
School-Based Interventions on Human Papillomavirus in Africa: A Systematic Scoping Review
 , , and
, , and
Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Protocol Registration
2.3. Research Question
2.4. Eligibility Criteria
- Refereed original research articles which reported the implementation of a school-based HPV intervention/program.
- Cohort studies, case-control studies, before and after studies, experimental studies, and controlled trials.
- Articles published in the English language.
- Articles with accessible full text.
- Studies conducted in Africa.
- ○
- Non-refereed articles.
- ○
- Non-articles such as dissertations, books, book chapters, bibliometric reviews, scoping reviews, systematic reviews and meta-analyses, editorials, letters, commentaries, opinions, etc.
- ○
- Articles published in Spanish, French, Arabic, Italian, or any other non-English language.
- ○
- Articles reporting school-based cross-sectional studies on HPV.
- ○
- Articles without accessible full text.
- ○
- Articles reporting clinic- or community-based HPV intervention/programs in Africa.
- ○
- Studies conducted among population groups in American, Asian, European, and Australian countries.
2.5. Search Strategy
2.6. Deduplication
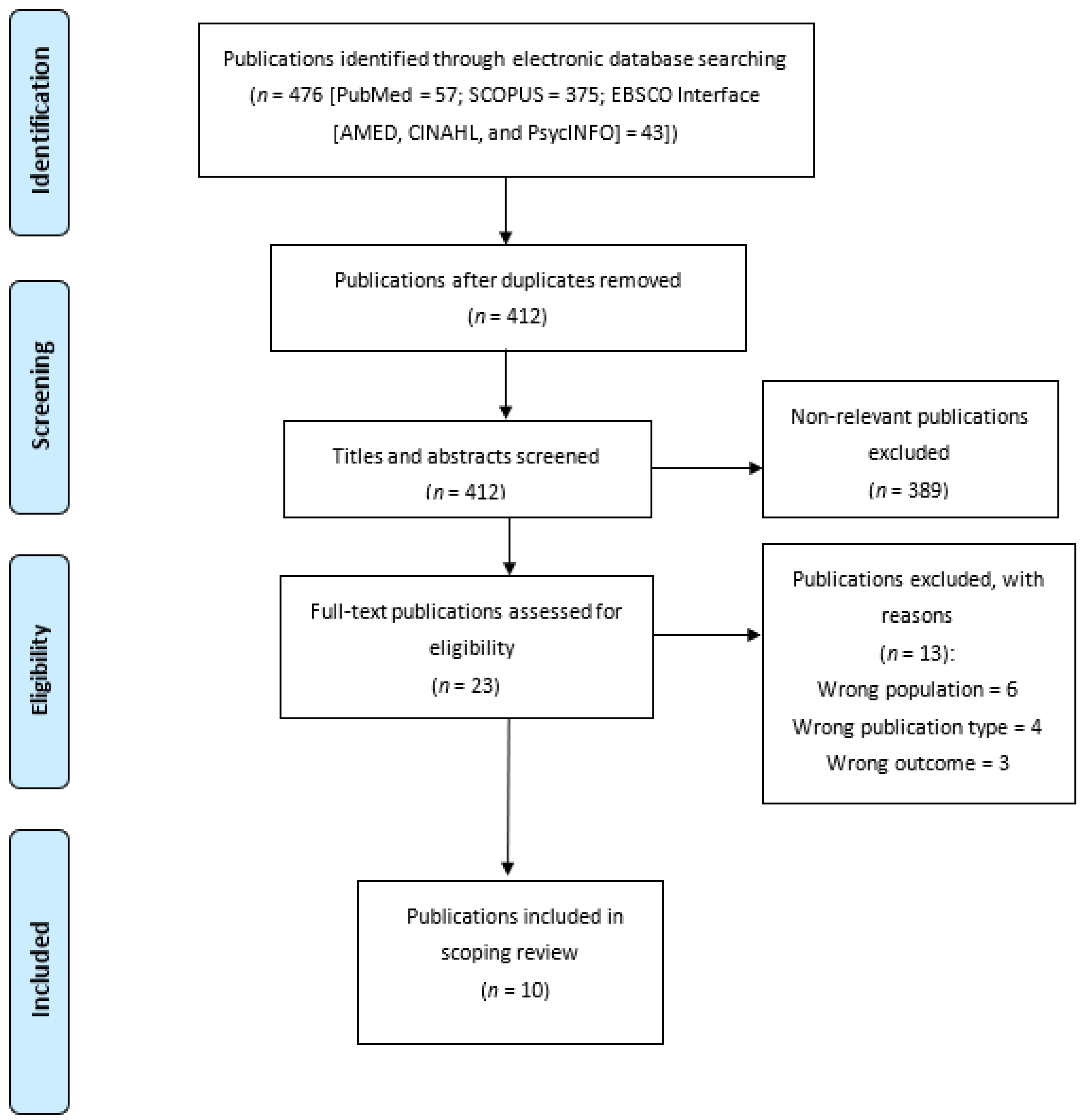
2.7. Selection of Studies
2.8. Quality Appraisal
2.9. Data Extraction, Collation and Summarization
3. Results
3.1. Awareness and Knowledge of Human Papillomavirus and Cervical Cancer
3.1.1. Extent of Knowledge Pre-Intervention
3.1.2. Change in Knowledge Post-Intervention
3.2. Determinants of Awareness and Knowledge of Cervical Cancer and Human Papillomavirus: Pre- and Post-Intervention
3.3. Impact of School-Based Interventions on Health Behavior
3.4. Determinants of Post-Intervention Health Behavior: Screening and Vaccination
3.5. Efficacy of HPV Vaccine and Other Issues
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
| Scopus-Based Search | |||
|---|---|---|---|
| Search Focus | No. | Search String | Hits |
| Publications on schools | #1 | (TITLE-ABS-KEY (school) OR TITLE-ABS-KEY (students) OR TITLE-ABS-KEY (adolescents) OR TITLE-ABS-KEY (youth)) | 4,508,053 |
| Publications on HPV | #2 | (TITLE-ABS-KEY (hpv) OR TITLE-ABS-KEY ( human AND papillomavir *) OR TITLE-ABS-KEY (human AND papilloma AND vir *)) | 79,064 |
| Publications on interventions | #3 | (TITLE-ABS-KEY (program *) OR TITLE-ABS-KEY (intervention) OR TITLE-ABS-KEY (implementation) OR TITLE-ABS-KEY (“case-control”) OR TITLE-ABS-KEY (“cohort study”) OR TITLE-ABS-KEY (“before and after study”) OR TITLE-ABS-KEY (“controlled trial”)) | 7,862,182 |
| Publications on African countries, territories, and dependencies | #4 | ((TITLE-ABS-KEY (angola) OR TITLE-ABS-KEY (benin) OR TITLE-ABS-KEY (botswana) OR TITLE-ABS-KEY (burkina AND faso) OR TITLE-ABS-KEY (burundi) OR TITLE-ABS-KEY (cameroon) OR TITLE-ABS-KEY (cabo AND verde) OR TITLE-ABS-KEY (cape AND verde) OR TITLE-ABS-KEY (central AND african AND republic) OR TITLE-ABS-KEY (chad) OR TITLE-ABS-KEY (comoros) OR TITLE-ABS-KEY (congo) OR TITLE-ABS-KEY (ivory AND coast) OR TITLE-ABS-KEY (democratic AND republic AND of AND congo) OR TITLE-ABS-KEY (djibouti) OR TITLE-ABS-KEY (equatorial AND guinea) OR TITLE-ABS-KEY (eritrea) OR TITLE-ABS-KEY (ethiopia) OR TITLE-ABS-KEY (gabon) OR TITLE-ABS-KEY (gambia) OR TITLE-ABS-KEY (ghana) OR TITLE-ABS-KEY (guinea) OR TITLE-ABS-KEY (guinea-bissau) OR TITLE-ABS-KEY (kenya) OR TITLE-ABS-KEY (lesotho) OR TITLE-ABS-KEY (liberia) OR TITLE-ABS-KEY (madagascar) OR TITLE-ABS-KEY (malawi) OR TITLE-ABS-KEY (mali) OR TITLE-ABS-KEY (mauritania) OR TITLE-ABS-KEY (mauritius) OR TITLE-ABS-KEY (mayotte) OR TITLE-ABS-KEY (mozambique) OR TITLE-ABS-KEY (namibia) OR TITLE-ABS-KEY (niger) OR TITLE-ABS-KEY (nigeria) OR TITLE-ABS-KEY (reunion) OR TITLE-ABS-KEY (rwanda) OR TITLE-ABS-KEY (saint AND helena) OR TITLE-ABS-KEY (sao AND tome AND principe) OR TITLE-ABS-KEY (senegal) OR TITLE-ABS-KEY (seychelles) OR TITLE-ABS-KEY (sierra AND leone) OR TITLE-ABS-KEY (somalia) OR TITLE-ABS-KEY (south AND africa) OR TITLE-ABS-KEY (south AND sudan))) OR ((TITLE-ABS-KEY (eswatini) OR TITLE-ABS-KEY (togo) OR TITLE-ABS-KEY (uganda) OR TITLE-ABS-KEY (zambia) OR TITLE-ABS-KEY (zimbabwe) O TITLE-ABS-KEY (egypt) OR TITLE-ABS-KEY (libya) OR TITLE-ABS-KEY (algeria) OR TITLE-ABS-KEY (tunisia) OR TITLE-ABS-KEY (morocco) OR TITLE-ABS-KEY (western AND sahara) OR TITLE-ABS-KEY (sudan) OR TITLE-ABS-KEY (tunisia))) | 1,148,745 |
| Publications on school-based HPV interventions in Africa | #5 (#1 AND #2 AND #3 AND #4) | ((TITLE-ABS-KEY (hpv) OR TITLE-ABS-KEY (human AND papillomavir *) OR TITLE-ABS-KEY (human AND papilloma AND vir *))) AND ((TITLE-ABS-KEY (program *) OR TITLE-ABS-KEY (intervention) OR TITLE-ABS-KEY (implementation) OR TITLE-ABS-KEY (“case-control”) OR TITLE-ABS-KEY (“cohort study”) OR TITLE-ABS-KEY (“before and after study”) OR TITLE-ABS-KEY ("controlled trial”))) AND ((TITLE-ABS-KEY (school) OR TITLE-ABS-KEY (students) OR TITLE-ABS-KEY (adolescents) OR TITLE-ABS-KEY (youth))) AND (((TITLE-ABS-KEY (angola) OR TITLE-ABS-KEY (benin) OR TITLE-ABS-KEY (botswana) OR TITLE-ABS-KEY (burkina AND faso) OR TITLE-ABS-KEY (burundi) OR TITLE-ABS-KEY (cameroon) OR TITLE-ABS-KEY (cabo AND verde) OR TITLE-ABS-KEY (cape AND verde) OR TITLE-ABS-KEY (central AND african AND republic) OR TITLE-ABS-KEY (chad) OR TITLE-ABS-KEY (comoros) OR TITLE-ABS-KEY (congo) OR TITLE-ABS-KEY (ivory AND coast) OR TITLE-ABS-KEY (democratic AND republic AND of AND congo) OR TITLE-ABS-KEY (djibouti) OR TITLE-ABS-KEY (equatorial AND guinea) OR TITLE-ABS-KEY (eritrea) OR TITLE-ABS-KEY (ethiopia) OR TITLE-ABS-KEY (gabon) OR TITLE-ABS-KEY (gambia) OR TITLE-ABS-KEY (ghana) OR TITLE-ABS-KEY (guinea) OR TITLE-ABS-KEY (guinea-bissau) OR TITLE-ABS-KEY (kenya) OR TITLE-ABS-KEY (lesotho) OR TITLE-ABS-KEY (liberia) OR TITLE-ABS-KEY (madagascar) OR TITLE-ABS-KEY (malawi) OR TITLE-ABS-KEY (mali) OR TITLE-ABS-KEY (mauritania) OR TITLE-ABS-KEY (mauritius) OR TITLE-ABS-KEY (mayotte) OR TITLE-ABS-KEY (mozambique) OR TITLE-ABS-KEY (namibia) OR TITLE-ABS-KEY (niger) OR TITLE-ABS-KEY (nigeria) OR TITLE-ABS-KEY (reunion) OR TITLE-ABS-KEY (rwanda) OR TITLE-ABS-KEY (saint AND helena) OR TITLE-ABS-KEY (sao AND tome AND principe) OR TITLE-ABS-KEY (senegal) OR TITLE-ABS-KEY (seychelles) OR TITLE-ABS-KEY (sierra AND leone) OR TITLE-ABS-KEY (somalia) OR TITLE-ABS-KEY (south AND africa) OR TITLE-ABS-KEY (south AND sudan))) OR ((TITLE-ABS-KEY (eswatini) OR TITLE-ABS-KEY (togo) OR TITLE-ABS-KEY (uganda) OR TITLE-ABS-KEY (zambia) OR TITLE-ABS-KEY (zimbabwe) OR TITLE-ABS-KEY (egypt) OR TITLE-ABS-KEY (libya) OR TITLE-ABS-KEY (algeria) OR TITLE-ABS-KEY (tunisia) OR TITLE-ABS-KEY (morocco) OR TITLE-ABS-KEY (western AND sahara) OR TITLE-ABS-KEY (sudan) OR TITLE-ABS-KEY (tunisia) | 375 |
| PubMed-Based Search | |||
| Search Focus | No. | Search String | Hits |
| Publications on schools | #1 | (((school[MeSH Terms]) OR (students[MeSH Terms])) OR (adolescents[MeSH Terms])) OR (youth[MeSH Terms]) | 2,378,151 |
| Publications on HPV | #2 | ((HPV[MeSH Terms]) OR (human papillomavirus[MeSH Terms])) OR (human papilloma virus[MeSH Terms]) | 36,659 |
| Publications on interventions | #3 | ((((((program * [MeSH Terms]) OR (intervention[MeSH Terms])) OR (implementation[MeSH Terms])) OR (case-control[MeSH Terms])) OR (cohort study[MeSH Terms])) OR (before and after study[MeSH Terms])) OR (controlled trial[MeSH Terms]) | 3,496,068 |
| Publications on African countries, territories, and dependencies | #4 | (((((((((((((((((((((((((((((((((((((((((((((((((((((((((((Algeria[MeSH Terms]) OR (Angola[MeSH Terms])) OR (Benin[MeSH Terms])) OR (Botswana[MeSH Terms])) OR (burkina faso[MeSH Terms])) OR (burundi[MeSH Terms])) OR (cabo verde[MeSH Terms])) OR (cape verde[MeSH Terms])) OR (cameroon[MeSH Terms])) OR (central african republic[MeSH Terms])) OR (chad[MeSH Terms])) OR (comoros[MeSH Terms])) OR (congo[MeSH Terms])) OR (ivory coast[MeSH Terms])) OR (cote d ivoire[MeSH Terms])) OR (djibouti[MeSH Terms])) OR (democratic republic of congo[MeSH Terms])) OR (egypt[MeSH Terms])) OR (equatorial guinea[MeSH Terms])) OR (eritrea[MeSH Terms])) OR (eswatini[MeSH Terms])) OR (ethiopia[MeSH Terms])) OR (gabon[MeSH Terms])) OR (gambia[MeSH Terms])) OR (ghana[MeSH Terms])) OR (guinea[MeSH Terms])) OR (guinea bissau[MeSH Terms])) OR (kenya[MeSH Terms])) OR (lesotho[MeSH Terms])) OR (liberia[MeSH Terms])) OR (libya[MeSH Terms])) OR (madagascar[MeSH Terms])) OR (malawi[MeSH Terms])) OR (mali[MeSH Terms])) OR (mauritania[MeSH Terms])) OR (mauritius[MeSH Terms])) OR (morocco[MeSH Terms])) OR (mozambique[MeSH Terms])) OR (namibia[MeSH Terms])) OR (niger[MeSH Terms])) OR (nigeria[MeSH Terms])) OR (rwanda[MeSH Terms])) OR (sao tome and principe[MeSH Terms])) OR (senegal[MeSH Terms])) OR (seychelles[MeSH Terms])) OR (sierra leone[MeSH Terms])) OR (somalia[MeSH Terms])) OR (south africa[MeSH Terms])) OR (south sudan[MeSH Terms])) OR (sudan[MeSH Terms])) OR (tanzania[MeSH Terms])) OR (togo[MeSH Terms])) OR (tunisia[MeSH Terms])) OR (uganda[MeSH Terms])) OR (zambia[MeSH Terms])) OR (zimbabwe[MeSH Terms])) OR (reunion[MeSH Terms])) OR (saint helena[MeSH Terms])) OR (western sahara[MeSH Terms])) OR (mayotte[MeSH Terms]) | 262,847 |
| Publications on school-based HPV interventions in Africa | #5 (#1 AND #2 AND #3 AND #4) | (((#1) AND (#2)) AND (#3)) AND (#4) | 57 |
| Allied and Complementary Medicine (AMED), CINAHL, And PsycInfo using the EBSCO Interface | |||
| Publications on schools | S1 | AB School OR AB students OR AB adolescents OR AB youth | 1,290,085 |
| Publications on HPV | S2 | AB human papillomavirus OR AB human papilloma virus OR AB hpv | 14,277 |
| Publications on interventions | S3 | AB program* OR AB intervention OR AB implementation OR AB case-control OR AB cohort study OR AB (before and after study) OR AB controlled trial | 1,883,416 |
| Publications on African countries, territories, and dependencies | S4 | AB algeria OR AB angola OR AB benin OR AB botswana OR AB burkina faso OR AB burundi OR AB cape verde OR AB cabo verde OR AB cameroon OR AB central african republic OR AB chad OR AB comoros OR AB congo OR AB cote d’ivoire OR AB ivory coast OR AB djibouti OR AB democratic republic of congo OR AB egypt OR AB equatorial guinea OR AB eritrea OR AB eswatini OR AB ethiopia OR AB gabon OR AB gambia OR AB ghana OR AB guinea OR AB guinea bissau OR AB kenya OR AB lesotho OR AB liberia OR AB libya OR AB madagascar OR AB malawi OR AB mali OR AB mauritania OR AB mauritius OR AB morocco OR AB mozambique OR AB namibia OR AB niger OR AB nigeria OR AB rwanda OR AB (sao tome and principe) OR AB senegal OR AB seychelles OR AB sierra leone OR AB somalia OR AB south Africa OR AB south sudan OR AB sudan OR AB tanzania OR AB togo OR AB tunisia OR AB uganda OR AB zambia OR AB zimbabwe OR AB reunion OR AB saint helena OR AB western sahara OR AB mayotte | 106,753 |
| Publications on school-based HPV interventions in Africa | S5 | S1 AND S2 AND S3 AND S4 | 51 |
References
- De Vuyst, H.; Alemany, L.; Lacey, C.; Chibwesha, C.J.; Sahasrabuddhe, V.; Banura, C.; Denny, L.; Parham, G.P. The burden of human papillomavirus infections and related diseases in sub-saharan Africa. Vaccine 2013, 31 (Suppl. 5), F32–F46. [Google Scholar] [CrossRef] [Green Version]
- Kombe, A.J.K.; Li, B.; Zahid, A.; Mengist, H.M.; Bounda, G.A.; Zhou, Y.; Jin, T. Epidemiology and Burden of Human Papillomavirus and Related Diseases, Molecular Pathogenesis, and Vaccine Evaluation. Front. Public Health 2021, 8, 552028. [Google Scholar] [CrossRef]
- Boyle, P.; Ngoma, T.; Sullivan, R.; Brawley, O. Cancer in Africa: The way forward. Ecancermedicalscience 2019, 13, 953. [Google Scholar] [CrossRef]
- Timbang, M.R.; Sim, M.W.; Bewley, A.F.; Farwell, D.G.; Mantravadi, A.; Moore, M.G. HPV-related oropharyngeal cancer: A review on burden of the disease and opportunities for prevention and early detection. Hum. Vaccin Immunother. 2019, 15, 1920–1928. [Google Scholar] [CrossRef]
- Bednarczyk, R.A. Addressing HPV vaccine myths: Practical information for healthcare providers. Hum. Vaccin Immunother. 2019, 15, 1628–1638. [Google Scholar] [CrossRef]
- Deignan, C.; Swartz, A.; Cooper, S.; Colvin, C.J. Stakeholders’ Understandings of Human Papillomavirus (HPV) Vaccination in Sub-Saharan Africa: A Rapid Qualitative Systematic Review. Vaccines 2021, 9, 496. [Google Scholar] [CrossRef]
- Lubeya, M.K.; Mwanahamuntu, M.; Chibwesha, C.; Mukosha, M.; Wamunyima, M.M.; Kawonga, M. Implementation strategies to increase human papillomavirus vaccination uptake for adolescent girls in sub-Saharan Africa: A scoping review protocol. PLoS ONE 2022, 17, e0267617. [Google Scholar] [CrossRef]
- Amponsah-Dacosta, E.; Blose, N.; Nkwinika, V.V.; Chepkurui, V. Human Papillomavirus Vaccination in South Africa: Programmatic Challenges and Opportunities for Integration with Other Adolescent Health Services? Front. Public Health 2022, 10, 799984. [Google Scholar] [CrossRef] [PubMed]
- WHO [World Health Organization]. WHO Guideline on School Health Services. 2021. Available online: https://www.who.int/publications/i/item/9789240029392 (accessed on 13 September 2022).
- Peters, M.D.; Godfrey, C.M.; Khalil, H.; McInerney, P.; Parker, D.; Soares, C.B. Guidance for conducting systematic scoping reviews. Int. J. Evid. -Based Healthc. 2015, 13, 141–146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schiavo, J.H. PROSPERO: An International Register of Systematic Review Protocols. Med. Ref. Serv. Q. 2019, 38, 171–180. [Google Scholar] [CrossRef]
- Nastri, L.; Moretti, A.; Migliaccio, S.; Paoletta, M.; Annunziata, M.; Liguori, S.; Toro, G.; Bianco, M.; Cecoro, G.; Guida, L. Do Dietary Supplements and Nutraceuticals Have Effects on Dental Implant Osseointegration? A Scoping Review. Nutrients 2020, 12, 268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Drikite, L.; Bedford, J.P.; O’Bryan, L.; Petrinic, T.; Rajappan, K.; Doidge, J.; Harrison, D.A.; Rowan, K.M.; Mouncey, P.R.; Young, D.; et al. Treatment strategies for new onset atrial fibrillation in patients treated on an intensive care unit: A systematic scoping review. Crit. Care (Lond. Engl.) 2021, 25, 257. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan-a web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dreyer, G.; Botha, M.H.; Snyman, L.C.; Visser, C.; Burden, R.; Laubscher, N.; Grond, B.; Richter, K.; Becker, P.J.; Harvey, J.; et al. Combining cervical cancer screening for mothers with schoolgirl vaccination during human papillomavirus (HPV) vaccine implementation in South Africa: Results from the VACCS1 and VACCS2 trials. Int. J. Gynecol. Cancer. 2022, 32, 592–598. [Google Scholar] [CrossRef]
- Vermandere, H.; Naanyu, V.; Mabeya, H.; Vanden Broeck, D.; Michielsen, K.; Degomme, O. Determinants of acceptance and subsequent uptake of the HPV vaccine in a cohort in Eldoret, Kenya. PLoS ONE 2014, 9, e109353. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mbulawa, Z.Z.A.; Somdyala, N.I.; Mabunda, S.A.; Williamson, A.L. Effect of Human Papillomavirus (HPV) Education Intervention on HPV Knowledge and Awareness Among High School Learners in Eastern Cape Province of South Africa. J. Cancer Educ. 2021. [Google Scholar] [CrossRef]
- Sadoh, A.E.; Okonkwobo, C.; Nwaneri, D.U.; Ogboghodo, B.C.; Eregiea, C.; Oviawe, O.; Famuyiwa, O. Effect of Peer Education on Knowledge of Human Papilloma Virus and Cervical Cancer among Female Adolescent Students in Benin City, Nigeria. Ann. Glob. Health 2018, 84, 121–128. [Google Scholar] [CrossRef] [Green Version]
- Indracanti, M.; Berhane, N.; Minyamer, T. Factors associated with pre-and post-educational intervention knowledge levels of hpv and cervical cancer among the male and female university students, northwest ethiopia. Cancer Manag. Res. 2021, 13, 7149–7163. [Google Scholar] [CrossRef]
- Baussano, I.; Sayinzoga, F.; Tshomo, U.; Tenet, V.; Vorsters, A.; Heideman, D.A.M.; Gheit, T.; Tommasino, M.; Umulisa, M.C.; Franceschi, S.; et al. Impact of Human Papillomavirus Vaccination, Rwanda and Bhutan. Emerg. Infect. Dis. 2021, 27, 1–9. [Google Scholar] [CrossRef]
- Dreyer, G.; Van Der Merwe, F.H.; Botha, M.H.; Snyman, L.C.; Constant, D.; Visser, C.; Harvey, J. School-based human papillomavirus vaccination: An opportunity to increase knowledge about cervical cancer and improve uptake of screening. S. Afr. Med. J. 2015, 105, 912–916. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ifediora, C.O.; Azuike, E.C. Targeting cervical cancer campaigns on teenage high schoolers in resource-limited economies: Lessons from an intervention study of Nigerian senior secondary school girls. Fam. Pract. 2019, 36, 600–606. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, K.E.; Erio, T.; Baisley, K.; Lees, S.; Watson-Jones, D. The impact of a human papillomavirus (HPV) vaccination campaign on routine primary health service provision and health workers in Tanzania: A controlled before and after study. BMC Health Serv. Res. 2018, 18, 173. [Google Scholar] [CrossRef]
- Botha, M.H.; Van der Merwe, F.H.; Snyman, L.C.; Dreyer, G. The Vaccine and Cervical Cancer Screen (VACCS) project: Acceptance of human papillomavirus vaccination in a school-based programme program in two provinces of South Africa. S. Afr. Med. J. 2015, 105, 40–43. [Google Scholar] [CrossRef] [PubMed]
- Suarez Mora, A.; Madrigal, J.M.; Jordan, L.; Patel, A. Effectiveness of an Educational Intervention to Increase Human Papillomavirus Knowledge in High-Risk Minority Women. J. Low Genit. Tract Dis. 2018, 22, 288–294. [Google Scholar] [CrossRef]
- Cory, L.; Cha, B.; Ellenberg, S.; Bogner, H.R.; Hwang, W.T.; Smith, J.S.; Haggerty, A.; Morgan, M.; Burger, R.; Chu, C. Effects of Educational Interventions on Human Papillomavirus Vaccine Acceptability: A Randomized Controlled Trial. Obstet Gynecol. 2019, 134, 376–384. [Google Scholar] [CrossRef]
- Sitaresmi, M.N.; Rozanti, N.M.; Simangunsong, L.B.; Wahab, A. Improvement of Parent’s awareness, knowledge, perception, and acceptability of human papillomavirus vaccination after a structured-educational intervention. BMC Public Health 2020, 20, 1836. [Google Scholar] [CrossRef] [PubMed]
- AlRadini, F.; El-Sheikh, A.; Bin Jamaan, N.; Hushan, H.; Binhuwaimel, W.; Alhedaithy, F.; Alanzi, S. Prevalence of Over-the-Counter Cosmeceutical Usage and the Impact of a Health Education Intervention in Female Saudi University Students. Clin. Cosmet. Investig. Dermatol. 2021, 14, 1867–1877. [Google Scholar] [CrossRef]
- Rani, U.; Darabaner, E.; Seserman, M.; Bednarczyk, R.A.; Shaw, J. Public Education Interventions and Uptake of Human Papillomavirus Vaccine: A Systematic Review. J. Public Health Manag. Pract. 2022, 28, E307–E315. [Google Scholar] [CrossRef]
- WHO [World Health Organization]. Immunization Coverage: Fact Sheet. 2021, p. 1. Available online: https://www.who.int/news-room/fact-sheets/detail/immunization-coverage (accessed on 18 September 2022).
- Ezeanochie, M.; Olasimbo, P. Awareness and uptake of human papilloma virus vaccines among female secondary school students in Benin City, Nigeria. Afr. Health Sci. 2020, 20, 45–50. [Google Scholar] [CrossRef]
- Jedy-Agba, E.; Joko, W.Y.; Liu, B.; Buziba, N.G.; Borok, M.; Korir, A.; Masamba, L.; Manraj, S.S.; Finesse, A.; Wabinga, H.; et al. Trends in cervical cancer incidence in sub-Saharan Africa. Br. J. Cancer 2020, 123, 148–154. Available online: https://www.nature.com/articles/s41416-020-0831-9 (accessed on 18 September 2022). [CrossRef] [PubMed]
- Kamaraju, S.; Drope, J.; Sankaranarayanan, R.; Shastri, S. Cancer Prevention in Low-Resource Countries: An Overview of the Opportunity. Am. Soc. Clin. Oncol. Educ. Book 2020, 40, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Hamdi, Y.; Abdeljaoued-Tej, I.; Zatchi, A.A.; Abdelhak, S.; Boubaker, S.; Brown, J.S.; Benkahla, A. Cancer in Africa: The Untold Story. Front. Oncol. 2021, 11, 650117. [Google Scholar] [CrossRef] [PubMed]
- Nicol, A.F.; Andrade, C.V.; Russomano, F.B.; Rodrigues, L.L.; Oliveira, N.S.; Provance, D.W., Jr. HPV vaccines: A controversial issue? Braz. J. Med. Biol. Res. 2016, 49, e5060. [Google Scholar] [CrossRef] [Green Version]
- Ko, L.K.; Taylor, V.M.; Mohamed, F.B.; Do, H.H.; Gebeyaw, F.A.; Ibrahim, A.; Ali, A.A.; Winer, R.L. “We brought our culture here with us”: A qualitative study of perceptions of HPV vaccine and vaccine uptake among East African immigrant mothers. Papillomavirus Res. 2019, 7, 21–25. [Google Scholar] [CrossRef]
- Nabirye, J.; Okwi, L.A.; Nuwematsiko, R.; Kiwanuka, G.; Muneza, F.; Kamya, C.; Babirye, J.N. Health system factors influencing uptake of Human Papilloma Virus (HPV) vaccine among adolescent girls 9-15 years in Mbale District, Uganda. BMC Public Health 2020, 20, 171. [Google Scholar] [CrossRef] [Green Version]

| Scheme | Author and Year of Publication | Sample Size | Country | Objectives | Study Design | Type of Intervention | Study Population | Conclusion |
|---|---|---|---|---|---|---|---|---|
| 1 | Dreyer, Botha, Snyman, et al. (2022) [16] | 5137 | South Africa | To evaluate the efficacy of school-based HPV vaccination linked with maternal cervical cancer screening | Intervention study/Cross-sectional observation study | Vaccination Health education Health screening | Primary school pupils and their mothers/female guardians | Parental consent is an important factor in vaccine uptake |
| 2 | Vermandere, Naanyu, Mabeya, et al. (2014) [17] | 287 | Kenya | To survey the acceptability, subsequent uptake and encountered barriers in the context of a pilot HPV vaccination program in Eldoret, Kenya | Longitudinal study | Pilot HPV vaccination program | Older age women | Vaccine uptake is dependent on the availability of correct and hands-on information about HPV vaccination opportunities and safety |
| 3 | Mbulawa, Somdyala, Mabunda and Williamson. (2021) [18] | 2652 | South Africa | To assess HPV infection and associated risks knowledge level among high school students in the Eastern Cape Province of South Africa | Cross-sectional design | Educational intervention | High school students [male and female] | HPV vaccination and CC screening uptake could be encouraged by increasing HPV awareness and knowledge in the community |
| 4 | Sadoh, Okonkwo, Nwaneri, et al. (2018) [19] | 1461 | Nigeria | To determine the effect of peer education on the knowledge of female adolescents about HPV, cervical cancer, its treatment and prevention | Cohort study | Educational intervention Peer training | Female secondary school students | Peer training is an effective tool for advancing knowledge and awareness about HPV and CC |
| 5 | Indracanti, Berhane, and Minyamer. (2021) [20] | 638 | Ethiopia | To understand the factors associated with HPV and cervical cancer knowledge levels among university students before and after an educational intervention | Institutional-based cross-sectional pre- and post-test comparative studies | Theory-based educational intervention | Male and female university students [undergraduate and postgraduate] | Educational intervention is significant in unraveling the burden of HPV and CC |
| 6 | Baussano, Sayinzoga, and Tshomo et al. (2021) [21] | 1198 [Rwanda] 987 [Bhutan] | Rwanda and Bhutan | To assess the impact of catch-up HPV vaccination programs in Rwanda and Bhutan | Repeat surveys | None | Female secondary school students | A catch-up HPV vaccination program with countrywide spread is efficacious in developing a national context |
| 7 | Dreyer, van der Merwe, Botha, et al. (2015) [22] | 777 | South Africa | To measure changes in knowledge and screening uptake when information and screening opportunities were provided | Longitudinal study | Educational intervention Cervical cancer screening Vaccination | Mothers of adolescent HPV vaccine recipients | Through information and screening, adolescent HPV vaccine campaigns can help to control CC in older women |
| 8 | Ifediora and Azuikec (2019) [23] | 432 | Nigeria | To determine the impact of two cervical cancer education techniques | Longitudinal cohort study | Health education | Female, final-year, high school students | The effectiveness and sustainability of knowledge gained from CC awareness campaigns among high school girls depends on their continued engagement with the activities |
| 9 | Gallagher, Erio, Baisley, et al. (2018) [24] | 19 health workers 33 control and 30 intervention health facilities | Tanzania | To determine the impact of the government’s school-based HPV vaccine campaign in Kilimanjaro region on the provision of routine primary health services and staff workload | Retrospective, controlled analysis | HPV vaccination campaigns | Healthcare workers | There was no evidence that the HPV vaccination campaign had negative effects on routine health services |
| 10 | Botha, van der Merwe, Snyman and Dreyer (2015) [25] | 2046 | South Africa | To investigate the acceptance of school-based HPV vaccination, the information provided, methods of obtaining consent and assent, and completion rates achieved | Prospective demonstration study | Health education Vaccination | Primary school girls | HPV vaccination is practical and safe in SA schools |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Amzat, J.; Kanmodi, K.K.; Aminu, K.; Egbedina, E.A. School-Based Interventions on Human Papillomavirus in Africa: A Systematic Scoping Review. Venereology 2023, 2, 43-58. https://doi.org/10.3390/venereology2010004
Amzat J, Kanmodi KK, Aminu K, Egbedina EA. School-Based Interventions on Human Papillomavirus in Africa: A Systematic Scoping Review. Venereology. 2023; 2(1):43-58. https://doi.org/10.3390/venereology2010004
Chicago/Turabian StyleAmzat, Jimoh, Kehinde Kazeem Kanmodi, Kafayat Aminu, and Eyinade Adeduntan Egbedina. 2023. "School-Based Interventions on Human Papillomavirus in Africa: A Systematic Scoping Review" Venereology 2, no. 1: 43-58. https://doi.org/10.3390/venereology2010004