
Seroprevalence of Coxiella burnetii in Occupational Settings: A Meta-Analysis of Italian Studies



Abstract
:Simple Summary
Abstract
1. Introduction
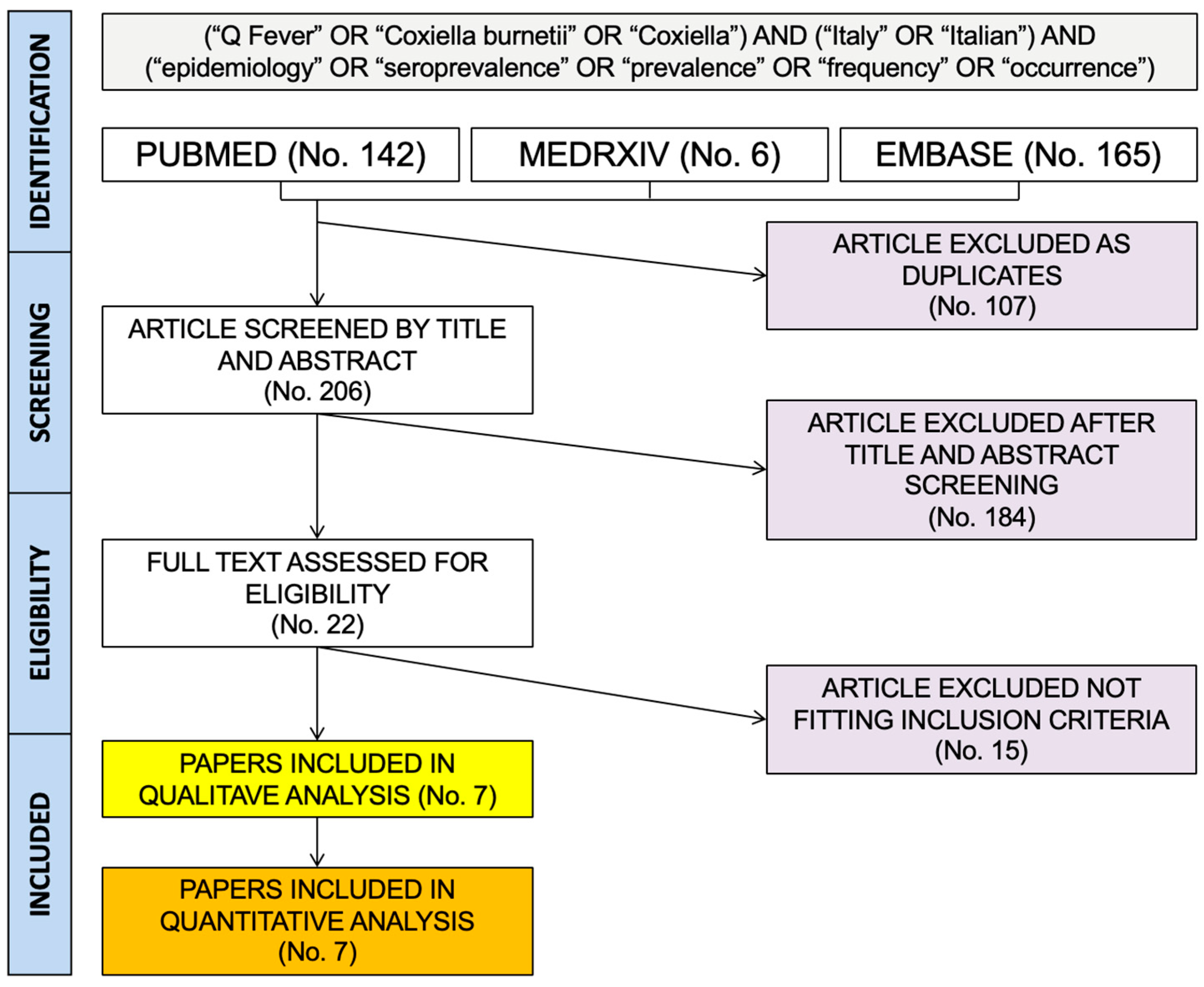
2. Materials and Methods
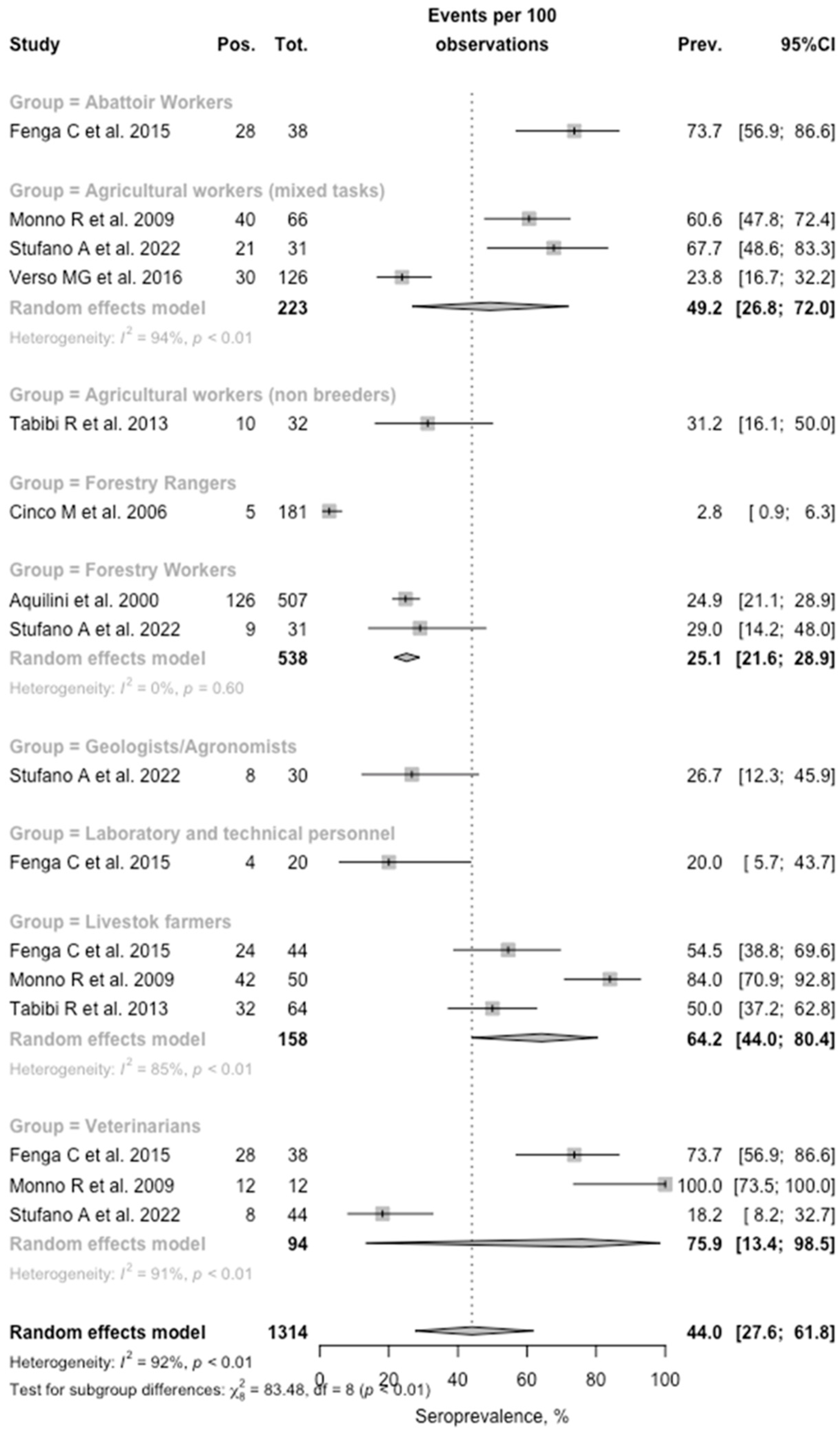
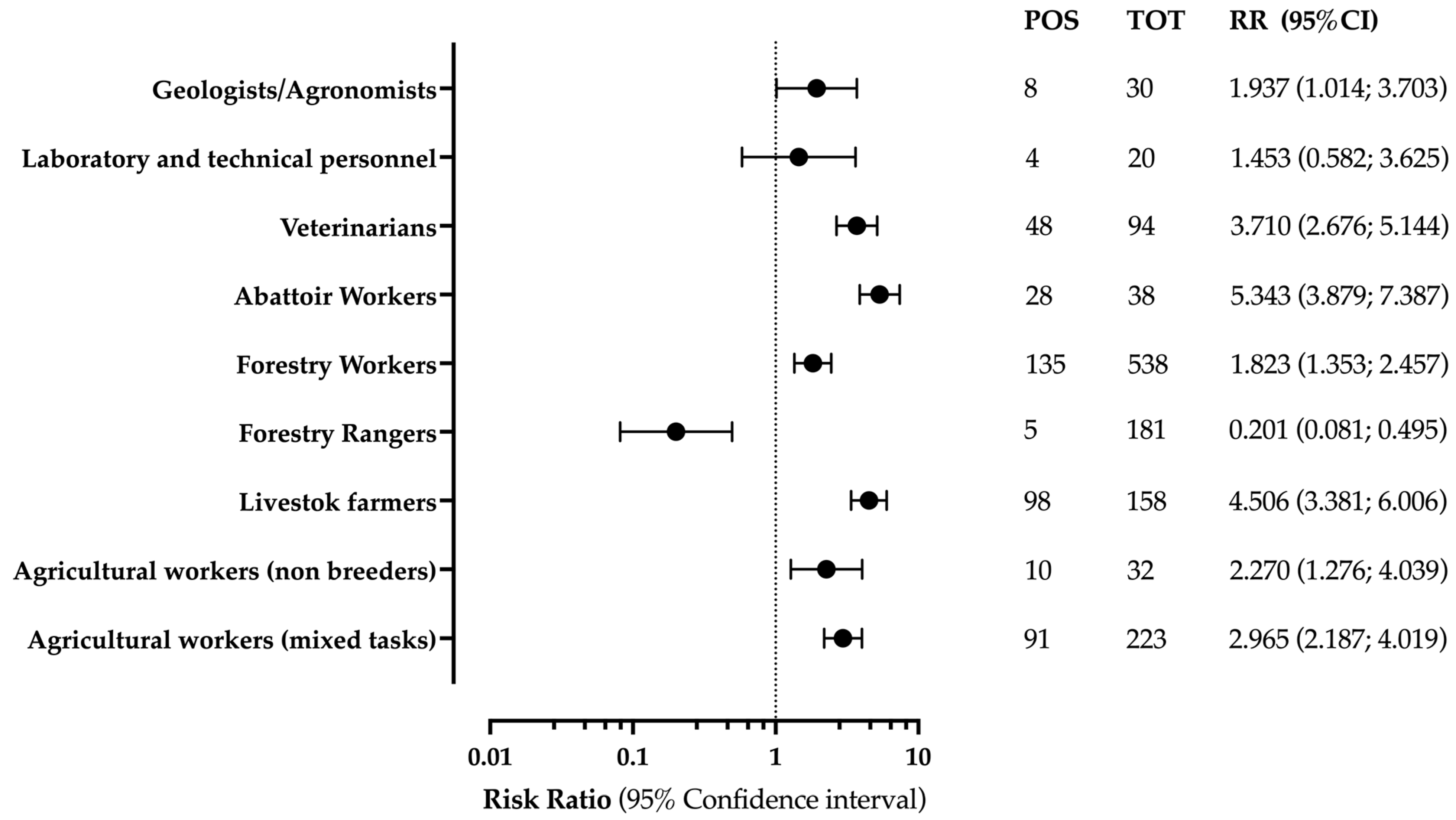
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

References
- Woldeyohannes, S.M.; Gilks, C.F.; Baker, P.; Perkins, N.R.; Reid, S.A. Seroprevlance of Coxiella Burnetii among Abattoir and Slaughterhouse Workers: A Meta-Analysis. One Health 2018, 6, 23–28. [Google Scholar] [CrossRef] [PubMed]
- España, P.P.; Uranga, A.; Cillóniz, C.; Torres, A. Q Fever (Coxiella Burnetii). Semin. Respir. Crit. Care Med. 2020, 41, 509–521. [Google Scholar] [CrossRef] [PubMed]
- González-Barrio, D.; Ruiz-Fons, F. Coxiella Burnetii in Wild Mammals: A Systematic Review. Transbound. Emerg. Dis. 2019, 66, 662–671. [Google Scholar] [CrossRef]
- Bailly, S.; Hozé, N.; Bisser, S.; Zhu-Soubise, A.; Fritzell, C.; Fernandes-Pellerin, S.; Mbouangoro, A.; Rousset, D.; Djossou, F.; Cauchemez, S.; et al. Transmission Dynamics of Q Fever in French Guiana: A Population-Based Cross-Sectional Study. Lancet Reg. Health-Am. 2022, 16, 100385. [Google Scholar] [CrossRef] [PubMed]
- Zakeri, A.; Montaseri, M.; Shekarforoush, S.S. Prevalence and Risk Factors Associated with Q Fever Infection in Slaughterhouse Workers in Fars Province, Iran. Int. Arch. Occup. Environ. Health, 2023; epub ahead of print. [Google Scholar] [CrossRef]
- Dragan, A.L.; Voth, D.E. Coxiella Burnetii: International Pathogen of Mystery. Microbes Infect. 2020, 22, 100–110. [Google Scholar] [CrossRef] [PubMed]
- De Souza Ribeiro Mioni, M.; Costa, F.B.; Ribeiro, B.L.D.; Teixeira, W.S.R.; Pelicia, V.C.; Labruna, M.B.; Rousset, É.; Sidi-Boumedine, K.; Thiéry, R.; Megid, J. Coxiella Burnetii in Slaughterhouses in Brazil: A Public Health Concern. PLoS ONE 2020, 15, e0241246. [Google Scholar] [CrossRef]
- Woldeyohannes, S.M.; Gilks, C.F.; Baker, P.; Perkins, N.R.; Reid, S.A. Q Fever awareness and risk profiles among agricultural show attendees. Aust. J. Rural Health 2022, 30, 601–607. [Google Scholar] [CrossRef]
- Tringali, G.; Mansueto, S. Epidemiology of Q Fever in Italy and in Other Mediterranean Countries. Ser. A Med. Microbiol. Infect. Dis. Virol. Parasitol. 1987, 267, 20–25. [Google Scholar] [CrossRef] [PubMed]
- Georgiev, M.; Afonso, A.; Neubauer, H.; Needham, H.; Thiéry, R.; Rodolakis, A.; Roest, H.J.; Stärk, K.D.; Stegeman, J.A.; Vellema, P.; et al. Review Articles Q Fever in Humans and Farm Animals in Four European Countries, 1982 to 2010. Eurosurveillance 2013, 18, 20407. [Google Scholar] [CrossRef]
- Ruppanner, R.; Brooks, D.; Morrish, D.; Spinelli, J.; Franti, C.E.; Behymer, D.E. Q Fever Hazards from Sheep and Goats Used in Research. Arch. Environ. Health 1982, 37, 103–110. [Google Scholar] [CrossRef]
- Monno, R.; Fumarola, L.; Trerotoli, P.; Cavone, D.; Massaro, T.; Spinelli, L.; Rizzo, C.; Musti, M. Seroprevalence of Q-Fever, Brucellosis and Leptospirosis in Farmers and Agricultural Workers in Bari, Southern Italy. Clin. Microbiol. Infect. 2009, 15, 142–143. [Google Scholar] [CrossRef] [Green Version]
- Monno, R.; Fumarola, L.; Trerotoli, P.; Cavone, D.; Giannelli, G.; Rizzo, C.; Ciceroni, L.; Musti, M. Seroprevalence of Q Fever, Brucellosis and Leptospirosis in Farmers and Agricultural Workers in Bari, Southern Italy. Ann. Agric. Environ. Med. 2009, 16, 205–209. Available online: https://www.aaem.pl/Seroprevalence-of-Q-fever-brucellosis-and-leptospirosis-in-farmers-and-agricultural-workers-in-Bari-Southern-Italy-,71564,0,2.html (accessed on 4 January 2023). [CrossRef] [Green Version]
- Tabibi, R.; Baccalini, R.; Barassi, A.; Bonizzi, L.; Brambilla, G.; Consonni, D.; Melzi D’eril, G.; Romanò, L.; Sokooti, M.; Somaruga, C.; et al. Occupational Exposure to Zoonotic Agents among Agricultural Workers in Lombardy Region, Northern Italy. Ann. Agric. Environ. Med. 2013, 20, 676–681. [Google Scholar]
- van der Giessen, J.; Vlaanderen, F.; Kortbeek, T.; Swaan, C.; van den Kerkhof, H.; Broens, E.; Rijks, J.; Koene, M.; De Rosa, M.; Uiterwijk, M.; et al. Signalling and responding to zoonotic threats using a One Health approach: A decade of the Zoonoses Structure in the Netherlands, 2011 to 2021. Eurosurveillance 2022, 27, 2200039. [Google Scholar] [CrossRef]
- Groten, T.; Kuenzer, K.; Moog, U.; Hermann, B.; Maier, K.; Boden, K. Who Is at Risk of Occupational Q Fever: New Insights from a Multi-Profession Cross-Sectional Study. BMJ Open 2020, 10, e030088. [Google Scholar] [CrossRef] [Green Version]
- Selvaggi, T.M.; Rezza, G.; Scagnelli, M.; Rigoli, R.; Rassu, M.; de Lalla, F.; Pellizzer, G.P.; Tramarin, A.; Bettini, C.; Zampieri, L.; et al. Investigation of a Q-Fever Outbreak in Northern Italy. Eur. J. Epidemiol. 1996, 12, 403–408. [Google Scholar] [CrossRef]
- Aquilini, D.; Parola, P.; Salvo, E.; Paladini, A. Seroepidemiology of the Rickettioses, Human Granulocytic Ehrlichiosis, Lyme Disease, Q Fever, and Tularemia in Forestry Workers in Tuscany, Italy. J. Spirochetal Tick-Borne Dis. 2000, 7, 35–41. [Google Scholar]
- Dal Pozzo, F.; Martinelle, L.; Léonard, P.; Renaville, B.; Renaville, R.; Thys, C.; Smeets, F.; Czaplicki, G.; van Esbroeck, M.; Saegerman, C. Q Fever Serological Survey and Associated Risk Factors in Veterinarians, Southern Belgium, 2013. Transbound. Emerg. Dis. 2017, 64, 959–966. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martini, M.; Baldelli, R.; de Calboli, L.P. An Epidemiological Study on Q Fever in the Emilia-Romagna Region, Italy. Zent. Bakteriol. 1994, 280, 416–422. [Google Scholar] [CrossRef] [PubMed]
- Sellens, E.; Norris, J.M.; Dhand, N.K.; Heller, J.; Hayes, L.; Gidding, H.F.; Willaby, H.; Wood, N.; Graves, S.; Bosward, K.L. Willingness of veterinarians in Australia to recommend Q fever vaccination in veterinary personnel: Implications for workplace health and safety compliance. PLoS ONE 2018, 13, e0198421. [Google Scholar] [CrossRef] [Green Version]
- Acharya, D.; Park, J.H.; Chun, J.H.; Kim, M.Y.; Yoo, S.J.; Lewin, A.; Lee, K. Seroepidemiologic Evidence of Q Fever and Associated Factors among Workers in Veterinary Service Laboratory in South Korea. PLoS Negl. Trop. Dis. 2022, 16, e0010054. [Google Scholar] [CrossRef] [PubMed]
- European Centre for Disease Prevention and Control (ECDC). Annual Epidemiological Report 2019. Q Fever; European Centre for Disease Prevention and Control (ECDC): Stockholm, Sweden, 2021.
- European Food Safety Authority (EFSA); European Centre for Disease Prevention and Control (ECDC). The European Union One Health 2021 Zoonoses Report. EFSA J. 2022, 20, 7666. [Google Scholar] [CrossRef]
- Fenga, C.; Gangemi, S.; de Luca, A.; Calimeri, S.; lo Giudice, D.; Pugliese, M.; Licitra, F.; Alibrandi, A.; Costa, C. Seroprevalence and Occupational Risk Survey for Coxiella Burnetii among Exposed Workers in Sicily, Southern Italy. Int. J. Occup. Med. Health 2015, 28, 901–907. [Google Scholar] [CrossRef]
- Stufano, A.; Iatta, R.; Sgroi, G.; Jahantigh, H.R.; Cagnazzo, F.; Flöel, A.; Lucchese, G.; Loconsole, D.; Centrone, F.; Mendoza-Roldan, J.A.; et al. Seroprevalence of Vector-Borne Pathogens in Outdoor Workers from Southern Italy and Associated Occupational Risk Factors. Parasit Vectors 2022, 15, 264. [Google Scholar] [CrossRef] [PubMed]
- Santoro, D.; Giura, R.; Colombo, M.C.; Antonelli, P.; Gramegna, M.; Gandola, O.; Gridabilla, G. Q Fever in Como, Northern Italy. Emerg. Infect. Dis. 2004, 10, 159–160. [Google Scholar] [CrossRef] [Green Version]
- Starnini, G.; Caccamo, F.; Farchi, F.; Babudieri, S.; Brunetti, B.; Rezza, G. An Outbreak of Q Fever in a Prison in Italy. Epidemiol. Infect. 2005, 133, 377–380. [Google Scholar] [CrossRef] [PubMed]
- Eurostat. European Economic Statistics—2010 Edition, 1st ed.; Gerstberger, C., Ed.; European Union: Luxembourg, 2011; ISBN 9789279161902. [Google Scholar]
- Maucorps, A.; Münch, A.; Brkanovic, S.; Schuh, B.; Dwyer, J.; Vigani, M.; Khafagy, A.; Coto Sauras, M.; Deschellette, P.; Lopez, A.; et al. The EU Farming Employment: Current Challenges and Future Prospects, Policy Department for Structural and Cohesion Policies Directorate-General for Internal Policies PE; Agriculture and Rural Development: Brussels, Belgium, 2019. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Altman, D.; Antes, G.; Atkins, D.; Barbour, V.; Barrowman, N.; Berlin, J.A.; et al. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Rethlefsen, M.L.; Kirtley, S.; Waffenschmidt, S.; Ayala, A.P.; Moher, D.; Page, M.J.; Koffel, J.B. PRISMA-S: An Extension to the PRISMA Statement for Reporting Literature Searches in Systematic Reviews. Syst. Rev. 2021, 10, 39. [Google Scholar] [CrossRef]
- Office of Health Assessment and Translation (OHAT); Division of the National Toxicology Program; National Institute of Environmental Health Sciences. Handbook for Conducting a Literature-Based Health Assessment Using OHAT Approach for Systematic Review and Evidence Integration; National Toxicology Program: Research Triangle Park, NC, USA, 2019. [Google Scholar]
- Eick, S.M.; Goin, D.E.; Chartres, N.; Lam, J.; Woodruff, T.J. Assessing Risk of Bias in Human Environmental Epidemiology Studies Using Three Tools: Different Conclusions from Different Tools. Syst. Rev. 2020, 9, 249. [Google Scholar] [CrossRef] [PubMed]
- R Development Core Team. R a Language and Environment for Statistical Computing: Reference Index; R Foundation for Statistical Computing: Vienna, Austria, 2010; ISBN 3900051070. [Google Scholar]
- Cinco, M.; Luzzati, R.; Mascioli, M.; Floris, R.; Brouqui, P. Serological Evidence of Rickettsia Infections in Forestry Rangers in North-Eastern Italy. Clin. Microbiol. Infect. 2006, 12, 493–495. [Google Scholar] [CrossRef] [Green Version]
- Verso, M.G.; Vesco, G.; Villari, S.; Galluzzo, P.; Gargano, V.; Matranga, D.; de Marchis, P.; Picciotto, D. Analysis of Seroprevalence against Coxiella Burnetii in a Sample of Farm Workers in Western Sicily. Ann. Agric. Environ. Med. 2016, 23, 71–74. [Google Scholar] [CrossRef] [PubMed]
- Cruz, R.; Santos, C.; Esteves, F.; Ferreira, A.S.; Vasconcelos-Nóbrega, C.; Mega, C.; Albuquerque, C.; Teixeira-de-Lemos, E.; Coelho, A.C.; Vala, H.; et al. Occupationally Acquired Q Fever in Shepherds and Sheep Milk Cheesemakers. Ecohealth 2020, 17, 255–257. [Google Scholar] [CrossRef] [PubMed]
- Sellens, E.; Bosward, K.L.; Norris, J.M.; Wood, N.; Heller, J.; Graves, S.; Gidding, H.F. Coxiella Burnetii Seroprevalence in Unvaccinated Veterinary Workers in Australia: Evidence to Support Q Fever Vaccination. Zoonoses Public Health 2020, 67, 79–88. [Google Scholar] [CrossRef] [PubMed]
- Park, J.H.; do Hwang, S.; Acharya, D.; Lee, S.H.; Hwang, K.J.; Yoo, S.J.; Lee, K. Seroreactivity and Risk Factors Associated with Coxiella Burnetii Infection among Cattle Slaughterhouse Workers in South Korea. Int. J. Environ. Res. Public Health 2018, 15, 2264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Szymańska-Czerwińska, M.; Galińska, E.M.; Niemczuk, K.; Knap, J.P. Prevalence of Coxiella Burnetii Infection in Humans Occupationally Exposed to Animals in Poland. Vector-Borne Zoonotic Dis. 2015, 15, 261–267. [Google Scholar] [CrossRef] [Green Version]
- O’Neill, T.J.; Sargeant, J.M.; Poljak, Z. The Effectiveness of Coxiella Burnetii Vaccines in Occupationally Exposed Populations: A Systematic Review and Meta-Analysis. Zoonoses Public Health 2014, 61, 81–96. [Google Scholar] [CrossRef]
- Manzoli, L.; Sotgiu, G.; Magnavita, N.; Durando, P.; Barchitta, M.; Carducci, A.; Conversano, M.; de Pasquale, G.; Dini, G.; Firenze, A.; et al. Evidence-Based Approach for Continuous Improvement of Occupational Health. Epidemiol. Prev. 2015, 39, 81–85. [Google Scholar]
- Meadows, S.; Jones-Bitton, A.; McEwen, S.A.; Jansen, J.; Patel, S.N.; Filejski, C.; Menzies, P. Coxiella Burnetii (Q Fever) Seropositivity and Associated Risk Factors in Sheep and Goat Farm Workers in Ontario, Canada. Vector-Borne Zoonotic Dis. 2016, 16, 643–649. [Google Scholar] [CrossRef]
- Tavella, A.; Trevisiol, K.; Morosetti, G.; Fobatscher, C.; Piffer, C.; Fugatti, A. Q Fever: The Importance of Surveillance in the Autonomous Province of Bolzano (Italy). Int. J. Infect. Dis. 2014, 21, 188–189. [Google Scholar] [CrossRef] [Green Version]
- Riccò, M.; Ferraro, P.; Peruzzi, S.; Balzarini, F.; Ranzieri, S. Hantaviruses in Agricultural and Forestry Workers: Knowledge, Attitudes and Practices in Italian Physicians. Trop. Med. Infect. Dis. 2021, 6, 169. [Google Scholar] [CrossRef]
- Riccò, M.; Peruzzi, S.; Ranzieri, S.; Magnavita, N. Occupational Hantavirus Infections in Agricultural and Forestry Workers: A Systematic Review and Metanalysis. Viruses 2021, 13, 2150. [Google Scholar] [CrossRef] [PubMed]
- Riccò, M. Epidemiology of Tick-Borne Encephalitis in North-Eastern Italy (2017–2020): International Insights from National Notification Reports. Acta Biomed. 2021, 92, e2021229. [Google Scholar] [PubMed]
- Riccò, M.; Bragazzi, N.L.; Vezzosi, L.; Balzarini, F.; Colucci, E.; Veronesi, L.; Riccò, M.; Bragazzi, N.L.; Vezzosi, L.; Balzarini, F.; et al. Knowledge, Attitudes, and Practices on Tick-Borne Human Diseases and Tick-Borne Encephalitis Vaccine among Farmers from North-Eastern Italy (2017). J. Agromed. 2020, 25, 73–85. [Google Scholar] [CrossRef] [PubMed]
- Riccò, M.; Gualerzi, G.; Ranzieri, S.; Ferraro, P.; Bragazzi, N.L. Knowledge, Attitudes, Practices (KAP) of Italian Occupational Physicians towards Tick Borne Encephalitis. Trop. Med. Infect. Dis. 2020, 5, 117. [Google Scholar] [CrossRef] [PubMed]
- Riccò, M.; Peruzzi, S.; Ranzieri, S.; Balzarini, F.; Valente, M.; Marchesi, F.; Bragazzi, N.L. Hantavirus Infections in Italy: Not Reported Doesn’t Mean Inexistent. Authors and Affiliations. Acta Biomed. 2020, 92, e2021324. [Google Scholar]
- Riccò, M.; Vezzosi, L.; Mezzoiuso, A.G. Occupational Eye Injury in the Agricultural Settings: A Retrospective Study from North-Eastern Italy. Acta Biomed. 2020, 90, 457–467. [Google Scholar]
- Riccò, M.; Vezzosi, L.; Balzarini, F.; Gualerzi, G.; Valente, M.; Bragazzi, N.L. Air Temperatures and Occupational Injuries in the Agricultural Settings: A Report from Northern Italy (Po River Valley, 2013–2017). Acta Biomed. 2020, 91, e2020094. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Item | Definition |
|---|---|
| Population of interest | Workers potentially exposed to C. burnetii |
| Investigated result | Seroprevalence of biomarkers for previous exposure to C. burnetii |
| Control | Healthy individuals not occupationally exposed |
| Outcome | Seroprevalence of previous infection of C. burnetii among occupationally exposed individuals; risk of Q Fever in occupational settings. |
| Study (Year) | Region | Occupational Settings | Procedure | Subjects (No.) | Positive (No., %) | Reference |
|---|---|---|---|---|---|---|
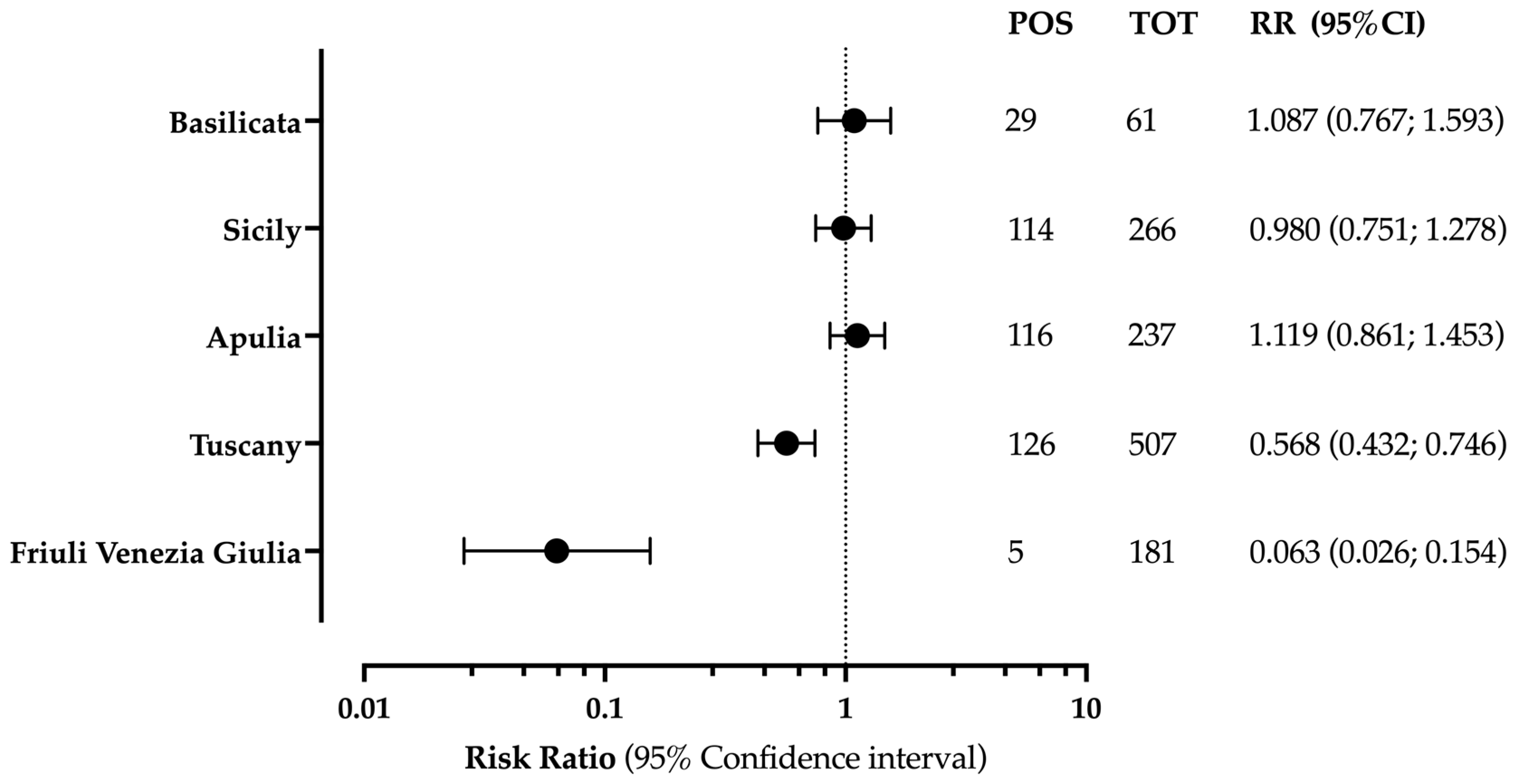
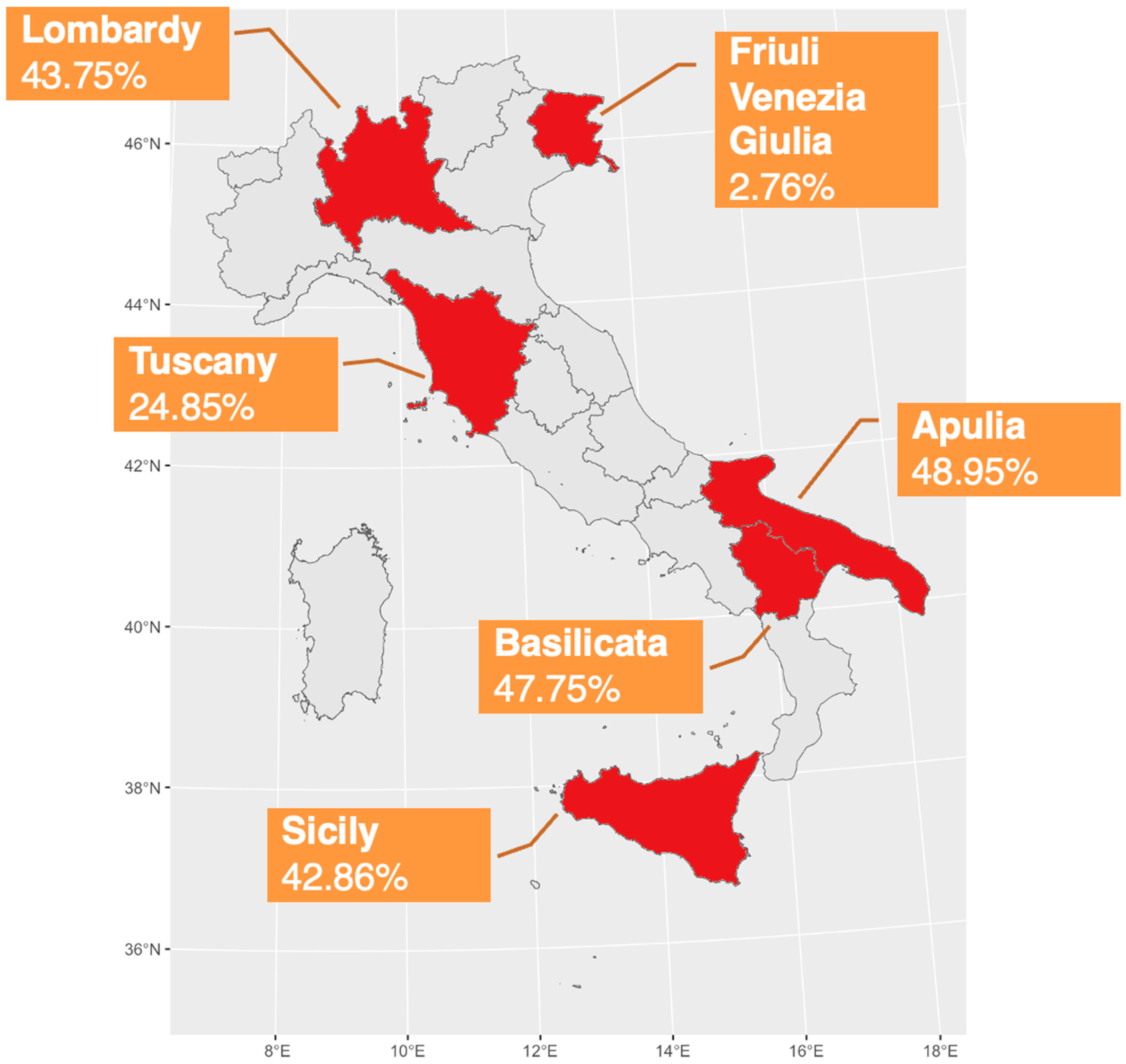
| Aquilini et al. (2000) | Tuscany | Forestry Workers | IFA | 507 | 126, 24.9% | [18] |
| Cinco et al. (2006) | Friuli Venezia Giulia | Forestry Rangers | ELISA | 181 | 5, 2.8% | [36] |
| Monno et al. (2009) | Apulia | Animal Farmers (breeders) | IFA | 50 | 42, 84.0% | [13] |
| Agricultural Workers (mixed tasks) | 66 | 40, 60.6% | ||||
| Veterinarians | 12 | 12, 100% | ||||
| Healthy donors (Controls) | 280 | 38, 13.6% | ||||
| Tabibi et al. (2013) | Lombardy | Animal Farmers (breeders) | CFT | 64 | 32, 50.0% | [14] |
| Agricultural Workers (non breeders) | 32 | 10, 31.2% | ||||
| Fenga et al. (2015) | Sicily | Veterinarians | ELISA | 38 | 28, 73.7% | [25] |
| Abattoir workers | 38 | 28, 73.7% | ||||
| Animal Farmers (breeders) | 44 | 24, 54.5% | ||||
| Laboratory workers | 20 | 4, 20.0% | ||||
| Healthy donors (Controls) | 42 | 6, 14.3% | ||||
| Verso et al. (2016) | Sicily | Agricultural Workers (mixed tasks) | IFA | 126 | 30, 23.8% | [37] |
| Stufano et al. (2022) | Apulia and Basilicata | Forestry workers | ELISA | 31 | 9, 29.0% | [26] |
| Farmers | 31 | 21, 67.7% | ||||
| Veterinarians | 44 | 8, 18.2% | ||||
| Geologists/Agronomists | 30 | 8, 26.7% | ||||
| Administrative employees (Controls) | 34 | 5, 14.7% |
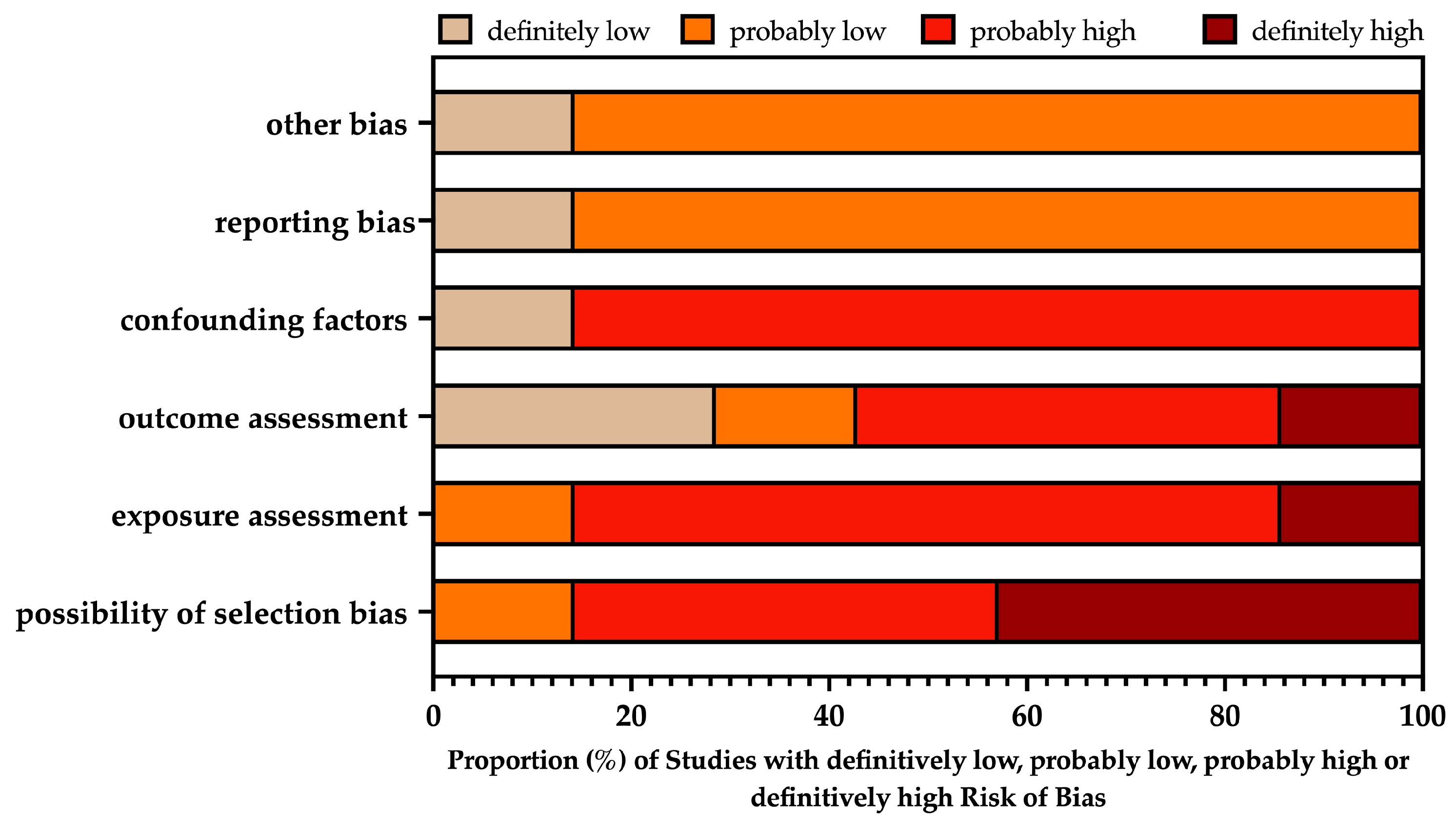
 = definitively high; = probably high;
= definitively high; = probably high;  = probably low; = definitively low.
= definitively high; = probably high; = probably low; = definitively low.
= probably low; = definitively low.
= definitively high; = probably high; = probably low; = definitively low.| Study | RISK OF BIAS | |||||
|---|---|---|---|---|---|---|
| D1 | D2 | D3 | D4 | D5 | D6 | |
| Aquilini et al. (2000) [18] | | | | | | |
| Cinco et al. (2006) [36] | | | | | | |
| Monno et al. (2009) [13] | | | | | | |
| Tabibi et al. (2013) [14] | | | | | | |
| Fenga et al. (2015) [25] | | | | | | |
| Verso et al. (2016) [37] | | | | | | |
| Stufano et al. (2022) [26] | | | | | | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Riccò, M.; Baldassarre, A.; Corrado, S.; Marchesi, F. Seroprevalence of Coxiella burnetii in Occupational Settings: A Meta-Analysis of Italian Studies. Zoonotic Dis. 2023, 3, 38-51. https://doi.org/10.3390/zoonoticdis3010005
Riccò M, Baldassarre A, Corrado S, Marchesi F. Seroprevalence of Coxiella burnetii in Occupational Settings: A Meta-Analysis of Italian Studies. Zoonotic Diseases. 2023; 3(1):38-51. https://doi.org/10.3390/zoonoticdis3010005
Chicago/Turabian StyleRiccò, Matteo, Antonio Baldassarre, Silvia Corrado, and Federico Marchesi. 2023. "Seroprevalence of Coxiella burnetii in Occupational Settings: A Meta-Analysis of Italian Studies" Zoonotic Diseases 3, no. 1: 38-51. https://doi.org/10.3390/zoonoticdis3010005