
Prevalence of Hepatitis B Virus Seromarkers in Female Sex Workers in Enugu State, Nigeria


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Area
2.2. Ethical Approval and Considerations
2.3. Data Collection
2.4. Study Design and Selection of Sample Population
2.5. Sample Collection
2.6. Sample Analysis and Test Procedure
2.7. Data Analysis
3. Results
3.1. Serological Patterns of HBV among FSWs
3.2. Prevalence of HBV among FSWs
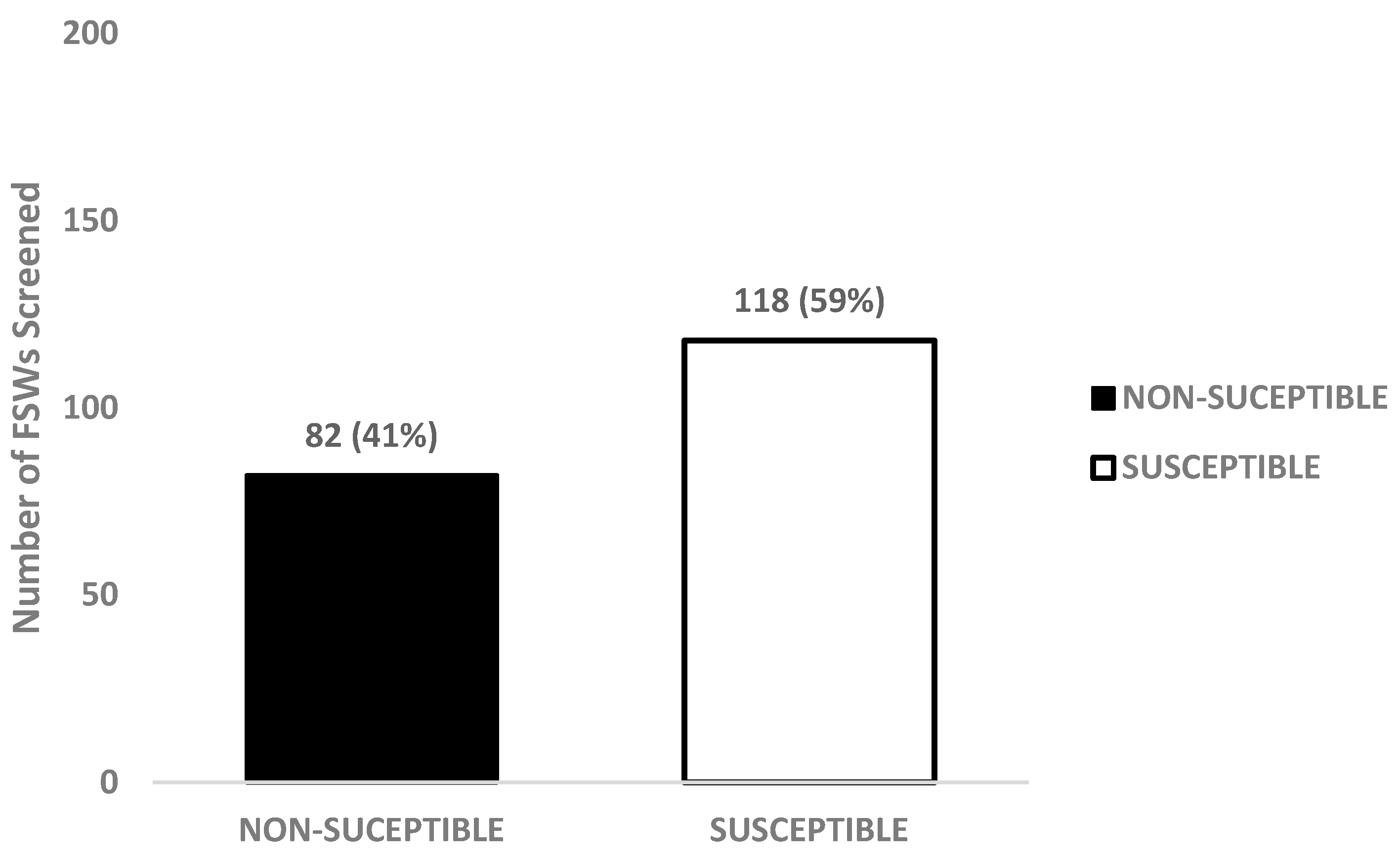
3.3. Susceptibility of FSWs to HBV
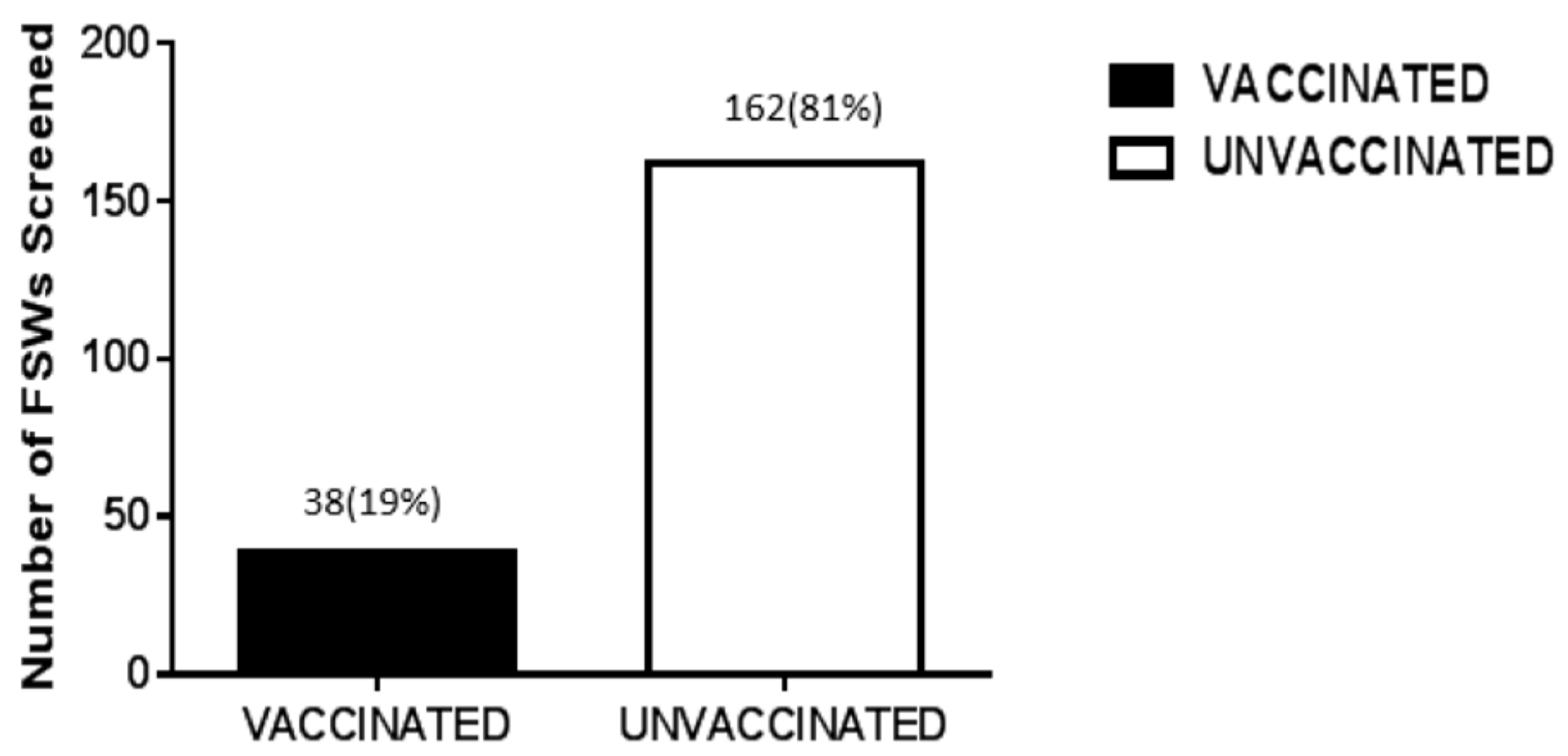
3.4. HBV Vaccination among FSWs
3.5. HBV Status of FSWs According to Age
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ringehan, M.; McKeating, J.A.; Protzer, U. Viral hepatitis and liver cancer. Phil. Trans. R. Soc. B 2017, 372, 20160274. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peligang, L.B.; Mello, V.M.; de Sousa, P.S.F.; Horta, M.A.P.; Soares, Á.D.; Nunes, J.P.d.S.; Nobrega, M.; Lewis-Ximenez, L.L. Transfusion transmissible infectious in blood donors in the province of Bié, Angola, during a 15-year follow-up, imply the need for pathogens reduction technologies. Pathogens 2021, 10, 1633. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Millions Persons Worldwide Are Living with HBV; Global Hepatitis Report. 2017. Available online: https://apps.who.int/iris/rest/bitstreams/1082592/retrieve (accessed on 10 February 2020).
- Weimer, A.; Tagny, C.T.; Tapko, J.B.; Gouws, C.; Tobian, A.A.R.; Ness, P.M.; Bloch, E.M. Blood transfusion safety in sub-Saharan Africa: A literature review of changes and challenges in the 21st century. Transfusion 2019, 59, 412–427. [Google Scholar] [CrossRef] [Green Version]
- El-Magrahe, H.; Furarah, A.R.; El-Figih, K.; El-Urshfany, S.; Ghenghesh, K.S. Maternal and neonatal seroprevalence of Hepatitis B surface antigen (HBsAg) in Tripoli, Libya. J. Infect. Dev. Ctries. 2010, 4, 168–170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, S.; Li, R.T.; Wang, Y.; Liu, Q.; Zhou, Y.H.; Hu, Y. Seroprevalence of hepatitis B surface antigen among pregnant women in Jiangsu, China, 17 years after introduction of hepatitis B vaccine. Int. J. Gynecol. Obstet. 2010, 109, 194–197. [Google Scholar] [CrossRef]
- Drazilova, S.; Kristian, P.; Janicko, M.; Halanova, M.; Safcak, D.; Dorcakova, P.D.; Marekova, M.; Pella, D.; Madarasova-Geckova, A.; Jarcuska, P.; et al. What is the role of the horizontal transmission of hepatitis B virus infection in young adult and middle-aged Roma population living in the settlements in East Slovakia? Int. J. Environ. Res. Public Health 2020, 17, 3293. [Google Scholar] [CrossRef]
- Belyhun, Y.; Maier, M.; Mulu, A.; Diro, E.; Liebert, G.U. Hepatitis viruses in Ethiopia: A systematic review and meta-analysis. BMC Infect. Dis. 2016, 16, 761. [Google Scholar] [CrossRef] [Green Version]
- Wu, J.; Han, M.; Li, J.; Yang, X.; Yang, D. Immunopathogenesis of HBV Infection. In Hepatitis B Virus Infection, Advances in Experimental Medicine and Biology; Tang, H., Ed.; Springer: Singapore, 2020; p. 1179. [Google Scholar]
- Hastings, K.L.; Green, M.D.; Gao, B.; Ganey, P.E.; Roth, R.A.; Burleson, G.R. Beyond Metabolism: Role of the Immune System in Hepatic Toxicity. Int. J. Toxicol. 2020, 39, 151–164. [Google Scholar] [CrossRef]
- Kao, J.H. Diagnosis of hepatitis B virus infection through serological and virological markers. Exp. Rev. Gastroenterol. Hepatol. 2008, 2, 553–562. [Google Scholar] [CrossRef]
- Attia, K.; Doffou, S.; Kissi, Y.; Bangoura, D.; Pianiza, S.; Mahassadi, K.; Bathaix, F.; Sayegh, M.; N’dri-Yoman, T. Virological profile of hepatitis B infection in Black African HBsAg chronic carriers. Open J. Gastroenterol. 2013, 3, 113–118. [Google Scholar] [CrossRef] [Green Version]
- Aktar, A.; Ali, M.A.; Haque, M.A.; Hossain, S.; Jasmine, T.; Zuman, K.; Islam, M.A.; Ahmad, F.; Sharmin, M.; Pandit, P.; et al. Prevalence of hepatitis B virus infection among children with liver disease admitted in Mymensingh medical college hospital. Mymensingh Med. J. 2021, 30, 897–902. [Google Scholar] [PubMed]
- Towell, V.; Cowie, B. Hepatitis B serology. Aust. Fam. Physician 2012, 41, 212–214. [Google Scholar] [PubMed]
- Shah, S.M.; Singh, S.P. Hepatitis B virus serology: Use and interpretation. Hepat. B Annu. 2007, 4, 39–54. [Google Scholar] [CrossRef]
- Kryger, P. Significance of anti-HBc IgM in the differential diagnosis of viral hepatitis. J. Virol. Methods 1985, 10, 283–289. [Google Scholar] [CrossRef]
- Gerlich, W.H.; Uy, A.; Lambrecht, F.; Thomssen, R. Cutoff levels of immunoglobulin M antibody against viral core antigen for differentiation of acute, chronic, and past hepatitis B virus infections. J. Clin. Microbiol. 1986, 24, 288–293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Libbus, M.K.; Phillips, L.M. Public health management of perinatal hepatitis B virus. Public Health Nurs. 2009, 26, 353–361. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, V.T.T.; McLaws, M.L.; Dore, G.J. Highly endemic hepatitis B infection in rural Vietnam. J. Gastroenterol. Hepatol. 2007, 22, 2093–2100. [Google Scholar] [CrossRef]
- World Health Organization. Baseline Report on Global Sexually Transmitted Infection Surveillance 2012; World Health Organization: Geneva, Switzerland, 2013.
- Shannon, K.; Strathdee, S.A.; Goldenberg, S.M.; Duff, P.; Mwangi, P.; Rusakova, M.; Reza-Paul, S.; Lau, J.; Deering, K.; Pickles, M.R.; et al. Global epidemiology of HIV among female sex workers: Influence of structural determinants. Lancet 2015, 385, 55–71. [Google Scholar] [CrossRef] [Green Version]
- Forbi, J.C.; Onyemauwa, N.; Gyar, S.D.; Oyeleye, A.O.; Entonu, P.; Agwale, S.M. High prevalence of hepatitis B virus among female sex workers in Nigeria. Revis. Instit. Med. Trop. São Paulo 2008, 50, 219–221. [Google Scholar] [CrossRef] [Green Version]
- WMA. WMA declaration of Helsinki-ethical principle for medical research involving human subjects. In Proceedings of the 59th WMA General Assembly Seoul, Seoul, Korea, 18 October 2008; Available online: http://wma.net/en/30publications/10policies/b3/index.html (accessed on 13 February 2020).
- Abulude, O.A.; Ahmed, I.; Sadisu, F.U. Assessment of hepatitis B viral infection as a predictor of hepatic enzymes and compounds alteration among antenatal patients. Med. Sci. 2017, 5, 24. [Google Scholar] [CrossRef] [Green Version]
- Ayodeji, A.O.; Ismai’la, A.; Umar, S.F. Comparative evaluation of chromatographic immunoassay and enzyme-linked immunosorbent assay in the diagnosis of hepatitis B viral infection in pregnancy. ARC J. Hematol. 2019, 4, 28–34. [Google Scholar]
- Zermiani, M.; Mengoli, C.; Rimondo, C.; Galvan, U.; Cruciani, M.; Serpelloni, G. Prevalence of sexually transmitted diseases and hepatitis C in a survey of female sex workers in the north-East of Italy. Open AIDS J. 2012, 6, 60. [Google Scholar] [CrossRef] [PubMed]
- Silverman, J.G.; Decker, M.R.; Gupta, J.; Dharmadhikari, A.; Seage, G.R., III; Raj, A. Syphilis and hepatitis B co-infection among HIV-infected, sex-trafficked women and girls, Nepal. Emerg. Infect. Dis. 2008, 14, 688–695. [Google Scholar] [CrossRef]
- Eledo, B.O.; Izah, S.C.; Onuoha, E.C. Sexually transmitted infections among female sex workers in some selected regions of Bayelsa State. Int. STD Res. Rev. 2017, 5, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Juárez-Figueroa, L.; Uribe-Salas, F.; Conde-Glez, C.; Hernández-Avila, M.; Olamendi-Portugal, M.; Uribe-Zúñiga, P.; Calderón, E. Low prevalence of hepatitis B markers among Mexican female sex workers. Sex. Trans. Infect. 1998, 74, 448–450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Danjuma, G.; Gidado, I. Assessment of Risk Factors and Prevalence of Viral Hepatitis B & C among Female Sex Workers (FSWs) in Jalingo, Northeastern Nigeria; World Hepatitis Summit: São Paulo, Brazil, 2017. [Google Scholar]
- Halim, N.K.D.; Kubenyinje, E.P.; Onunu, A. Sero-prevalence of hepatitis B surface antigen (HBsAg) in sexually transmitted disease patients. J. College Med. 2004, 9, 107–109. [Google Scholar]
- Mbaawuaga, E.M.; Iroegbu, C.U.; Ike, A.C.; Jombo, G.T.A. Studies on prevalence, co-infection and associated risk factors of hepatitis B virus (HBV) and Human immunodeficiency virus (HIV) in Benue State, Nigeria. Sci. J. Public Health 2014, 2, 569–576. [Google Scholar]
- Ophori, E.A.; Tula, M.Y.; Azih, A.V.; Okojie, R.; Ikpo, P.E. Current trends of immunization in Nigeria: Prospect and challenges. Trop. Med. Health 2014, 42, 67–75. [Google Scholar] [CrossRef] [Green Version]
- Jibrin, Y.B.; Kolo, P.M.; Mohammed, A.; Sanya, E.O.; Aliyu, L.D. Burden of hepatitia B and C infections among pregnant women in Bauchi, North-eastern Nigeria. Sub Sahar. Afr. J. Med. 2016, 3, 188. [Google Scholar]
- Lemoine, M.; Nayagam, S.; Thursz, M. Viral hepatitis in resource-limited countries and access to antiviral therapies: Current and future challenges. Future Virol. 2013, 8, 371–380. [Google Scholar] [CrossRef] [Green Version]
- CDC. Hepatitis B FAQs for Health Professionals: Division of Viral Hepatitis and National Centre for HIV/AIDS Viral Hepatitis STD and TB Prevention. 2018. Available online: https://www.cdc.gov/hepatitis/hbv/bfaq.htm (accessed on 26 February 2020).
- Olayinka, A.T.; Oyemakinde, A.; Balogun, M.S.; Ajudua, A.; Nguku, P.; Aderinola, M.; Egwuenu-Oladejo, A.; Ajisegiri, S.W.; Sha’aibu, S.; Musa, B.O.P.; et al. Seroprevalence of Hepatitis B Infection in Nigeria: A National Survey. Am. J. Trop. Med. Hyg. 2016, 95, 902–907. [Google Scholar] [CrossRef] [PubMed]
- Ajuwon, B.I.; Yujuico, I.; Roper, K.; Richardson, A.; Sheel, M.; Lidbury, B.A. Hepatitis B virus infection in Nigeria: A systematic review and meta-analysis of data published between 2010 and 2019. BMC Infect. Dis. 2021, 21, 1120. [Google Scholar] [CrossRef] [PubMed]
- Jeon, J.W.; Kim, S.M.; Cho, H.; Baek, C.H.; Kim, H.; Shin, S.; Kim, Y.H.; Han, D.J.; Kim, S.B. Presence of hepatitis B surface antibody in addition to hepatitis B core antibody confers protection against hepatitis B virus infection in hepatitis B surface antigen-negative patients undergoing kidney transplantation. Transplantation 2018, 102, 1717–1723. [Google Scholar] [CrossRef] [PubMed]
- Du, X.; Liu, Y.; Ma, L.; Lu, J.; Jin, Y.; Ren, S.; He, Z.; Chen, X. Virological and serological features of acute hepatitis B in adults. Medicine 2017, 96, 7. [Google Scholar] [CrossRef]
- Dan-Nwafor, C.; Adeoye, I.; Aderemi, K.; Adebobola, B.; Nguku, P.; Ade-Yusuf, I.; Udom, E. Knowledge, serological markers and risk factors associated with hepatitis B and C virus infection among Kuje prison inmates, Federal Capital Territory, Nigeria. Int. J. Infect. Dis. 2018, 73, 374. [Google Scholar] [CrossRef]
- Adelekan, A.L.; Omoregie, P.I.; Edoni, E.R. Sexual practices of female sex workers who inject drugs in Oshogbo, Nigeria. Int. Scholar. Res. Not. 2014, 2014, 1–7. [Google Scholar] [CrossRef]
- Ochu, C.L.; Beynon, C.M. Hepatitis B vaccination coverage, knowledge and sociodemographic determinants of uptake in high risk public safety workers in Kaduna State, Nigeria: A cross sectional survey. Brit. Med. J. 2017, 7, e015845. [Google Scholar] [CrossRef]
- Nsirimobu, I.P.; Peterside, O. Hepatitis B vaccination rate among medical students at the University of Port Harcourt Teaching Hospital (UPTH), Nigeria. Nig. Health J. 2014, 14, 64–70. [Google Scholar]
- Al-Mekhaizeem, K.A.; Miriello, M.; Sherker, A.H. The frequency and significance of isolated hepatitis B core antibody and the suggested management of patients. Can. Med. Assoc. J. 2001, 165, 1063–1064. [Google Scholar]
- Zobeiri, M. Occult hepatitis B: Clinical viewpoint and management. Hep. Res. Treat. 2013, 2013, 259148. [Google Scholar] [CrossRef]
- Allain, J.P. Occult hepatitis B virus infection: Implications in transfusion. Vox Sang. 2004, 86, 83–91. [Google Scholar] [CrossRef] [PubMed]
- Anaedobe, C.G.; Fowotade, A.; Omoruyi, C.E.; Bakare, R.A. Prevalence, socio-demographic features and risk factors of hepatitis B virus infection among pregnant women in Southwestern Nigeria. Pan Afr. Med. J. 2015, 20, 406. [Google Scholar] [CrossRef] [PubMed]
- Mbaawuaga, E.M.; Iroegbu, C.U.; Ike, A.C. Hepatitis B Virus (HBV) Serological Patterns in Benue State, Nigeria. Open J. Med. Microbiol. 2014, 4, 43008. [Google Scholar] [CrossRef] [Green Version]
- Mzingwane, M.L.; Mamvura, T. Hepatitis B virus seroprevalence and serology patterns in a cohort of HIV positive individuals from Harare, Zimbabwe. J. Viruses 2014, 2014, 691953. [Google Scholar] [CrossRef] [Green Version]
- Ifeorah, I.M.; Bakarey, A.S.; Adewumi, M.O.; Faleye, F.O.C.; Akere, A.; Omoruyi, C.E.; Ogunwale, A.O.; Uttah, C.C.; Oketade, M.A.; Adeniji, J.A. Patterns of Serologic Markers of Hepatitis B Virus Infection and the Risk of Transmission Among Pregnant Women in Southwestern Nigeria. J. Immunassay Immunochem. 2017, 38, 639–651. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Serologic Patterns | Frequency Occurrence (%) | Interpretation |
|---|---|---|
| HBsAg+, anti-HBs−, total anti-HBc+ | 6(3) | Infected and Contagious |
| HBsAg+, anti-HBs+, total anti-HBc+ | 1(0.5) | Infected and Contagious |
| HBsAg+, anti-HBs−, total anti-HBc- | 1(0.5) | Infected and Contagious |
| HBsAg−, anti-HBs+, total anti-HBc− | 38(19) | Uninfected with immunity from vaccination |
| HBsAg−, anti-HBs+, total anti-HBc+ | 19(9.5) | Exposed with immunity from previous HBV infection |
| HBsAg−, anti-HBs−, total anti-HBc+ | 17(8.5) | Exposed with no evidence of immunity |
| HBsAg−, anti-HBs−, total anti-HBc− | 118(59) | Non-exposed and non-immune to HBV |
| Total | 200 | |
| HBsAg+ present | 8(4) | HBV carrier status |
| Anti-HBs+ present | 57(28.5) | Immunity status |
| Total Anti-HBc+ (only) present | 17(8.5) | Previous exposure |
| HBV Status (HBsAg) | Prevalence % |
|---|---|
| Positive | 8(4) (Intermediate Endemicity) |
| Negative | 192(96) |
| Total | 200(100) |
| Serological Patterns Observed | Frequency Occurrence (%) | Indication |
|---|---|---|
| HBsAg+, anti-HBs+, HBeAg−, anti-HBe−, anti-HBc+. | 1(0.5) | Early convalesce stage |
| HBsAg+, anti-HBs−, HBeAg−, anti-HBe−, anti-HBc−. | 1(0.5) | Possible early stage of HBV infection |
| HBsAg+, anti-HBs−, HBeAg−, anti-HBe+, anti-HBc+. | 6(3) | Possible late acute or chronic HBV infection with low infectivity |
| Total | 8(4) |
| HBV Infection Status | Vaccination History | Total (%) | ||
|---|---|---|---|---|
| Yes (%) | No (%) | Don’t Know | ||
| Current Infection | 2(1.0) | 5(2.5) | 1(0.5) | 8(4) |
| Vaccine response | 4(2.0) | 30(15.0) | 4(2.0) | 38(19.0) |
| Exposed (immune) from past infection | 0(0) | 11(5.5) | 8(4.0) | 19(9.5) |
| Exposed with no evidence of immunity | 0(0) | 14(7.0) | 3(1.5) | 17(8.5) |
| Unexposed | 10(5.0) | 89(44.5) | 19(9.5) | 118(59.0) |
| Total | 16(8.0) | 149(74.5) | 35(17.5) | 200(100) |
| Age Group | Number Tested | Infected and Contagious | Past Exposure | Unexposed |
|---|---|---|---|---|
| 10–19 | 11(5.5) | 1(9.1) | 2(18.2) | 8(72.7) |
| 20–29 | 109(54.5) | 6(5.5) | 34(31.2) | 67(61.5) |
| 30–39 | 66(33) | 0(0) | 32(48.5) | 34(51.5) |
| 40–49 | 12(6) | 1(8.3) | 4(33.3) | 8(66.7) |
| 50–59 | 2(1) | 0(0) | 2(100) | 0(0) |
| Total | 200 | 8(4) | 74(37) | 118(59.0) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aniche, O.M.-C.; Orabueze, I.N.; Nwafia, I.N.; Ihezuo, J.U.; Chinaka, C.B.; Egbe, K.A.; Ike, A.C. Prevalence of Hepatitis B Virus Seromarkers in Female Sex Workers in Enugu State, Nigeria. Venereology 2022, 1, 124-134. https://doi.org/10.3390/venereology1010009
Aniche OM-C, Orabueze IN, Nwafia IN, Ihezuo JU, Chinaka CB, Egbe KA, Ike AC. Prevalence of Hepatitis B Virus Seromarkers in Female Sex Workers in Enugu State, Nigeria. Venereology. 2022; 1(1):124-134. https://doi.org/10.3390/venereology1010009
Chicago/Turabian StyleAniche, Oluchi Mary-Cynthia, Ibuchukwu Nkeonyenasoya Orabueze, Ifeyinwa Nkiruka Nwafia, Justina Uchechi Ihezuo, Chinwe Blessing Chinaka, Kingsley Andrew Egbe, and Anthony Chibuogwu Ike. 2022. "Prevalence of Hepatitis B Virus Seromarkers in Female Sex Workers in Enugu State, Nigeria" Venereology 1, no. 1: 124-134. https://doi.org/10.3390/venereology1010009