
A Review of the Important Weapons against Antimicrobial Resistance in Sub-Saharan Africa
 , , , and
, , , and 
{kind=link}
{kind=link}
Abstract
:1. Introduction
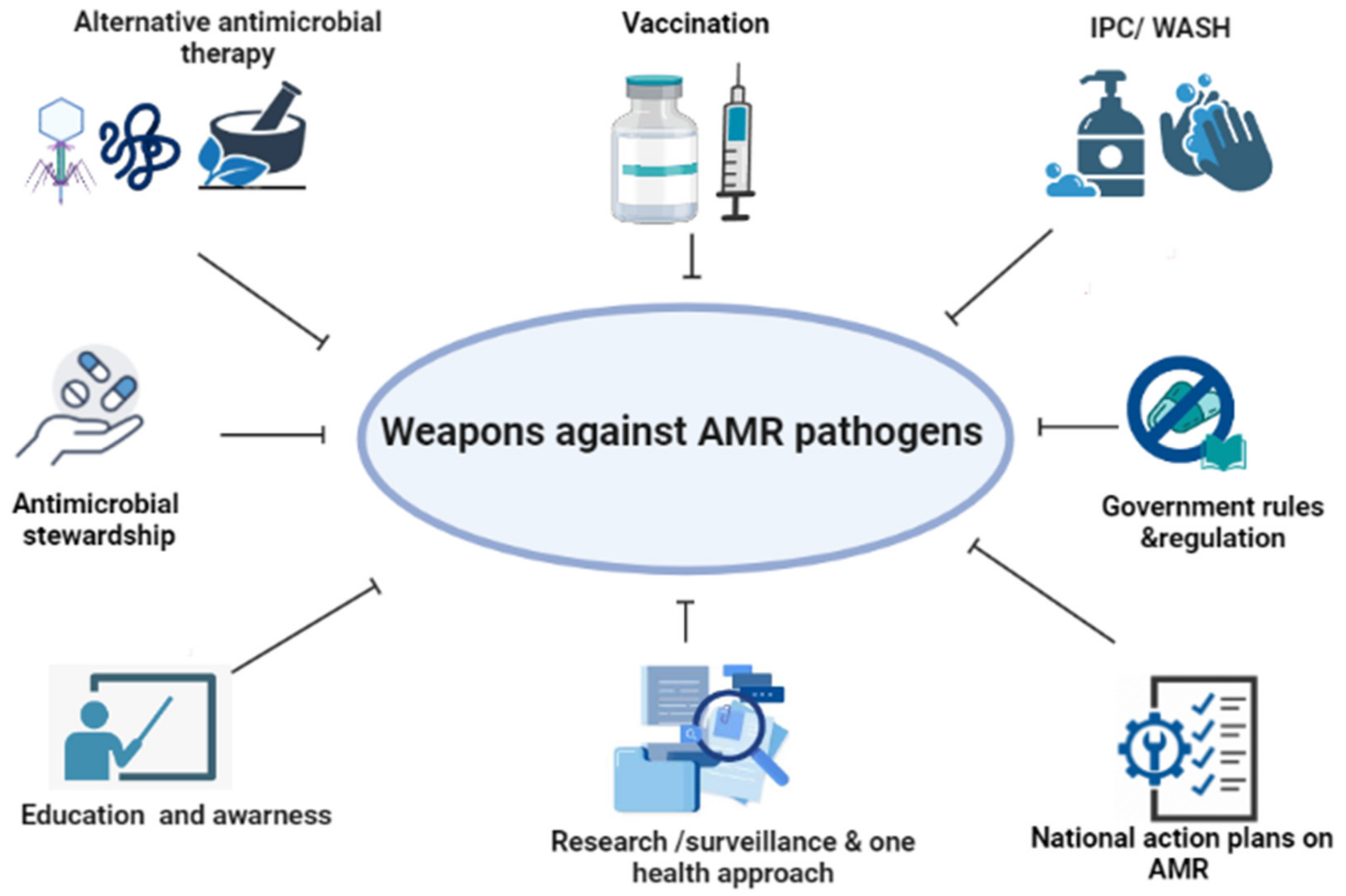
2. Important Weapons against AMR
2.1. Vaccines
2.2. Education and Awareness
- Training healthcare professionals
- Public awareness/engagement
2.3. Infection Prevention and Control by Improving WASH
2.4. Natural Products
2.4.1. Phytochemical Compounds
2.4.2. Antimicrobial Peptides (AMPs)
2.4.3. Bacteriophage Therapy
2.4.4. Carbon-Based Nanomaterials
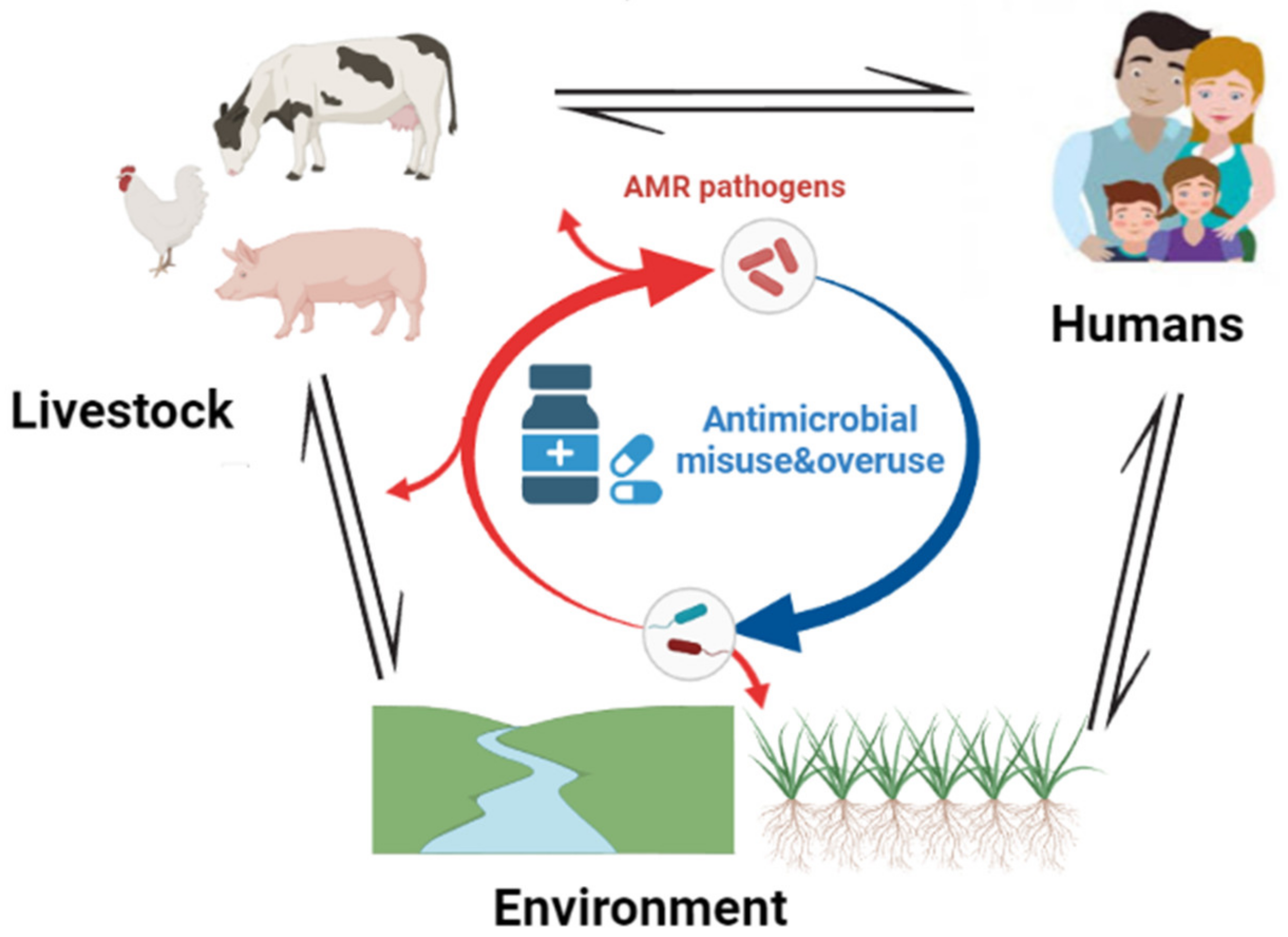
2.5. One Health Approach
2.6. AMR Surveillance Program
2.7. Antimicrobial Stewardship Programs
2.8. Functional National Action Plans (NAPs) on AMR
2.9. Political Will/Governance/Regulations
3. Advanced Techniques in Deciphering AMR
3.1. Metagenomics
3.2. Whole-Genome Sequencing (WGS)
3.3. AMR Prediction Using AI Based on Genomics Data
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Aminov, R. History of antimicrobial drug discovery: Major classes and health impact. Biochem. Pharmacol. 2017, 133, 4–19. [Google Scholar] [CrossRef]
- Cook, M.A.; Wright, G.D. The past, present, and future of antibiotics. Sci. Transl. Med. 2022, 14, eabo7793. [Google Scholar] [CrossRef] [PubMed]
- Hall, T.J.; Villapún, V.M.; Addison, O.; Webber, M.A.; Lowther, M.; Louth, S.E.T.; Mountcastle, S.E.; Brunet, M.Y.; Cox, S.C. A call for action to the biomaterial community to tackle antimicrobial resistance. Biomater. Sci. 2020, 8, 4951–4974. [Google Scholar] [CrossRef] [PubMed]
- Kimera, Z.I.; Frumence, G.; Mboera, L.E.G.; Rweyemamu, M.; Mshana, S.E.; Matee, M.I.N. Assessment of Drivers of Antimicrobial Use and Resistance in Poultry and Domestic Pig Farming in the Msimbazi River Basin in Tanzania. Antibiotics 2020, 9, 838. [Google Scholar] [CrossRef] [PubMed]
- Saeed, S.I.; Mergani, A.; Aklilu, E.; Kamaruzzaman, N.F. Antimicrobial Peptides: Bringing Solution to the Rising Threats of Antimicrobial Resistance in Livestock. Front. Veter. Sci. 2022, 9, 851052. Available online: https://www.frontiersin.org/article/10.3389/fvets.2022.851052 (accessed on 29 May 2022).
- Pariente, N.; PLoS Biology Staff Editors. The antimicrobial resistance crisis needs action now. PLoS Biol. 2022, 20, e3001918. [Google Scholar] [CrossRef]
- Gow, N.A.; Johnson, C.; Berman, J.; Coste, A.T.; Cuomo, C.A.; Perlin, D.S.; Bicanic, T.; Harrison, T.S.; Wiederhold, N.; Bromley, M.; et al. The importance of antimicrobial resistance in medical mycology. Nat. Commun. 2022, 13, 5352. [Google Scholar] [CrossRef]
- Arastehfar, A.; Gabaldón, T.; Garcia-Rubio, R.; Jenks, J.; Hoenigl, M.; Salzer, H.; Ilkit, M.; Lass-Flörl, C.; Perlin, D. Drug-Resistant Fungi: An Emerging Challenge Threatening Our Limited Antifungal Armamentarium. Antibiotics 2020, 9, 877. [Google Scholar] [CrossRef] [PubMed]
- WHO. World Health Organization.WHO Fungal Priority Pathogens List Toguide Research, Development and Public Health Action. 2022. Available online: https://www.who.int/publications/i/item/9789240060241 (accessed on 20 December 2022).
- Muhaj, F.F.; George, S.J.; Nguyen, C.D.; Tyring, S.K. Antimicrobials and resistance part II: Antifungals, antivirals, and antiparasitics. J. Am. Acad. Dermatol. 2022, 86, 1207–1226. [Google Scholar] [CrossRef]
- Musengimana, G.; Tuyishime, E.; Kiromera, A.; Malamba, S.S.; Mulindabigwi, A.; Habimana, M.R.; Baribwira, C.; Ribakare, M.; Habimana, S.D.; DeVos, J.; et al. Acquired HIV drug resistance among adults living with HIV receiving first-line antiretroviral therapy in Rwanda: A cross-sectional nationally representative survey. Antivir. Ther. 2022, 27, 13596535221102690. [Google Scholar] [CrossRef]
- Nisabwe, L.; Brice, H.; Umuhire, M.C.; Gwira, O.; Harelimana, J.D.D.; Nzeyimana, Z.; Sebatunzi, O.R.; Rusingiza, E.K.; Hahirwa, I.; Muvunyi, C.M. Knowledge and attitudes towards antibiotic use and resistance among undergraduate healthcare students at University of Rwanda. J. Pharm. Policy Pract. 2020, 13, 7. [Google Scholar] [CrossRef]
- Laxminarayan, R. The overlooked pandemic of antimicrobial resistance. Lancet 2022, 399, 606–607. [Google Scholar] [CrossRef]
- Murray, C.J.; Ikuta, K.S.; Sharara, F.; Swetschinski, L.; Aguilar, G.R.; Gray, A.; Han, C.; Bisignano, C.; Rao, P.; Wool, E.; et al. Global burden of bacterial antimicrobial resistance in 2019: A systematic analysis. Lancet 2022, 399, 629–655. [Google Scholar] [CrossRef]
- Gahamanyi, N.; Mboera, L.E.G.; Matee, M.I.; Mutangana, D.; Komba, E.V.G. Prevalence, Risk Factors, and Antimicrobial Resistance Profiles of Thermophilic Campylobacter Species in Humans and Animals in Sub-Saharan Africa: A Systematic Review. Int. J. Microbiol. 2020, 2020, 2092478. Available online: https://www.hindawi.com/journals/ijmicro/2020/2092478/ (accessed on 23 November 2020). [CrossRef] [PubMed] [Green Version]
- Anthony, W.E.; Burnham, C.-A.D.; Dantas, G.; Kwon, J.H. The Gut Microbiome as a Reservoir for Antimicrobial Resistance. J. Infect. Dis. 2021, 223 (Suppl. 3), S209–S213. [Google Scholar] [CrossRef] [PubMed]
- Patangia, D.V.; Ryan, C.A.; Dempsey, E.; Ross, R.P.; Stanton, C. Impact of antibiotics on the human microbiome and consequences for host health. Microbiologyopen 2022, 11, e1260. [Google Scholar] [CrossRef] [PubMed]
- Rosini, R.; Nicchi, S.; Pizza, M.; Rappuoli, R. Vaccines against Antimicrobial Resistance. Front. Immunol. 2020, 11, 1048. Available online: https://www.frontiersin.org/article/10.3389/fimmu.2020.01048 (accessed on 19 June 2022). [CrossRef] [PubMed]
- Kashoma, I.P.; Kassem, I.I.; John, J.; Kessy, B.M.; Gebreyes, W.; Kazwala, R.R.; Rajashekara, G. Prevalence and Antimicrobial Resistance ofCampylobacterIsolated from Dressed Beef Carcasses and Raw Milk in Tanzania. Microb. Drug Resist. 2016, 22, 40–52. [Google Scholar] [CrossRef] [Green Version]
- Blake, K.L.; O’Neill, A.J. Transposon library screening for identification of genetic loci participating in intrinsic susceptibility and acquired resistance to antistaphylococcal agents. J. Antimicrob. Chemother. 2013, 68, 12–16. [Google Scholar] [CrossRef] [Green Version]
- Blair, J.M.A.; Webber, M.A.; Baylay, A.J.; Ogbolu, D.O.; Piddock, L.J.V. Molecular mechanisms of antibiotic resistance. Nat. Rev. Microbiol. 2015, 13, 42–51. [Google Scholar] [CrossRef]
- Wright, G.D. Molecular mechanisms of antibiotic resistance. Chem. Commun. 2011, 47, 4055–4061. [Google Scholar] [CrossRef]
- Jassim, S.A.A.; Limoges, R.G. Bacteriophage and Antimicrobial Resistance In Bacteriophages: Practical Applications for Nature’s Biocontrol; Jassim, S.A.A., Limoges, R.G., Eds.; Springer International Publishing: Cham, Switzerland, 2017; pp. 19–57. [Google Scholar] [CrossRef]
- Bisi-Johnson, M.A.; Obi, C.L.; Samuel, B.B.; Eloff, J.N.; Okoh, A.I. Antibacterial activity of crude extracts of some South African medicinal plants against multidrug resistant etiological agents of diarrhoea. BMC Complement. Altern. Med. 2017, 17, 321. [Google Scholar] [CrossRef]
- Bloom, D.E.; Black, S.; Salisbury, D.; Rappuoli, R. Antimicrobial resistance and the role of vaccines. Proc. Natl. Acad. Sci. USA 2018, 115, 12868–12871. [Google Scholar] [CrossRef] [Green Version]
- Amewu, R.K.; Amoateng, P.; Arthur, P.K.; Asare, P.; Asiamah, I.; Boamah, D.; Otchere, I.D.; Amengor, C.D.; Ekuadzi, E.; Chibale, K.; et al. Drug discovery research in Ghana, challenges, current efforts, and the way forward. PLoS Neglected Trop. Dis. 2022, 16, e0010645. [Google Scholar] [CrossRef]
- Jansen, K.U.; Knirsch, C.; Anderson, A.S. The role of vaccines in preventing bacterial antimicrobial resistance. Nat. Med. 2018, 24, 10–19. [Google Scholar] [CrossRef]
- Rukambile, E.; Sintchenko, V.; Muscatello, G.; Wang, Q.; Kiiru, J.; Maulaga, W.; Magidanga, B.; Banda, G.; Kock, R.; Alders, R. Campylobacter and Salmonella in Scavenging Indigenous Chickens in Rural Central Tanzania: Prevalence, Antimicrobial Resistance, and Genomic Features. Microbiol. Res. 2021, 12, 440–454. [Google Scholar] [CrossRef]
- Tadesse, B.T.; Ashley, E.A.; Ongarello, S.; Havumaki, J.; Wijegoonewardena, M.; González, I.J.; Dittrich, S. Antimicrobial resistance in Africa: A systematic review. BMC Infect. Dis. 2017, 17, 616. [Google Scholar] [CrossRef] [Green Version]
- Tompkins, K.; Juliano, J.J.; van Duin, D. Antimicrobial Resistance in Enterobacterales and Its Contribution to Sepsis in Sub-saharan Africa. Front. Med. 2021, 8, 615649. Available online: https://www.frontiersin.org/articles/10.3389/fmed.2021.615649 (accessed on 14 August 2022). [CrossRef] [PubMed]
- Elton, L.; Thomason, M.J.; Tembo, J.; Velavan, T.P.; Pallerla, S.R.; Arruda, L.B.; Vairo, F.; Montaldo, C.; Ntoumi, F.; Hamid, M.M.A.; et al. Antimicrobial resistance preparedness in sub-Saharan African countries. Antimicrob. Resist. Infect. Control. 2020, 9, 145. [Google Scholar] [CrossRef] [PubMed]
- Africa, C.D.C. Multi-Country Research on Antimicrobial Resistance in Africa Reveals Only Five of 15 Antibiotic-Resistant Pathogens Designated by the WHO as Priority Pathogens Are Consistently Tested. Available online: https://aslm.org/press-release/multi-country-research-on-antimicrobial-resistance-in-africa-reveals-only-five-of-15-antibiotic-resistant-pathogens-designated-by-the-who-as-priority-pathogens-are-consistently-tested/ (accessed on 22 November 2022).
- Gyawali, R.; Ibrahim, S.A. Natural products as antimicrobial agents. Food Control. 2014, 46, 412–429. [Google Scholar] [CrossRef]
- Možina, S.S.; Klančnik, A.; Kovac, J.; Jeršek, B.; Bucar, F. Antimicrobial natural products against Campylobacter. In Natural Antimicrobial Agents; Mérillon, J.-M., Riviere, C., Eds.; Springer International Publishing: Cham, Switzerland, 2018; pp. 3–30. [Google Scholar] [CrossRef]
- Gahamanyi, N.; Munyaneza, E.; Dukuzimana, E.; Tuyiringire, N.; Pan, C.-H.; Komba, E.V.G. Ethnobotany, Ethnopharmacology, and Phytochemistry of Medicinal Plants Used for Treating Human Diarrheal Cases in Rwanda: A Review. Antibiotics 2021, 10, 1231. [Google Scholar] [CrossRef] [PubMed]
- Sasirekha, B.; Gahamanyi, N. Photosensitizers: An Effective Alternative Approach to Microbial Pathogen in Frontiers in Clinical Drug Research (Anti Infectives); Bentham Science Publishers B.V: Sharjah, United Arab Emirates, 2017; Volume 3, pp. 187–205. [Google Scholar]
- Kakasis, A.; Panitsa, G. Bacteriophage therapy as an alternative treatment for human infections. A comprehensive review. Int. J. Antimicrob. Agents 2019, 53, 16–21. [Google Scholar] [CrossRef] [PubMed]
- Amaratunga, K.; Communicable and Infectious Disease Steering Committee (CIDSC); Tarasuk, J.; Tsegaye, L.; Archibald, C. Antimicrobial Resistance (AMR) Surveillance Task Group Advancing surveillance of antimicrobial resistance: Summary of the 2015 CIDSC Report. Can. Commun. Dis. Rep. 2016, 42, 232–237. [Google Scholar] [CrossRef]
- White, A.; Hughes, J.M. Critical Importance of a One Health Approach to Antimicrobial Resistance. EcoHealth 2019, 16, 404–409. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wuijts, S.; Berg, H.H.J.L.V.D.; Miller, J.; Abebe, L.; Sobsey, M.; Andremont, A.; Medlicott, K.O.; Van Passel, M.W.J.; Husman, A.M.D.R. Towards a research agenda for water, sanitation and antimicrobial resistance. J. Water Health 2017, 15, 175–184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Autran, B.; Carcelain, G.; Combadiere, B.; Debre, P. Therapeutic Vaccines for Chronic Infections. Science 2004, 305, 205–208. [Google Scholar] [CrossRef] [PubMed]
- Riedel, S. Edward Jenner and the History of Smallpox and Vaccination. Bayl. Univ. Med. Cent. Proc. 2005, 18, 21–25. [Google Scholar] [CrossRef]
- Iwasaki, A.; Omer, S.B. Why and How Vaccines Work. Cell 2020, 183, 290–295. [Google Scholar] [CrossRef]
- Micoli, F.; Bagnoli, F.; Rappuoli, R.; Serruto, D. The role of vaccines in combatting antimicrobial resistance. Nat. Rev. Microbiol. 2021, 19, 287–302. [Google Scholar] [CrossRef]
- Lipsitch, M.; Siber, G.R. How Can Vaccines Contribute to Solving the Antimicrobial Resistance Problem? Mbio 2016, 7, e00428-16. [Google Scholar] [CrossRef] [Green Version]
- Bloom; Curtis, N. D.E. The Value of Vaccination In Hot Topics in Infection and Immunity in Children VII; Curtis, N., Finn, A., Pollard, A.J., Eds.; Springer: New York, NY, USA, 2011; pp. 1–8. [Google Scholar] [CrossRef]
- Rodrigues, C.; Plotkin, S.A. Impact of Vaccines; Health, Economic and Social Perspectives. Front. Microbiol. 2020, 11, 1526. [Google Scholar] [CrossRef]
- Alghamdi, S. The role of vaccines in combating antimicrobial resistance (AMR) bacteria. Saudi J. Biol. Sci. 2021, 28, 7505–7510. [Google Scholar] [CrossRef] [PubMed]
- WHO. Bacterial Vaccines in Clinical and Preclinical Development. 2021. Available online: https://www.who.int/publications-detail-redirect/9789240052451 (accessed on 15 July 2022).
- Musa, B.M.; Adamu, A.L.; Galadanci, N.A.; Zubayr, B.; Odoh, C.N.; Aliyu, M.H. Trends in prevalence of multi drug resistant tuberculosis in sub-Saharan Africa: A systematic review and meta-analysis. PLoS ONE 2017, 12, e0185105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hlashwayo, D.F.; Sigaúque, B.; Bila, C.G. Epidemiology and antimicrobial resistance of Campylobacter spp. in animals in Sub-Saharan Africa: A systematic review. Heliyon 2020, 6, e03537. [Google Scholar] [CrossRef] [PubMed]
- Ismail, S.; Shahid, F.; Khan, A.; Bhatti, S.; Ahmad, S.; Naz, A.; Almatroudi, A.; Qamar, M.T.U. Pan-vaccinomics approach towards a universal vaccine candidate against WHO priority pathogens to address growing global antibiotic resistance. Comput. Biol. Med. 2021, 136, 104705. [Google Scholar] [CrossRef]
- Madhi, S.A.; Rees, H. Special focus on challenges and opportunities for the development and use of vaccines in Africa. Hum. Vaccines Immunother. 2018, 14, 2335–2339. [Google Scholar] [CrossRef] [Green Version]
- Amponsah-Dacosta, E.; Muloiwa, R.; Wiysonge, C.S.; Gold, M.; Hussey, G.; Kagina, B.M. Developing vaccinology expertise for Africa: Fifteen years and counting. Pan Afr. Med. J. 2021, 38, 313. [Google Scholar] [CrossRef]
- Stoop, N.; Hirvonen, K.; Maystadt, J.-F. Institutional mistrust and child vaccination coverage in Africa. BMJ Glob. Health 2021, 6, e004595. [Google Scholar] [CrossRef]
- Janusz, C.B.; Frye, M.; Mutua, M.K.; Wagner, A.L.; Banerjee, M.; Boulton, M.L. Vaccine Delay and Its Association With Undervaccination in Children in Sub-Saharan Africa. Am. J. Prev. Med. 2021, 60 (Suppl. 1), S53–S64. [Google Scholar] [CrossRef]
- Bobo, F.T.; Asante, A.; Woldie, M.; Dawson, A.; Hayen, A. Child vaccination in sub-Saharan Africa: Increasing coverage addresses inequalities. Vaccine 2022, 40, 141–150. [Google Scholar] [CrossRef]
- Saied, A.A.; Metwally, A.A.; Dhawan, M.; Choudhary, O.P.; Aiash, H. Strengthening vaccines and medicines manufacturing capabilities in Africa: Challenges and perspectives. EMBO Mol. Med. 2022, 14, e16287. [Google Scholar] [CrossRef]
- Haenssgen, M.J.; Xayavong, T.; Charoenboon, N.; Warapikuptanun, P.; Zaw, Y.K. The Consequences of AMR Education and Awareness Raising: Outputs, Outcomes, and Behavioural Impacts of an Antibiotic-Related Educational Activity in Lao PDR. Antibiotics 2018, 7, 95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ajuebor, O.; Shetty, N.; Mah, K.; Cometto, G. Health workers’ education and training to prevent antimicrobial resistance. Bull. World Health Organ. 2019, 97, 791. [Google Scholar] [CrossRef] [PubMed]
- Nand, P.; Wilson, M.; Cohen, S.H.; Brown, J. Curbing antimicrobial resistance: Do physicians receive adequate education about antibiograms? J. Infect. 2016, 72, 127–129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lubwama, M.; Onyuka, J.; Ayazika, K.T.; Ssetaba, L.J.; Siboko, J.; Daniel, O.; Mushi, M.F. Knowledge, attitudes, and perceptions about antibiotic use and antimicrobial resistance among final year undergraduate medical and pharmacy students at three universities in East Africa. PLoS ONE 2021, 16, e0251301. [Google Scholar] [CrossRef]
- Majumder, A.A.; Singh, K.; Hilaire, M.G.-S.; Rahman, S.; Sa, B.; Haque, M. Tackling Antimicrobial Resistance by promoting Antimicrobial stewardship in Medical and Allied Health Professional Curricula. Expert Rev. Anti-infective Ther. 2020, 18, 1245–1258. [Google Scholar] [CrossRef]
- Pezzani, M.D.; Tornimbene, B.; Pessoa-Silva, C.; de Kraker, M.; Rizzardo, S.; Salerno, N.D.; Harbarth, S.; Tacconelli, E. Methodological quality of studies evaluating the burden of drug-resistant infections in humans due to the WHO Global Antimicrobial Resistance Surveillance System target bacteria. Clin. Microbiol. Infect. 2021, 27, 687–696. [Google Scholar] [CrossRef]
- Catalán-Matamoros, D.; Pariente, A.; Elías-Pérez, C. What we know about media communication on antibiotics and antimicrobial resistance: A systematic review of the scientific literature. Patient Educ. Couns. 2019, 102, 1427–1438. [Google Scholar] [CrossRef]
- Venant, E.; Stanley, B.K.; Mosha, M.J.; Msovela, K.E.; Mushi, D.J.; Masanja, P.; Wiedenmayer, K.; Ombaka, E. P23 Assessment of knowledge, attitude and practice towards antimicrobial use and resistance among students in three secondary schools in Dodoma City. JAC-Antimicrobial Resist. 2022, 4 (Suppl. 1), dlac004.022. [Google Scholar] [CrossRef]
- Mitchell, J.; Cooke, P.; Ahorlu, C.; Arjyal, A.; Baral, S.; Carter, L.; Dasgupta, R.; Fieroze, F.; Fonseca-Braga, M.; Huque, R.; et al. Community engagement: The key to tackling Antimicrobial Resistance (AMR) across a One Health context? Glob. Public Health 2021, 17, 2647–2664. [Google Scholar] [CrossRef]
- Willis, L.D.; Chandler, C. Quick fix for care, productivity, hygiene and inequality: Reframing the entrenched problem of antibiotic overuse. BMJ Glob. Health 2019, 4, e001590. [Google Scholar] [CrossRef]
- Godman, B.; Egwuenu, A.; Wesangula, E.; Schellack, N.; Kalungia, A.C.; Tiroyakgosi, C.; Kgatlwane, J.; Mwita, J.C.; Patrick, O.; Niba, L.L.; et al. Tackling Antimicrobial Resistance across Sub-Saharan Africa: Current Challenges and Implications for the Future. Expert Opin. Drug Saf. 2022, 21, 1089–1111. [Google Scholar] [CrossRef]
- Michaelidou, M.; Karageorgos, S.; Tsioutis, C. Antibiotic Use and Antibiotic Resistance: Public Awareness Survey in the Republic of Cyprus. Antibiotics 2020, 9, 759. [Google Scholar] [CrossRef] [PubMed]
- Pinder, R.J.; Berry, D.; Sallis, A.; Chadborn, T. Antibiotic Prescribing and Behaviour Change in Healthcare Settings: Literature Review and Behavioural Analysis. In Department of Health & Public Health England, Report, Feb. 2015; Department of Health & Public Health England: London, UK. [CrossRef]
- Ayukekbong, J.A.; Ntemgwa, M.; Atabe, A.N. The threat of antimicrobial resistance in developing countries: Causes and control strategies. Antimicrob. Resist. Infect. Control. 2017, 6, 47. [Google Scholar] [CrossRef] [PubMed]
- World Bank. Drug-Resistant Infections: A Threat to Our Economic Future. Available online: https://documents.worldbank.org/en/publication/documents-reports/documentdetail/323311493396993758/final-report (accessed on 9 October 2022).
- Williams, M.R.; Stedtfeld, R.D.; Guo, X.; Hashsham, S.A. Antimicrobial Resistance in the Environment. Water Environ. Res. 2016, 88, 1951–1967. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. Progress on WASH in Health Care Facilities 2000–2021: Special Focus on WASH and Infection Prevention and Control (IPC). Available online: https://www.who.int/publications-detail-redirect/progress-on-wash-in-health-care-facilities-2000-2021--special-focus-on-wash-and-infection-prevention-and-control-(ipc) (accessed on 1 March 2023).
- Sano, D.; Wester, A.L.; Schmitt, H.; Amarasiri, M.; Kirby, A.; Medlicott, K.; Husman, A.M.D.R. Updated research agenda for water, sanitation and antimicrobial resistance. J. Water Health 2020, 18, 858–866. [Google Scholar] [CrossRef]
- Bain, R.; Johnston, R.; Mitis, F.; Chatterley, C.; Slaymaker, T. Establishing Sustainable Development Goal Baselines for Household Drinking Water, Sanitation and Hygiene Services. Water 2018, 10, 1711. [Google Scholar] [CrossRef] [Green Version]
- Ikhimiukor, O.O.; Odih, E.E.; Donado-Godoy, P.; Okeke, I.N. A bottom-up view of antimicrobial resistance transmission in developing countries. Nat. Microbiol. 2022, 7, 757–765. [Google Scholar] [CrossRef]
- WHO. Technical Brief on Water, Sanitation, Hygiene and Wastewater Management to Prevent Infections and Reduce the Spread of Antimicrobial Resistance. Available online: https://www.who.int/publications/i/item/9789240006416 (accessed on 20 October 2022).
- Prendergast, A.J.; Gharpure, R.; Mor, S.; Viney, M.; Dube, K.; Lello, J.; Berger, C.; Siwila, J.; Joyeux, M.; Hodobo, T.; et al. Putting the “A” into WaSH: A call for integrated management of water, animals, sanitation, and hygiene. Lancet Planet. Heal. 2019, 3, e336–e337. [Google Scholar] [CrossRef] [Green Version]
- Kraemer, S.A.; Ramachandran, A.; Perron, G.G. Antibiotic Pollution in the Environment: From Microbial Ecology to Public Policy. Microorganisms 2019, 7, 180. [Google Scholar] [CrossRef] [Green Version]
- Essack, S. Water, sanitation and hygiene in national action plans for antimicrobial resistance. Bull. World Health Organ. 2021, 99, 606–608. [Google Scholar] [CrossRef]
- Ramay, B.M.; Caudell, M.A.; Cordón-Rosales, C.; Archila, L.D.; Palmer, G.H.; Jarquin, C.; Moreno, P.; McCracken, J.P.; Rosenkrantz, L.; Amram, O.; et al. Antibiotic use and hygiene interact to influence the distribution of antimicrobial-resistant bacteria in low-income communities in Guatemala. Sci. Rep. 2020, 10, 13767. [Google Scholar] [CrossRef]
- WHO; UNICEF. Half of Health Care Facilities Globally Lack Basic Hygiene Services—WHO, UNICEF. Available online: https://www.who.int/news/item/30-08-2022-half-of-health-care-facilities-globally-lack-basic-hygiene-services---who--unicef (accessed on 12 September 2022).
- Chandra, H.; Bishnoi, P.; Yadav, A.; Patni, B.; Mishra, A.P.; Nautiyal, A.R. Antimicrobial Resistance and the Alternative Resources with Special Emphasis on Plant-Based Antimicrobials—A Review. Plants 2017, 6, 16. [Google Scholar] [CrossRef]
- Borges, A.; Abreu, A.C.; Dias, C.; Saavedra, M.J.; Borges, F.; Simões, M. New Perspectives on the Use of Phytochemicals as an Emergent Strategy to Control Bacterial Infections Including Biofilms. Molecules 2016, 21, 877. [Google Scholar] [CrossRef]
- Bartlett, J.G.; Gilbert, D.N.; Spellberg, B. Seven Ways to Preserve the Miracle of Antibiotics. Clin. Infect. Dis. 2018, 56, 1445–1450. [Google Scholar] [CrossRef] [PubMed]
- Rawat, P.; Singh, P.K.; Kumar, V. Evidence based traditional anti-diarrheal medicinal plants and their phytocompounds. Biomed. Pharmacother. 2017, 96, 1453–1464. [Google Scholar] [CrossRef] [PubMed]
- Abdulhafiz, F.; Ibrahim, S.; Reduan, M.F.H.; Hamzah, Z.; Reddy, L.V.; Mohammed, A. Phytochemical analysis and antimicrobial activity of the fruit and petiole extracts of Alocasia longiloba against Escherichia coli and Staphylococcus aureus. AIP Conf. Proc. 2022, 2454, 020026. [Google Scholar] [CrossRef]
- Shin, B.; Park, W. Zoonotic Diseases and Phytochemical Medicines for Microbial Infections in Veterinary Science: Current State and Future Perspective. Front. Veter Sci. 2018, 5, 166. [Google Scholar] [CrossRef]
- Gonelimali, F.D.; Lin, J.; Miao, W.; Xuan, J.; Charles, F.; Chen, M.; Hatab, S.R. Antimicrobial Properties and Mechanism of Action of Some Plant Extracts Against Food Pathogens and Spoilage Microorganisms. Front. Microbiol. 2018, 9, 1639. [Google Scholar] [CrossRef]
- Ajayi, A.; Tanayen, J.; Magomere, A.; Ezeonwumelu, J. Antinociceptive and Anti-Inflammatory Effects of Aqueous Extract of Chenopodium Opulifolium Schrad Leaves. J. Intercult. Ethnopharmacol. 2016, 6, 14–21. [Google Scholar] [CrossRef] [PubMed]
- Bahmani, M.; Saki, K.; Shahsavari, S.; Rafieian-Kopaei, M.; Sepahvand, R.; Adineh, A. Identification of medicinal plants effective in infectious diseases in Urmia, northwest of Iran. Asian Pac. J. Trop. Biomed. 2015, 5, 858–864. [Google Scholar] [CrossRef] [Green Version]
- Tugume, P.; Kakudidi, E.K.; Buyinza, M.; Namaalwa, J.; Kamatenesi, M.; Mucunguzi, P.; Kalema, J. Ethnobotanical survey of medicinal plant species used by communities around Mabira Central Forest Reserve, Uganda. J. Ethnobiol. Ethnomedicine 2016, 12, 1–28. [Google Scholar] [CrossRef] [Green Version]
- Beressa, T.B.; Deyno, S.; Mtewa, A.G.; Aidah, N.; Tuyiringire, N.; Lukubye, B.; Weisheit, A.; Tolo, C.U.; Ogwang, P.E. Potential Benefits of Antiviral African Medicinal Plants in the Management of Viral Infections: Systematic Review. Front. Pharmacol. 2021, 12, 682794. Available online: https://www.frontiersin.org/articles/10.3389/fphar.2021.682794 (accessed on 4 March 2023). [CrossRef]
- AlSheikh, H.M.A.; Sultan, I.; Kumar, V.; Rather, I.A.; Al-Sheikh, H.; Jan, A.T.; Haq, Q.M.R. Plant-Based Phytochemicals as Possible Alternative to Antibiotics in Combating Bacterial Drug Resistance. Antibiotics 2020, 9, 480. [Google Scholar] [CrossRef] [PubMed]
- Russell, W.; Duthie, G. Plant secondary metabolites and gut health: The case for phenolic acids. Proc. Nutr. Soc. 2011, 70, 389–396. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simões, M.; Bennett, R.N.; Rosa, E.A.S. Understanding antimicrobial activities of phytochemicals against multidrug resistant bacteria and biofilms. Nat. Prod. Rep. 2009, 26, 746–757. [Google Scholar] [CrossRef] [PubMed]
- Cox, S.D.; Mann, C.M.; Markham, J.L.; Bell, H.C.; Gustafson, J.E.; Warmington, J.R.; Wyllie, S.G. The mode of antimicrobial action of the essential oil of Melaleuca alternifolia (tea tree oil). J. Appl. Microbiol. 2000, 88, 170–175. [Google Scholar] [CrossRef]
- Maroyi, A. Alternative Medicines for HIV/AIDS in Resource-Poor Settings: Insight from Traditional Medicines Use in Sub- Saharan Africa. Trop. J. Pharm. Res. 2014, 13, 1527–1536. [Google Scholar] [CrossRef] [Green Version]
- Mandal, S.M.; Roy, A.; Ghosh, A.K.; Hazra, T.K.; Basak, A.; Franco, O.L. Challenges and future prospects of antibiotic therapy: From peptides to phages utilization. Front. Pharmacol. 2014, 5, 105. [Google Scholar] [CrossRef]
- Datta, S.; Roy, A. Antimicrobial Peptides as Potential Therapeutic Agents: A Review. Int. J. Pept. Res. Ther. 2021, 27, 555–577. [Google Scholar] [CrossRef]
- Fosgerau, K.; Hoffmann, T. Peptide therapeutics: Current status and future directions. Drug Discov. Today 2015, 20, 122–128. [Google Scholar] [CrossRef] [Green Version]
- Borah, A.; Deb, B.; Chakraborty, S. A Crosstalk on Antimicrobial Peptides. Int. J. Pept. Res. Ther. 2021, 27, 229–244. [Google Scholar] [CrossRef]
- Makumi, A.; Mhone, A.L.; Odaba, J.; Guantai, L.; Svitek, N. Phages for Africa: The Potential Benefit and Challenges of Phage Therapy for the Livestock Sector in Sub-Saharan Africa. Antibiotics 2021, 10, 1085. [Google Scholar] [CrossRef]
- Squires, R.A. Bacteriophage therapy for management of bacterial infections in veterinary practice: What was once old is new again. N. Z. Veter. J. 2018, 66, 229–235. [Google Scholar] [CrossRef]
- Green, S.I.; Kaelber, J.T.; Ma, L.; Trautner, B.W.; Ramig, R.F.; Maresso, A.W. Bacteriophages from ExPEC Reservoirs Kill Pandemic Multidrug-Resistant Strains of Clonal Group ST131 in Animal Models of Bacteremia. Sci. Rep. 2017, 7, srep46151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Zyl, L.J.; Nemavhulani, S.; Cass, J.; Cowan, D.A.; Trindade, M. Three novel bacteriophages isolated from the East African Rift Valley soda lakes. Virol. J. 2016, 13, 204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zaytseva, O.; Neumann, G. Carbon nanomaterials: Production, impact on plant development, agricultural and environmental applications. Chem. Biol. Technol. Agric. 2016, 3, 17. [Google Scholar] [CrossRef] [Green Version]
- Al-Jumaili, A.; Alancherry, S.; Bazaka, K.; Jacob, M.V. Review on the Antimicrobial Properties of Carbon Nanostructures. Materials 2017, 10, 1066. [Google Scholar] [CrossRef]
- Anand, A.; Unnikrishnan, B.; Wei, S.-C.; Chou, C.P.; Zhang, L.-Z.; Huang, C.-C. Graphene oxide and carbon dots as broad-spectrum antimicrobial agents—A minireview. Nanoscale Horizons 2018, 4, 117–137. [Google Scholar] [CrossRef]
- Sengupta, I.; Bhattacharya, P.; Talukdar, M.; Neogi, S.; Pal, S.K.; Chakraborty, S. Bactericidal effect of graphene oxide and reduced graphene oxide: Influence of shape of bacteria. Colloid Interface Sci. Commun. 2018, 28, 60–68. [Google Scholar] [CrossRef]
- Bhatnagar, N. Phytonanotechnology for curbing the menace of MDR Bacteria: A review. Mater. Today Proc. 2021, 43, 3322–3324. [Google Scholar] [CrossRef]
- Atlas, R.M. One Health: Its Origins and Future In One Health: The Human-Animal-Environment Interfaces in Emerging Infectious Diseases: The Concept and Examples of a One Health Approach; Mackenzie, J.S., Jeggo, M., Daszak, P., Richt, J.A., Eds.; Springer: Berlin/Heidelberg, Germany, 2013; pp. 1–13. [Google Scholar] [CrossRef]
- One Health High-Level Expert Panel (OHHLEP); Adisasmito, W.B.; Almuhairi, S.; Behravesh, C.B.; Bilivogui, P.; Bukachi, S.A.; Casas, N.; Becerra, N.C.; Charron, D.F.; Chaudhary, A.; et al. One Health: A new definition for a sustainable and healthy future. PLoS Pathog. 2022, 18, e1010537. [Google Scholar] [CrossRef]
- Evans, B.; Leighton, F. A history of One Health. Rev. Sci. Tech. 2014, 33, 413–420. [Google Scholar] [CrossRef] [PubMed]
- McEwen, S.A.; Collignon, P.J. Antimicrobial Resistance: A One Health Perspective. Microbiol. Spectr. 2018, 6, 521–547. [Google Scholar] [CrossRef] [Green Version]
- Woolhouse, M.; Ward, M.; Van Bunnik, B.; Farrar, J. Antimicrobial resistance in humans, livestock and the wider environment. Philos. Trans. R. Soc. B Biol. Sci. 2015, 370, 20140083. [Google Scholar] [CrossRef] [PubMed]
- The Global Leaders Group on Antimicrobial Resistance. Available online: https://www.amrleaders.org/resources (accessed on 10 August 2022).
- Cornejo, J.; Asenjo, G.; Zavala, S.; Venegas, L.; Galarce, N.; Hormazábal, J.C.; Vergara-E, C.; Lapierre, L. Advances in Integrated Antimicrobial Resistance Surveillance and Control Strategies in Asia-Pacific Economic Cooperation Economies: Assessment of a Multiyear Building Capacity Project. Antibiotics 2022, 11, 1022. [Google Scholar] [CrossRef] [PubMed]
- Wu, D.; Walsh, T.R.; Wu, Y. World Antimicrobial Awareness Week 2021—Spread Awareness, Stop Resistance. China CDC Wkly. 2021, 3, 987–993. [Google Scholar] [CrossRef]
- Langford, B.J.; Matson, K.L.; Eljaaly, K.; Apisarnthanarak, A.; Bailey, P.L.; MacMurray, L.; Marra, A.R.; Simonsen, K.A.; Sreeramoju, P.; Nori, P.; et al. Ten ways to make the most of World Antimicrobial Awareness Week. Antimicrob. Steward. Health Epidemiology 2022, 2, e187. [Google Scholar] [CrossRef]
- O’Brien, M.; Perez, A.; Errecaborde, K. Transforming the One Health workforce: Lessons learned from initiatives in Africa, Asia and Latin America. Rev. Sci. Tech. Int. Off. Epizoot. 2019, 38, 239–250. [Google Scholar] [CrossRef]
- Hitziger, M.; Berezowski, J.; Dürr, S.; Falzon, L.C.; Léchenne, M.; Lushasi, K.; Markosyan, T.; Mbilo, C.; Momanyi, K.N.; Özçelik, R.; et al. System Thinking and Citizen Participation Is Still Missing in One Health Initiatives—Lessons From Fifteen Evaluations. Front. Public Health 2021, 9, 653398. Available online: https://www.frontiersin.org/articles/10.3389/fpubh.2021.653398 (accessed on 19 September 2022). [CrossRef]
- ILRI. One Health Africa Directory. Available online: https://datastudio.google.com/reporting/4ee89aa5-23ce-4cf7-accb-7b1048b6e557/page/LOAUB?s=hPV54T-zIrc (accessed on 10 August 2022).
- Rwego, I.B.; Babalobi, O.O.; Musotsi, P.; Nzietchueng, S.; Tiambo, C.K.; Kabasa, J.D.; Naigaga, I.; Kalema-Zikusoka, G.; Pelican, K. One Health capacity building in sub-Saharan Africa. Infect. Ecol. Epidemiology 2016, 6, 34032. [Google Scholar] [CrossRef] [Green Version]
- Katale, B.Z.; Misinzo, G.; Mshana, S.E.; Chiyangi, H.; Campino, S.; Clark, T.G.; Good, L.; Rweyemamu, M.M.; Matee, M.I. Genetic diversity and risk factors for the transmission of antimicrobial resistance across human, animals and environmental compartments in East Africa: A review. Antimicrob. Resist. Infect. Control. 2020, 9, 127. [Google Scholar] [CrossRef] [PubMed]
- Mshana, S.E.; Matee, M.; Rweyemamu, M. Antimicrobial resistance in human and animal pathogens in Zambia, Democratic Republic of Congo, Mozambique and Tanzania: An urgent need of a sustainable surveillance system. Ann. Clin. Microbiol. Antimicrob. 2013, 12, 28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buregyeya, E.; Atusingwize, E.; Nsamba, P.; Nalwadda, C.; Osuret, J.; Kalibala, P.; Nuwamanya, R.; Okech, S.; Ssekamatte, T.; Nitumusiima, S.; et al. Lessons from a community based interdisciplinary learning exposure: Benefits for both students and communities in Uganda. BMC Med. Educ. 2021, 21, 5. [Google Scholar] [CrossRef] [PubMed]
- Africa, C.D.C. One Health Programme. Available online: https://africacdc.org/programme/surveillance-disease-intelligence/one-health/ (accessed on 11 August 2022).
- Groseclose, S.L.; Buckeridge, D.L. Public Health Surveillance Systems: Recent Advances in Their Use and Evaluation. Annu. Rev. Public Health 2017, 38, 57–79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. Global Antimicrobial Resistance and Use Surveillance System (GLASS) Report: 2021. Available online: https://www.who.int/publications-detail-redirect/9789240027336 (accessed on 21 August 2022).
- Njukeng, P.A.; Ako-Arrey, D.E.; Amin, E.T.; Njumkeng, C.; Wirsiy, F.S. Antimicrobial Resistance in the Central African Region: A Review. J. Environ. Sci. Public Health 2019, 3, 358–378. [Google Scholar] [CrossRef]
- Fuller, W.F.; Hamzat, O.T.; Aboderin, A.O.; Gahimbare, L.; Kapona, O.; Yahaya, A.A.; Kasambara, W.; Nikiema, J.-B.; Ilboudo, D.W.; Mpundu, M.M. National action plan on antimicrobial resistance: An evaluation of implementation in the World Health Organization Africa region. J. Public Health Afr. 2022, 13, 2000. [Google Scholar] [CrossRef]
- Kariuki, S.; Kering, K.; Wairimu, C.; Onsare, R.; Mbae, C. Antimicrobial Resistance Rates and Surveillance in Sub-Saharan Africa: Where Are We Now? Infect. Drug Resist. 2022, 15, 3589–3609. [Google Scholar] [CrossRef]
- Department Health. South Africa Antimicrobial Resistance National Action Plan 2018–2024. Available online: https://www.who.int/publications/m/item/south-africa-south-african-antimicrobial-resistance-national-strategy-framework-a-one-health-approach (accessed on 15 August 2022).
- MCC. National Antimicrobial Resistance Surveillance Framework Tanzania. Available online: https://www.mifugouvuvi.go.tz/uploads/publications/sw1602246063-NATIONAL%20ANTIMICROBIAL%20RESISTANCE%20SURVEILLANCE%20FRAMEWORK.pdf (accessed on 16 August 2022).
- Hein, W.; Aglanu, L.M.; Mensah-Sekyere, M.; Harant, A.; Brinkel, J.; Lamshöft, M.; Lorenz, E.; Eibach, D.; Amuasi, J. Fighting Antimicrobial Resistance: Development and Implementation of the Ghanaian National Action Plan (2017–2021). Antibiotics 2022, 11, 613. [Google Scholar] [CrossRef]
- Kariuki, S.; Keddy, K.H.; Antonio, M.; Okeke, I.N. Antimicrobial resistance surveillance in Africa: Successes, gaps and a roadmap for the future. Afr. J. Lab. Med. 2018, 7, 924. [Google Scholar] [CrossRef] [Green Version]
- Akpan, M.R.; Isemin, N.U.; Udoh, A.E.; Ashiru-Oredope, D. Implementation of antimicrobial stewardship programmes in African countries: A systematic literature review. J. Glob. Antimicrob. Resist. 2020, 22, 317–324. [Google Scholar] [CrossRef]
- Malani, A.N.; Richards, P.G.; Kapila, S.; Otto, M.H.; Czerwinski, J.; Singal, B. Clinical and economic outcomes from a community hospital’s antimicrobial stewardship program. Am. J. Infect. Control. 2013, 41, 145–148. [Google Scholar] [CrossRef] [PubMed]
- Kaki, R.; Elligsen, M.; Walker, S.; Simor, A.; Palmay, L.; Daneman, N. Impact of antimicrobial stewardship in critical care: A systematic review. J. Antimicrob. Chemother. 2011, 66, 1223–1230. [Google Scholar] [CrossRef] [PubMed]
- Stach, L.M.; Hedican, E.B.; Herigon, J.C.; Jackson, M.A.; Newland, J.G. Clinicians’ Attitudes Towards an Antimicrobial Stewardship Program at a Children’s Hospital. J. Pediatr. Infect. Dis. Soc. 2012, 1, 190–197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Antimicrobial Stewardship Programmes in Health-Care Facilities in Low- and Middle-Income Countries: A WHO Practical Toolkit. Available online: https://apps.who.int/iris/handle/10665/329404 (accessed on 10 September 2022).
- Davey, P.; Marwick, C.A.; Scott, C.L.; Charani, E.; McNeil, K.; Brown, E.; Ramsay, C.R.; Wiffen, P.J.; Wilcox, M. Interventions to improve antibiotic prescribing practices for hospital inpatients. Cochrane Database Syst. Rev. 2013, 4, CD003543. [Google Scholar] [CrossRef]
- Brink, A.J.; Messina, A.P.; Feldman, C.; Richards, G.A.; Becker, P.J.; Goff, D.A.; Bauer, K.A.; Nathwani, D.; van den Bergh, D.; on behalf of theNetcare Antimicrobial Stewardship Study Alliance. Antimicrobial stewardship across 47 South African hospitals: An implementation study. Lancet Infect. Dis. 2016, 16, 1017–1025. [Google Scholar] [CrossRef] [Green Version]
- Howard, P.; Pulcini, C.; Levy, H.G.; West, R.M.; Gould, I.M.; Harbarth, S.; Nathwani, D.; ESCMID Study Group for Antimicrobial Policies (ESGAP); ISC Group on Antimicrobial Stewardship. An international cross-sectional survey of antimicrobial stewardship programmes in hospitals. J. Antimicrob. Chemother. 2015, 70, 1245–1255. [Google Scholar] [CrossRef] [Green Version]
- Boyles, T.H.; Whitelaw, A.; Bamford, C.; Moodley, M.; Bonorchis, K.; Morris, V.; Rawoot, N.; Naicker, V.; Lusakiewicz, I.; Black, J.; et al. Antibiotic Stewardship Ward Rounds and a Dedicated Prescription Chart Reduce Antibiotic Consumption and Pharmacy Costs without Affecting Inpatient Mortality or Re-Admission Rates. PLoS ONE 2013, 8, e79747. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Global Action Plan on Antimicrobial Resistance. Available online: https://www.who.int/publications/i/item/9789241509763 (accessed on 10 September 2022).
- Munkholm, L.; Rubin, O. The global governance of antimicrobial resistance: A cross-country study of alignment between the global action plan and national action plans. Glob. Health 2020, 16, 109. [Google Scholar] [CrossRef]
- World Health Organization. Supporting Countries with National Action Plan Implementation. Available online: https://www.who.int/activities/supporting-countries-with-national-action-plan-implementation (accessed on 10 September 2022).
- Kakkar, M.; Chatterjee, P.; Chauhan, A.S.; Grace, D.; Lindahl, J.; Beeche, A.; Jing, F.; Chotinan, S. Antimicrobial resistance in South East Asia: Time to ask the right questions. Glob. Health Action 2018, 11, 1483637. [Google Scholar] [CrossRef]
- Wernli, D.; Haustein, T.; Conly, J.; Carmeli, Y.; Kickbusch, I.; Harbarth, S. A Call for Action: The Application of the International Health Regulations to the Global Threat of Antimicrobial Resistance. PLoS Med. 2011, 8, e1001022. [Google Scholar] [CrossRef] [Green Version]
- Bretaudeau, L.; Tremblais, K.; Aubrit, F.; Meichenin, M.; Arnaud, I. Good Manufacturing Practice (GMP) Compliance for Phage Therapy Medicinal Products. Front. Microbiol. 2020, 11, 1161. [Google Scholar] [CrossRef]
- Opota, O.; Croxatto, A.; Prod’Hom, G.; Greub, G. Blood culture-based diagnosis of bacteraemia: State of the art. Clin. Microbiol. Infect. 2015, 21, 313–322. [Google Scholar] [CrossRef] [Green Version]
- Waddington, C.; Carey, M.E.; Boinett, C.J.; Higginson, E.; Veeraraghavan, B.; Baker, S. Exploiting genomics to mitigate the public health impact of antimicrobial resistance. Genome Med. 2022, 14, 15. [Google Scholar] [CrossRef] [PubMed]
- CRyPTIC Consortium and the 100,000 Genomes Project; Allix-Béguec, C.; Arandjelovic, I.; Bi, L.; Beckert, P.; Bonnet, M.; Bradley, P.; Cabibbe, A.M.; Cancino-Muñoz, I.; Caulfield, M.J.; et al. Prediction of Susceptibility to First-Line Tuberculosis Drugs by DNA Sequencing. N. Engl. J. Med. 2018, 379, 1403–1415. [Google Scholar] [CrossRef] [PubMed]
- Gahamanyi, N.; Song, D.-G.; Yoon, K.-Y.; Mboera, L.E.G.; Matee, M.I.; Mutangana, D.; Komba, E.V.G.; Pan, C.-H.; Amachawadi, R.G. Genomic Characterization of Fluoroquinolone-Resistant Thermophilic Campylobacter Strains Isolated from Layer Chicken Feces in Gangneung, South Korea by Whole-Genome Sequencing. Genes 2021, 12, 1131. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Jiao, M.; Liu, Y.; Ren, Z.; Li, A. Application of Metagenomic Next-Generation Sequencing in Mycobacterium tuberculosis Infection. Front. Med. 2022, 9, 802719. Available online: https://www.frontiersin.org/articles/10.3389/fmed.2022.802719 (accessed on 7 September 2022). [CrossRef] [PubMed]
- de Abreu, V.A.C.; Perdigão, J.; Almeida, S. Metagenomic Approaches to Analyze Antimicrobial Resistance: An Overview. Front. Genet. 2021, 11, 575592. Available online: https://www.frontiersin.org/articles/10.3389/fgene.2020.575592 (accessed on 4 March 2023). [CrossRef]
- Munk, P.; Andersen, V.D.; de Knegt, L.; Jensen, M.S.; Knudsen, B.E.; Lukjancenko, O.; Mordhorst, H.; Clasen, J.; Agersø, Y.; Folkesson, A.; et al. A sampling and metagenomic sequencing-based methodology for monitoring antimicrobial resistance in swine herds. J. Antimicrob. Chemother. 2017, 72, 385–392. [Google Scholar] [CrossRef] [Green Version]
- Aslam, B.; Khurshid, M.; Arshad, M.I.; Muzammil, S.; Rasool, M.; Yasmeen, N.; Shah, T.; Chaudhry, T.H.; Rasool, M.H.; Shahid, A.; et al. Antibiotic Resistance: One Health One World Outlook. Front. Cell. Infect. Microbiol. 2021, 11, 771510. Available online: https://www.frontiersin.org/articles/10.3389/fcimb.2021.771510 (accessed on 19 August 2022). [CrossRef]
- Hendriksen, R.S.; Bortolaia, V.; Tate, H.; Tyson, G.H.; Aarestrup, F.; McDermott, P.F. Using Genomics to Track Global Antimicrobial Resistance. Front. Public Health 2019, 7, 242. Available online: https://www.frontiersin.org/articles/10.3389/fpubh.2019.00242 (accessed on 28 August 2022). [CrossRef] [Green Version]
- Duggett, N.; AbuOun, M.; Randall, L.; Horton, R.; Lemma, F.; Rogers, J.; Crook, D.; Teale, C.; Anjum, M.F. The importance of using whole genome sequencing and extended spectrum beta-lactamase selective media when monitoring antimicrobial resistance. Sci. Rep. 2020, 10, 19880. [Google Scholar] [CrossRef] [PubMed]
- Mlotshwa, B.C.; Mwesigwa, S.; Mboowa, G.; Williams, L.; Retshabile, G.; Kekitiinwa, A.; Wayengera, M.; Kyobe, S.; Brown, C.W.; Hanchard, N.A.; et al. The collaborative African genomics network training program: A trainee perspective on training the next generation of African scientists. Anesthesia Analg. 2017, 19, 826–833. [Google Scholar] [CrossRef] [Green Version]
- NIHR Global Health Research Unit on Genomic Surveillance of AMR Whole-genome sequencing as part of national and international surveillance programmes for antimicrobial resistance: A roadmap. BMJ Glob. Health 2020, 5, e002244. [CrossRef] [PubMed]
- Becker, S.L. WGS for infection prevention and control in Africa. Lancet Microbe 2020, 1, e95–e96. [Google Scholar] [CrossRef] [PubMed]
- Ren, Y.; Chakraborty, T.; Doijad, S.; Falgenhauer, L.; Falgenhauer, J.; Goesmann, A.; Hauschild, A.-C.; Schwengers, O.; Heider, D. Prediction of antimicrobial resistance based on whole-genome sequencing and machine learning. Bioinformatics 2022, 38, 325–334. [Google Scholar] [CrossRef] [PubMed]
- Kouchaki, S.; Yang, Y.; Walker, T.M.; Walker, A.S.; Wilson, D.; Peto, T.E.A.; Crook, D.W.; Clifton, D.A. CRyPTIC Consortium Application of machine learning techniques to tuberculosis drug resistance analysis. Bioinformatics 2019, 35, 2276–2282. [Google Scholar] [CrossRef]
- Yang, Y.; Niehaus, K.E.; Walker, T.M.; Iqbal, Z.; Walker, A.S.; Wilson, D.J.; Peto, T.E.A.; Crook, D.W.; Smith, E.G.; Zhu, T.; et al. Machine learning for classifying tuberculosis drug-resistance from DNA sequencing data. Bioinformatics 2018, 34, 1666–1671. [Google Scholar] [CrossRef] [Green Version]
- Lau, H.J.; Lim, C.H.; Foo, S.C.; Tan, H.S. The role of artificial intelligence in the battle against antimicrobial-resistant bacteria. Curr. Genet. 2021, 67, 421–429. [Google Scholar] [CrossRef]
- Otaigbe, I. Scaling up artificial intelligence to curb infectious diseases in Africa. Front. Digit. Health. 2022, 4, 1030427. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gahamanyi, N.; Umuhoza, T.; Saeed, S.I.; Mayigane, L.N.; Hakizimana, J.N. A Review of the Important Weapons against Antimicrobial Resistance in Sub-Saharan Africa. Appl. Biosci. 2023, 2, 136-156. https://doi.org/10.3390/applbiosci2020011
Gahamanyi N, Umuhoza T, Saeed SI, Mayigane LN, Hakizimana JN. A Review of the Important Weapons against Antimicrobial Resistance in Sub-Saharan Africa. Applied Biosciences. 2023; 2(2):136-156. https://doi.org/10.3390/applbiosci2020011
Chicago/Turabian StyleGahamanyi, Noel, Therese Umuhoza, Shamsaldeen Ibrahim Saeed, Landry Ndriko Mayigane, and Jean Nepomuscene Hakizimana. 2023. "A Review of the Important Weapons against Antimicrobial Resistance in Sub-Saharan Africa" Applied Biosciences 2, no. 2: 136-156. https://doi.org/10.3390/applbiosci2020011