

A Missing Flexor Digitorum Brevis Tendon and Its Relationship to Sex and Ancestry: Evaluation in Hispanic Population
 ,
, {kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Acquisition
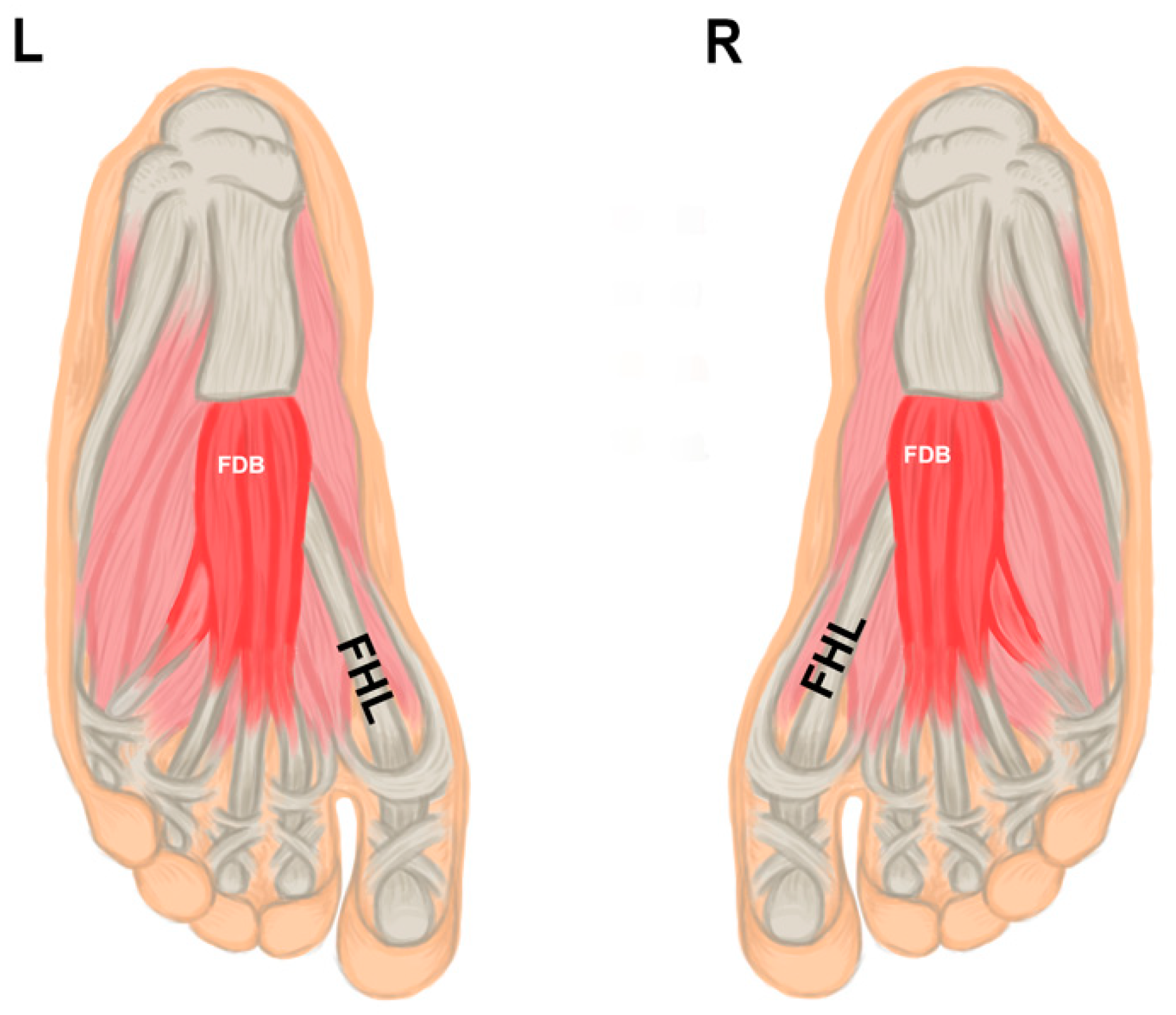
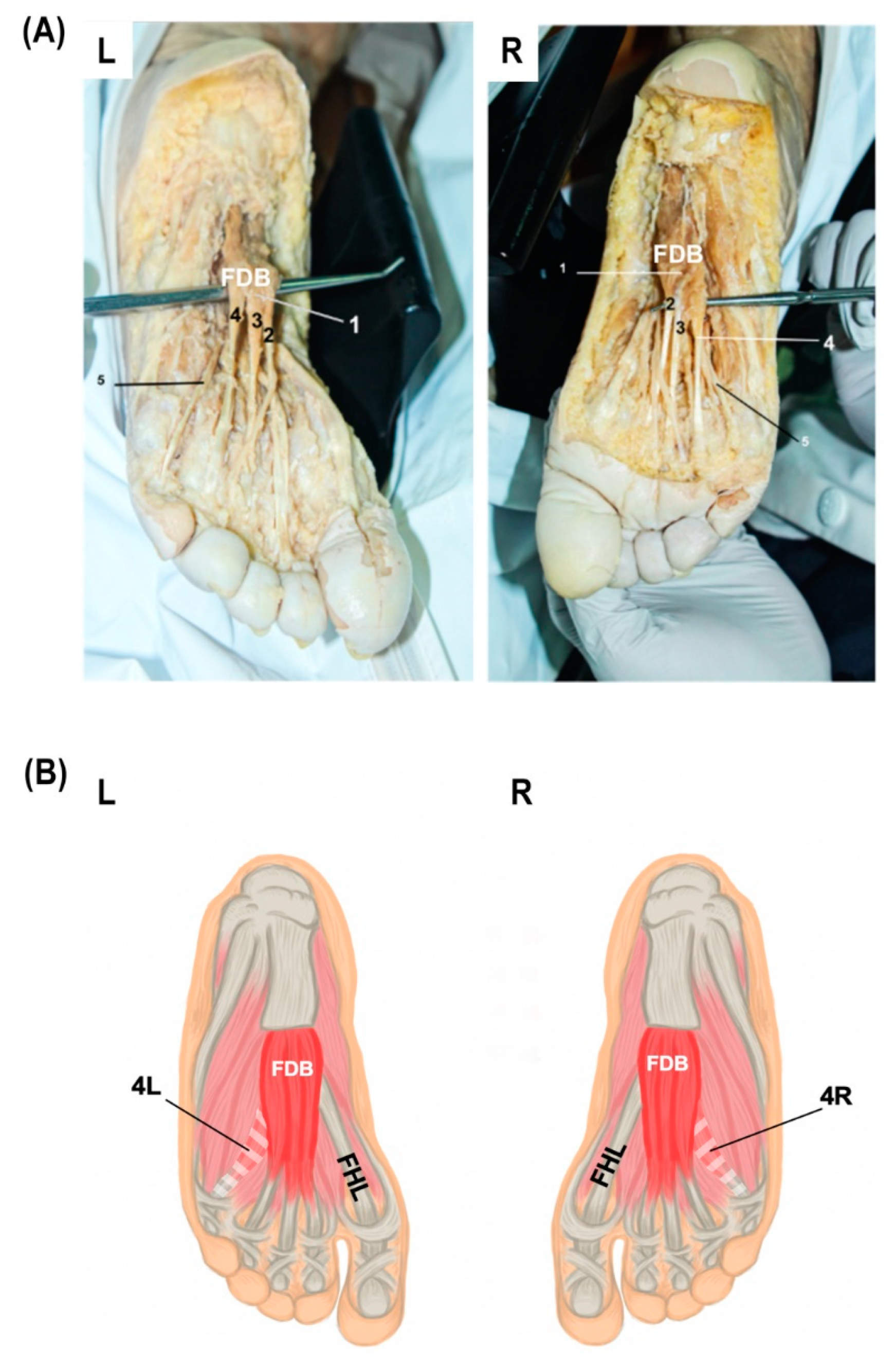
2.2. Plantar Aspect of the Foot Dissection
2.3. Statistical Analysis
2.4. Ethical and Bioethical Principles
3. Results
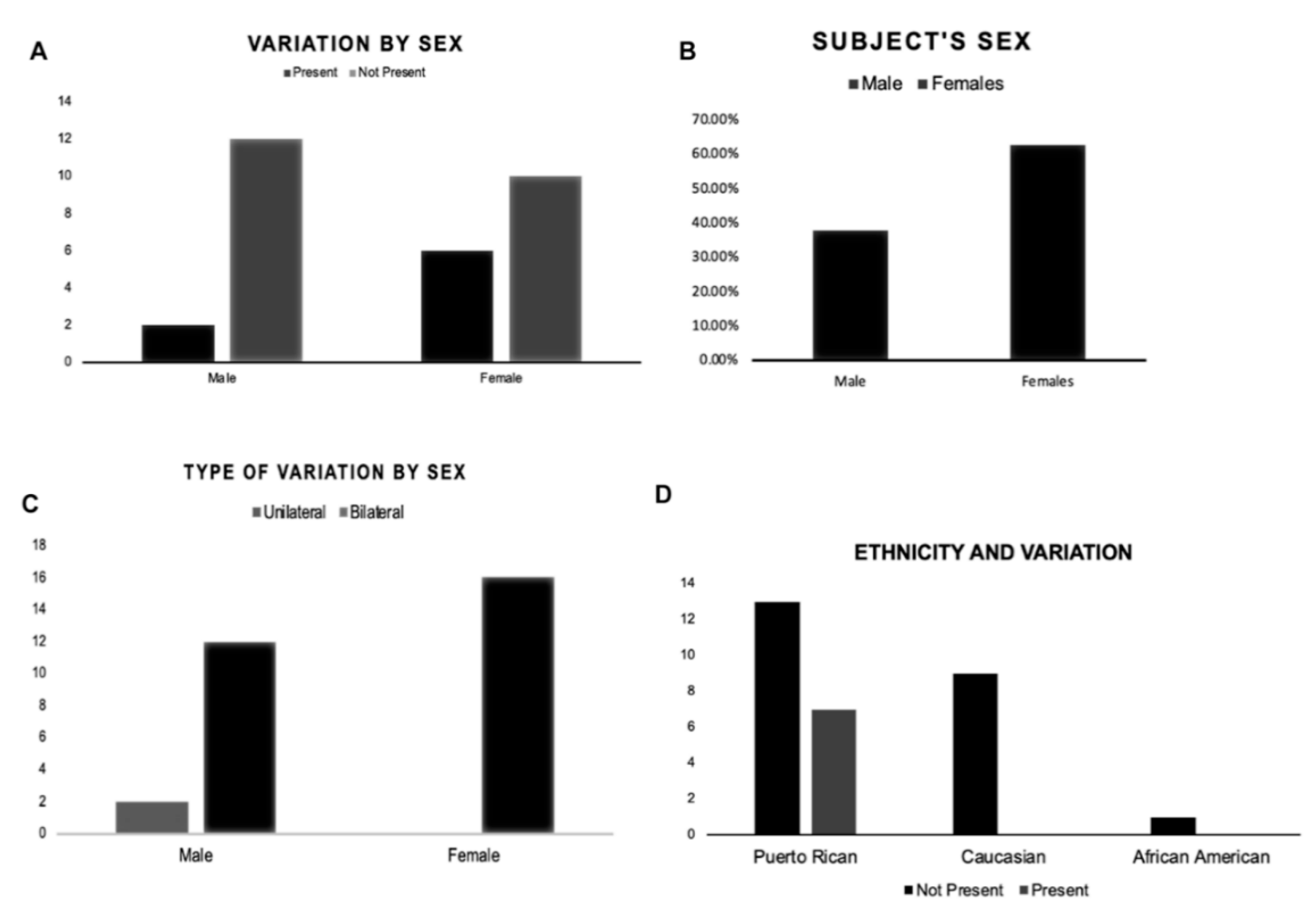
3.1. Descriptive Statistics
3.2. Association between Sex, Ancestry, and Presence or Absence of the FDB Fourth Tendon
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bergmann, R.A.; Thompson, S.A.; Afifi, A.K.; Saadeh, F.A. Compendium of Human Anatomic Variation; Urban & Schwarzenberg: Baltimore, MD, USA; Munich, Germany, 1988; pp. 27–28. [Google Scholar]
- Aparisi Gómez, M.P.; Aparisi, F.; Bartoloni, A.; Ferrando Fons, M.A.; Battista, G.; Guglielmi, G.; Bazzocchi, A. Anatomical variation in the ankle and foot: From incidental finding to inductor of pathology. Part II: Midfooot and forefoot. Insights Imaging 2019, 10, 69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bernhard, A.; Miller, J.; Keeler, J.; Siesel, K.; Bridges, E. Absence of the Fourth Tendon of the Flexor Digitorum Brevis Muscle: A Cadaveric Study. Foot Ankle Spec. 2013, 6, 286–289. [Google Scholar] [CrossRef] [PubMed]
- Ferreira Arquez, H. An Anatomical Study of The Musculus Flexor Digitorum Brevis. Int. Arch. Med. 2017, 10, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Vega, J.; Redó, D.; Savín, G.; Malagelada, F.; Dalmau-Pastor, M. Anatomical variations of flexor hallucis longus tendon increase safety in hindfoot endoscopy. Knee Surg. Sports Traumatol. Arthrosc. 2017, 25, 1929–1935. [Google Scholar] [CrossRef] [PubMed]
- Ilayperuma, I. On the variations of the muscle flexor digitorum brevis: Anatomical insight. Int. J. Morphol. 2012, 30, 337–340. [Google Scholar] [CrossRef] [Green Version]
- Rosse, C.; Gaddum-Rosse, P. Hollinshead’s Textbook from Anatomy, 6th ed.; Lippincott–Raven: Philadelphia, PA, USA, 1997. [Google Scholar]
- Agarwal, R.; Khajuria, S.; Saini, H. Study of Absence of 4th Tendon of Flexor Digitorum Brevis Muscle. Int. J. Anat. Res. 2017, 5, 47–50. [Google Scholar] [CrossRef] [Green Version]
- Nathan, H.; Gloobe, H. Flexor digitorum brevis--anatomical variations. Anat. Anzeiger. 1974, 135, 295–301. [Google Scholar]
- Yalçın, B.; Ozan, H. Some variations of the musculus flexor digitorum brevis. Anat. Sci. Int. 2005, 80, 189–192. [Google Scholar] [CrossRef]
- Lobo, S.W.; Menezes, R.G.; Mamata, S.; Baral, P.; Hunnargi, S.A.; Kanchan, T.; Bhat, N.B. Phylogenetic variation in flexor digitorum brevis: A Nepalese cadaveric study. Nepal Med. Coll. J. 2008, 10, 230–232. [Google Scholar] [PubMed]
- Becerro de Bengoa Vallejo, R.; Viejo Tirado, F.; Prados Frutos, J.C.; Losa Iglesias, M.E.; Jules, K.T. Transfer of the flexor digitorum brevis tendon. J. Am. Podiatr. Med. Assoc. 2008, 98, 27–35. [Google Scholar] [CrossRef] [PubMed]
- Claassen, H.; Wree, A. Isolated flexor muscles of the little toe in the feet of an individual with atrophied or lacking 4th head of the M. extensor digitorum brevis and lacking the 4th tendon of the M. extensor digitorum longus. Ann. Anat. 2003, 185, 81–84. [Google Scholar] [CrossRef] [PubMed]
- Putti, A.B.; Arnold, G.P.; Abboud, R.J. Foot pressure differences in men and women. Foot Ankle Surg. 2010, 16, 21–24. [Google Scholar] [CrossRef] [PubMed]
- Silva, A.M.; Shen, W.; Heo, M.; Gallagher, D.; Wang, Z.; Sardinha, L.B.; Heymsfield, S.B. Ethnicity-related skeletal muscle differences across the lifespan. Am. J. Hum. Biol. 2010, 22, 76–82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaney, D.M.; Lee, M.S.; Khan, M.A.; Krueger, W.A.; Mandracchia, V.J.; Yoho, R.M. Study of ten anatomical variants of the foot and ankle. J. Amer. Podiatr. Med. Assoc. 1996, 86, 532–537. [Google Scholar] [CrossRef] [PubMed]
- McNutt, E.J.; Zipfel, B.; DeSilva, J.M. The evolution of the human foot. Evol. Anthropol. 2018, 27, 197–217. [Google Scholar] [CrossRef] [PubMed]
- Grogono, B.J.S.; Jowsey, J. Flexor Accessorius Longus an Unusual Muscle Anomaly. J. Bone Jt. Surg. 1965, 47, 118–119. [Google Scholar] [CrossRef]
- Farris, D.J.; Kelly, L.A.; Cresswell, A.G.; Lichtwark, G.A. The functional importance of human foot muscles for bipedal locomotion. Proc. Natl. Acad. Sci. USA 2019, 116, 1645–1650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hartrampf, C.R.; Scheflan, M.; Bowstwick, J. The flexor digitorum brevis muscle Island pedicle flap: A new in dimension heel reconstruction. Plast. Reconstr. Surg. 1980, 66, 264–270. [Google Scholar] [CrossRef]
- Stimec, B.V.; Dash, J.; Assal, M.; Stern, R.; Fasel, J.H.D. Additional muscular slip of the flexor digitorum longus muscle to the fifth toe. Surg. Radiol. Anat. 2018, 40, 533–535. [Google Scholar] [CrossRef]
- Tarpey, M.D.; Amorese, A.J.; Balestrieri, N.P.; Ryan, T.E.; Schmidt, C.A.; McClung, J.M.; Spangenburg, E.E. Characterization and utilization of the flexor digitorum brevis for assessing skeletal muscle function. Skelet. Muscle 2018, 8, 14. [Google Scholar] [CrossRef]
- Powers Scott, K.; Smuder Ashley, J.; Judge Andrew, R. Oxidative stress and disuse muscle atrophy. Curr. Opin. Clin. Nutr. Metab. Care 2012, 15, 240–245. [Google Scholar] [CrossRef] [PubMed]
- Malavaki, C.J.; Sakkas, G.K.; Mitrou, G.I.; Kalyva, A.; Stefanidis, I.; Myburgh, K.H.; Karatzaferi, C. Skeletal muscle atrophy: Disease-induced mechanisms may mask disuse atrophy. J. Muscle Res. Cell Motil. 2015, 36, 405–421. [Google Scholar] [CrossRef] [PubMed]
- Clark, B.C. In vivo alterations in skeletal muscle form and function after disuse atrophy. Med. Sci. Sport. Exerc. 2009, 41, 1869–1875. [Google Scholar] [CrossRef] [PubMed]
- Thangarajan, R.; Bakthavatchalam, P.; Potu, B.; Huban, T. Anatomical variation of the flexor digitorum brevis muscle revisited: A case report from South Indian population. Int. J. Anat. Var. 2010, 3, 1000–1002. [Google Scholar]
- Kaissar, Y. The Fourth Slip of the Flexor Digitorum Brevis Muscle of the Human Foot: A Systematic Review and Meta-Analysis. Anat. Appl. 2015, 120, 59–70. [Google Scholar]
- Malhotra, K.; Davda, K.; Singh, D. The pathology and management of lesser toe deformities. EFORT Open Rev. 2017, 1, 409–419. [Google Scholar] [CrossRef] [PubMed]
- Gonçalves, H.; Kajetanek, C.; Graff, W.; Thiongo, M.; Laporte, C. Flexor digitorum brevis tendon transfer to the flexor digitorum longus tendon according to Valtin in posttraumatic flexible claw toe deformity due to extrinsic toe flexor shortening. Orthop. Traumatol. Surg. Res. 2015, 101, 257–260. [Google Scholar] [CrossRef] [Green Version]
- García-González, A.; Bayod, J.; Prados-Frutos, J.C.; Losa-Iglesias, M.; Jules, K.T.; Becerro de Bengoa-Vallejo, R.; Doblaré, M. Finite-element simulation of flexor digitorum longus or flexor digitorum brevis tendon transfer for the treatment of claw toe deformity. J. Biomech. 2009, 42, 1697–1704. [Google Scholar] [CrossRef]
- Deldar, R.; Merle, C.; Attinger, C.E.; Evans, K.K. Soft tissue coverage of lower extremity defects: Pearls and pitfalls in the chronic wound population. Plast. Aesthet. Res. 2022, 9, 13. [Google Scholar] [CrossRef]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Quiñones-Rodriguez, J.I.; Mantilla-Rosa, C.; Rodríguez, F.; Villamil, C.I.; Fernández, J.; González-Solá, M.; Torres-Toro, C.; Rosario, M.G. A Missing Flexor Digitorum Brevis Tendon and Its Relationship to Sex and Ancestry: Evaluation in Hispanic Population. Anatomia 2022, 1, 210-216. https://doi.org/10.3390/anatomia1020021
Quiñones-Rodriguez JI, Mantilla-Rosa C, Rodríguez F, Villamil CI, Fernández J, González-Solá M, Torres-Toro C, Rosario MG. A Missing Flexor Digitorum Brevis Tendon and Its Relationship to Sex and Ancestry: Evaluation in Hispanic Population. Anatomia. 2022; 1(2):210-216. https://doi.org/10.3390/anatomia1020021
Chicago/Turabian StyleQuiñones-Rodriguez, Jailenne I., Cristian Mantilla-Rosa, Félix Rodríguez, Catalina I. Villamil, Juan Fernández, Maryvi González-Solá, Cristhian Torres-Toro, and Martin G. Rosario. 2022. "A Missing Flexor Digitorum Brevis Tendon and Its Relationship to Sex and Ancestry: Evaluation in Hispanic Population" Anatomia 1, no. 2: 210-216. https://doi.org/10.3390/anatomia1020021