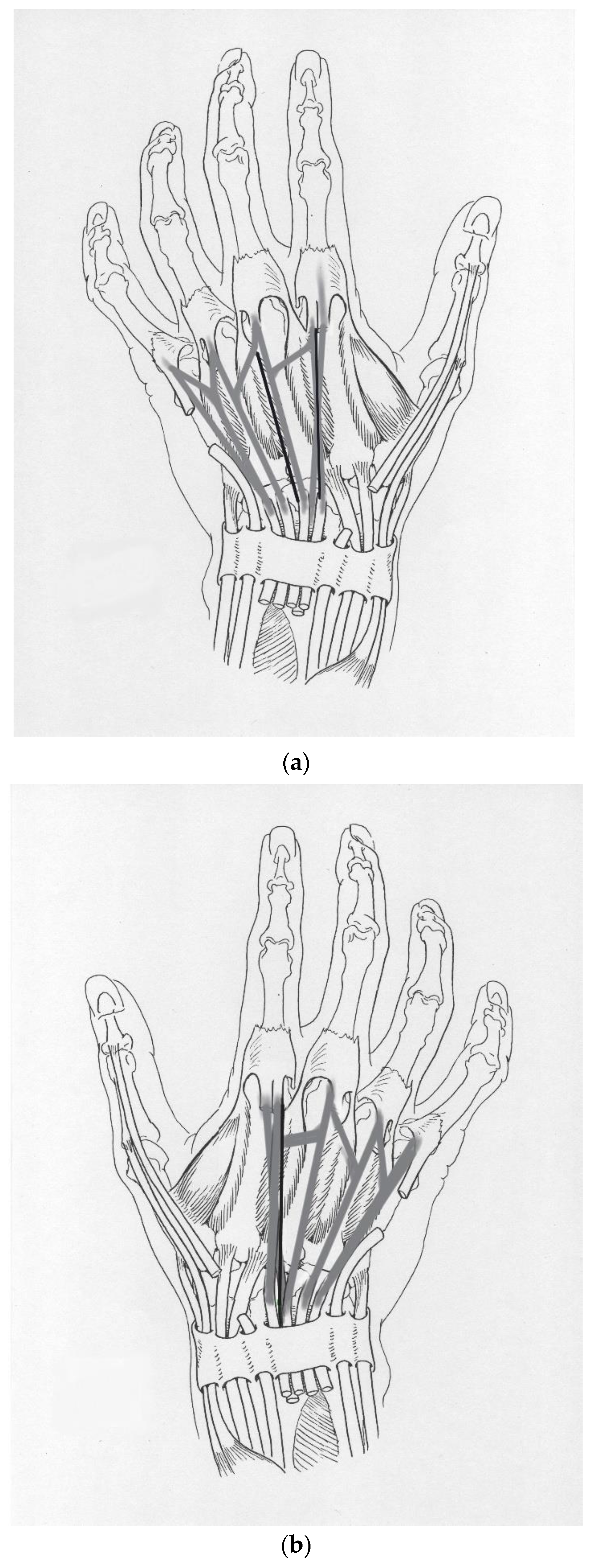
The extensor compartment of the forearm and wrist in humans can have multiple anatomical variations. Many of these variations are asymptomatic and incidentally found during surgery, trauma response, or assessments of the hand in instances of pain. The extensor indicis et digiti medii muscle (EIMe) originates from the extensor indicis proprius muscle (EIP) (Figure 1a). It plays a role in the extension of the second finger. The origin of the EIP varies between the ulna, radius, carpus, or interosseous membrane [1]. More unusual origins for the EIP include the lunate, scaphoid, and capitate bones with termination at the head of the proximal phalanx of the index finger or second finger [1]. The muscle belly of the EIP runs deep to the extensor digitorum communis tendons (EDCs) and is found rather invariably among humans, gorillas, and chimpanzees [1,2]. Variations in size, origin, insertion, duplications, and/or supernumerary tendons, however, can be found [1,2]. Another variant of the EIP is a duplicated EIP (DEIP), which is a complete duplication of the EIP muscle and should not be confused with a distal splitting to have multiple tendons (Figure 1b).
The EIMe and DEIP are categorized as “supernumerary tendons, with normal muscle origins” [1]. In the literature, supernumerary tendons are classified as: complete duplication of the EIP tendon, separate muscles coexisting with normal extensor pollicis longus (EPL) and EIP while providing tendons to the first and second fingers, the extensor medii proprius muscle (EMP) and extensor indicis et medii communis muscle (EIMC), and special tendons to the second, third, and fourth fingers [1]. Specifically, duplicated tendons that insert at the second and third fingers have been observed, with the combined muscle referred to as the EIMC and the muscle inserting on the middle finger as the EMP [1]. It should be noted that the extensor digiti medii and EMP are synonymous terms, but throughout this work, EMP will be used. Similarly, the EIMC can also be referred to as the extensor indicis et medii proprius or extensor indicis et medii accessorius [3,4,5,6,7,8]. We will use EIMC for consistency. Throughout this work, EIMe refers to the muscle that splits off from the EIMC, which then extends onto the second finger. It should be noted that because the EIMe has a different origin and insertion points, it is considered a separate anatomical variant from a tendinous slip. As a muscular variant of the EIP, the EIMe also plays a role in independent digit extension. Specific rates for the presence of the EIMe were difficult to find. Multiple works, however, have reported the prevalence of other extensor tendon variants, including the EIP, EMP, EIMC, and extensor pollicis et indicis muscle tendon (EPI). Yammine (2015) describes the systematic review and meta-analysis of 21 studies and reports a pooled prevalence estimate of 1.6% for the EIMC, specifically [2]. The article further states that the EIMC was most often found in North American populations when compared to European, Indian, and Japanese populations [2]. We presume the EIMC was present in the left hand of this donor if the observed variant in the first finger was correctly identified as the EIMe. Because of the limited visibility in the photos taken for Granite et al. (2022) [8] and the subsequent cremation of the donor’s remains, it is not possible to reflect the superficial structures in order to obtain an unobstructed view of the muscle for more definitive identification as the EIMe. With respect to the DEIP, because it is a duplication, this variant serves the same function as a singular EIP. Historically, the prevalence of the DEIP has varied from 2.7% to 16%. Cauldwell et al. (1943) reported a prevalence of 2.7%, whereas Wood (1868) reported 9.3%, and von Schroeder (1995) reported 16% [1,6,9]. A DEIP involves a completely duplicated and robust muscle belly, which should not be confused with splitting into an additional distal slip.
The purpose of this case report is to alert surgeons and anatomists of the existence of the EIMe anatomical variation and the possibility that this variation may also be present in future patients or donors. It also serves to clarify any alternative, synonymous names for select variants that exist in the literature in order to reduce confusion.
2. Case Description
During routine anatomical dissection of human cadaveric donors during the 2021 first-year medical gross anatomy course and 2021 graduate nursing advanced anatomy course at the Uniformed Services University of the Health Sciences, Granite et al. (2022) found a 70-year-old White male donor with bilateral agenesis of the extensor carpi ulnaris muscle (ECU) [10]. The donor’s cause of death was pneumonia.
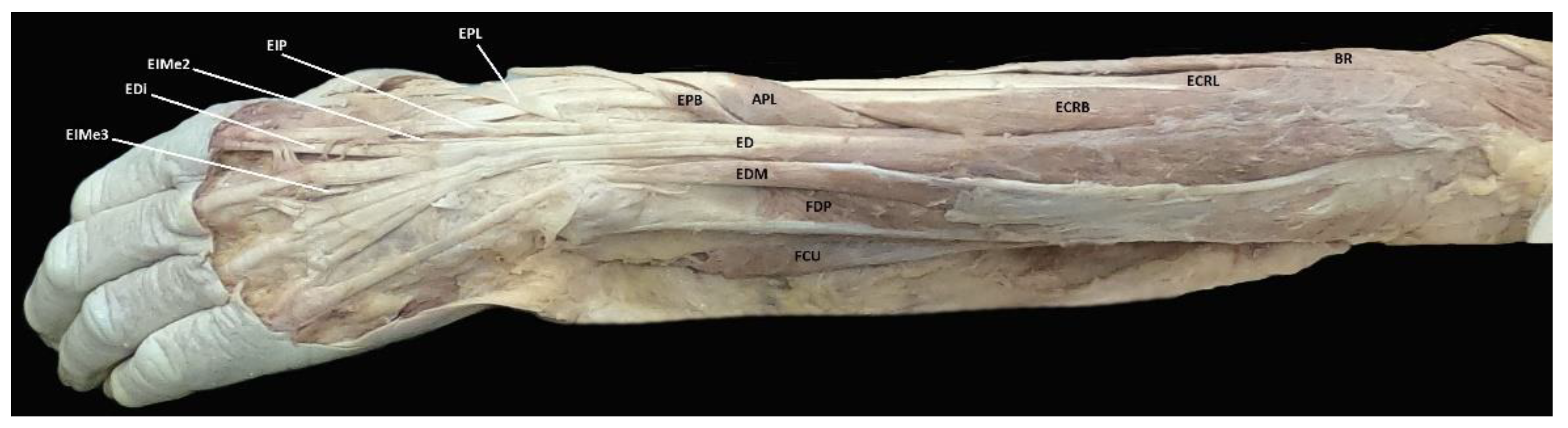
After the case report on bilateral agenesis of the ECU was published in February 2022, we noted an unfamiliar muscle and tendon variant present on the left hand of the donor [10]. The variant in question was located on the dorsal aspect of the left hand and appeared to be a separate tendon from both the extensor digitorum muscle (ED) and EIP tendons. Because the donor was cremated, further dissection of the limb to remove the superficial tendons and determine the origin of the tendon in question was not possible. There are, however, other works describing the presence of a variant matching what was observed in this donor [1,2,3,4,5,6,7,8,11]. After reviewing descriptions of variants affecting the extensor compartment of the forearm and wrist, we have reason to believe that the tendon in question for this donor is the EIMe (Figure 2).
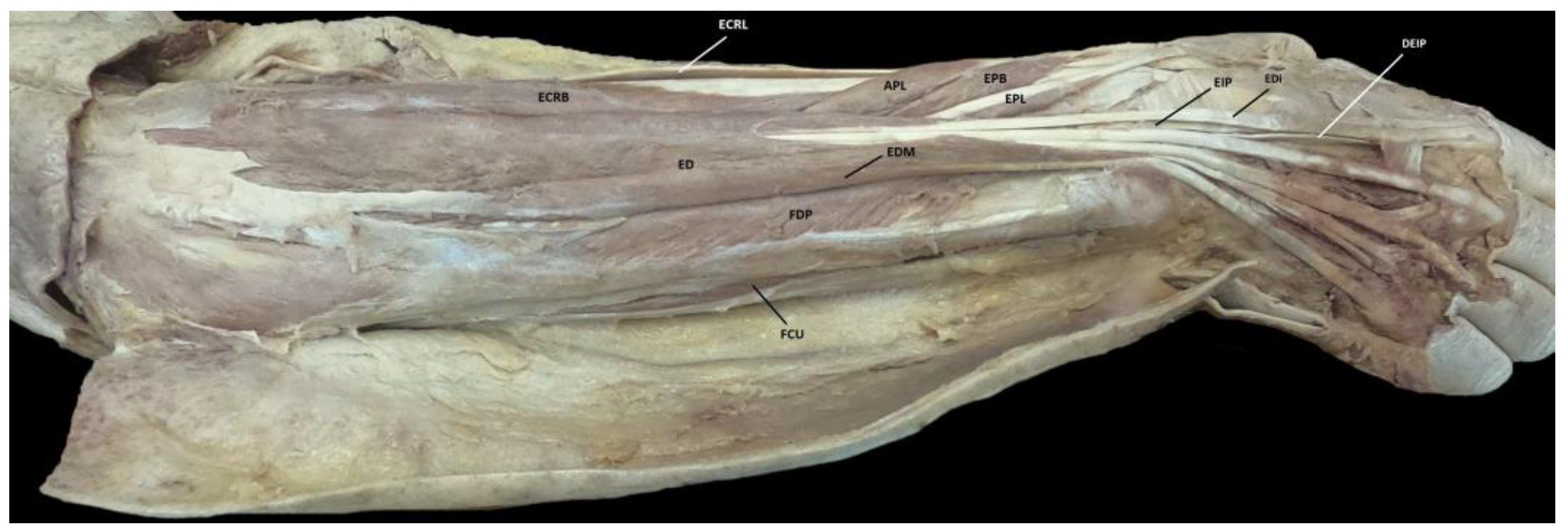
We noted that the EIMe is located radial to the ED tendon of the second finger on the left hand, but a different variant was present ulnar to the ED tendon of the second finger on the right hand (Figure 3). Because it is fairly robust, we believe that DEIP is a more appropriate designation of this variant rather than simply an additional distal slip.
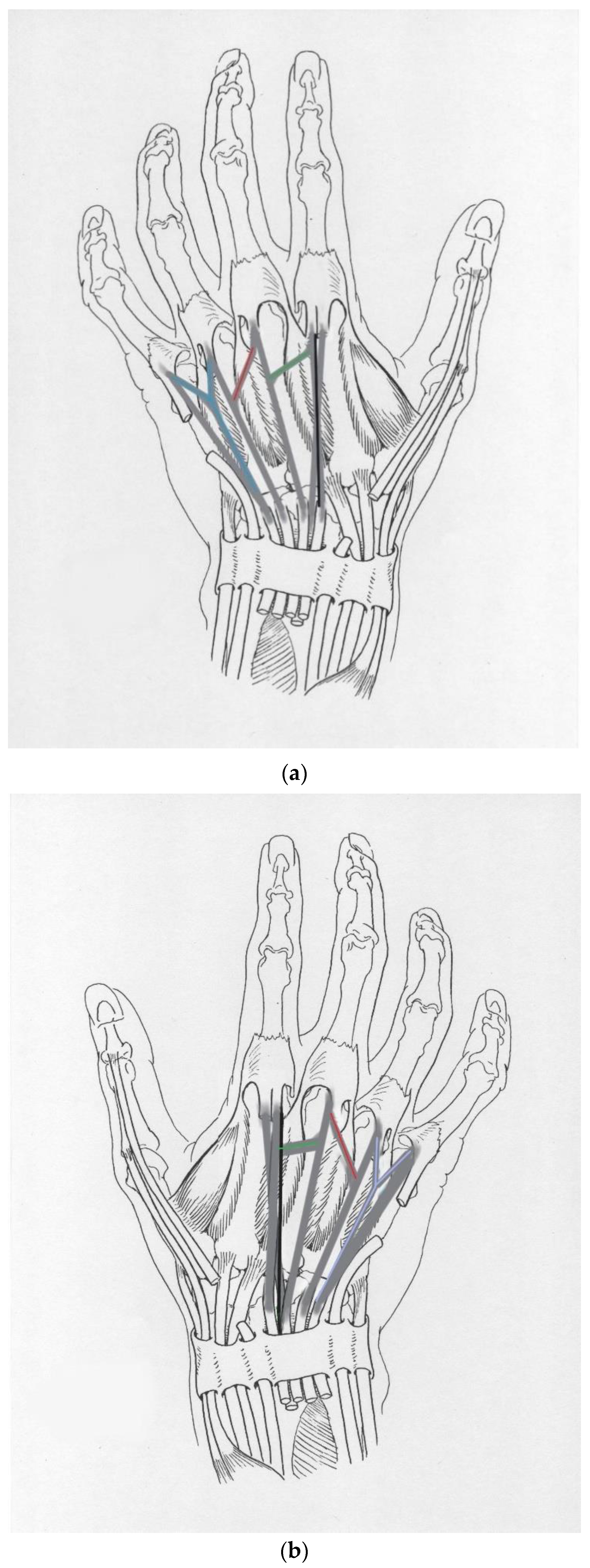
The presence of juncturae tendinum (JT) was also noted bilaterally (Figure 4a,b). Based on the classifications outlined by Abdel-Hamid et al. (2013), we believe there are at least six cumulative JTs in this donor [12]. Specifically, three JTs were noted in the left hand: a type 2 JT between the second and third digits, a type 3r JT between the third and fourth digits, and a type 3y JT between the fourth and fifth digits (Figure 4a). Three JTs were noted in the right hand: a type 2 JT between the second and third digits, a type 3r between the third and fourth digits, and a type 3y JT between the fourth and fifth digits (Figure 4b).
3. Discussion
Reported variations of the EIP and its tendon include one or more distal slips and attachment of slips to other digits, including the EMP, EIMC, and EPI. Yammine (2015) reported an EMP prevalence of 3.7%, with a bilateral variation being rarer, while prevalence of the EIMC tendon was 1.6%, and the prevalence of the EPI was 0.75% [2]. Yammine (2015) has cited variations in frequencies based on gender, ancestry, laterality, and side [2].
With respect to slips of the EIP, single-slip EIPs are the most common, whereas the prevalence steeply decreases with the increased number of slips [2,6]. Yammine (2015) reports a pooled prevalence estimate of 92.6%, 7.2%, and 0.3% for the single-, double-, and triple-slip EIP, respectively [2]. The single-slip variation frequently inserts on the ulnar side of the EDC of the second finger (EDC-index) in 98.3% [2]. The attachment location of these single-, double-, or triple-slip EIPs may also vary. Yammine (2015) reports a prevalence of 53.5% for additional EIP slips on the ulnar side of the ED to the second digit [2]. The ulnar location of the observed right-hand variant remains consistent with Yammine’s data. However, we believe that this observed variant is more robust than a typical extra slip of the EIP and is more likely to be a DEIP. The prevalence of a DEIP ranges from 2.7% to 16% [1,6,9].
Although the actions or functions may be similar for the tendinous slips of the ED to the second digit and the EIMe, the EIMe has its own muscle belly and origin and, as a result, is referenced as a distinctly different muscle in the anatomical variation literature [1,2,3,4,5,6,7,8,11].
Komiyama et al. (2019) reported variations of the EIP by classification of supernumerary muscles or tendons into four types, each with two subtypes [4]. However, they did not observe any cases of EIMC or EMIe and, therefore, did not include these variations in their subtype classifications. In general, it is agreed that, for the second finger, the most frequent variation of the EIP is the presence of a single supernumerary tendon, mostly occurring on the ulnar side of the ED tendon [4,6].
Embryological development of the upper limb begins at approximately 26 days after fertilization with the presence of the apical ectodermal ridge [13]. Of the four embryological developmental zones, the three that are relevant to this work are the zeugopod (future forearm), mesopod (future wrist), and autopod (future hand) [13]. After zones are established, cartilage and other cells begin to form joints, bones, tendons, and muscles. Muscle fibers can be found in the limb bud by week 7 of development [13]. Specific limb development occurs along three axes: proximodistal, anteroposterior, and dorsoventral. The proximodistal axis influences limb growth proximally to distally. The anteroposterior axis is important for developing ulnar and radial structures, with the Sonic Hedgehog gene (SHH) specifically affecting the development of the second and third fingers via chemical growth and differentiation signaling [13]. The dorsoventral axis is important for development of both the dorsal and ventral structures, with the Wnt family member 7A gene (WNT7A) in the dorsal ectoderm and LIM homeobox transcription factor 1 beta (LMX1B) in the dorsal mesoderm being responsible for the development of extensor tendons in the hand [13].
The EIP can be involved in pain syndromes, trauma, and tendon transfers during reconstructive surgery. Examples include external trauma, extensor indicis proprius syndrome [4], rheumatoid arthritis, and osteoarthritis [11]. In cases of reconstruction involving trauma, options for grafts depend on which ligaments are still present [14]. Grafts sourced from the extensor retinaculum or flexor digitorum superficialis are often used in finger reconstruction requiring joint stabilization [14]. The EIP is frequently used for tendon transfer following extensor rupture due to rheumatoid arthritis [14]. In cases where a DEIP is present, this could allow for tendon transfer of one EIP with preservation of the alternate EIP.
Similar to the EIP, the relevance for the EIMe likely revolves around the surgical possibilities. Currently recognized extra tendon sources aside from the EDC include the EIP, EMP, EIMC, EPI, and EDM [15]. Although clinical practice currently revolves around utilizing the EIP, further research could evaluate the legitimacy of using the EIMe for tendon transfer, if it is a robust graft source, in place of the EIP. Yammine (2019) determined that there is a 40% probability of finding extra slips and an 8.5% probability of an EIP variant tendon (EMP, EIMC, or EPI) being present [15]. Extra slips and EIP variant tendons can be used in reconstructive surgery [15]. If slips are to be used as replacement tendons, surgeons should remember that there are variations in their frequency based on ethnicity [15]. There is also the possibility of retaining second finger extension despite traditional EIP tendon transfer if the EIMe is present. Use of MRI to gain an understanding of each patient’s musculature within the hand can allow surgeons to alter approaches as needed.
Other considerations for the identified muscle and tendon variant of the left hand include the EMP, extensor digiti brevis manus muscle (EDBM), and extensor indicis brevis manus muscle (EIBM). The EMP originates at the ulna below the EIP and either inserts at the extensor aponeurosis of the third finger or splits to supply slips to both the second and third fingers [1]. Von Schroeder and Botte (1991) describe the EMP as a distinctly different muscle belly from the EIP that inserts into the third finger [5]. It is possible for the EMP to be fused to part of the EIP, making its identification difficult in some cases [1]. The EDBM originates from the ulna or ulnar half of the carpal bones, which is notably narrower when compared to the wider range of origins for the EIP [1]. It is described as a “short carpal extensor” that inserts either into the metacarpals or other extensor tendons of a respective digit [1]. Similar in name and origin to the EDBM, the EIBM is an EDBM variant with at least one muscle belly and/or tendon that is distinguishable from the EIP [1,16,17]. The EIBM inserts at either the proximal or distal phalanx of the second digit [16,17]. Like the EDBM, the EIBM can join extensor tendons, such as the EIP [1]. Interestingly, the EIBM and EIP coexistence has been reported by Esakkiammal et al. (2021), while EDBM and EIP presence may be mutually exclusive [16].
Bilateral presence of JT was also noted in the donor. Abdel-Hamid et al. (2013) defines JT as “short bands of connective tissue present between the adjacent extensor tendons on the dorsum of the hand” [12]. There are various classifications of JT based on the thickness of the connective tissue, whether it is filamentous or tendinous, and the shape or angle of the band’s connections [12]. Variations in incidence exist based on the type and location of the JT in the second, third, or fourth intermetacarpal spaces of the hand [12].
4. Conclusions
Although the extensor compartment of the forearm and hand can have extensive anatomical variations, not all variations are equally common. While the prevalence of the EMP is 3.7% and the EPI is 0.75%, the prevalence of the EIMC is 1.6% [2]. These variations are all quite rare in the literature. This may be due to a general decreased awareness of authors of their existence in patients or donors.
A major limitation of this case report was identifying the possible EIMe after the donor had been sent for incineration. Our hypothesis that the tendon and muscle observed inserting into the second and third digits of the left hand is the EIMe was based on the available images of the donor and the descriptions of the EIMe in other works. We also believe it is possible that the EIMC is also present if the identified variant is the EIMe, but no longer have the means to verify this suspicion. We believe the observed variant of the second digit on the right hand is a DEIP. In the same way, because the donor was cremated, this case report was limited in verifying a complete duplication of the EIP. However, because it is fairly robust, we believe that this is a more appropriate designation rather than simply an additional distal slip.
The importance of identifying anatomical variations is twofold: to alert anatomists of these possible variations that may have embryonic development origins, and to ensure surgeons are aware of alternate tendons that may prove useful during select procedures.
Author Contributions
Conceptualization, I.P. and G.G.; methodology, I.P.; formal analysis, I.P., M.X.L. and G.G.; investigation, I.P., M.X.L. and G.G.; resources, I.P.; writing—original draft preparation, I.P.; writing—review and editing, G.G. and E.M.; visualization, I.P., G.W. and G.G.; supervision, G.G. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
We would like to thank the families of our donors for their beneficent contribution. Without their generosity, this article would not have been possible. We would also like to thank Sara Chae for assisting us in our literature review.
Conflicts of Interest
The authors declare no conflict of interest.
Disclaimer
The opinions or assertions contained herein are the private ones of the author/speaker and are not to be construed as official or reflecting the views of the Department of Defense, the Uniformed Services University of the Health Sciences or any other agency of the U.S. Government. The contents of this presentation are the sole responsibility of the author(s) and do not necessarily reflect the views, opinions or policies of Uniformed Services University of the Health Sciences (USUHS), The Henry M. Jackson Foundation for the Advancement of Military Medicine, Inc., the Department of Defense (DoD) or the Departments of the Army, Navy, or Air Force. Mention of trade names, commercial products, or organizations does not imply endorsement by the U.S. Government.
References
- Anatomy Atlases: An Anatomy Digital Library—Curated by Ronald A. Bergman, Ph.D. Available online: http://www.anatomyatlases.org/AnatomicVariants/MuscularSystem/Text/E/25Extensor.shtml (accessed on 10 January 2023).
- Yammine, K. The prevalence of the extensor indicis tendon and its variants: A systematic review and meta-analysis. Surg. Radiol. Anat. 2015, 37, 247–254. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez, M.H.; Weinzweig, N.; Kay, T.; Grindel, S. Anatomy of the Extensor Tendons to the Index Finger. J. Hand Surg. 1996, 21, 988–991. [Google Scholar] [CrossRef] [PubMed]
- Komiyama, M.; New, T.M.; Toyota, N.; Shimada, Y. Variations of the Extensor Indicis Muscle and Tendon. J. Hand Surg. (Br. Eur. Vol.) 1999, 24, 575–578. [Google Scholar] [CrossRef] [PubMed]
- Von Schroeder, H.P.; Botte, M. The extensor medii proprius and anomalous extensor tendons to the long finger. J. Hand Surg. 1991, 16, 1141–1145. [Google Scholar] [CrossRef] [PubMed]
- Von Schroeder, H.P.; Botte, M.J. Anatomy of the Extensor Tendons of the Fingers: Variations and Multiplicity. J. Hand Surg. 1995, 20, 27–34. [Google Scholar] [CrossRef] [PubMed]
- Yalcine, B.; Kutoglu, T.; Ozan, H.; Gurbuz, H. The Extensor Indicis Et Medii Communis. Clin. Anat. 2006, 19, 112–114. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, Y. Anatomical Study on the Extensor Digitorum Profundus Muscle in the Japanese. Okajimas Folia Anat. Jap. 1990, 66, 339–354. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cauldwell, E.W.; Anson, B.J.; Wright, R.R. The extensor indicis proprius muscle: A study of 263 consecutive specimens. Q. Bull. Northwestern Univ. Med. Sch. 1943, 17, 267–279. [Google Scholar]
- Granite, G.; Maynes, E.; Leighton, M.X.; Wind, G.; Nesti, L. Bilateral Agenesis of the Extensor Carpi Ulnaris Muscle of a 70 Year-Old White Male Donor. J. Surg. 2022, 7, 1470. [Google Scholar] [CrossRef]
- Fischer, K.; Breitfeld, T.; Damert, H.G.; Rothkotter, H.J. Multiple Variations of Extensor Muscles in a Single Hand. Int. J. Anat. Var. 2016, 9, 32–34, eISSN: 1308-4038. Available online: https://www.pulsus.com/scholarly-articles/multiple-variations-of-extensor-muscles-in-a-single-hand.pdf (accessed on 10 January 2023).
- Abdel-Hamid, G.A.; El-Beshbishy, R.A.; Abdel Aal, I.H. Anatomical variations of the hand extensors. Folia Morphol. 2013, 72, 249–257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Qattan, M.M.; Kozin, S.H. Update on Embryology of the Upper Limb. J. Hand Surg. 2013, 38, 1835–1844. [Google Scholar] [CrossRef] [PubMed]
- UpToDate—Surgical Reconstruction of the Upper Extremity by Kevin C. Chung and Hidemasa Yoneda. Available online: https://www-uptodate-com.usu01.idm.oclc.org/contents/surgical-reconstruction-of-the-upper-extremity (accessed on 22 July 2022).
- Yammine, K. Predicting Tendon Tissue Grafting Source From the extensors of Long Fingers: A Systematic Review of Cadaveric Studies. HAND 2019, 14, 651–657. [Google Scholar] [CrossRef] [PubMed]
- Esakkiammal, N.; Chauhan, R.; Sharma, R. Clinical Significance of Presence of Extensor Indicis Brevis Manus—A Case Report. J. Clin. Diagn. Res. 2017, 11, 5–6. [Google Scholar] [CrossRef]
- Solomon, D.; Atlaw, D.; Gezahegn, H. Extensor Indicis Brevis Muscle: A Case Report. Int. Med. Case Rep. J. 2021, 14, 323. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
(a) Schematic of the left hand with the extensor indicis et digiti medii muscle (EIMe) indicated by the thick black lines. (b) Schematic of the right hand with the duplicated extensor indicis proprius muscle (DEIP) indicated by the thick black line.
Figure 1.
(a) Schematic of the left hand with the extensor indicis et digiti medii muscle (EIMe) indicated by the thick black lines. (b) Schematic of the right hand with the duplicated extensor indicis proprius muscle (DEIP) indicated by the thick black line.

Figure 2.
Facilitated display highlighting the following left forearm muscles: APL = Abductor Pollicis Longus Muscle, BR = Brachioradialis Muscle, ECRB = Extensor Carpi Radialis Brevis Muscle, ECRL = Extensor Carpi Radialis Longus Muscle, ED = Extensor Digitorum Muscle, EDi = Extensor Digitorum Muscle Tendon to the Index Finger, EDM = Extensor Digiti Minimi Muscle, EIP = Extensor Indicis Proprius Muscle, EIMe2 = Extensor Indicis et Digiti Medii Muscle Tendon of the Second Digit, EIMe3 = Extensor Indicis et Digiti Medii Muscle Tendon of the Third Digit, EPB = Extensor Pollicis Brevis Muscle, EPL = Extensor Pollicis Longus Muscle, and FCU = Flexor Carpi Ulnaris Muscle.
Figure 2.
Facilitated display highlighting the following left forearm muscles: APL = Abductor Pollicis Longus Muscle, BR = Brachioradialis Muscle, ECRB = Extensor Carpi Radialis Brevis Muscle, ECRL = Extensor Carpi Radialis Longus Muscle, ED = Extensor Digitorum Muscle, EDi = Extensor Digitorum Muscle Tendon to the Index Finger, EDM = Extensor Digiti Minimi Muscle, EIP = Extensor Indicis Proprius Muscle, EIMe2 = Extensor Indicis et Digiti Medii Muscle Tendon of the Second Digit, EIMe3 = Extensor Indicis et Digiti Medii Muscle Tendon of the Third Digit, EPB = Extensor Pollicis Brevis Muscle, EPL = Extensor Pollicis Longus Muscle, and FCU = Flexor Carpi Ulnaris Muscle.

Figure 3.
Facilitated display highlighting the following right forearm muscles: APL = Abductor Pollicis Longus Muscle, ECRB = Extensor Carpi Radialis Brevis Muscle, ECRL = Extensor Carpi Radialis Longus Muscle, ED = Extensor Digitorum Muscle, EDi = Extensor Digitorum Muscle Tendon to the Index Finger, EDM = Extensor Digiti Minimi Muscle, EIP = Extensor Indicis Proprius Muscle, DEIP = Duplicated Extensor Indicis Proprius Muscle Tendon, EPB = Extensor Pollicis Brevis Muscle, EPL = Extensor Pollicis Longus Muscle, and FCU = Flexor Carpi Ulnaris Muscle.
Figure 3.
Facilitated display highlighting the following right forearm muscles: APL = Abductor Pollicis Longus Muscle, ECRB = Extensor Carpi Radialis Brevis Muscle, ECRL = Extensor Carpi Radialis Longus Muscle, ED = Extensor Digitorum Muscle, EDi = Extensor Digitorum Muscle Tendon to the Index Finger, EDM = Extensor Digiti Minimi Muscle, EIP = Extensor Indicis Proprius Muscle, DEIP = Duplicated Extensor Indicis Proprius Muscle Tendon, EPB = Extensor Pollicis Brevis Muscle, EPL = Extensor Pollicis Longus Muscle, and FCU = Flexor Carpi Ulnaris Muscle.

Figure 4.
(a) Schematic of the left hand highlighting the juncturae tendinum (JT): a type 2 JT between the second and third digits (highlighted in green), a type 3r JT between the third and fourth digits (highlighted in red), and a type 3y JT between the fourth and fifth digits (highlighted in blue). (b) Schematic of the right hand highlighting the juncturae tendinum (JT): a type 2 JT between the second and third digits (highlighted in green), a type 3r between the third and fourth digits (highlighted in red), and a type 3y JT between the fourth and fifth digits (highlighted in light purple).
Figure 4.
(a) Schematic of the left hand highlighting the juncturae tendinum (JT): a type 2 JT between the second and third digits (highlighted in green), a type 3r JT between the third and fourth digits (highlighted in red), and a type 3y JT between the fourth and fifth digits (highlighted in blue). (b) Schematic of the right hand highlighting the juncturae tendinum (JT): a type 2 JT between the second and third digits (highlighted in green), a type 3r between the third and fourth digits (highlighted in red), and a type 3y JT between the fourth and fifth digits (highlighted in light purple).

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Penkwitz, I.; Wind, G.; Maynes, E.; Leighton, M.X.; Granite, G. Presumed Presence of Extensor Indicis et Digiti Medii Communis Muscle in a 70-Year-Old White Male Donor. Anatomia 2023, 2, 109-116. https://doi.org/10.3390/anatomia2010010
AMA Style
Penkwitz I, Wind G, Maynes E, Leighton MX, Granite G. Presumed Presence of Extensor Indicis et Digiti Medii Communis Muscle in a 70-Year-Old White Male Donor. Anatomia. 2023; 2(1):109-116. https://doi.org/10.3390/anatomia2010010
Chicago/Turabian StylePenkwitz, Isabella, Gary Wind, Elizabeth Maynes, Maria Ximena Leighton, and Guinevere Granite. 2023. "Presumed Presence of Extensor Indicis et Digiti Medii Communis Muscle in a 70-Year-Old White Male Donor" Anatomia 2, no. 1: 109-116. https://doi.org/10.3390/anatomia2010010