
Recurrent Candida Vulvovaginitis


1
School of Medicine, Kabale University, Kabale P.O. Box 317, Uganda
2
Department of Medical Microbiology & Immunology, Faculty of Medicine, Gulu University, Gulu P.O. Box 166, Uganda
*
Authors to whom correspondence should be addressed.
Venereology 2022, 1(1), 114-123; https://doi.org/10.3390/venereology1010008
Submission received: 23 March 2022
/
Revised: 26 April 2022
/
Accepted: 7 May 2022
/
Published: 24 May 2022
Abstract
:Vulvovaginal candidiasis (VVC), predominantly caused by Candida albicans, is estimated to affect about 138 million women each year worldwide and 492 million over their lifetimes. Recurrent VVC (RVVC), defined as four or more episodes of VVC in a year, is increasingly recognized and constitutes up to 10% of the cases of VVC. RVVC is an important clinical and global public health challenge project that will affect about 160 million per year by 2030. RVVC significantly affects the quality of life of the affected women. Host factors, such as underlying immunosuppressive conditions and genetic predisposition, are suggested key risk factors for recurrence. However, an increasingly higher prevalence of non-albicans Candida (NAC) species, such as C. glabrata, C. tropicalis, C. krusei, C. parapsilosis, C. dubliniensis, C. guilliermondii, and others, which are either intrinsically resistant to azoles or have higher minimum inhibitory concentrations to most antifungal agents, such as fluconazole, which are commonly used for the treatment of VVC/RVVC, has been reported. Therefore, treatment remains a challenge. Long-term maintenance antifungal is required to avoid recurrence of symptoms. Alternative treatment includes boric acid and topical amphotericin B; however, they are associated with serious side effects, limiting their use. The oral echinocandin ibrexafungerp is well-tolerated and efficacious against Candida vulvovaginitis. RVVC presents a unique area for continued research and development.
1. Introduction
Candida vulvovaginitis, or vulvovaginal candidiasis (VVC), was first documented by Wilkinson in 1849 and continues to be a debilitating problem that affects the quality of life of many women [1]. It is one of the most common manifestations of Candida infection, estimated to affect approximately 75% of women at some point in their lifetime. Furthermore, over 5% of women suffer at least four episodes of VVC in a year, and this is referred to as recurrent vulvovaginal candidiasis (RVVC) [2,3,4].
The hallmark for the diagnosis of VVC is an acute inflammatory condition of the vulvovaginal mucosa induced by overgrowth of Candida that commonly exist as a member of the vulvovaginal microbiota [5]. Although most VVC can be effectively treated with antifungal agents, such as topical or systemic azoles/triazoles, VVC recurrence is a common problem and sometimes may be very troublesome [6]. RVVC is a multifactorial disease whose symptoms are governed by the interplay between Candida species (albicans and non-albicans Candida species), co-existent bacterial flora (such as Lactobacillus spp.), the microenvironment (that is, the inflammatory status, oxidative stress, and estrogen levels), and the host factors, including the immune status, social behaviors, and genetic factors [7]. A variation in any of these factors may induce RVVC [8]. Candida albicans is the predominant pathogen responsible for up to 90% of VVC, while other non-albicans Candida (NAC) species, most commonly C. glabrata, C. parapsilosis complex, C. krusei, and C. dubliniensis, account for 10 to 20% of VVC cases and are associated with complicated VVC, which exhibits less severe symptoms than C. albicans VVC but higher recurrence rates [9,10].
There is an increasing burden of RVCC, imposing management challenges, particularly with the growing burden of antifungal-resistant Candida isolates. In this review, we provide an update on the epidemiology, pathogenesis, risk factors, diagnosis, and treatment of RVVC.
2. Epidemiology
The precise burden of RVVC is unknown. A recent study systematically evaluated epidemiological studies from 1985 to 2016. The study, by Foxman and colleagues, was based on the 6000 online surveys from five western European countries and the United States and documented a global annual prevalence of 3871 RVVC cases per 100,000 women, at a frequency of 9% in patients of reproductive age (18 to 49 years) [3]. VVC was noted to affect about 138 million women each year worldwide and 492 million over their lifetimes [3]. It was projected that the population of women with RVCC will increase to almost 158 million in 2030 [3,11]. Candida species is reported as the second-most common cause of vaginitis in the USA [12].
3. Etiology
C. albicans accounts for the majority of the cases of RVVC. However, emerging evidence increasingly points to the causal role of NAC species, particularly C. glabrata and C. parapsilosis [10,13,14]. This has been attributed to be due to widespread use of over-the-counter drugs, longer-term use of suppressive azoles, and the use of short courses of antifungal drugs. Although the severity of symptoms is milder with the NAC species, they have been associated with antimycotic resistance and generally respond to higher MICs of azoles [13].
4. Pathogenesis
The pathogenesis of VVC is a process that is determined by the virulence of the Candida species; these different virulence factors are created by the interaction of the host with microorganisms, which may eventually lead to tissue damage, making them even more pathogenic. These virulence factors include modifying the expression of adhesins to help the Candida adhere to epithelial cells, the capability to make a morphological switch from yeast to hyphae, invasiveness through the expression of invasins, the formation of biofilms, the secretion of hydrolytic enzymes, such as secreted aspartyl proteases (SAP) and candidalysin, and the ability to escape from phagocytosis by neutrophils and macrophages [15,16,17].
Candida species exists in two morphological forms, i.e., the unicellular yeast, and multicellular hyphae [17]. Initially, yeast cells adhere to the vaginal epithelium [18]. Following this initial contact, hyphae will grow out of the yeast cells, then eventually transition from yeast to filamentous growth. This is one of the most important virulence traits. The filamentous form is more invasive than the yeast form; hence, it penetrates the tissue and escapes from recognition by the immune system of the host.
The evolution of the disease is determined to a great extent by the hyphal-expressed adhesins, whereas, in general, yeast cells adhere directly to the epithelial cells, which is ensued by transition to hyphae form. There is evidence of direct adhesion of the Candida hyphal form to the epithelial cells as hyphae grow from one epithelial cell to another [17].
Following adherence to the vaginal epithelial cells, yeast cells of Candida form hyphae and become detectable by the immune system. A significantly high hyphal burden is required for epithelial activation because the presence of hyphae goes undetected below a certain threshold level. This is attributed to the dual lifestyle of Candida species as vaginal microbiota and an opportunistic pathogen [19].
There are two pathways in place to differentiate between the colonizing yeast and the invasive hyphal form. Candida species can be recognized via two different pathways. The first pathway is represented by an early response that occurs in a morphologically independent manner. The second pathway starts when a burden threshold of hyphae is reached; this is a stronger response to hyphae, which, in turn, leads to activation of epithelial cells and the production of cytokines, chemokines, and other inflammatory mediators. There seems to be a local mucosal overreaction caused by an exaggerated inflammatory response accounting for vulvovaginal symptoms. This response can be triggered by host pattern recognition receptors (PRP) interacting with fungal-pathogen-associated molecular patterns (PAMPs) and other more complex mechanisms (i.e., secreted aspartyl proteases (Sap)-mediated NLRP3 activation and the cytolytic peptide toxin candidalysin) [20,21]. The activation of the innate immune system by a series of proinflammatory cytokines and chemokines leads to the recruitment of neutrophils to the vaginal mucosa, subsequently exacerbating symptomatic disease [20,21,22].
Furthermore, Candida species apply tissue damage by direct invasion by hyphal filaments or secretion of virulence effectors. Invasion of Candida species can occur with the help of invasins after a switch from the yeast to the hyphal form. Invasion into host cells can be achieved by endocytosis or active penetration. This, consequently, leads to damage to the epithelial cells via necrosis and apoptosis and, hence, a loss of epithelium [18,23].
Recognition is triggered by a high burden of hyphae above the normal threshold. The hyphal form was needed to cause damage to the epithelium, releasing pro-inflammatory cytokines and neutrophil recruitment [17]. A study completed by Fidel et al., 2004 demonstrated that healthy women with no prior history of vulvovaginal candidiasis showed a differential susceptibility to develop symptomatic VVC of 15%, while women with a history of recurrent VVC were at 55% [5].
Candida species have a great ability to form biofilm. This virulence trait is a key contributing factor to antifungal resistance and is a likely contributor to treatment failure in RVVC [18,24]. Candida secretes extracellular matrix (ECM), which results in a “biofilm” in which the Candida yeast cells embed. This ECM consists of exopolymeric macromolecules, including polysaccharides, proteins, lipids, and nucleic acids, which are secreted by sessile cells within the biofilm. A biofilm is characterized by a complex colony of yeast-form and hyphal cells surrounded by ECM, and it provides protection for the yeast against the host’s immune system, and antifungal agents bring about drug resistance. The biofilm slowly disperses yeast-form cells into the surroundings, which may be able to colonize other surfaces [19,24]. It seems that this morphogenesis reflects the integrity/nteractionn of multiple genetic and environmental factors responsible for the virulence of fungi [15].
5. Vaginal Microbiome and Risk Factors for Vulvovaginal Candidiasis
VVC is well-recognized as a multifactorial disease, where the Candida species and its virulence factors, disbalance in vaginal microbiome (dysbiosis), host-related precipitating factors, and idiopathic factors, such as genetics, determine the disease onset and propensity to recur [8].
Alteration in the vaginal microbiome leading to fungal dysbiosis can result in VVC and its symptoms. A healthy vaginal normal flora consists of different microorganisms. The primary colonizing bacteria of normal vagina mucosa are of the genus Lactobacillus (90–95%), such as L. crispatus, L. iners, and L. jensenii, but also fungi such as C. albicans and C. glabrata, living in symbiosis [8,25]. Lactobacillus species have been known as the gatekeepers of the vaginal ecosystem. They play several important roles in maintaining a healthy vaginal microbiome. Lactobacillus species decrease the opportunism of potentially pathogenic microorganisms by microbial competition, which reduces the adherence of Candida species to the vaginal epithelium [16,26]. Lactobacillus maintain the vaginal pH between 4 and 4.5, which is normal in healthy women of reproductive age. As the fermentation of glycogen within the vaginal epithelium produces lactic acid, the vaginal pH decreases and non-resident microbiota are suppressed, thereby protecting against opportunistic infections [18,26,27,28].
Furthermore, Lactobacillus spp produce bacteriocins that positively affect the commensal community through their antimicrobial function by limiting pathogens. Moreover, Lactobacillus spp induce the expression of genes that prevent the adherence of yeast to the epithelium and limit yeast-to-hyphal formation, keeping the Candida yeast cells in their less invasive form and, consequently, inhibiting overgrowth of Candida species [16,26].
Lactobacillus spp also cause modulation of the local immune system [16]. When the healthy microbial balance is disturbed, Lactobacillus spp may lose their ascendancy, and other microorganisms, such as C. albicans, can foster and cause overgrowth. Multiple factors can alter the vaginal microbiota and disturb the balance between the tolerance and invasion of Candida species. Important drivers for the pathogenesis of VVC are changes in the Lactobacillus community, elevated estrogen levels (i.e., due to oral contraceptives, hormone replacement therapy (HRT) used in post-menopause, being in the luteal phase of the menstruation cycle, or pregnancy), an elevated pH, and the presence of glucose and eicosanoids (such as prostaglandin E2 and thromboxane B2) [8,29]. Other determinants have an inhibitory effect on VVC, such as lactate and the presence of short-chain fatty acids, such as acetate, butyrate, and propionate B, immunodeficiency due to genetic aberrations, local immune overreaction, the inefficiency of prescribed antifungal agents, and, to a lesser extent, the development of antifungal resistance contributes to RVVC [8,29].
A broad spectrum of host-related precipitating factors, such as genetic background (polymorphism, familial, ethnicity), uncontrolled diabetes mellitus, altered immune status, pregnancy, use of steroids, and antibiotic overuse, as well as behavioral factors, such as sexual activity, hormone replacement therapy, and use of contraceptives, including intrauterine devices, have been associated to promote VVC pathology [3,4,8].
In 20 to 30% of the RVVC patients, the risk factors remain unknown. It is suggested that the Candida species, its virulence, and inter-individual differences play a key role in idiopathic RVVC pathogenesis. Several epidemiologic and cohort studies demonstrated that genetic mutations and polymorphisms and ethnicity play a role [8,24]. Moreover, NAC species are also associated with recurrent infections in VVC patients, likely because of their natural resistance towards azole-based antifungals. Incomplete clearance of infection can result in a rapid relapse, causing the prolongation of debilitating symptoms and healthcare-burdening allergic responses to Candida antigens [8].
6. Clinical Manifestations
Most patients with VVC are symptomatic. The typical VVC symptoms include pruritus, burning, soreness, irritation, discomfort, dyspareunia (painful sexual intercourse), and abnormal vaginal discharge. Vaginal examination may reveal vulval, introital, and vaginal erythema, edema, excoriation, and fissure formation, together with a cottage-cheese-like vaginal discharge; however, this is nonspecific [4,30]. These symptoms have not only become an epidemiological and clinical problem but also include larger social and psychological consequences. These recurrent cases are debilitating and impact quality of life. Women with RVVC report a loss of confidence and self-esteem, inability to carry on with their normal physical activities, and difficulties with their sexual life and intimate relationships. It is also associated with psychological stress, including depression and anxiety, often drug-resistant mucosal infection that has a substantial negative impact on work, and quality of life [31].
7. Diagnosis
Laboratory testing is recommended to confirm the diagnosis of VVC because self-diagnosis based on symptoms has an accuracy rate of only 28% for C. albicans in self-treating women due to the many non-specific symptoms, making over-the-counter antifungals often ineffective [11,32]. The gold standard for the diagnosis of VVC is by culturing the cells and microscopic detection of yeast cells and hyphae in Candida-positive cultures [3,33]. Gram staining of vaginal discharge mixed with potassium hydroxide (KOH) is used to distinguish Candida yeast cells and hyphae, which is relevant for the staging of the pathogenesis. The pH of the vaginal discharge is also an important indicator and normally stays within a range of 4.0 to 4.5 [4,9,34].
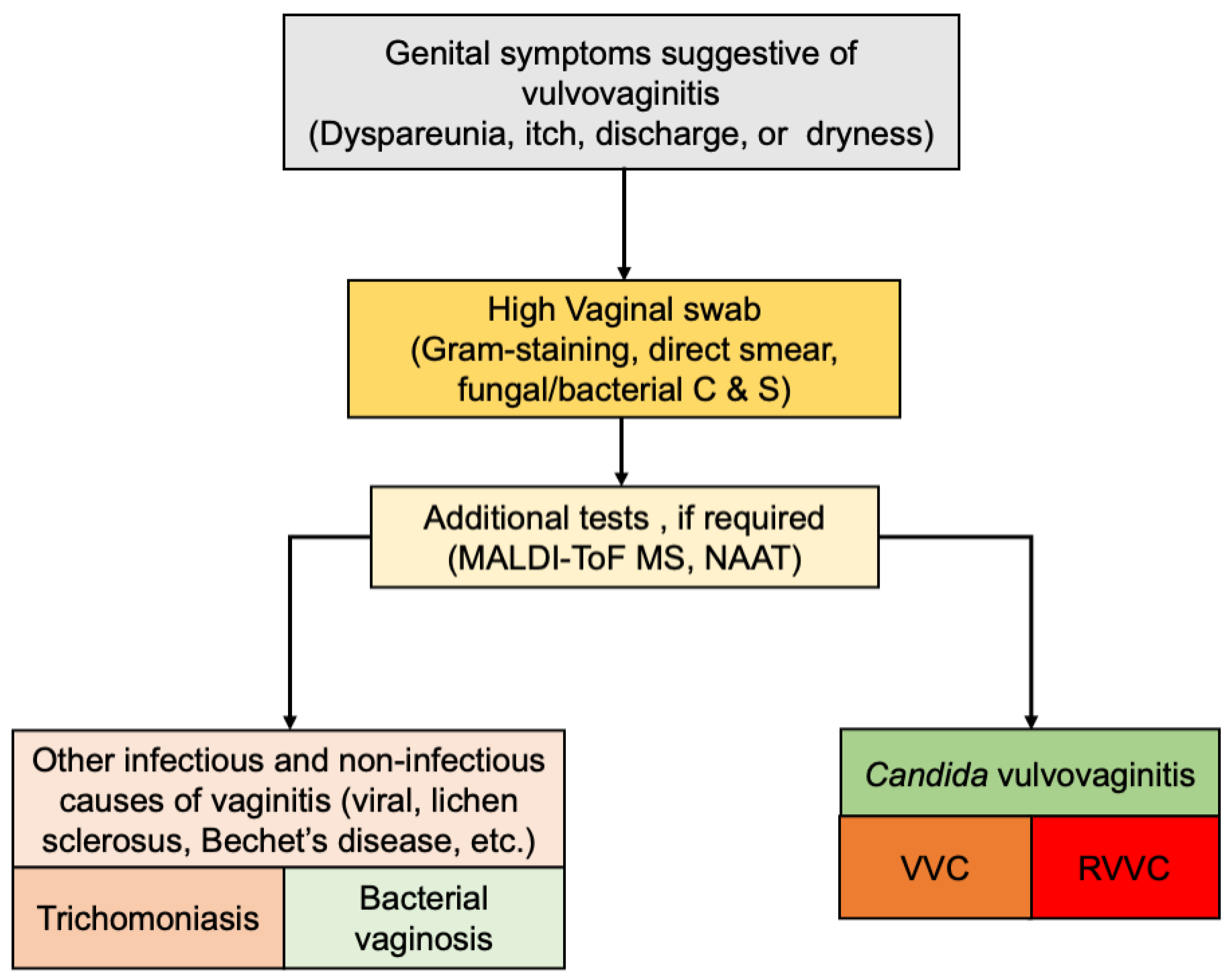
For further differentiation between Candida species, additional culturing is needed, e.g., with chromogenic agar or Sabouraud’s dextrose agar. In fact, culture is the most selective procedure in the sense of the isolation of the pathogen, and molecular methods, such as sequencing of the internal transcribed spacer (ITS sequencing), are often used for epidemiologic investigation. Newer methods, such as matrix-assisted laser desorption ionization time-of-flight mass spectrometry (MALDI-ToF MS), are needed to identify the specific species [35,36] (Figure 1). This is especially relevant in the case of RVVC, in which NAC species are becoming more prevalent. Similarly, susceptibility testing may be of adjuvant need in RVVC as these infections are more resistant to antifungal agents [34].
8. Current Treatment Options for Recurrent Vulvovaginal Candidiasis
Many antifungal regimens are available for treatment, some of them with adverse effects that end up reducing women’s adherence to treatment. Additionally, the lack of clear criteria for prescription of available drugs and their free use due to self-medication by women has contributed to the increasing antifungal resistance found in some clinical trials [13,16,29] (Table 1).
VVC and RVVC are often treated with azole agents that are fungistatic due to the inhibition of ergosterol biosynthesis in Candida species [37]; however, they are substantially less active against NAC species [41]. The standard treatment for RVVC caused by NAC is more complicated, requiring prolonged suppressive azole therapies, and is often unsuccessful. It consists of 10 to 14 days of induction therapy with a topical antifungal agent or oral fluconazole 150 mg, followed by fluconazole 150 mg once a week for 6 months. Recurrence rates of 60% to 70% are observed [11].
Fluconazole is a cost-effective, well-tolerated medication that is easily administered orally and is the most-used antifungal drug in many countries. Fluconazole resistance has been reported in women with RVVC. It is easily attained over the counter. However, epidemiological studies suggest that almost all patients diagnosed with fluconazole-resistant C. albicans have a history of prior exposure to fluconazole [42].
The rates of azole resistance are highly variable, and they may be influenced by the prescribing patterns of clinicians for both treatment and prophylaxis. It was observed that women with RVVC with vulval excoriation, longer disease time, and a family history of atopic disease are at a greater risk of not responding to maintenance treatment with fluconazole [11].
The current treatment options for VVC include azoles sold without a prescription for oral or intravaginal use. The side effects of oral treatment reported include headache, abdominal pain, and nausea, while the excessive use and overuse of such topical agents have had other adverse consequences, such as oedema, irritability of the skin, and perhaps even chronic vulvar pain condition (vulvodynia). In addition, long-term treatments are expensive, and approximately 50% of women experience the recurrence of symptoms a few months after treatment completion [43].
The efficacy of therapeutics, such as amphotericin B and boric acid, has been assessed for the treatment of RVVC but never proven. However, in multicenter studies, both drugs, when delivered intravaginally for 14 to 21 days, were found to be effective in around 70% of patients [33,34]. Indeed, sessile cells, i.e., biofilm-contained Candida cells, have been shown to tolerate antifungal concentrations 1000-fold greater than their planktonic counterparts [44]. Therefore, an alternative therapeutic strategy for RVVC may be through microbiome replacement therapy in the form of Lactobacillus probiotics [45].
Probiotic therapy involves the administration of live microorganisms, which directly results in a health benefit for the patient. Due to the diversity of Lactobacillus within the vaginal microbiome, it is difficult to estimate which species would be most important to replace with probiotic therapy [46].
Echinocandins are broad-spectrum and possess fungicidal activity with a safety profile better than other antifungals. They act by inhibition of (1-3)-β-d-glycan synthase. However they are only available for administration by intravenous infusion, hence the need for orally available options [38]. NAC species resistance to echinocandins is increasingly prevalent at between 3 and 30% among patients who are extensively using echinocandins, especially in strains exhibiting less susceptibility to fluconazole and other azoles [47,48].
Ibrexafungerp is the first orally available (1-3)-β-d-glycan synthase inhibitor, a key enzyme in the biosynthesis of β-1,3-d-glucan and a major component of the fungal cell wall [39]. It was developed to address this increase in antifungal resistance. Although ibrexafungerp has similar mechanisms of action, it is different in structure and interacts differently with the target enzyme, resulting in a lower rate of resistance to ibrexafungerp [49]. It demonstrates broad in vitro activity against wild-type azole-resistant and echinocandin-resistant NAC species. It shows efficacy in low pH environments, which suggests its effectiveness against VVC [50]. It is dosed at 300 mg by mouth twice in one day. It does not cause liver toxicity, and its activity is not impacted by a low vaginal pH. It is active against C. glabrata. Ibrexafungerp is contraindicated during pregnancy [51]. Table 2 summarizes the current guidelines for the management of VVC.
9. Conclusions
In summary, RVVC remains an important clinical and global public health challenge and adversely affects the quality of life of the affected women. The clinical presentation is similar to first-episode VVC but perhaps milder. However, an increasingly higher prevalence of NAC species is being reported among women with VVC. NAC species are invariably resistant to most antifungal agents, such as fluconazole, which are commonly used for the treatment of VVC/RVVC. Therefore, treatment remains a challenge. Alternative treatment includes boric acid and topical amphotericin B; however, they are associated with serious side effects, limiting their use in a significant proportion of patients. Recently, the oral echinocandin ibrexafungerp has been shown to have a significant efficacy against VVC/RVVC and was approved for this indication. RVVC presents a unique area for continued research and development.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Wilkinson, J.S. Some remarks upon the development of epiphytes with the description of new vegetable formation found in connexion with the human uterus. Lancet 1849, 54, 448–451. [Google Scholar]
- Brown, G.D.; Denning, D.W.; Gow, N.A.R.; Levitz, S.M.; Netea, M.G.; White, T.C. Hidden killers: Human fungal infections. Sci. Transl. Med 2012, 4, 165rv13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Denning, D.W.; Kneale, M.; Sobel, J.D.; Rautemaa-Richardson, R. Global burden of recurrent vulvovaginal candidiasis: A systematic review. Lancet Infect. Dis. 2018, 18, e339–e347. [Google Scholar] [CrossRef]
- Sobel, J.D. Recurrent vulvovaginal candidiasis. Am. J. Obs. Gynecol. 2016, 214, 15–21. [Google Scholar] [CrossRef]
- Fidel, P.L., Jr.; Barousse, M.; Espinosa, T.; Ficarra, M.; Sturtevant, J.; Martin, D.H.; Quayle, A.J.; Dunlap, K. An intravaginal line candida challenge in humans leads to new hypotheses for the immunopathogenesis of vulvovaginal candidiasis. Infect. Immun. 2004, 72, 2939–2946. [Google Scholar] [CrossRef] [Green Version]
- Barajas, J.F.; Wehrs, M.; To, M.; Cruickshanks, L.; Urban, R.; McKee, A.; Gladden, J.; Goh, E.-B.; Brown, M.E.; Pierotti, D.; et al. Isolation and characterization of bacterial cellulase Producers for biomass deconstruction. A microbiology laboratory course. J. Microbiol. Biol. Educ. 2019, 20, 50. [Google Scholar] [CrossRef]
- Cole, A.M. Innate host defense of human vaginal and cervical mucosae. In Antimicrobial Peptides and Human Disease. Current Topics in Microbiology and Immunology; Springer: Berlin/Heidelberg, Germany, 2006; Volume 306, pp. 199–230. [Google Scholar]
- Rosati, D.; Bruno, M.; Jaeger, M.; Ten Oever, J.; Netea, M.G. Recurrent Vulvovaginal Candidiasis: An Immunological Perspective. Microorganisms 2020, 8, 144. [Google Scholar] [CrossRef] [Green Version]
- Sobel, J.D.; Faro, S.; Force, R.W.; Foxman, B.; Ledger, W.; Nyirjesy, P.R.; Reed, B.D.; Summers, P.R. Vulvovaginal candidiasis: Epidemiologic, diagnostic, and therapeutic considerations. Am. J. Obs. Gynecol 1998, 178, 203–211. [Google Scholar] [CrossRef]
- Deorukhkar, S.C.; Saini, S.; Mathew, S. Non-albicans Candida infection: An emerging threat. Interdiscip. Perspect. Infect. Dis. 2014, 2014, 615958. [Google Scholar] [CrossRef] [Green Version]
- Pappas, P.G.; Kauffman, C.A.; Andes, D.R.; Clancy, C.J.; Marr, K.A.; Ostrosky-Zeichner, L.; Reboli, A.C.; Schuster, M.G.; Vazquez, J.A.; Walsh, T.J.; et al. Clinical Practice Guideline for the Management of Candidiasis: 2016 Update by the Infectious Diseases Society of America. Clin. Infect. Dis 2016, 62, e1–e50. [Google Scholar] [CrossRef]
- Anderson, M.R.; Klink, K.; Cohrssen, A. Evaluation of vaginal complaints. JAMA 2004, 291, 1368–1379. [Google Scholar] [CrossRef] [PubMed]
- Makanjuola, O.; Bongomin, F.; Fayemiwo, S.A. An update on the roles of non-albicans Candida species in vulvovaginitis. J. Fungi 2018, 4, 121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fidel, P.L.; Vazquez, J.A.; Sobel, J.D. Candida glabrata: Review of epidemiology, pathogenesis, and clinical disease with comparison to C. albicans. Clin. Microbiol. Rev. 1999, 12, 80–96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mayer, F.L.; Wilson, D.; Hube, B. Candida albicans pathogenicity mechanisms. Virulence 2013, 4, 119–128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zangl, I.; Pap, I.J.; Aspock, C.; Schuller, C. The role of Lactobacillus species in the control of Candida via biotrophic interactions. Microb. Cell 2019, 7, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Moyes, D.L.; Richardson, J.P.; Naglik, J. Candida albicans-epithelial interactions and pathogenicity mechanisms: Scratching the surface. Virulence 2015, 6, 338–346. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kalia, N.; Singh, J.; Kaur, M. Microbiota in vaginal health and pathogenesis of recurrent vulvovaginal infections: A critical review. Ann. Clin. Microbiol. Antimicrob. 2020, 19, 5. [Google Scholar] [CrossRef]
- Cauchie, M.; Desmet, S.; Lagrou, K. Candida and its dual lifestyle as a commensal and a pathogen. Res. Microbiol. 2017, 168, 802–810. [Google Scholar] [CrossRef]
- Richardson, J.P.; Willems, H.M.E.; Moyes, D.L.; Shoaie, S.; Barker, K.S.; Tan, S.L.; Palmer, G.E.; Hube, B.; Naglik, J.R.; Peters, B.M. Candidalysin Drives Epithelial Signaling, Neutrophil Recruitment, and Immunopathology at the Vaginal Mucosa. Infect. Immun. 2018, 86, e00645-17. [Google Scholar] [CrossRef] [Green Version]
- Ardizzoni, A.; Wheeler, R.T.; Pericolini, E. It Takes Two to Tango: How a Dysregulation of the Innate Immunity, CoupledWith Candida Virulence, Triggers VVC Onset. Front. Microbiol 2021, 12, 692491. [Google Scholar] [CrossRef]
- Willems, H.M.E.; Ahmed, S.S.; Liu, J.; Xu, Z.; Peters, B.M. Vulvovaginal Candidiasis: A Current Understanding and Burning Questions. J. Fungi 2020, 6, 27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wachtler, B.; Citiulo, F.; Jablonowski, N.; Forster, S.; Dalle, F.; Schaller, M.; Wilson, D.; Hube, B. Candida albicans-epithelial interactions: Dissecting the roles of active penetration, induced endocytosis and host factors on the infection process. PLoS ONE 2012, 7, e36952. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Re, A.C.S.; Martins, J.F.; Cunha-Filho, M.; Gelfuso, G.M.; Aires, C.P.; Gratieri, T. New perspectives on the topical management of recurrent candidiasis. Drug Deliv. Transl. Res. 2021, 11, 1568–1585. [Google Scholar] [CrossRef] [PubMed]
- Ravel, J.; Gajer, P.; Abdo, Z.; Schneider, G.M.; Koenig, S.S.; McCulle, S.L.; Karlebach, S.; Gorle, R.; Russell, J.; Tacket, C.O.; et al. Vaginal microbiome of reproductive-age women. Proc. Natl. Acad. Sci. USA 2011, 108, 4680–4687. [Google Scholar] [CrossRef] [Green Version]
- Valenti, P.; Rosa, L.; Capobianco, D.; Lepanto, M.S.; Schiavi, E.; Cutone, A.; Paesano, R.; Mastromarino, P. Role of Lactobacilli and Lactoferrin in the Mucosal Cervicovaginal Defense. Front. Immunol 2018, 9, 376. [Google Scholar] [CrossRef]
- Lykke, M.R.; Becher, N.; Haahr, T.; Boedtkjer, E.; Jensen, J.S.; Uldbjerg, N. Vaginal, Cervical and Uterine pH in Women with Normal and Abnormal Vaginal Microbiota. Pathogens 2021, 10, 90. [Google Scholar] [CrossRef]
- Miller, E.A.; Beasley, D.E.; Dunn, R.R.; Archie, E.A. Lactobacilli Dominance and Vaginal pH: Why Is the Human Vaginal Microbiome Unique? Front. Microbiol. 2016, 61, 607–608. [Google Scholar] [CrossRef]
- Bauters, T.G.; Dhont, M.A.; Temmerman, M.I.; Nelis, H.J. Prevalence of vulvovaginal candidiasis and susceptibility to fluconazole in women. Am. J. Obs. Gynecol 2002, 187, 569–574. [Google Scholar] [CrossRef]
- Sobel, J.D.; Wiesenfeld, H.C.; Martens, M.; Danna, P.; Hooton, T.M.; Rompalo, A.; Sperling, M.; Livengood, C., 3rd; Horowitz, B.; Von Thron, J.; et al. Maintenance fluconazole therapy for recurrent vulvovaginal candidiasis. N. Engl. J. Med. 2004, 351, 876–883. [Google Scholar] [CrossRef]
- Blostein, F.; Levin-Sparenberg, E.; Wagner, J.; Foxman, B. Recurrent vulvovaginal candidiasis. Ann. Epidemio. 2017, 27, 575–582. [Google Scholar] [CrossRef]
- Workowski, K.A.; Bolan, G.A. Sexually transmitted diseases treatment guidelines. MMWR Recomm. Rep. Morb. Mortal. Wkly. Rep. Recomm. Rep. 2015, 64, 1–137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gonçalves, B.; Ferreira, C.; Alves, C.T.; Henriques, M.; Azeredo, J.; Silva, S. Vulvovaginal candidiasis: Epidemiology, microbiology and risk factors. Crit. Rev. Microbiol. 2016, 42, 905–927. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lema, V.M. Recurrent Vulvo-Vaginal Candidiasis: Diagnostic and Management Challenges in a Developing Country Context. Obs. Gynecol. Int. J. 2017, 7, 260. [Google Scholar] [CrossRef]
- Schoch, C.L.; Seifert, K.A.; Huhndorf, S.; Robert, V.; Spouge, J.L.; Levesque, C.A.; Chen, W. Fungal Barcoding Consortium. Nuclear ribosomal internal transcribed spacer (ITS) region as a universal DNA barcode marker for Fungi. Proc. Natl. Acad. Sci. USA 2012, 109, 6241–6246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, R. A Moldy Application of MALDI: MALDI-ToF Mass Spectrometry for Fungal Identification. J. Fungi 2019, 5, 4. [Google Scholar] [CrossRef] [Green Version]
- Gulati, M.; Nobile, C.J. Candida albicans biofilms: Development, regulation, and molecular mechanisms. Microbes Infect. 2016, 18, 310–321. [Google Scholar] [CrossRef] [Green Version]
- Walker, S.S.; Xu, Y.; Triantafyllou, I.; Waldman, M.F.; Mendrick, C.; Brown, N.; Mann, P.; Chau, A.; Patel, R.; Bauman, N.; et al. Discovery of a novel class of orally active antifungal beta-1,3-D-glucan synthase inhibitors. Antimicrob. Agents Chemother. 2011, 55, 5099–5106. [Google Scholar] [CrossRef] [Green Version]
- Ghannoum, M.; Arendrup, M.C.; Chaturvedi, V.P.; Lockhart, S.R.; McCormick, T.S.; Chaturvedi, S.; Berkow, E.L.; Juneja, D.; Tarai, B.; Azie, N.; et al. Ibrexafungerp: A novel oral Triterpenoid antifungal in development for the treatment of Candida auris infections. Antibiotics 2020, 9, 539. [Google Scholar] [CrossRef]
- Prutting, S.; Cerveny, J. Boric acid vaginal suppositories: A brief review. Infect. Dis. Obstet. Gynaecol. 1998, 6, 191–194. [Google Scholar] [CrossRef]
- Sobel, J.D.; Chaim, W.; Nagappan, V.; Leaman, D. Treatment of vaginitis caused by Candida glabrata: Use of topical boric acid and flucytosine. Am. J. Obs. Gynecol. 2003, 189, 297–1300. [Google Scholar] [CrossRef] [Green Version]
- Marchaim, D.; Lemanek, L.; Bheemreddy, S.; Kaye, K.S.; Sobel, J.D. Fluconazole-resistant Candida albicans vulvovaginitis. Obs. Gynecol. 2012, 120, 1407–1414. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Phillips, A.J. Treatment of non-albicans Candida vaginitis with amphotericin B vaginal suppositories. Am. J. Obs. Gynecol. 2005, 192, 2009–2012. [Google Scholar] [CrossRef] [PubMed]
- Ramage, G.; Rajendran, R.; Sherry, L.; Williams, C. Fungal biofilm resistance. Int. J. Microbiol. 2012, 2012, 528521. [Google Scholar] [CrossRef] [PubMed]
- Falagas, M.E.; Betsi, G.I.; Athanasiou, S. Probiotics for prevention of recurrent vulvovaginal candidiasis: A review. J. Antimicrob. Chemother. 2006, 58, 266–272. [Google Scholar] [CrossRef] [Green Version]
- Gardiner, G.E.; Heinemann, C.; Baroja, M.L.; Bruce, A.W.; Beuerman, D.; Madrenas, J.; Reid, G. Oral Administration of the Probiotic Combination Lactobacillus Rhamnosus GR-1 and L. Fermentum RC-14 for Human Intestinal Applications. Int. Dairy J. 2002, 12, 191–196. [Google Scholar] [CrossRef]
- Alexander, B.D.; Pfeiffer, C.D.; Jimenez-Ortigosa, C.; Catania, J.; Booker, R.; Castanheira, M.; Messer, S.A.; Perlin, D.S.; Pfaller, M.A. Increasing echinocandin resistance in Candida glabrata: Clinical failure correlates with FKS mutations and elevated minimum inhibitory concetrations. Clin. Infect. Dis 2013, 56, 1724–1732. [Google Scholar] [CrossRef] [Green Version]
- Beyda, N.D.; John, J.; Kilic, A.; Alam, M.J.; Lasco, T.M.; Garey, K.W. FKS mutant Candida glabrata: Risk factors and outcomes in patients with candidemia. Clin. Infect. Dis 2014, 59, 819–825. [Google Scholar] [CrossRef] [Green Version]
- Jimenez-Ortigosa, C.; Perez, W.B.; Angulo, D.; Borroto-Esoda, K.; Perlin, D.S. Novo acquisition of resitance to SCY-078 in Candida glabrata involves FKS mutation that both overlap and are distinct from those conferring echinocandin resistance. Chemother. Antimicrob. Agents 2017, 61, e00833-17. [Google Scholar] [CrossRef] [Green Version]
- Larkin, E.L.; Long, L.; Isham, N.; Borroto-Esoda, K.; Barat, S.; Angulo, D.; Wring, S.; Ghannoum, M. A novel 1,3-Beta-d-Glucan inhibitor, Ibrexafungerp (formerly SCY-078), shows potent activity in the lower pH environment of vulvovaginitis. Antimicrob. Agents Chemother. 2019, 63, e02611-18. [Google Scholar] [CrossRef] [Green Version]
- Phillips, N.A.; Bachmann, G.; Haefner, H.; Martens, M.; Stockdale, C. Topical Treatment of Recurrent Vulvovaginal Candidiasis: An Expert Consensus. Women’s Health Reports 2021, 3, 38–42. [Google Scholar] [CrossRef]
- Guideline Development Group Cara Saxon Lead Author; Edwards, A.; Rautemaa-Richardson, R.; Owen, C.; Nathan, B.; Palmer, B.; Wood, C.; Ahmed, H.; Ahmad, S.; Patient Representatives, M.F.; et al. British association for sexual health and HIV national guideline for the management of vulvovaginal candidiasis (2019). Int. J. STD AIDS 2020, 31, 1124–1144. [Google Scholar]
Figure 1.
Diagnostic algorithm for Candida vulvovaginitis. MALD-ToF MS, matrix-assisted laser desorption time-of-flight mass spectrometer; C & S, culture and sensitivity; NAAT, nucleic acid amplification tests.
Figure 1.
Diagnostic algorithm for Candida vulvovaginitis. MALD-ToF MS, matrix-assisted laser desorption time-of-flight mass spectrometer; C & S, culture and sensitivity; NAAT, nucleic acid amplification tests.


{kind=link}
Table 1.
Summary of antifungal classes used in the treatment of Candida vulvovaginitis.
| Antifungal Class (Example) | Mechanism of Action | Adverse Events | Resistance |
|---|---|---|---|
| Azoles (clotrimazole, fluconazole) [37] | Impaired ergosterol synthesis due to inhibition of 14-α-lanosterol demethylase | Anaphylaxis, phototoxicity, cardiomyopathy, gastrointestinal disturbances. | Mutation in ERG11, the gene coding for 14-α-lanosterol demethylase. |
| Echinocandins [38,39] (ibrexafungerp) | Inhibition of 1,3-β-D-glucan synthesis in fungal cell wall resulting in loss of structural integrity, osmotic instability, and cell death. | Hepatic toxicity | Mutations in glucan synthase complex genes. |
| Polyenes (Nystatin, Amphotericin B) [34] | Binds to ergosterol in fungi membranes to form pore and increase membrane permeability. | Nystatin; well-tolerated. Amphotericin B. Nephrotoxicity, hepatic toxicity | Resistance may be caused by replacement of ergosterol with precursor sterols. |
| Others: Boric acid [40] | Exact mechanism is unknown. Vaginal acidification causes cell membrane dysfunction. | Toxicity when systemically absorbed. |
| Intervention | Vulvovaginal Candidiasis | Recurrent Vulvovaginal Candidiasis |
|---|---|---|
| Recommended oral regimen | Non-pregnant: Fluconazole capsule 150 mg as a single dose. If oral therapy is contraindicated, clotrimazole pessary 500 mg as a single dose, intravaginally. Pregnancy: Clotrimazole pessary 500 mg PV at night for up to 7 nights. NAC spp and azole resistance: Nystatin pessaries 100,000 units intravaginally every night for 14 days | Non-pregnant: Induction: Fluconazole 150 mg orally every 72 h × 3 doses. Maintenance: Fluconazole 150 mg orally once a week for 6 months. Pregnancy: Induction: topical imidazole therapy for up to 10–14 days according to symptomatic response. Maintenance: clotrimazole pessaries 500 mg intravaginally weekly. NAC spp and azole resistance: Nystatin pessaries 100,000 unit intravaginally at night for 14 nights/month for 6 months. |
| Alternative regimens | Non-pregnant: Clotrimazole vaginal cream (10%) 5 g as a single dose OR Clotrimazole pessary 200 mg intravaginally at night for 3 consecutive nights OR Econazole pessary 150 mg intravaginally as a single dose or 150 mg intravaginally at night for 3 consecutive nights. OR Fenticonazole capsule intravaginally as a single dose 600 mg or 200 mg intravaginally at night for 3 consecutive days. OR Itraconazole 200 mg orally twice daily for 1 day PO. OR Miconazole capsule 1200 mg intravaginally as a single dose, or 400 mg intravaginally at night for 3 consecutive nights. OR Miconazole vaginal cream (2%) 5 g intravaginally at night for 7 consecutive nights. Pregnancy: Clotrimazole vaginal cream (10%) 5 g at night for up to 7 nights. OR Clotrimazole pessary 200 mg or 100 mg intravaginally at night for 7 nights OR Econazole pessary 150 mg intravaginally at night for 7 consecutive nights. OR Miconazole pessary 1200 mg or 400 mg intravaginally at night for 7 consecutive nights. OR Miconazole vaginal cream (2%) 5 g intravaginally at night for 7 consecutive nights. NAC spp and azole resistance: Boric acid suppositories 600 mg intravaginally at night for 14 nights. OR Amphotericin B vaginal suppositories 50 mg intravaginally at night for 14 nights. OR Flucytosine 5 g cream or 1 g pessary with amphotericin or nystatin intravaginally at night for 14 nights. | Non-pregnant: Induction: topical imidazole therapy can be increased to 7–14 days according to symptomatic response. Maintenance for 6 months: Clotrimazole pessary 500 mg intravaginally once a week. Itraconazole 50–100 mg orally daily. NAC spp and azole resistance: Consider 14 nights per month of the alternative regimens. |
Abbreviations: NAC spp, non-albicans Candida species.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Nsenga, L.; Bongomin, F. Recurrent Candida Vulvovaginitis. Venereology 2022, 1, 114-123. https://doi.org/10.3390/venereology1010008
AMA Style
Nsenga L, Bongomin F. Recurrent Candida Vulvovaginitis. Venereology. 2022; 1(1):114-123. https://doi.org/10.3390/venereology1010008
Chicago/Turabian StyleNsenga, Lauryn, and Felix Bongomin. 2022. "Recurrent Candida Vulvovaginitis" Venereology 1, no. 1: 114-123. https://doi.org/10.3390/venereology1010008