
Phototherapy-Based Treatment for Sexually Transmitted Infections—Shining Light into Unexplored Territory

 , ,
, ,
Abstract
:1. Introduction
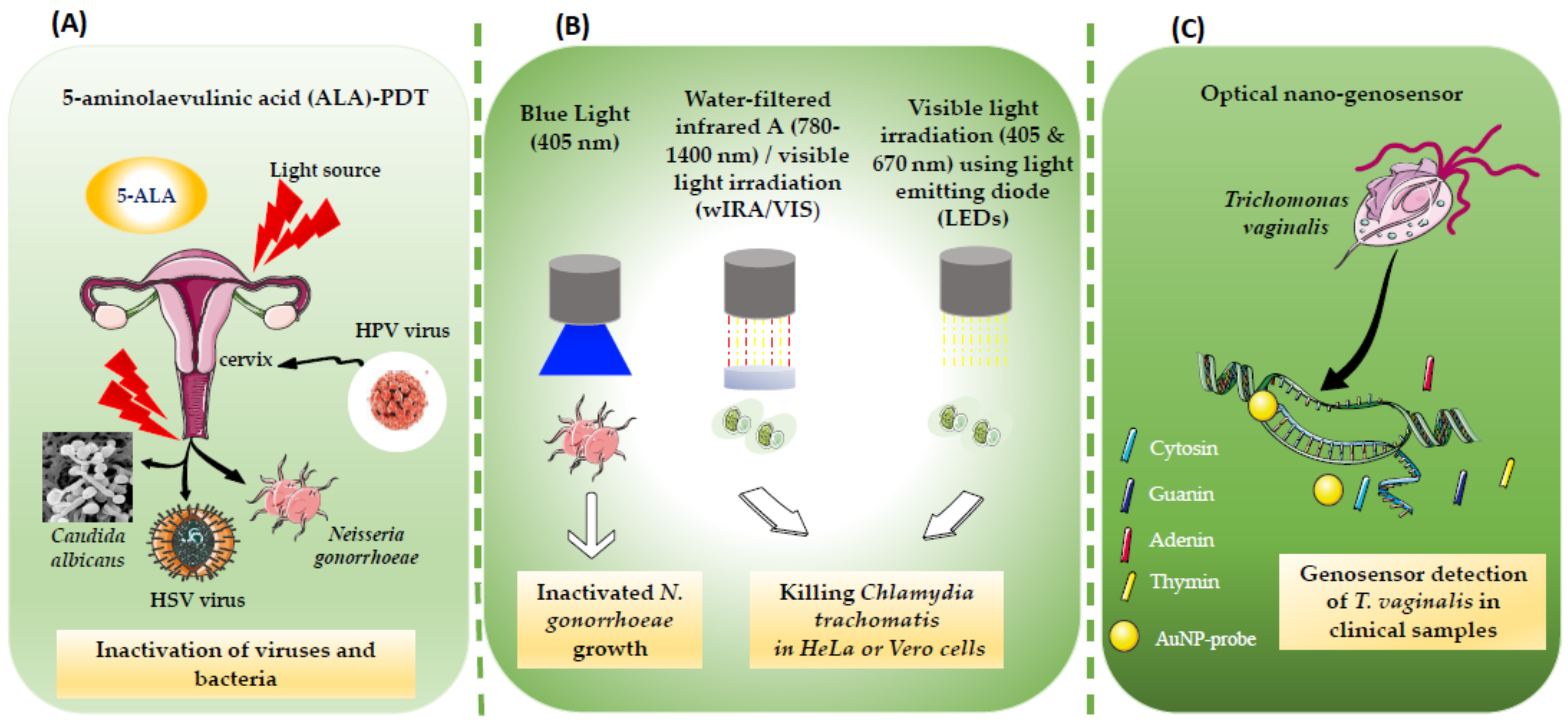
2. PT for Viral STIs
3. PT for Bacterial STIs
4. PT for Parasitic STIs
5. PDT for Fungal STIs
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Sexually Transmitted Infections (STIs). Available online: https://www.who.int/westernpacific/health-topics/sexually-transmitted-infections (accessed on 19 November 2021).
- Williamson, D.A.; Chen, M.Y. Emerging and Reemerging Sexually Transmitted Infections. N. Engl. J. Med. 2020, 382, 2023–2032. [Google Scholar] [CrossRef] [PubMed]
- Smith, L.; Angarone, M.P. Sexually Transmitted Infections. Urol. Clin. N. Am. 2015, 42, 507–518. [Google Scholar] [CrossRef] [PubMed]
- Ciccarese, G.; Herzum, A.; Pastorino, A.; Dezzana, M.; Casazza, S.; Mavilia, M.G.; Copello, F.; Parodi, A.; Drago, F. Prevalence of Genital HPV Infection in STI and Healthy Populations and Risk Factors for Viral Persistence. Eur. J. Clin. Microbiol. Infect. Dis. 2021, 40, 885–888. [Google Scholar] [CrossRef] [PubMed]
- Cole, S. Herpes Simplex Virus: Epidemiology, Diagnosis, and Treatment. Nurs. Clin. N. Am. 2020, 55, 337–345. [Google Scholar] [CrossRef]
- Kardani, K.; Basimi, P.; Fekri, M.; Bolhassani, A. Antiviral Therapy for the Sexually Transmitted Viruses: Recent Updates on Vaccine Development. Expert Rev. Clin. Pharmacol. 2020, 13, 1001–1046. [Google Scholar] [CrossRef]
- Juliana, N.C.A.; Deb, S.; Ouburg, S.; Chauhan, A.; Pleijster, J.; Ali, S.M.; Morré, S.A.; Sazawal, S.; Ambrosino, E. The Prevalence of Chlamydia Trachomatis and Three Other Non-Viral Sexually Transmitted Infections among Pregnant Women in Pemba Island Tanzania. Pathogens 2020, 9, 625. [Google Scholar] [CrossRef]
- Gannon-Loew, K.E.; Holland-Hall, C. A Review of Current Guidelines and Research on the Management of Sexually Transmitted Infections in Adolescents and Young Adults. Ther. Adv. Infect. Dis. 2020, 7, 2049936120960664. [Google Scholar] [CrossRef]
- Doernberg, S.B.; Komarow, L.; Tran, T.T.T.; Sund, Z.; Pandori, M.W.; Jensen, D.; Tsalik, E.L.; Deal, C.D.; Chambers, H.F.; Fowler, V.G.; et al. Simultaneous Evaluation of Diagnostic Assays for Pharyngeal and Rectal Neisseria Gonorrhoeae and Chlamydia Trachomatis Using a Master Protocol. Clin. Infect. Dis. 2020, 71, 2314–2322. [Google Scholar] [CrossRef]
- Yarbrough, M.L.; Burnham, C.-A.D. The ABCs of STIs: An Update on Sexually Transmitted Infections. Clin. Chem. 2016, 62, 811–823. [Google Scholar] [CrossRef] [Green Version]
- Lin, K.-Y.; Sun, H.-Y.; Lee, T.-F.; Chuang, Y.-C.; Wu, U.-I.; Liu, W.-C.; Chang, S.-Y.; Chen, Y.-J.; Hung, C.-C.; Chang, S.-C. High Prevalence of Sexually Transmitted Coinfections among At-Risk People Living with HIV. J. Formos. Med. Assoc. 2021, 120, 1876–1883. [Google Scholar] [CrossRef]
- Tien, V.; Punjabi, C.; Holubar, M.K. Antimicrobial Resistance in Sexually Transmitted Infections. J. Travel. Med. 2020, 27, taz101. [Google Scholar] [CrossRef]
- Williams, E.; Fairley, C.K.; Williamson, D. Novel Strategies for Prevention and Treatment of Antimicrobial Resistance in Sexually-Transmitted Infections. Curr. Opin. Infect. Dis. 2021, 34, 591–598. [Google Scholar] [CrossRef]
- Li, Y.; Yu, T.; Yan, H.; Li, D.; Yu, T.; Yuan, T.; Rahaman, A.; Ali, S.; Abbas, F.; Dian, Z.; et al. Vaginal Microbiota and HPV Infection: Novel Mechanistic Insights and Therapeutic Strategies. Infect. Drug Resist. 2020, 13, 1213–1220. [Google Scholar] [CrossRef]
- Zhang, T.; Hu, R.; Tang, Y.; Zhang, Y.; Qin, L.; Shen, Y.; Wang, B.; Zhang, L.; Cao, L.; Zhou, Y.; et al. The Effect of Local Photodynamic Therapy with 5-Aminolevulinic Acid in the Treatment of Vaginal Intraepithelial Lesions with High-Risk HPV Infection. Photodiagn. Photodyn. Ther. 2022, 37, 102728. [Google Scholar] [CrossRef]
- Fathi, R.; Tsoukas, M.M. Genital Warts and Other HPV Infections: Established and Novel Therapies. Clin. Dermatol. 2014, 32, 299–306. [Google Scholar] [CrossRef]
- Schnürch, H.-G.; Ackermann, S.; Alt-Radtke, C.D.; Angleitner, L.; Barinoff, J.; Beckmann, M.W.; Böing, C.; Dannecker, C.; Fehm, T.; Gaase, R.; et al. Diagnosis, Therapy and Follow-up of Vaginal Cancer and Its Precursors. Guideline of the DGGG and the DKG (S2k-Level, AWMF Registry No. 032/042, October 2018). Geburtshilfe Und Frauenheilkd. 2019, 79, 1060–1078. [Google Scholar] [CrossRef] [Green Version]
- Chumworathayi, B.; Thinkhamrop, J.; Blumenthal, P.D.; Thinkhamrop, B.; Pientong, C.; Ekalaksananan, T. Cryotherapy for HPV Clearance in Women with Biopsy-Confirmed Cervical Low-Grade Squamous Intraepithelial Lesions. Int. J. Gynaecol. Obstet. 2010, 108, 119–122. [Google Scholar] [CrossRef]
- Afanasiev, M.D.D.S.M.S.; Dushkin, M.D.A.D.; Grishacheva, D.S.T.G.; Afanasiev, M.D.D.S.S.S.; Karaulov Academician Ras, M.D.D.S.A.V. Photodynamic Therapy for Early-Stage Cervical Cancer Treatment. Photodiagn. Photodyn. Ther. 2021, 37, 102620. [Google Scholar] [CrossRef]
- Viviano, M.; Kenfack, B.; Catarino, R.; Tincho, E.; Temogne, L.; Benski, A.-C.; Tebeu, P.-M.; Meyer-Hamme, U.; Vassilakos, P.; Petignat, P. Feasibility of Thermocoagulation in a Screen-and-Treat Approach for the Treatment of Cervical Precancerous Lesions in Sub-Saharan Africa. BMC Womens Health 2017, 17, 2. [Google Scholar] [CrossRef] [Green Version]
- Gutierrez, P.; Garza, J.; Gandhi, K.; Voice, A.; Stout, E.; Ventolini, G. Carbon Dioxide (CO2) Laser Ablation Treatment of a Peri-Urethral Genital Wart: A Case Report. Case Rep. Womens Health 2020, 27, e00226. [Google Scholar] [CrossRef]
- Cosper, P.F.; McNair, C.; González, I.; Wong, N.; Knudsen, K.E.; Chen, J.J.; Markovina, S.; Schwarz, J.K.; Grigsby, P.W.; Wang, X. Decreased Local Immune Response and Retained HPV Gene Expression during Chemoradiotherapy Are Associated with Treatment Resistance and Death from Cervical Cancer. Int. J. Cancer 2020, 146, 2047–2058. [Google Scholar] [CrossRef]
- Foster, C.C.; Lee, A.Y.; Furtado, L.V.; Hart, J.; Alpert, L.; Xiao, S.-Y.; Hyman, N.H.; Sharma, M.R.; Liauw, S.L. Treatment Outcomes and HPV Characteristics for an Institutional Cohort of Patients with Anal Cancer Receiving Concurrent Chemotherapy and Intensity-Modulated Radiation Therapy. PLoS ONE 2018, 13, e0194234. [Google Scholar] [CrossRef]
- Chera, B.S.; Amdur, R.J.; Green, R.; Shen, C.; Gupta, G.; Tan, X.; Knowles, M.; Fried, D.; Hayes, N.; Weiss, J.; et al. Phase II Trial of De-Intensified Chemoradiotherapy for Human Papillomavirus-Associated Oropharyngeal Squamous Cell Carcinoma. J. Clin. Oncol. 2019, 37, 2661–2669. [Google Scholar] [CrossRef]
- Sindhu, S.K.; Bauman, J.E. Current Concepts in Chemotherapy for Head and Neck Cancer. Oral. Maxillofac. Surg. Clin. N. Am. 2019, 31, 145–154. [Google Scholar] [CrossRef]
- Bonomi, M.; Ahmed, T.; Warner, D.; Waltonen, J.; Sullivan, C.; Porosnicu, M.; Batt, K.; Ruiz, J.; Cappellari, J. Human Papillomavirus-Related Small Cell Carcinoma of the Oropharynx: A Case Report and Literature Review. Cancers Head Neck 2017, 2, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perrone, A.M.; Tesei, M.; Ferioli, M.; De Terlizzi, F.; Della Gatta, A.N.; Boussedra, S.; Dondi, G.; Galuppi, A.; Morganti, A.G.; De Iaco, P. Results of a Phase I-II Study on Laser Therapy for Vaginal Side Effects after Radiotherapy for Cancer of Uterine Cervix or Endometrium. Cancers 2020, 12, 1639. [Google Scholar] [CrossRef] [PubMed]
- Bogani, G.; Ditto, A.; Martinelli, F.; Mosca, L.; Chiappa, V.; Rossetti, D.; Leone Roberti Maggiore, U.; Sabatucci, I.; Lorusso, D.; Raspagliesi, F. LASER Treatment for Women with High-Grade Vaginal Intraepithelial Neoplasia: A Propensity-Matched Analysis on the Efficacy of Ablative versus Excisional Procedures. Lasers Surg. Med. 2018, 50, 933–939. [Google Scholar] [CrossRef] [PubMed]
- Boonlikit, S. Recurrence of High-Grade Vaginal Intraepithelial Neoplasia after Various Treatments. Curr. Probl. Cancer 2022, 46, 100792. [Google Scholar] [CrossRef] [PubMed]
- Farmer, E.; Cheng, M.A.; Hung, C.-F.; Wu, T.-C. Vaccination Strategies for the Control and Treatment of HPV Infection and HPV-Associated Cancer. Recent Results Cancer Res. 2021, 217, 157–195. [Google Scholar] [CrossRef]
- Dadar, M.; Chakraborty, S.; Dhama, K.; Prasad, M.; Khandia, R.; Hassan, S.; Munjal, A.; Tiwari, R.; Karthik, K.; Kumar, D.; et al. Advances in Designing and Developing Vaccines, Drugs and Therapeutic Approaches to Counter Human Papilloma Virus. Front. Immunol. 2018, 9, 2478. [Google Scholar] [CrossRef]
- Taylor, M.; Gerriets, V. Acyclovir. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Feng, E.; Balint, E.; Vahedi, F.; Ashkar, A.A. Immunoregulatory Functions of Interferons during Genital HSV-2 Infection. Front. Immunol. 2021, 12, 724618. [Google Scholar] [CrossRef]
- Lau, A.; Kong, F.Y.S.; Fairley, C.K.; Templeton, D.J.; Amin, J.; Phillips, S.; Law, M.; Chen, M.Y.; Bradshaw, C.S.; Donovan, B.; et al. Azithromycin or Doxycycline for Asymptomatic Rectal Chlamydia Trachomatis. N. Engl. J. Med. 2021, 384, 2418–2427. [Google Scholar] [CrossRef]
- Zofkie, A.C.; Fomina, Y.Y.; Roberts, S.W.; McIntire, D.D.; Nelson, D.B.; Adhikari, E.H. Effectiveness of Chlamydia Trachomatis Expedited Partner Therapy in Pregnancy. Am. J. Obstet. Gynecol. 2021, 225, 325.e1–325.e7. [Google Scholar] [CrossRef]
- Adachi, K.N.; Nielsen-Saines, K.; Klausner, J.D. Chlamydia Trachomatis Screening and Treatment in Pregnancy to Reduce Adverse Pregnancy and Neonatal Outcomes: A Review. Front. Public Health 2021, 9, 531073. [Google Scholar] [CrossRef]
- Gnanadurai, R.; Fifer, H. Mycoplasma Genitalium: A Review. Microbiology 2020, 166, 21–29. [Google Scholar] [CrossRef]
- Unemo, M.; Lahra, M.M.; Cole, M.; Galarza, P.; Ndowa, F.; Martin, I.; Dillon, J.-A.R.; Ramon-Pardo, P.; Bolan, G.; Wi, T. World Health Organization Global Gonococcal Antimicrobial Surveillance Program (WHO GASP): Review of New Data and Evidence to Inform International Collaborative Actions and Research Efforts. Sex. Health 2019, 16, 412–425. [Google Scholar] [CrossRef] [Green Version]
- Poncin, T.; Fouere, S.; Braille, A.; Camelena, F.; Agsous, M.; Bebear, C.; Kumanski, S.; Lot, F.; Mercier-Delarue, S.; Ngangro, N.N.; et al. Multidrug-Resistant Neisseria Gonorrhoeae Failing Treatment with Ceftriaxone and Doxycycline in France, November 2017. Eurosurveillance 2018, 23, 1800264. [Google Scholar] [CrossRef]
- Salmerón, P.; Viñado, B.; Arando, M.; Alcoceba, E.; Romero, B.; Menéndez, B.; Bernal, S.; Idigoras, P.; Colomina, J.; Martin-Saco, G.; et al. Neisseria Gonorrhoeae Antimicrobial Resistance in Spain: A Prospective Multicentre Study. J. Antimicrob. Chemother. 2021, 76, 1523–1531. [Google Scholar] [CrossRef]
- Bouchemal, K.; Bories, C.; Loiseau, P.M. Strategies for Prevention and Treatment of Trichomonas Vaginalis Infections. Clin. Microbiol. Rev. 2017, 30, 811–825. [Google Scholar] [CrossRef] [Green Version]
- Graves, K.J.; Novak, J.; Secor, W.E.; Kissinger, P.J.; Schwebke, J.R.; Muzny, C.A. A Systematic Review of the Literature on Mechanisms of 5-Nitroimidazole Resistance in Trichomonas Vaginalis. Parasitology 2020, 147, 1383–1391. [Google Scholar] [CrossRef]
- Lam, S. Photodynamic Therapy of Lung Cancer. Semin. Oncol. 1994, 21, 15–19. [Google Scholar] [CrossRef] [Green Version]
- Kessel, D. Photodynamic Therapy: Critical PDT Theory. Photochem. Photobiol. 2022. [Google Scholar] [CrossRef]
- Dougherty, T.J. Hematoporphyrin Derivative for Detection and Treatment of Cancer. J. Surg. Oncol. 1980, 15, 209–210. [Google Scholar] [CrossRef]
- Kou, J.; Dou, D.; Yang, L. Porphyrin Photosensitizers in Photodynamic Therapy and Its Applications. Oncotarget 2017, 8, 81591–81603. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.; Jiang, C.; Figueiró Longo, J.P.; Azevedo, R.B.; Zhang, H.; Muehlmann, L.A. An Updated Overview on the Development of New Photosensitizers for Anticancer Photodynamic Therapy. Acta. Pharm. Sin. B 2018, 8, 137–146. [Google Scholar] [CrossRef]
- Bellnier, D.A.; Greco, W.R.; Loewen, G.M.; Nava, H.; Oseroff, A.R.; Dougherty, T.J. Clinical Pharmacokinetics of the PDT Photosensitizers Porfimer Sodium (Photofrin), 2-[1-Hexyloxyethyl]-2-Devinyl Pyropheophorbide-a (Photochlor) and 5-ALA-Induced Protoporphyrin IX. Lasers Surg. Med. 2006, 38, 439–444. [Google Scholar] [CrossRef]
- Mfouo-Tynga, I.S.; Dias, L.D.; Inada, N.M.; Kurachi, C. Features of Third Generation Photosensitizers Used in Anticancer Photodynamic Therapy: Review. Photodiagn. Photodyn. Ther. 2021, 34, 102091. [Google Scholar] [CrossRef]
- Kharkwal, G.B.; Sharma, S.K.; Huang, Y.-Y.; Dai, T.; Hamblin, M.R. Photodynamic Therapy for Infections: Clinical Applications. Lasers Surg. Med. 2011, 43, 755–767. [Google Scholar] [CrossRef] [Green Version]
- Kombe Kombe, A.J.; Li, B.; Zahid, A.; Mengist, H.M.; Bounda, G.-A.; Zhou, Y.; Jin, T. Epidemiology and Burden of Human Papillomavirus and Related Diseases, Molecular Pathogenesis, and Vaccine Evaluation. Front. Public Health 2020, 8, 552028. [Google Scholar] [CrossRef]
- De Sanjosé, S.; Diaz, M.; Castellsagué, X.; Clifford, G.; Bruni, L.; Muñoz, N.; Bosch, F.X. Worldwide Prevalence and Genotype Distribution of Cervical Human Papillomavirus DNA in Women with Normal Cytology: A Meta-Analysis. Lancet Infect. Dis. 2007, 7, 453–459. [Google Scholar] [CrossRef]
- Pennycook, K.B.; McCready, T.A. Condyloma Acuminata. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Hu, Z.; Zheng, H.; Zeng, K. Patterns of Multiple Human Papillomavirus Clearance during 5-Aminolevulinic Acid-Based Photodynamic Therapy in Patients with Genital Warts. Photodiagn. Photodyn. Ther. 2021, 35, 102454. [Google Scholar] [CrossRef] [PubMed]
- Yin, G.; Zhang, Y.; Geng, M.; Cai, B.; Zheng, Y. Cure of Condyloma Acuminata Covering the Glans Penis Using Aminolevulinic Acid/Photodynamic Therapy. Photodiagn. Photodyn. Ther. 2020, 30, 101658. [Google Scholar] [CrossRef] [PubMed]
- Inada, N.M.; Buzza, H.H.; Carbinatto, F.M.; Blanco, K.C.; de Andrade, C.T.; Vollet-Filho, J.D.; Bagnato, V.S.; Allison, R.R. Optical Techniques for the Diagnosis and Treatment of Lesions Induced by the Human Papillomavirus—A Resource Letter. Photodiagn. Photodyn. Ther. 2018, 23, 106–110. [Google Scholar] [CrossRef] [PubMed]
- Owczarek, W.; Slowinska, M.; Walecka, I.; Ciazynska, M.; Nowicka, D.; Walczak, L.; Paluchowska, E. Correlation of the ALA-PDT Treatment Efficacy and the HPV Genotype Profile of Genital Warts after Cryotherapy Failure and Podophyllotoxin Therapy in Male Patients. Life 2021, 11, 146. [Google Scholar] [CrossRef]
- Kechichian, E.; Helou, E.; Sarkis, J.; Hayek, C.; Labaki, C.; Nemr, E.; Tomb, R. The Place of 5-Aminolaevulinic Acid-Photodynamic Therapy in the Treatment Landscape of Urethral Warts: A Systematic Review. Photodiagn. Photodyn. Ther. 2021, 33, 102204. [Google Scholar] [CrossRef]
- Stern, P.L.; van der Burg, S.H.; Hampson, I.N.; Broker, T.R.; Fiander, A.; Lacey, C.J.; Kitchener, H.C.; Einstein, M.H. Therapy of Human Papillomavirus-Related Disease. Vaccine 2012, 30 (Suppl. S5), F71–F82. [Google Scholar] [CrossRef] [Green Version]
- Mistrangelo, M.; Dal Conte, I.; Volpatto, S.; DI Benedetto, G.; Testa, V.; Currado, F.; Morino, M. Current Treatments for Anal Condylomata Acuminata. Minerva Chir. 2018, 73, 100–106. [Google Scholar] [CrossRef]
- Hu, Z.; Zheng, H.; Zeng, K. Predictors of Human Papillomavirus Persistence or Clearance after 5-Aminolevulinic Acid-Based Photodynamic Therapy in Patients with Genital Warts. Photodiagn. Photodyn. Ther. 2021, 35, 102431. [Google Scholar] [CrossRef]
- Xie, J.; Ao, C.; Li, J.; Jiang, L.; Liu, H.; Zeng, K. 5-Aminolevulinic Acid Photodynamic Therapy for Condyloma Acuminatum of Urethral Meatus. J. Dermatolog. Treat. 2019, 30, 714–717. [Google Scholar] [CrossRef]
- Buzzá, H.H.; Stringasci, M.D.; de Arruda, S.S.; Crestana, R.H.S.; de Castro, C.A.; Bagnato, V.S.; Inada, N.M. HPV-Induced Condylomata Acuminata Treated by Photodynamic Therapy in Comparison with Trichloroacetic Acid: A Randomized Clinical Trial. Photodiagn. Photodyn. Ther. 2021, 35, 102465. [Google Scholar] [CrossRef]
- Hu, S.; Yang, Y.; Jiang, B.; Su, D.; Zhang, L.; Huang, Z.; Zhang, F. Treatment of Condyloma Acuminatum Using the Combination of Laser Ablation and ALA-PDT. Photodiagn. Photodyn. Ther. 2019, 25, 193–196. [Google Scholar] [CrossRef]
- Shi, H.; Zhang, X.; Ma, C.; Yu, N.; Wang, J.; Xia, L.; Ge, X.; Liu, M.; Duan, A. Clinical Analysis of Five Methods Used to Treat Condylomata Acuminata. Dermatology 2013, 227, 338–345. [Google Scholar] [CrossRef]
- Szeimies, R.-M.; Schleyer, V.; Moll, I.; Stocker, M.; Landthaler, M.; Karrer, S. Adjuvant Photodynamic Therapy Does Not Prevent Recurrence of Condylomata Acuminata after Carbon Dioxide Laser Ablation-A Phase III, Prospective, Randomized, Bicentric, Double-Blind Study. Dermatol. Surg. 2009, 35, 757–764. [Google Scholar] [CrossRef]
- Kim, J.-H.; Kim, J.; Kim, K.; No, J.H.; Kim, Y.B.; Suh, D.H. Risk Factor and Treatment of Vaginal Intraepithelial Neoplasia After Hysterectomy for Cervical Intraepithelial Neoplasia. J. Low Genit. Tract. Dis. 2022, 26, 147–151. [Google Scholar] [CrossRef]
- Hampson, L.; Martin-Hirsch, P.; Hampson, I.N. An Overview of Early Investigational Drugs for the Treatment of Human Papilloma Virus Infection and Associated Dysplasia. Expert. Opin. Investig. Drugs 2015, 24, 1529–1537. [Google Scholar] [CrossRef]
- Zhang, W.; Zhang, A.; Sun, W.; Yue, Y.; Li, H. Efficacy and Safety of Photodynamic Therapy for Cervical Intraepithelial Neoplasia and Human Papilloma Virus Infection. Medicine 2018, 97, e10864. [Google Scholar] [CrossRef]
- Tao, X.H.; Guan, Y.; Shao, D.; Xue, W.; Ye, F.S.; Wang, M.; He, M.H. Efficacy and Safety of Photodynamic Therapy for Cervical Intraepithelial Neoplasia: A Systemic Review. Photodiagn. Photodyn. Ther. 2014, 11, 104–112. [Google Scholar] [CrossRef]
- Bodner, K.; Bodner-Adler, B.; Wierrani, F.; Kubin, A.; Szölts-Szölts, J.; Spängler, B.; Grünberger, W. Cold-Knife Conization versus Photodynamic Therapy with Topical 5-Aminolevulinic Acid (5-ALA) in Cervical Intraepithelial Neoplasia (CIN) II with Associated Human Papillomavirus Infection: A Comparison of Preliminary Results. Anticancer. Res. 2003, 23, 1785–1788. [Google Scholar]
- Wang, J.; Xu, J.; Chen, J.; He, Q.; Xiang, L.; Huang, X.; Ding, G.; Xu, S. Successful Photodynamic Therapy with Topical 5-Aminolevulinic Acid for Five Cases of Cervical Intraepithelial Neoplasia. Arch. Gynecol. Obstet. 2010, 282, 307–312. [Google Scholar] [CrossRef]
- Li, D.; Zhang, F.; Shi, L.; Lin, L.; Cai, Q.; Xu, Y. Treatment of HPV Infection-Associated Low Grade Cervical Intraepithelial Neoplasia with 5-Aminolevulinic Acid-Mediated Photodynamic Therapy. Photodiagn. Photodyn. Ther. 2020, 32, 101974. [Google Scholar] [CrossRef]
- Cang, W.; Gu, L.; Hong, Z.; Wu, A.; Di, W.; Qiu, L. Effectiveness of Photodynamic Therapy with 5-Aminolevulinic Acid on HPV Clearance in Women without Cervical Lesions. Photodiagn. Photodyn. Ther. 2021, 34, 102293. [Google Scholar] [CrossRef] [PubMed]
- Wu, A.; Li, Q.; Ling, J.; Gu, L.; Hong, Z.; Di, W.; Qiu, L. Effectiveness of Photodynamic Therapy in Women of Reproductive Age with Cervical High-Grade Squamous Intraepithelial Lesions (HSIL/CIN2). Photodiagn. Photodyn. Ther. 2021, 36, 102517. [Google Scholar] [CrossRef] [PubMed]
- Su, Y.; Zhang, Y.; Tong, Y.; Zhang, L.; Li, P.; Zhang, H.; Zhang, X.; Tang, Y.; Qin, L.; Shen, Y.; et al. Effect and Rational Application of Topical Photodynamic Therapy (PDT) with 5-Aminolevulinic Acid (5-ALA) for Treatment of Cervical Intraepithelial Neoplasia with Vaginal Intraepithelial Neoplasia. Photodiagn. Photodyn. Ther. 2022, 37, 102634. [Google Scholar] [CrossRef] [PubMed]
- Herpes Simplex Virus. Available online: https://www.who.int/news-room/fact-sheets/detail/herpes-simplex-virus (accessed on 26 November 2021).
- Fisman, D.N. Health Related Quality of Life in Genital Herpes: A Pilot Comparison of Measures. Sex. Transm. Infect. 2005, 81, 267–270. [Google Scholar] [CrossRef] [Green Version]
- Makarov, O.V.; Khashukaeva, A.Z.; Svitich, O.A.; Markova, È.A.; Khlynova, S.A.; Labzhinov, P.A.; Zverev, V.V. Anti-herpetic effect of photodynamic action in an in vitro experiment. Zhurnal Mikrobiol. Epidemiol. Immunobiol. 2014, 1, 48–55. [Google Scholar]
- Osiecka, B.J.; Nockowski, P.; Kwiatkowski, S.; Szepietowski, J.C. Photodynamic Therapy with Red Light and 5-Aminolaevulinic Acid for Herpes Simplex Recurrence: Preliminary Results. Acta. Derm. Venereol. 2017, 97, 1239–1240. [Google Scholar] [CrossRef] [Green Version]
- Donnarumma, G.; De Gregorio, V.; Fusco, A.; Farina, E.; Baroni, A.; Esposito, V.; Contaldo, M.; Petruzzi, M.; Pannone, G.; Serpico, R. Inhibition of HSV-1 Replication by Laser Diode-Irradiation: Possible Mechanism of Action. Int. J. Immunopathol. Pharmacol. 2010, 23, 1167–1176. [Google Scholar] [CrossRef]
- Ferreira, D.C.; Reis, H.L.B.; Cavalcante, F.S.; Santos, K.R.N.D.; Passos, M.R.L. Recurrent Herpes Simplex Infections: Laser Therapy as a Potential Tool for Long-Term Successful Treatment. Rev. Soc. Bras. Med. Trop. 2011, 44, 397–399. [Google Scholar] [CrossRef]
- Davis, E.C.; Callender, V.D. Postinflammatory Hyperpigmentation. J. Clin. Aesthet. Dermatol. 2010, 3, 20–31. [Google Scholar]
- Preissig, J.; Hamilton, K.; Markus, R. Current Laser Resurfacing Technologies: A Review That Delves Beneath the Surface. Semin. Plast. Surg. 2012, 26, 109–116. [Google Scholar] [CrossRef] [Green Version]
- Kaufman, B.P.; Aman, T.; Alexis, A.F. Postinflammatory Hyperpigmentation: Epidemiology, Clinical Presentation, Pathogenesis and Treatment. Am. J. Clin. Dermatol. 2018, 19, 489–503. [Google Scholar] [CrossRef]
- Barrett, T.; de Zwaan, S. Picosecond Alexandrite Laser Is Superior to Q-Switched Nd:YAG Laser in Treatment of Minocycline-Induced Hyperpigmentation: A Case Study and Review of the Literature. J. Cosmet. Laser Ther. 2018, 20, 387–390. [Google Scholar] [CrossRef]
- Wang, J.V.; Christman, M.P.; Feng, H.; Ferzli, G.; Jeon, H.; Geronemus, R.G. Laser-Assisted Delivery of Tranexamic Acid for Melasma: Pilot Study Using a Novel 1927 Nm Fractional Thulium Fiber Laser. J. Cosmet. Dermatol. 2021, 20, 105–109. [Google Scholar] [CrossRef]
- Unemo, M.; Ross, J.; Serwin, A.B.; Gomberg, M.; Cusini, M.; Jensen, J.S. Background Review for the “2020 European Guideline for the Diagnosis and Treatment of Gonorrhoea in Adults”. Int. J. STD AIDS 2021, 32, 108–126. [Google Scholar] [CrossRef]
- Klausner, J.D.; Bristow, C.C.; Soge, O.O.; Shahkolahi, A.; Waymer, T.; Bolan, R.K.; Philip, S.S.; Asbel, L.E.; Taylor, S.N.; Mena, L.A.; et al. Resistance-Guided Treatment of Gonorrhea: A Prospective Clinical Study. Clin. Infect. Dis. 2021, 73, 298–303. [Google Scholar] [CrossRef]
- Wang, Y.; Ferrer-Espada, R.; Baglo, Y.; Goh, X.S.; Held, K.D.; Grad, Y.H.; Gu, Y.; Gelfand, J.A.; Dai, T. Photoinactivation of Neisseria Gonorrhoeae: A Paradigm-Changing Approach for Combating Antibiotic-Resistant Gonococcal Infection. J. Infect. Dis. 2019, 220, 873–881. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Ferrer-Espada, R.; Gu, Y.; Dai, T. Antimicrobial Blue Light: An Alternative Therapeutic for Multidrug-Resistant Gonococcal Infections? MOJ Sol. Photoenergy Syst. 2017, 1, 00009. [Google Scholar] [CrossRef]
- Marti, H.; Koschwanez, M.; Pesch, T.; Blenn, C.; Borel, N. Water-Filtered Infrared a Irradiation in Combination with Visible Light Inhibits Acute Chlamydial Infection. PLoS ONE 2014, 9, e102239. [Google Scholar] [CrossRef] [Green Version]
- Wasson, C.J.; Zourelias, J.L.; Aardsma, N.A.; Eells, J.T.; Ganger, M.T.; Schober, J.M.; Skwor, T.A. Inhibitory Effects of 405 Nm Irradiation on Chlamydia Trachomatis Growth and Characterization of the Ensuing Inflammatory Response in HeLa Cells. BMC Microbiol. 2012, 12, 176. [Google Scholar] [CrossRef] [Green Version]
- Kissinger, P. Trichomonas Vaginalis: A Review of Epidemiologic, Clinical and Treatment Issues. BMC Infect. Dis. 2015, 15, 307. [Google Scholar] [CrossRef] [Green Version]
- Ilbeigi, S.; Dehdari Vais, R.; Sattarahmady, N. Photo-Genosensor for Trichomonas Vaginalis Based on Gold Nanoparticles-Genomic DNA. Photodiagn. Photodyn. Ther. 2021, 34, 102290. [Google Scholar] [CrossRef]
- Silva Fonseca, T.H.; Alacoque, M.; Silva Oliveira, F.M.; Soares, B.M.; Leite, H.V.; Caliari, M.V.; Gomes, M.A.; Busatti, H. Photodynamic Therapy as a New Approach to Trichomonas Vaginalis Inactivation. Photodiagn. Photodyn. Ther. 2018, 22, 91–95. [Google Scholar] [CrossRef]
- Du, M.; Xuan, W.; Zhen, X.; He, L.; Lan, L.; Yang, S.; Wu, N.; Qin, J.; Zhao, R.; Qin, J.; et al. Antimicrobial Photodynamic Therapy for Oral Candida Infection in Adult AIDS Patients: A Pilot Clinical Trial. Photodiagn. Photodyn. Ther. 2021, 34, 102310. [Google Scholar] [CrossRef]
- Pinto, M.V.M.; Baron, M.; Corrêa, M.; Berton, J.; de Mattos, C.O.C.; Pieczaki, M.; Ronis, A.; Fortuny, E.; Padilha, M.R. Use of the Scar Acceleration Method—Mac® in the Treatment of Vulvovaginal Candidiasis: A Proposal for Treatment in Public Health in Sus, Brazil. Open J. Appl. Sci. 2020, 10, 758–765. [Google Scholar] [CrossRef]
- Wang, T.; Dong, J.; Yin, H.; Zhang, G. Blue Light Therapy to Treat Candida Vaginitis with Comparisons of Three Wavelengths: An in Vitro Study. Lasers Med. Sci. 2020, 35, 1329–1339. [Google Scholar] [CrossRef]
- De Santi, M.E.S.O.; Prates, R.A.; França, C.M.; Lopes, R.G.; Sousa, A.S.; Ferreira, L.R.; Bussadori, S.K.; Fernandes, A.U.; Deana, A.M. Antimicrobial Photodynamic Therapy as a New Approach for the Treatment of Vulvovaginal Candidiasis: Preliminary Results. Lasers Med. Sci. 2018, 33, 1925–1931. [Google Scholar] [CrossRef]
- Machado-de-Sena, R.M.; Corrêa, L.; Kato, I.T.; Prates, R.A.; Senna, A.M.; Santos, C.C.; Picanço, D.A.; Ribeiro, M.S. Photodynamic Therapy Has Antifungal Effect and Reduces Inflammatory Signals in Candida Albicans-Induced Murine Vaginitis. Photodiagn. Photodyn. Ther. 2014, 11, 275–282. [Google Scholar] [CrossRef]
- Ichimura, H.; Yamaguchi, S.; Kojima, A.; Tanaka, T.; Niiya, K.; Takemori, M.; Hasegawa, K.; Nishimura, R. Eradication and Reinfection of Human Papillomavirus after Photodynamic Therapy for Cervical Intraepithelial Neoplasia. Int. J. Clin. Oncol. 2003, 8, 322–325. [Google Scholar] [CrossRef]
- Wierrani, F.; Kubin, A.; Jindra, R.; Henry, M.; Gharehbaghi, K.; Grin, W.; Söltz-Szötz, J.; Alth, G.; Grünberger, W. 5-Aminolevulinic Acid-Mediated Photodynamic Therapy of Intraepithelial Neoplasia and Human Papillomavirus of the Uterine Cervix—A New Experimental Approach. Cancer Detect. Prev. 1999, 23, 351–355. [Google Scholar] [CrossRef]
- Soergel, P.; Wang, X.; Stepp, H.; Hertel, H.; Hillemanns, P. Photodynamic Therapy of Cervical Intraepithelial Neoplasia with Hexaminolevulinate. Lasers Surg. Med. 2008, 40, 611–615. [Google Scholar] [CrossRef]
- Yamaguchi, S.; Tsuda, H.; Takemori, M.; Nakata, S.; Nishimura, S.; Kawamura, N.; Hanioka, K.; Inoue, T.; Nishimura, R. Photodynamic Therapy for Cervical Intraepithelial Neoplasia. Oncology 2005, 69, 110–116. [Google Scholar] [CrossRef] [PubMed]
- Istomin, Y.P.; Lapzevich, T.P.; Chalau, V.N.; Shliakhtsin, S.V.; Trukhachova, T.V. Photodynamic Therapy of Cervical Intraepithelial Neoplasia Grades II and III with Photolon. Photodiagn. Photodyn. Ther. 2010, 7, 144–151. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Ferrer-Espada, R.; Baglo, Y.; Gu, Y.; Dai, T. Antimicrobial Blue Light Inactivation of Neisseria Gonorrhoeae: Roles of Wavelength, Endogenous Photosensitizer, Oxygen, and Reactive Oxygen Species. Lasers Surg. Med. 2019, 51, 815–823. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Type of Disease | Type of Photosensitizer | Light Source | Light Parameters | References |
|---|---|---|---|---|
| Condyloma acuminata (penis) | 5-ALA | Helium-neon laser | Wavelength 635 nm Power density 100 mW/cm2 | [55] |
| Genital warts and Subclinical Human papilloma virus (HPV) | 5-aminolevulinic acid (ALA) | Carbon diode (CO2) laser | Wavelength 635 nm Fluence 100 J/cm2 Power density 100 mW/cm2 | [61] |
| Condyloma acuminata (urethral) | 5-ALA | Semiconductor laser | Wavelength 635 nm Power density 100 mW/cm2 Fluence 100 J/cm2 | [62] |
| HPV Condyloma (perianal and vulval regions) | Methyl aminolevulinate | LEDs | Wavelength 630 nm Power density 80 mW/cm2 Fluence 100 J/cm2 | [63] |
| Condyloma acuminata | 5-ALA | CO2 laser light | Fluence 100–150 J/cm2 Power density 60–100 mW/cm2 | [64] |
| Condyloma acuminata | 5-ALA | Cylindrical laser fiber High energy narrow-band red light therapy equipment | Urethral meatus with a spot size <3 cm: Wavelength 630 ± 5 nm Fluence 100–150 J/cm2 Power density 150–300 mW/cm2 Size ≥ 3 cm Wavelength 633 ± 5 nm Fluence 105 J/cm2 | [65] |
| Condyloma acuminata | 5-ALA | CO2 laser red light | Wavelength 600–740 nm Fluence 100 J/cm2 Power density 100 mW/cm2 | [66] |
| Cervical intraepithelial neoplasia | Polyhematoporphyrin ether/ester | YAG-OPO laser (laser pumped optical parametric oscillator) | Wavelength 630 nm Fluence 100 J/cm2 | [102] |
| Cervical intraepithelial neoplasia | 5-ALA | Thermal light source emitting a broadband red light Illuminate the cervical canal | 150 W halogen lamp Power density 90 mW/cm2 Fluence 100 J/cm2 Power density 300 mW/cm2 Fluence 50 J/cm2 | [103] |
| Cervical intraepithelial neoplasia | Hexaminolevulinate (HAL) | Red coherent laser and a special light catheter | Wavelength 633 nm | [104] |
| Cervical intraepithelial neoplasia | Photofrin | Excimer dye laser Or YAG-OPO laser | Wavelength 630 nm Fluence 100 J/cm2 | [105] |
| Cervical intraepithelial neoplasia | Photolon (a combination of chlorin e6 potassium salt and low-weight polyvinylpyrrolidone) | Therapeutic laser device “LD680-2000” | Wavelength 670 nm Power density 200 mW/cm2 Fluence 100 J/cm2 | [106] |
| Cervical intraepithelial neoplasia | 5-ALA | Semiconductor laser | Wavelength 635 nm Power density 100–150 mW/cm2 Fluence 100 J/cm2 | [72] |
| Cervical intraepithelial neoplasia combined with high-risk HPV | 5-ALA | Red laser | Wavelength 633 nm Fluence 80 J/cm2 | [73] |
| High-risk HPV without cervical lesions | 5-ALA | Cylindrical semiconductor laser fiber | Wavelength 635 nm Power density 100 mW/cm2 Fluence 100 J/cm2 | [74] |
| Cervical intraepithelial neoplasia combined with high-risk HPV | 5-ALA | LED | Wavelength 635 nm Fluence 100 J/cm2 | [75] |
| Cervical intraepithelial neoplasia with vaginal intraepithelial neoplasia | 5-ALA | LED optical fibers Semiconductor laser | Wavelength 635 nm Fluence 80–120 J/cm2 | [76] |
| Early stage cervical cancer | Photoran E6 Fotoditazin | LED Flexible cylindrical diffuser | Wavelength 400 nm Power 1–1.2 W Fluence 400 J/cm2 | [19] |
| HSV (HSV-1 (VR-3 strain) and HSV-2 (MS strain)) infected Vero cell culture | Fotoditazin preparation (chlorin E6 derivative) | NI | NI | [79] |
| Genital and oral herpes | 5-ALA | Red light from a halogen lamp | Wavelength 630 ± 20 nm Power density 100 mW/cm2 Fluence 120 J/cm2 | [80] |
| HSV-I strain infected human epithelial cell | NI | Diode laser | Wavelength 830 nm | [81] |
| Hyperemic lesions labial herpes | NI | Low intensity red laser Direct machining control (DMC) Photon Laser II | Wavelength 660 nm Power density 100 mW/cm2 Fluence 30 J/cm2 | [82] |
| Neisseria gonorrhoeae (N. gonorrhoeae) (ATCC 700825) 4 clinical N. gonorrhoeae isolates | NI | LED | Wavelength 405 nm Power density 60 mW/cm2 | [90] |
| N. gonorrhoeae (ATCC 700825) one multidrug-resistant clinical strain of N. gonorrhoeae | NI | Blue light | Wavelength 405 nm Fluence 54 J/cm2 | [91] |
| N. gonorrhoeae (ATCC 700825) | NI | LED | Wavelength 405 nm, 470 nm Power density 60 mW/cm2 | [107] |
| Chlamydia (C.) pecorum 1710S C. trachomatis serovar E | NI | Water-filtered infrared A combined with visible light (wIRA/VIS) | Wavelengths 380 nm up to 1400 nm Power density 3700 W/m2 | [92] |
| C. trachomatis serovar E | NI | Warfighter Accelerated Recovery by Photobiomodulation (WARP) 10 LED | Wavelengths 405 nm, 670 nm Power density 60 mW/cm2 Fluence 5 J/cm2 | [93] |
| Trichomonas vaginalis CDC 085 strain (ATCC 50143) | Methylene blue | LED monochromatic light source | Wavelength 630 nm Power 300 mW | [96] |
| HIV/AIDS, co-infected with Candida (C.) albicans in the oral cavity | Methylene blue | LED | Wavelength 633 nm Power density 20.72 mW/cm2 Fluence 37.29 J/cm2 | [97] |
| Vulvovaginal candidiasis (C. albicans) | Methylene blue | PDT using the MAC Scar Acceleration Method Red laser | Wavelength 660 nm Power 100 mW | [98] |
| C. albicans | NI | Blue LED light sources | Wavelength 415 nm Power density 50 mW/cm2 | [99] |
| Vaginal candidiasis C. albicans (mouse model) | Methylene blue and protoporphyrin IX | LEDs | Wavelengths 660 nm, 630 nm Power 800 mW | [100] |
| C. albicans (mouse model) | Methylene blue | Red laser | Wavelength 660 nm Power density 100 mW/cm2 Fluence 18 J/cm2, 36 J/cm2 | [101] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mammari, N.; Hamblin, M.R.; Rauger, P.; Boyer, L.; Varbanov, M. Phototherapy-Based Treatment for Sexually Transmitted Infections—Shining Light into Unexplored Territory. Venereology 2022, 1, 170-186. https://doi.org/10.3390/venereology1020012
Mammari N, Hamblin MR, Rauger P, Boyer L, Varbanov M. Phototherapy-Based Treatment for Sexually Transmitted Infections—Shining Light into Unexplored Territory. Venereology. 2022; 1(2):170-186. https://doi.org/10.3390/venereology1020012
Chicago/Turabian StyleMammari, Nour, Michael R. Hamblin, Pauline Rauger, Laurence Boyer, and Mihayl Varbanov. 2022. "Phototherapy-Based Treatment for Sexually Transmitted Infections—Shining Light into Unexplored Territory" Venereology 1, no. 2: 170-186. https://doi.org/10.3390/venereology1020012