
The Impact and Spillover Effects of HIV Self-Test Technology on HIV Outcomes of the South African Working Class


Abstract
:1. Introduction
2. Material and Methods
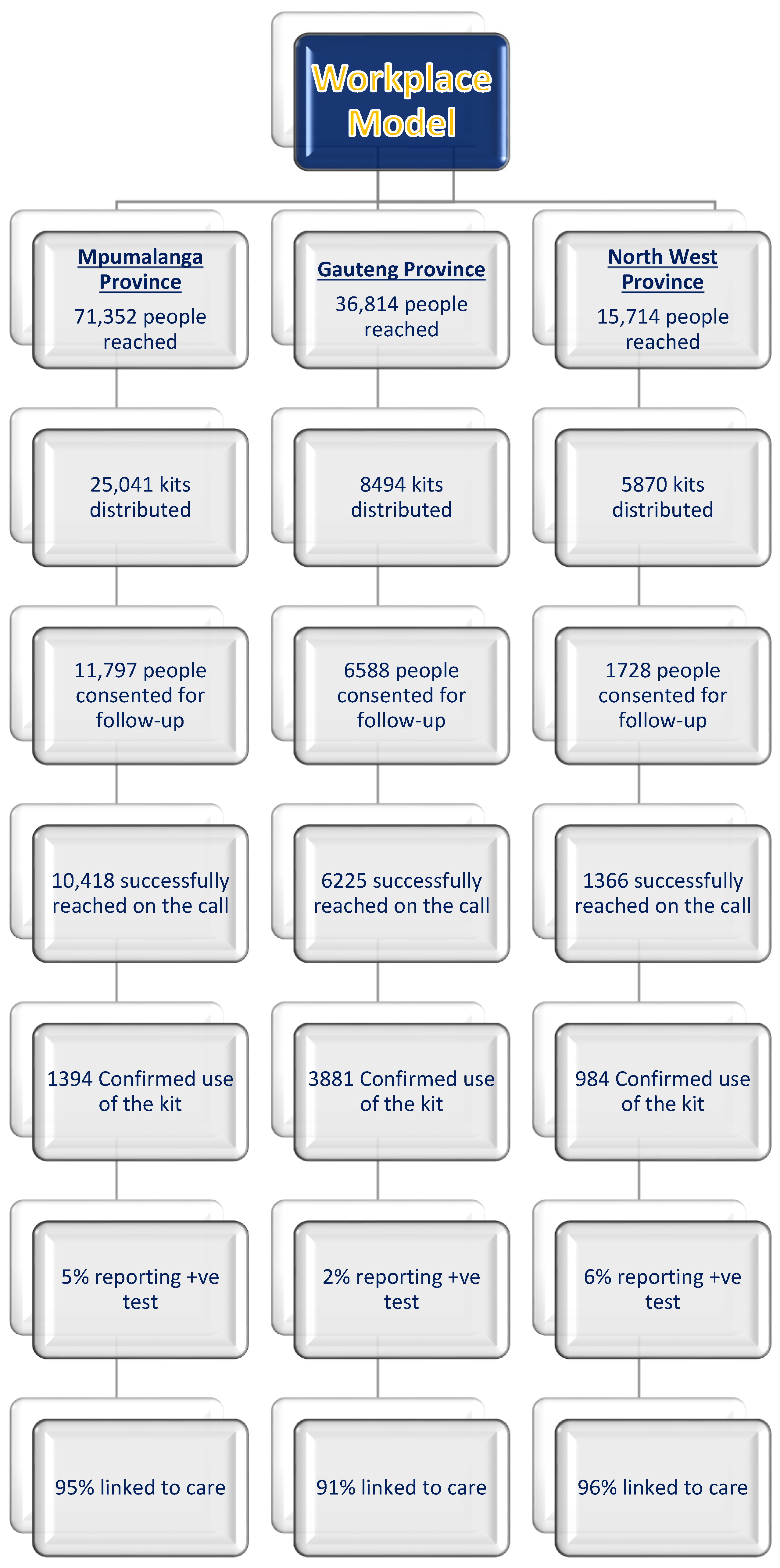
2.1. Workplace HIVST Distribution and Data Collection
- an oral-fluid-based self-testing kit,
- the instruction leaflet,
- a referral card with instructions for further action in the event of a positive screening result,
- a contact number for a representative of the organization distributing the kits.
2.2. Statistical Analysis
3. Results
3.1. Descriptive Analysis
3.2. Results of Two-Stage Least-Squared Model
3.3. Robustness Checks
4. Discussion
Limitations
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lima, V.D.; St-Jean, M.; Rozada, I.; Shoveller, J.A.; Nosyk, B.; Hogg, R.S.; Sereda, P.; Barrios, R.; Montaner, J.S.G. Progress towards the United Nations 90-90-90 and 95-95-95 targets: The experience in British Columbia, Canada. J. Int. AIDS Soc. 2017, 20, e25011. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, J.; Sullivan, P.S.; Curran, J.W. Progress in the HIV epidemic: Identifying goals and measuring success. PLoS Med. 2019, 16, e1002729. [Google Scholar] [CrossRef] [PubMed]
- Barr, D.; Garnett, G.P.; Mayer, K.H.; Morrison, M. Key populations are the future of the African HIV/AIDS pandemic. J. Int. AIDS Soc. 2021, 24, e25750. [Google Scholar] [CrossRef] [PubMed]
- Hatzold, K.; Gudukeya, S.; Mutseta, M.N.; Chilongosi, R.; Nalubamba, M.; Nkhoma, C.; Munkombwe, H.; Munjoma, M.; Mkandawire, P.; Mabhunu, V.; et al. HIV self-testing: Breaking the barriers to uptake of testing among men and adolescents in sub-Saharan Africa, experiences from STAR demonstration projects in Malawi, Zambia and Zimbabwe. J. Int. AIDS Soc. 2019, 22, e25244. [Google Scholar] [CrossRef]
- WHO. Guidelines on HIV Self-Testing and Partner Notification. WHO Publication. 2016. Available online: https://www.who.int/hiv/pub/self-testing/hiv-self-testing-guidelines/en/ (accessed on 9 August 2022).
- Verrall, A.J.; Seah, V.; Lye, D.C.; Leo, Y.S.; Archuleta, S. High specificity of OraQuick® rapid HIV-1/2 antibody testing during dengue infection. J. Clin. Virol. 2020, 131, 104584. [Google Scholar] [CrossRef]
- Siedner, M.J.; Baisley, K.; Koole, O.; Mpofana, I.; Ording-Jespersen, G.; Matthews, P.; Herbst, K.; Smit, T.; Pillay, D. Does antiretroviral therapy use affects the accuracy of HIV rapid diagnostics assays? Experience from a demographic health and surveillance site in rural South Africa. Diagn. Microbiol. Infect. Dis. 2020, 9, 115031. [Google Scholar] [CrossRef]
- Weihs, M.; Meyer-Weitz, A. Barriers to workplace HIV testing in South Africa: A systematic review of the literature. AIDS Care 2016, 28, 495–499. [Google Scholar] [CrossRef]
- Mwisongo, A.; Mohlabane, N.; Tutshana, B.; Peltzer, K. Barriers and facilitators associated with HIV testing uptake in South African health facilities offering HIV Counselling and Testing. Health SA Gesondheid 2016, 21, 86–95. [Google Scholar]
- Mashishi, B.; Makhathini, Z.; Adu-Gyamfi, C. The evolving HIV epidemic and its impact on the HIV testing algorithm: Is it time to change the HIV testing algorithm in South Africa? J. Clin. Virol. 2021, 144, 104990. [Google Scholar] [CrossRef]
- Kelvin, E.A.; George, G.; Kinyanjui, S.; Mwai, E.; Romo, M.L.; Oruko, F.; Odhiambo, J.O.; Nyaga, E.N.; Mantell, J.E.; Govender, K. Announcing the availability of oral HIV self-test kits via text message to increase HIV testing among hard-to-reach truckers in Kenya: A randomized controlled trial. BMC Public Health 2019, 19, 7. [Google Scholar] [CrossRef] [Green Version]
- Shahmanesh, M.; Mthiyane, T.N.; Herbsst, C.; Neuman, M.; Adeagbo, O.; Mee, P.; Chimbindi, N.; Smit, T.; Okesola, N.; Harling, G.; et al. Effect of peer-distributed HIV self-test kits on demand for biomedical HIV prevention in rural KwaZulu-Natal, South Africa: A three-armed cluster-randomised trial comparing social networks versus direct delivery. BMJ Glob. Health 2021, 6, e004574. [Google Scholar] [CrossRef] [PubMed]
- Amstutz, A.; Kopo, M.; Lejone, T.I.; Khesa, L.; Kao, M.; Muhairwe, J.; Glass, T.R.; Labhardt, N.D. “If it is left, it becomes easy for me to get tested”: Use of oral self-tests and community health workers to maximize the potential of home-based HIV testing among adolescents in Lesotho. J. Int. AIDS Soc. 2020, 23, e25563. [Google Scholar] [CrossRef]
- Matsimela, K.; Sande, L.A.; Mostert, C.; Majam, M.; Phiri, J.; Zishiri, V.; Madondo, C.; Khama, S.; Chidarikire, T.; d’Elbée, M.; et al. The cost and intermediary cost-effectiveness of oral HIV self-test kit distribution across 11 distribution models in South Africa. BMJ Glob. Health 2021, 6, e005019. [Google Scholar] [CrossRef] [PubMed]
- Mostert, C.; Vall, C. Long run educational and spill-over effects of cash transfer. Evidence from South Africa. Econ. Hum. Biol. 2020, 36, 100817. [Google Scholar] [CrossRef] [PubMed]
- Mostert, C.M. The impact of national health promotion policy on stillbirth and maternal mortality in South Africa. Public Health 2021, 198, 118–122. [Google Scholar] [CrossRef]
- Mostert, C. The impact of the medical aid schemes on health outcomes of the South African population in the post-apartheid era. J. Community Med. Public Health Care 2021, 8, 92. [Google Scholar] [CrossRef]
- Mostert, C.M. The impact of the school feeding programme on the education and health outcomes of South African children. Child. Youth Serv. Rev. 2021, 126, 106029. [Google Scholar] [CrossRef]
- Ajayi, A.I.; Awopegba, O.E.; Adeagbo, O.A.; Ushie, B.A. Low coverage of HIV testing among adolescents and young adults in Nigeria: Implication for achieving the UNAIDS first 95. PLoS ONE 2020, 15, e0233368. [Google Scholar] [CrossRef]
- Julien, A.; Anthierens, S.; Van Rie, A.; West, R.; Maritze, M.; Twine, R.; Kahn, K.; Lippman, S.A.; Pettifor, A.; Leslie, H.H. Health Care Providers’ Challenges to High-Quality HIV Care and Antiretroviral Treatment Retention in Rural South Africa. Qual. Health Res. 2021, 31, 722–735. [Google Scholar] [CrossRef]
- Hlongwa, M.; Mashamba-Thompson, T.; Makhunga, S.; Hlongwana, K. Barriers to HIV testing uptake among men in sub-Saharan Africa: A scoping review. Afr. J. AIDS Res. 2020, 19, 13–23. [Google Scholar] [CrossRef] [Green Version]
- Hale, B.; Harbertson, J.; Kolou, M.; Sevalie, S.; Cole, R.; Parwon, Z.J.; Merkel, M.O.; Triplett, D.; Wankie, C.; Adams, M.; et al. Reconfirming HIV serostatus in three West African Military ART clinics. J. Clin. Virol. 2021, 141, 104898. [Google Scholar] [CrossRef] [PubMed]
- Pan, P.; Xue, Y.; Gao, J.; Zhu, Q.; Liu, J.; Jiang, Y.; Jin, C. Fifteen years of the proficiency testing program for HIV-1 viral load testing laboratories in China, 2005–2019. J. Clin. Virol. 2021, 142, 104911. [Google Scholar] [CrossRef]
- Hecht, J.; Sanchez, T.; Sullivan, P.S.; DiNenno, E.A.; Cramer, N.; Delaney, K.P. Increasing Access to HIV Testing Through Direct-to-Consumer HIV Self-Test Distribution—United States, March 31, 2020–March 30, 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1322–1325. [Google Scholar] [CrossRef] [PubMed]
- Ryan, S.; Hahn, E.; Rao, A.; Mwinnyaa, G.; Black, J.; Maharaj, R.; Mvandaba, N.; Nyanisa, Y.; Quinn, T.C.; Hansoti, B. The impact of HIV knowledge and attitudes on HIV testing acceptance among patients in an emergency department in the Eastern Cape, South Africa. BMC Public Health 2020, 20, 1066. [Google Scholar] [CrossRef] [PubMed]
- Fields, E.L.; Gayles, T.A. Considerations for Addressing Low HIV Testing Rates among Adolescent Men Who Have Sex with Men. Pediatrics 2020, 145, e20193996. [Google Scholar] [CrossRef] [PubMed]
- He, L.; Pan, X.; Yang, J.; Ma, Q.; Jiang, J.; Wang, W.; Qiu, J.; Zou, Y.; Wang, P.; Zhao, D.; et al. HIV risk behavior and HIV testing among rural and urban men who have sex with men in Zhejiang Province, China: A respondent-driven sampling study. PLoS ONE 2020, 15, e0231026. [Google Scholar] [CrossRef]
- Indravudh, P.P.; Fielding, K.; Kumwenda, M.K.; Nzawa, R.; Chilongosi, R.; Desmond, N.; Nyirenda, R.; Neuman, M.; Johnson, C.C.; Baggaley, R.; et al. Effect of community-led delivery of HIV self-testing on HIV testing and antiretroviral therapy initiation in Malawi: A cluster-randomised trial. PLoS Med. 2020, 18, e1003608. [Google Scholar] [CrossRef]
- MacPherson, P.; Lalloo, D.; Webb, E.; Maheswaran, H.; Choko, A.T.; Makombe, S.D.; Butterworth, A.E.; Van Oosterhout, J.J.; Desmond, N.; Thindwa, D.; et al. Effect of Optional Home Initiation of HIV Care Following HIV Self-testing on Antiretroviral Therapy Initiation Among Adults in Malawi. JAMA 2014, 312, 372–379. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Variable | Treated Cohorts | Control Cohorts |
|---|---|---|
| Reported testing uptake | 55% | 45% |
| Reported testing uptake in males | 56% | 44% |
| Reported testing uptake in females | 54% | 46% |
| Reported testing uptake in urban settings | 52% | 48% |
| Reported testing uptake in rural settings | 56% | 44% |
| Reported ART uptake | 61% | 39% |
| Observations | 3255 | 3004 |
| 2SLS Estimation | Workplace |
|---|---|
| 1st Stage Treatment (infrequent testing cohort) | HIVST Technology 0.097 |
| Standard errors | (0.003) |
| p-value | 0.003 |
| HIVST Technology | Confirmed Testing 0.255 |
| Standard errors | (0.003) |
| p-value | 0.001 |
| Age fix effect | YES |
| Industry fix effect | YES |
| Region fix effect | YES |
| Month fix effect | YES |
| Intensity fix effect | YES |
| Gender fix effect | YES |
| Mean for HIV testing uptake | 0.923 |
| Observations | 6259 |
| F-stat 1st SLS | 151.721 |
| R-squared 2nd SLS | 0.087 |
| 2SLS | Workplace |
|---|---|
| Rural | |
| HIVST Technology | Testing uptake 0.315 |
| Standard errors | (0.004) |
| p-value | 0.002 |
| Urban | |
| HIVST Technology | Testing uptake 0.196 |
| Standard errors | (0.003) |
| p-value | 0.001 |
| Age fix effect | YES |
| Industry fix effect | YES |
| Month fix effect | YES |
| Intensity fix effect | YES |
| Gender fix effect | YES |
| Rural mean for HIV testing uptake | 0.946 |
| Urban mean for HIV testing uptake | 0.900 |
| Observations rural | 3317 |
| Observations urban | 2942 |
| F-stat 1st SLS rural | 95.112 |
| F-stat 1st SLS urban | 88.058 |
| R-squared 2nd SLS rural | 0.077 |
| R-squared 2nd SLS urban | 0.067 |
| 2SLS | Workplace |
|---|---|
| Males | |
| HIVST Technology | HIV testing uptake 0.333 |
| Standard errors | (0.003) |
| p-value | 0.001 |
| Females | |
| HIVST Technology | HIV testing uptake 0.178 |
| Standard errors | (0.005) |
| p-value | 0.003 |
| Age fix effect | YES |
| Industry fix effect | YES |
| Region fix effect | YES |
| Month fix effect | YES |
| Intensity fix effect | YES |
| Males mean for HIV testing uptake | 0.962 |
| Females mean for HIV testing uptake | 0.884 |
| Observations males | 3380 |
| Observations females | 2879 |
| F-stat 1st SLS males | 97.445 |
| F-stat 1st SLS females | 81.549 |
| R-squared 2nd SLS males | 0.078 |
| R-squared 2nd SLS females | 0.071 |
| 2SLS | Workplace |
|---|---|
| HIVST Technology | ART uptake 0.045 |
| Standard errors | (0.021) |
| p-value | 0.002 |
| Age fix effect | YES |
| Industry fix effect | YES |
| Region fix effect | YES |
| Month fix effect | YES |
| Intensity fix effect | YES |
| Gender fix effect | YES |
| Mean for ART uptake | 0.591 |
| Observations | 751 |
| F-stat 1st SLS | 58.627 |
| R-squared 2nd SLS | 0.061 |
| OLS | Workplace |
|---|---|
| Rural | |
| HIVST Technology | Testing uptake 0.537 |
| Standard errors | (0.005) |
| p-value | 0.003 |
| Urban | |
| HIVST Technology | Testing uptake 0.312 |
| Standard errors | (0.004) |
| p-value | 0.001 |
| Age fix effect | YES |
| Industry fix effect | YES |
| Month fix effect | YES |
| Intensity fix effect | YES |
| Gender fix effect | YES |
| Rural mean for HIV testing uptake | 0.946 |
| Urban mean for HIV testing uptake | 0.900 |
| Observations rural | 3317 |
| Observations urban | 2942 |
| OLS | Workplace |
|---|---|
| Males | |
| HIVST Technology | HIV testing uptake 0.556 |
| Standard errors | (0.004) |
| p-value | 0.004 |
| Females | |
| HIVST Technology | HIV testing uptake 0.399 |
| Standard errors | (0.005) |
| p-value | 0.002 |
| Age fix effect | YES |
| Industry fix effect | YES |
| Region fix effect | YES |
| Month fix effect | YES |
| Intensity fix effect | YES |
| Males mean for HIV testing uptake | 0.962 |
| Females mean for HIV testing uptake | 0.884 |
| Observations males | 3380 |
| Observations females | 2879 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mostert, C.M. The Impact and Spillover Effects of HIV Self-Test Technology on HIV Outcomes of the South African Working Class. Venereology 2022, 1, 187-198. https://doi.org/10.3390/venereology1020013
Mostert CM. The Impact and Spillover Effects of HIV Self-Test Technology on HIV Outcomes of the South African Working Class. Venereology. 2022; 1(2):187-198. https://doi.org/10.3390/venereology1020013
Chicago/Turabian StyleMostert, Cyprian M. 2022. "The Impact and Spillover Effects of HIV Self-Test Technology on HIV Outcomes of the South African Working Class" Venereology 1, no. 2: 187-198. https://doi.org/10.3390/venereology1020013