
A Preliminary Predictive Model for Proliferative Lupus Nephritis in Juvenile Systemic Lupus Erythematosus


1
Department of Paediatrics, Faculty of Medicine, Universiti Teknologi MARA (UiTM), Sungai Buloh 47000, Malaysia
2
Institute for Research, Development and Innovation, International Medical University, Bukit Jalil, Kuala Lumpur 57000, Malaysia
3
Faculty of Medicine, International Medical University, Bukit Jalil, Kuala Lumpur 57000, Malaysia
4
Paediatric Rheumatology Unit, Selayang Hospital, Batu Caves 68100, Malaysia
*
Authors to whom correspondence should be addressed.
Rheumato 2023, 3(1), 86-97; https://doi.org/10.3390/rheumato3010007
Submission received: 19 December 2022
/
Revised: 13 February 2023
/
Accepted: 17 February 2023
/
Published: 22 February 2023
(This article belongs to the Special Issue The Kidneys in Autoimmune Disease: From Basic Mechanisms to Clinical Outcomes)
Abstract
:Proliferative lupus nephritis, which is diagnosed by renal biopsy, has significant impact on the treatment choices and long-term prognosis of juvenile SLE (jSLE). Renal biopsies are however not always possible or available, thus leading to an ongoing search for alternative biomarkers. This study aimed to develop a clinical predictive machine learning model using routine standard parameters as an alternative tool to evaluate the probability of proliferative lupus nephritis (ISN/RPS Class III or IV). Data were collected retrospectively from jSLE patients seen at Selayang Hospital from 2004 to 2021. A total of 22 variables including demographic, clinical and laboratory features were analyzed. A recursive feature elimination technique was used to identify factors to predict pediatric proliferative lupus nephritis. Various models were then used to build predictive machine learning models and assessed for sensitivity, specificity and accuracy. There were 194 jSLE patients (165 females), of which 111 had lupus nephritis (54 proliferative pattern). A combination of 11 variables consisting of gender, ethnicity, fever, nephrotic state, hypertension, urine red blood cells (RBC), C3, C4, duration of illness, serum albumin, and proteinuria demonstrated the highest accuracy of 79.4% in predicting proliferative lupus nephritis. A decision-tree model performed the best with an AROC of 69.9%, accuracy of 73.85%, sensitivity of 78.72% and specificity of 61.11%. A potential clinically useful predictive model using a combination of 11 non-invasive variables to collectively predict pediatric proliferative lupus nephritis in daily practice was developed.
1. Introduction
Systemic lupus erythematosus (SLE) is a chronic multisystem autoimmune disease with a juvenile onset (before the age of 18 years) in only 10–20% of all patients. Juvenile SLE is associated with significant morbidity, mortality and long-term organ damage [1,2,3]. It is a rare disease with an estimated incidence of approximately 0.3 to 2.2 per 100,000 children years and a prevalence rate ranging widely between 3.3 and 9.7 per 100,000 children and adolescents [3,4,5,6,7]. There are distinct variations amongst different ethnicities worldwide, with the highest prevalence reported among the African American, Hispanic and Asian populations [1,2,8,9,10]. In addition, children and adolescents with SLE present with more severe disease predominantly affecting major organs and tend to run a more aggressive disease course [11,12,13,14,15,16]. The clinical presentation of jSLE is also highly heterogeneous with distinct differences when compared with adult-onset SLE. The organ systems more commonly affected in jSLE include cutaneous, haematological, renal and central nervous systems [1,2,4,17,18,19,20]. This higher prevalence of renal and neurological involvement in children also accounts for the higher disease activity seen in jSLE, especially in non-Caucasian populations [1,8,21,22].
The kidneys are one of the major organs affected in both juvenile and adult forms of SLE, and this affects up to 40–70% of all SLE patients. This renal involvement is correlated with a higher morbidity and damage accrual, as well as mortality [1,12,17,19,23,24]. The higher damage accrual in lupus nephritis occurs not only via glomerular and tubulointerstitial lesions but also from vascular involvement [25]. Even a single episode of lupus nephritis occurring in early life can result in podocyte and nephron loss, exacerbating normal age-related nephron changes [25]. This in turn potentiates the risk of progression to end-stage renal failure in about 15% of children with lupus nephritis [24]. Additionally, premature cardiovascular mortality has been reported in 10–26% of adult patients with lupus nephritis, occurring as early as 5 years after diagnosis. Lupus nephritis is also associated with progressive deterioration in the quality of life within 6–12 months after the initiation of dialysis [25,26,27,28]. Therefore, early, prompt and optimal treatment of lupus nephritis is essential to prevent further morbidities, the accrual of damage and possible mortality.
Current lupus nephritis treatment is primarily guided by the histopathological classification of renal involvement according to the International Society of Nephrology, Renal Pathology Society (ISN/RPS) [29,30]. Patients identified with proliferative lupus nephritis (Class III and IV) generally have a poorer prognosis and are subjected to more intensive immunosuppressive therapies [23,30,31]. Therefore, all patients with features suggestive of renal involvement should undergo further investigations including a renal biopsy to determine the exact nature and extent of the disease. Unfortunately, the indications for renal biopsy, especially the amount of proteinuria, is yet to be determined for children, although it is well established in adults [24].
In addition, access to renal biopsy or the corresponding histopathological services may not be available to children in remote regions, low-income countries or communities in conflict zones [32,33]. Renal biopsies may also be contraindicated due to inherent renal defects such as the presence of only one kidney, or medical conditions with uncontrolled hypertension or coagulopathy either due to disease or from concomitant drugs. Under such circumstances, non-invasive predictive machine learning models will be an extremely useful substitute to identify those with proliferative lupus nephritis who require the most urgent or more aggressive immunosuppressive treatments. There have been some attempts to develop such models amongst patients with adult-onset SLE, but the data remain limited and such research is still lacking in juvenile SLE [34].
The aim of our study was to develop a predictive machine learning model to identify jSLE patients with a significant risk of developing proliferative lupus nephritis. This will facilitate early effective therapy and the avoidance of significant morbidity whilst improving outcomes in the future. A robust predictive model will reduce the reliance on invasive renal biopsy and would be especially crucial in poorly resourced countries without access to such expertise.
2. Materials and Methods
This was a retrospective study conducted at the Pediatric Rheumatology Unit, Selayang Hospital, Selangor, Malaysia, which is currently the sole pediatric rheumatology referral center for patients from the whole country. The records of all children with jSLE seen at this center from January 2004 to December 2021 were reviewed. Patients were included in our study if they were first diagnosed with SLE before the age of 18 years at our center, fulfilled the Systemic Lupus International Collaborating Clinics (SLICC) criteria retrospectively [35] and had a duration of follow-up of at least 6 months at our center. Data was collated from the patients’ electronic medical records (EMR) and included demographic data, date of onset of symptoms, date of initial SLE diagnosis, disease duration, clinical features (present or absent) and laboratory findings (normal or abnormal) at diagnosis, and renal biopsy results.
Ethical approval for this study was obtained from the Medical Research & Ethics Committee Malaysia (NMRR-20-2549-57246) and we received approval for a waiver of informed consent.
2.1. Data Pre-Processing
This study used the demographic, clinical and laboratory data of jSLE patients at Selayang Hospital to build, train and evaluate classifier models for predicting the risk of proliferative lupus nephritis in children with SLE. A total of 22 features including demographic characteristics, clinical characteristics and laboratory investigations were combined into a single dataset for feature selection. After removing instances with missing values in at least one of these features, 194 patients were retained for feature selection, model training and evaluation. The outcome variable with non-proliferative or no lupus nephritis was encoded as category 0 and proliferative lupus nephritis as category 1. ‘No lupus nephritis’ was defined as patients who did not have any renal involvement. The classification into ‘proliferative’ or ‘non-proliferative lupus nephritis’ was based on histopathological changes (ISN/RPS Classification) found on renal biopsies. Proliferative lupus nephritis involved Class III or IV changes on renal biopsy whilst non-proliferative was either Class I, II or purely class V. Class III or IV coexisting with Class V was classified as proliferative.
2.2. Feature Selection: Support Vector Machine Classification (SVM)-Recursive Feature Elimination (RFE)
The RFE is a feature selection method that was used to identify important features and then build various models with different feature subsets of a dataset. The selection process involved selecting significant features and removing the weaker ones until it had achieved the optimum number needed for peak performance. In this study, the caret package in R-studio (which is a classification and regression training function) was used to carry out SVM-RFE, which is an SVM-based feature selection algorithm. SVM is a supervised learning model used for classification. The algorithm was configured to explore all possible subsets of the features from demographic, clinical and laboratory test datasets. Hence, only participants (n = 194) that had complete data for all three datasets (demographic, clinical and laboratory test) were included in the analysis.
The SVM-RFE eliminated features that were least important in iterations and considered the interdependencies with other features and also the two categories (no lupus nephritis and non-proliferative lupus nephritis versus proliferative lupus nephritis). To determine the optimal number of features, 10-fold cross-validation with three repeats was used and the results were visualized using a plot showing the accuracy of the different feature subset sizes. The final feature subset was selected from the iteration in which SVM achieved the best classification performance.
2.3. Model Training and Parameter Tuning
The dataset containing the final feature subset was first randomly split into a 70:30 ratio. Seventy percent of the dataset was used as the training dataset to train the model and the remaining 30% of the dataset was used to evaluate the accuracy of the model. The training dataset was used to train five machine learning models, namely support vector machine (SVM) with linear kernel, support vector machine (SVM) with radial kernel, K nearest neighbors (Knn), random forest (RF), and decision-tree Rpart (Rpart). All these five models were developed using the R ‘caret’ and ‘e1071’ packages.
Using the training dataset and the 10-fold cross-validation method, the hyperparameters of each model were tuned to obtain the set of optimal hyperparameters with the ‘train’ function in the ‘caret’ package. The package by default created a grid of tuning parameters with a grip size of 3^p (p is the number of tuning parameters). This process was repeated three times and the optimal values (values that maximize the model accuracy) were automatically chosen as the model hyperparameters.
2.4. Model Evaluation
The performance of each of these models with the optimal set of hyperparameters was evaluated on the test dataset. The accuracy (percentage of correct predictions), sensitivity and specificity were calculated. The performance of the models was visualized using the area under the receiver operating characteristic curve (AROC) and confusion matrixes. The modes were then evaluated on the test set based on sensitivity, specificity and area under curve (AUC).
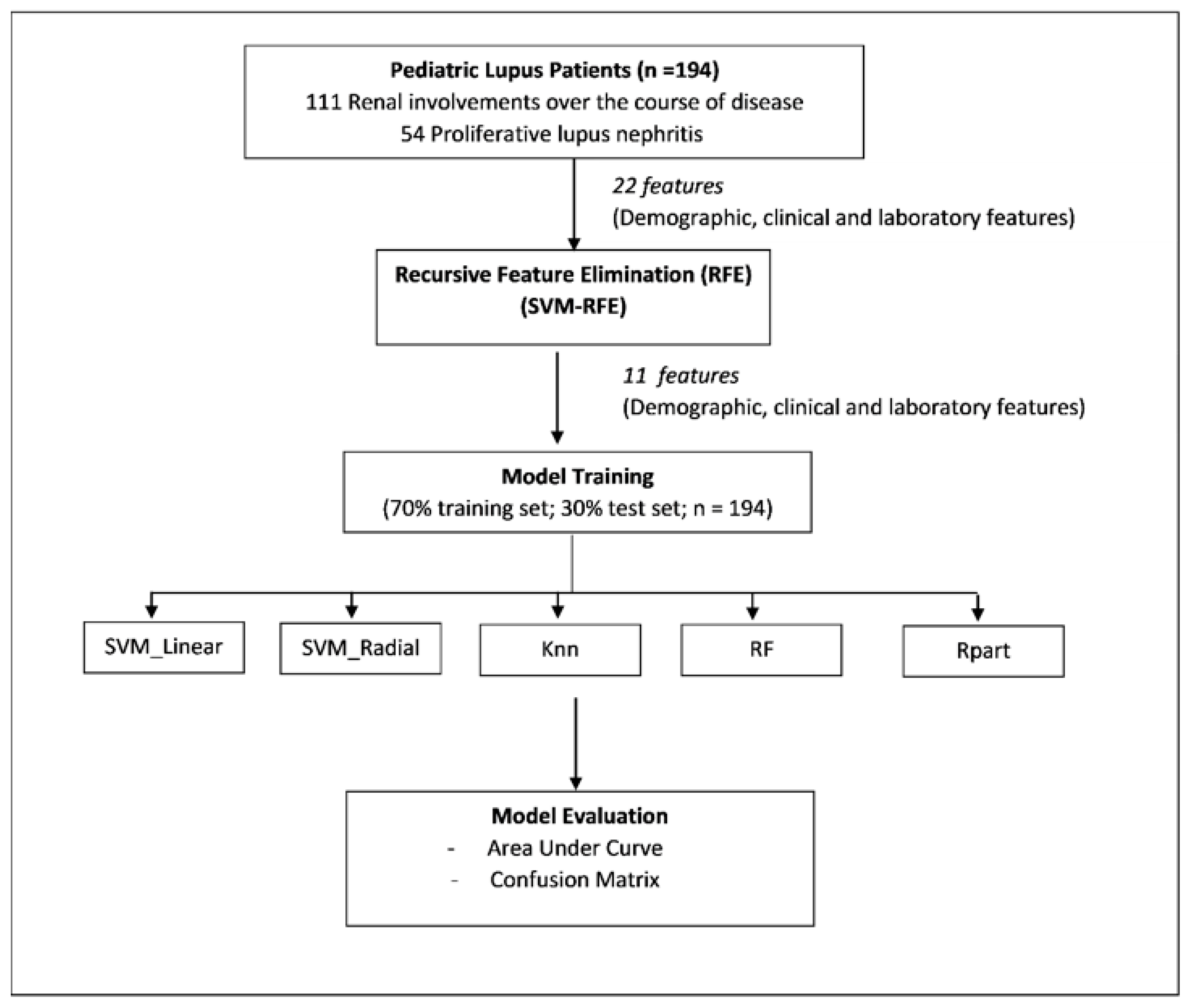
The process for the feature selection, model training and evaluation is summarized in Figure 1.
3. Results
3.1. Demographic and Characteristic of Study Population
There was a total of 224 jSLE patients, of which 194 had complete datasets and were included into the study. The majority (68.9%) were of Malay ethnicity and 165 (85.5%) were females, with an overall female: male ratio of 5.5:1. The median age at diagnosis was peripubertal, at 11.7 years, and there was a marked gender variation with age. The female preponderance increased with advancing age, with the teenage group of 13–18 years of age having an extremely high female: male ratio of 23.4:1. Of the 194 patients, 111 patients had renal involvement over the course of their disease, of which 54 patients were confirmed to have proliferative lupus nephritis. The demographic characteristics of the study population are summarized in Table 1.
3.2. Clinical Features and Major Organ Manifestations at Presentation
The most frequent presenting clinical features were fever (89.1%), vasculitic rash (69.9%) and fatigue (68.4%).
At diagnosis, 34.2% had renal involvement. Other major organs affected included the liver (24.9%), central nervous system and heart (both 12.9%). The frequency of clinical features at presentation are shown in Table 2.
The prevalence of baseline clinical and immunological symptoms, as satisfied by the SLICC classification criteria, is summarized below in Table 3. The most frequently observed criteria at diagnosis were ANA (98.4%), followed by low complement levels (88.6%) and a positive direct Coombs test result (76.7%). The least frequently observed criteria were antiphospholipid antibodies (11.9%).
3.3. Determination of Variables That Could Predict Proliferative Lupus Nephritis among the jSLE Cases
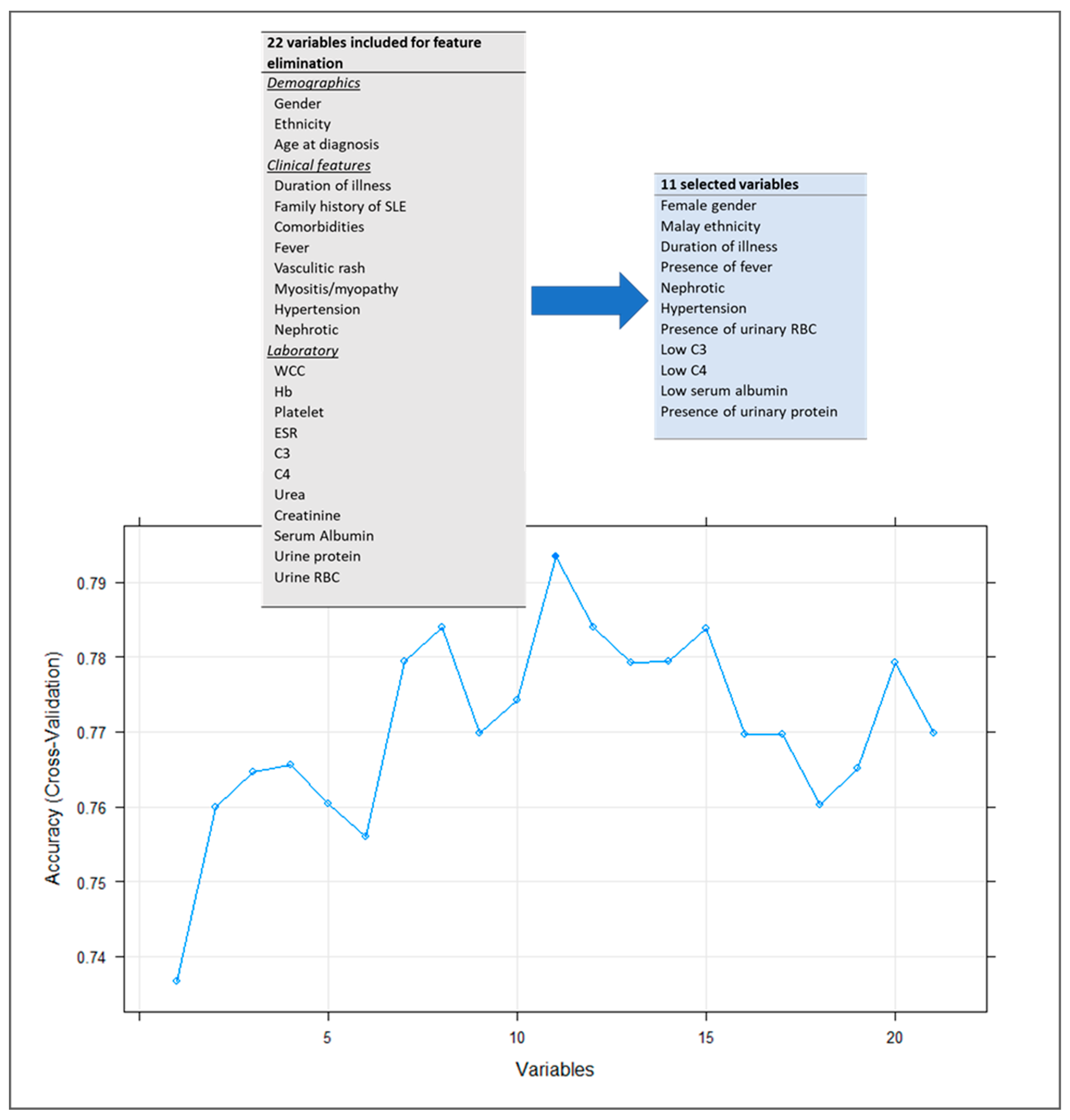
A total of 22 variables, including demographic, clinical and laboratory features, were included for feature elimination to identify variables that were not required in predicting proliferative lupus nephritis in patients with jSLE. Figure 2 indicates that a combination of 11 variables, namely (1) gender, (2) ethnicity, (3) fever, (4) nephrotic (defined as clinically edematous state), (5) hypertension, (6) Urine RBC, (7) Complement 3 (C3), (8) Complement 4 (C4), (9) duration of illness, (10) serum albumin, and (11) urine protein collectively, had the highest accuracy of 79.4% in predicting proliferative lupus nephritis. Clinical features such as fever, nephrotic, hypertension, urine RBC and urine protein are categorized as present or absent. Laboratory findings such as complement 3, complement 4 and serum albumin are categorized as normal or abnormal.
These 11 variables were then used to train and test five machine leaning models, namely support vector machine (SVM) with linear kernel, support vector machine (SVM) with radial kernel, K nearest neighbors (Knn), random forest (RF), and decision-tree Rpart (Rpart), to predict proliferative lupus nephritis. The performance evaluations of these models are summarized in Table 4.
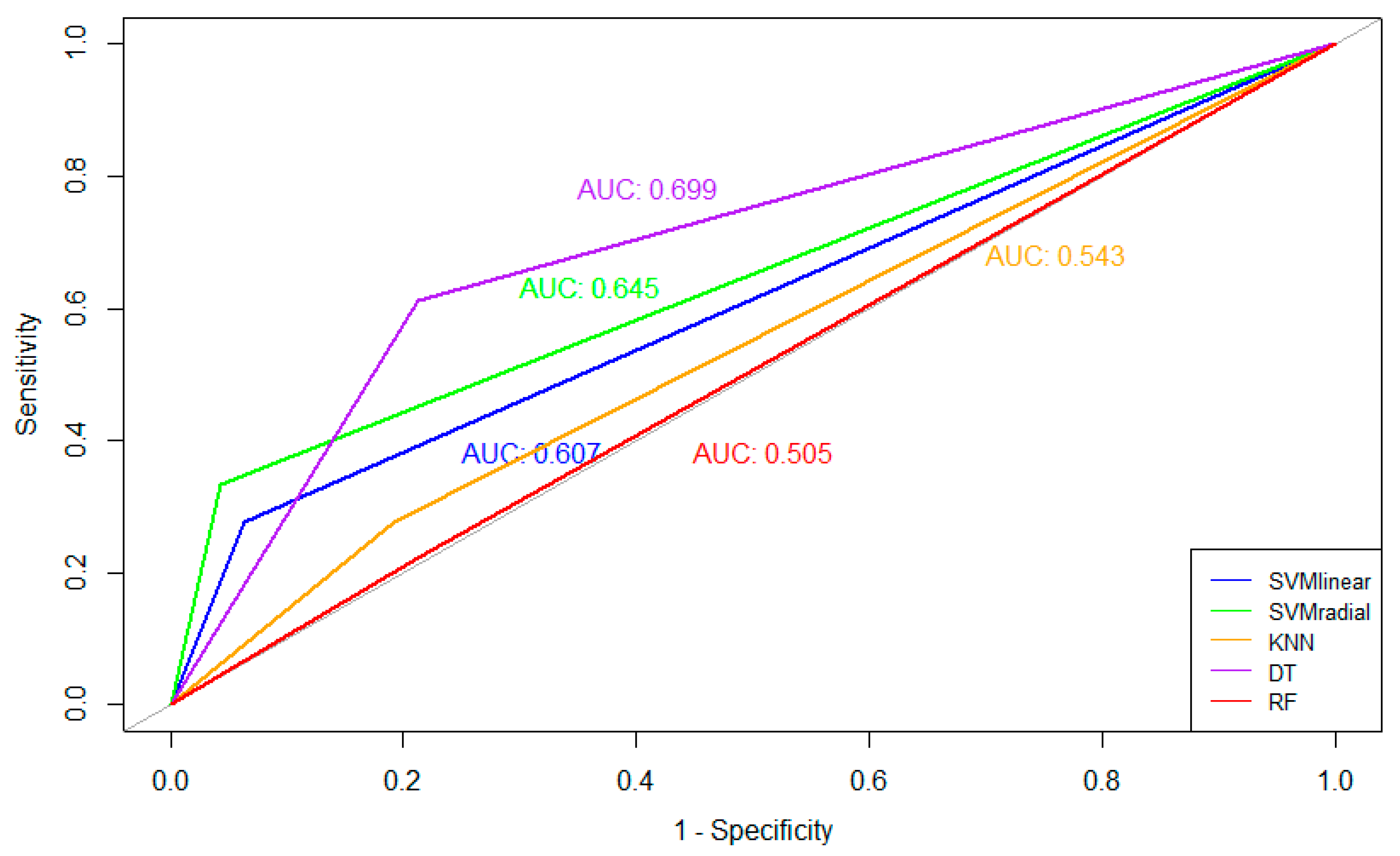
During the process of testing, the models SVM Radial and RF had an accuracy of 78.46% for predicting proliferative lupus nephritis, but the specificity of these models was low (33.33% and 50.00%, respectively). The SVM Radial model had the highest sensitivity (95.74%) in predicting proliferative lupus nephritis, but the specificity was the second lowest (33.33%). Overall, the decision-tree Rpart model performed the best by having high accuracy (73.85%), specificity (78.72%) and sensitivity (61.11%) when predicting proliferative lupus nephritis. Figure 3 shows that the decision-tree Rpart model performed the best based on the highest AROC value (69.9%), followed by the SVM Radial model, the SVM-Linear model and the knn model. The random forest model gave the lowest AROC at 50.5%. The confusion matrixes of all these five models are presented in Figure 4.
4. Discussion
This study is important because it provides a preliminary machine learning model that can be used to predict proliferative lupus nephritis in children. Renal involvement is common in SLE (40–70%) and affects jSLE patients both at onset and during the course of disease [1,12,17,19,23,24]. It is important as it adversely affects the long-term prognosis and survival of jSLE patients [14,18,21,36,37,38]. The current gold standard for diagnosis of lupus nephritis is a renal biopsy, and the histopathological classification is used to guide treatment all around the world. However, this invasive procedure may be unattainable under certain circumstances, such as uncontrolled hypertension and coagulopathy, or due to external situations such as war or in resource-poor countries [32,33].
It is therefore not surprising that there have been numerous attempts to use non-invasive biomarkers to predict lupus nephritis activity and renal flares. Some of the commonly used biomarkers include serum creatinine, urinary protein excretion, complement levels and anti-dsDNA antibody levels. However, these biomarkers are imprecise and lack a robust model to differentiate between proliferative and non-proliferative renal lesions [23,39,40]. Recent research has also identified other promising serum and urinary biomarkers such as NGAL (neutrophil gelatinase-associated lipocalin), MCP-1 (monocyte chemoattractant protein), TWEAK (tumor necrosis factor-like weak inducer of apoptosis), VCAM (vascular cell adhesion molecule), adiponectin, hemopexin, kidney injury molecule-1 and HMGB1 (high mobility group box protein 1) [23,41]. However, these biomarkers are still experimental, and any future potential use will likely be hindered by the cost of these tests as well as the lack of availability, especially in low-resource countries.
In our study, we similarly found that previously reported individual biomarkers such as complements and serum albumin were useful to predict lupus nephritis [23,40,42]. However, the robustness of this predictive model was enhanced by using a combination of 11 variables selected by machine learning in our study, when compared with using single biomarkers alone. In addition, these 11 variables consisted of routine standard clinical and laboratory parameters, which are typically obtained in the management of any child with jSLE. All of these biomarkers, with the exception of complement levels, are readily available in most healthcare facilities, including those in resource-limited countries. Our model specifically did not include the utility of anti-dsDNA antibodies, although this is a known biomarker for lupus nephritis. This investigation is often not readily available or the results are not available on an urgent basis in many countries, especially in those with low resources [23,40].
In evaluating these predictive machine learning models, we found that the decision-tree Rpart model provides the best performance in terms of balancing both specificity and sensitivity in predicting the presence of proliferative lupus nephritis. This distinction between non-proliferative and proliferative lupus nephritis is important as it differentiates those who might require more than standard immune suppression, including more potent immunosuppressives or even biologic agents to ensure optimal outcomes [20,30,31].
4.1. Strengths
The main strength of this model is that it has the potential utility in routine clinical practice to assess the risk of proliferative lupus nephritis in children using readily available variables. It can help clinicians to objectively evaluate the kidneys in addition to using standard disease activity measures in any patient with biochemical or clinical signs indicative of active lupus nephritis. This additional information of predicting proliferative lupus nephritis enables clinicians to make better informed decisions on treatment, thus potentially improving outcome and survival [23,30,31]. Even in settings where renal biopsies are easily available, this model can help to provide a more precise indication on when to perform a renal biopsy, especially in children where the indications are not well established [24]. In resource-poor settings, this model can potentially be used to identify proliferative lupus nephritis and guide treatment decisions in place of a renal biopsy, which may not be available. In addition, in places with inadequate access to specialty services, such as conflict zones or remote areas, this model could also help non-specialty doctors with potentially lifesaving treatment decisions.
4.2. Limitations
The limitation of this predictive model is that it is useful for risk assessment and clinical decisions that are only applicable to a time point during the disease course. It cannot be used to predict the long-term course and renal outcomes of jSLE, particularly whether a patient might develop proliferative lupus nephritis in the future, as this model was built on data obtained at the initial diagnosis of a disease that tends to evolve over time. Furthermore, not all patients with renal involvement had a renal biopsy, including those who had a mild involvement that initially responded to steroids, and this could potentially cause a bias in the overall modelling. In addition, this model requires the presence of all 11 variables in a patient, failing which this model cannot work.
4.3. Recommendations
This model could be further improved by obtaining data over a longer time frame and incorporating the changes in the biomarkers over the course of the disease. Additionally, the sensitivity and specificity of this preliminary model is limited by the small sample size. Further refining and validation of this model needs to be performed in other paediatric cohorts to improve its precision and sensitivity for disease prediction. Future studies should also be conducted prospectively to ensure the completeness of data variables. This may lead to the introduction of other potentially important variables that were not considered in this study.
5. Conclusions
A potential clinically useful predictive model was successfully developed by machine learning, featuring a combination of 11 non-invasive common risk factors, to identify jSLE patients at risk of proliferative lupus nephritis in daily practice. This preliminary model has important clinical utility, especially in circumstances where a renal biopsy is either contraindicated or unavailable in low-resource countries or regions with poor access to specialty services. Further prospective validation of this preliminary model is planned.
Author Contributions
Conceptualization, S.C.L., E.W.L.C. and S.P.T.; Data curation, S.S.M.; Formal analysis, S.C.L. and E.W.L.C.; Methodology, S.C.L., E.W.L.C. and S.P.T.; Writing—original draft, S.C.L., E.W.L.C. and S.P.T.; Writing—review and editing, S.C.L. and S.P.T. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study received approval from the Medical Research & Ethics Committee Malaysia (NMRR-20-2549-57246).
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
The authors would like to thank the Director General, Ministry of Health Malaysia for granting the use of the Ministry of Health facilities for the conduct of this research.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Hiraki, L.T.; Benseler, S.M.; Tyrrell, P.N.; Hebert, D.; Harvey, E.; Silverman, E.D. Clinical and Laboratory Characteristics and Long-Term Outcome of Pediatric Systemic Lupus Erythematosus: A Longitudinal Study. J. Pediatr. 2008, 152, 550–556. [Google Scholar] [CrossRef]
- Levy, D.M.; Kamphuis, S. Systemic Lupus Erythematosus in Children and Adolescents. Pediatr. Clin. N. Am. 2012, 59, 345–364. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kamphuis, S.; Silverman, E.D. Prevalence and burden of pediatric-onset systemic lupus erythematosus. Nat. Rev. Rheumatol. 2010, 6, 538–546. [Google Scholar] [CrossRef] [PubMed]
- Watson, L.; Leone, V.; Pilkington, C.; Tullus, K.; Rangaraj, S.; McDonagh, J.E.; Gardner-Medwin, J.; Wilkinson, N.; Riley, P.; Tizard, J.; et al. Disease activity, severity, and damage in the UK juvenile-onset systemic lupus erythematosus cohort. Arthritis Rheum. 2012, 64, 2356–2365. [Google Scholar] [CrossRef]
- Arkachaisri, T. Pediatric Rheumatology in Southeast Asia: Insights from the Singapore Experience. Curr. Rheumatol. Rep. 2010, 13, 117–122. [Google Scholar] [CrossRef]
- Huang, J.L.; Yao, T.C.; See, L.-C. Prevalence of pediatric systemic lupus erythematosus and juvenile chronic arthritis in a Chinese population: A nation-wide prospective population-based study in Taiwan. Ann. Rheum. Dis. 2005, 22, 776–780. [Google Scholar]
- Mackie, F.E.; Kainer, G.; Adib, N.; Boros, C.; Elliott, E.; Fahy, R.; Munro, J.; Murray, K.; Rosenberg, A.; Wainstein, B.; et al. The national incidence and clinical picture of SLE in children in Australia—A report from the Australian Paediatric Surveillance Unit. Lupus 2014, 24, 66–73. [Google Scholar] [CrossRef]
- Hiraki, L.T.; Benseler, S.M.; Tyrrell, P.N.; Harvey, E.; Hebert, D.; Silverman, E.D. Ethnic Differences in Pediatric Systemic Lupus Erythematosus. J. Rheumatol. 2009, 36, 2539–2546. [Google Scholar] [CrossRef]
- Danchenko, N.; Satia, J.A.; Anthony, M.S. Epidemiology of systemic lupus erythematosus: A comparison of worldwide disease burden. Lupus 2006, 15, 308–318. [Google Scholar] [CrossRef]
- Levy, D.M.; Peschken, C.; Tucker, L.; Chédeville, G.; Huber, A.M.; Pope, J.; the Canadian Network for Improved Outcomes in SLE 1000 Faces Investigators; Silverman, E.D. Influence of ethnicity on childhood-onset systemic lupus erythematosus: Results from a multiethnic multicenter Canadian cohort. Arthritis Care Res. 2012, 65, 152–160. [Google Scholar] [CrossRef] [Green Version]
- Tucker, L.; Uribe, A.; Fernández, M.; Vilá, L.; McGwin, G.; Apte, M.; Fessler, B.; Bastian, H.; Reveille, J.; Alarcón, G. Adolescent onset of lupus results in more aggressive disease and worse outcomes: Results of a nested matched case–control study within LUMINA, a multiethnic US cohort (LUMINA LVII). Lupus 2008, 17, 314–322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mina, R.; Brunner, H.I. Pediatric Lupus—Are There Differences in Presentation, Genetics, Response to Therapy, and Damage Accrual Compared with Adult Lupus? Rheum. Dis. Clin. N. Am. 2010, 36, 53–80. [Google Scholar] [CrossRef] [Green Version]
- Glidden, R.S.; Mantzouranis, E.C.; Borel, Y. Systemic lupus erythematosus in childhood: Clinical manifestations and improved survival in fifty-five patients. Clin. Immunol. Immunopathol. 1983, 29, 196–210. [Google Scholar] [CrossRef] [PubMed]
- Mina, R.; Brunner, H.I. Update on differences between childhood-onset and adult-onset systemic lupus erythematosus. Thromb. Haemost. 2013, 15, 218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brunner, H.I.; Gladman, D.D.; Ibañez, D.; Urowitz, M.D.; Silverman, E.D. Difference in disease features between childhood-onset and adult-onset systemic lupus erythematosus. Arthritis Rheum. 2008, 58, 556–562. [Google Scholar] [CrossRef]
- Artim-Esen, B.; Şahin, S.; Çene, E.; Şahinkaya, Y.; Barut, K.; Adrovic, A.; Ozluk, Y.; Kılıçaslan, I.; Omma, A.; Gül, A.; et al. Comparison of Disease Characteristics, Organ Damage, and Survival in Patients with Juvenile-onset and Adult-onset Systemic Lupus Erythematosus in a Combined Cohort from 2 Tertiary Centers in Turkey. J. Rheumatol. 2017, 44, 619–625. [Google Scholar] [CrossRef]
- Gheith, R.E.; El-Gazzar, I.I.; El Fishawy, H.S.; El-Din, A.M.N.; Bahgat, D.M.; Gheita, T.A. Juvenile and juvenile-onset systemic lupus erythematosus patients: Clinical characteristics, disease activity and damage. Egypt. Pediatr. Assoc. Gaz. 2017, 65, 49–53. [Google Scholar] [CrossRef]
- Lee, P.-Y.; Yeh, K.-W.; Yao, T.-C.; Lee, W.-I.; Lin, Y.-J.; Huang, J.-L. The outcome of patients with renal involvement in pediatric-onset systemic lupus—A 20-year experience in Asia. Lupus 2013, 22, 1534–1540. [Google Scholar] [CrossRef]
- Pluchinotta, F.R.; Schiavo, B.; Vittadello, F.; Martini, G.; Perilongo, G.; Zulian, F. Distinctive clinical features of pediatric systemic lupus erythematosus in three different age classes. Lupus 2007, 16, 550–555. [Google Scholar] [CrossRef]
- Lim, S.C.; Chan, W.L.E.; Tang, S.P. Clinical features, disease activity and outcomes of Malaysian children with paediatric systemic lupus erythematosus: A cohort from a tertiary centre. Lupus 2020, 29, 1106–1114. [Google Scholar] [CrossRef]
- Brunner, H.I.; Silverman, E.D.; To, T.; Bombardier, C.; Feldman, B.M. Risk factors for damage in childhood-onset systemic lupus erythematosus: Cumulative disease activity and medication use predict disease damage. Arthritis Rheum. 2002, 46, 436–444. [Google Scholar] [CrossRef] [PubMed]
- Tang, S.; Lim, S.; Arkachaisri, T. Childhood-Onset Systemic Lupus Erythematosus: Southeast Asian Perspectives. J. Clin. Med. 2021, 10, 559. [Google Scholar] [CrossRef] [PubMed]
- Wenderfer, S.E.; Ruth, N.M.; Brunner, H.I. Advances in the care of children with lupus nephritis. Pediatr. Res. 2016, 81, 406–414. [Google Scholar] [CrossRef] [Green Version]
- Oni, L.; Wright, R.D.; Marks, S.; Beresford, M.W.; Tullus, K. Kidney outcomes for children with lupus nephritis. Pediatr. Nephrol. 2020, 36, 1377–1385. [Google Scholar] [CrossRef]
- Anders, H.-J.; Rovin, B. A pathophysiology-based approach to the diagnosis and treatment of lupus nephritis. Kidney Int. 2016, 90, 493–501. [Google Scholar] [CrossRef] [PubMed]
- Yap, D.Y.; Tang, C.S.; Ma, M.K.; Lam, M.F.; Chan, T.M. Survival analysis and causes of mortality in patients with lupus nephritis. Nephrol. Dial. Transplant. 2012, 27, 3248–3254. [Google Scholar] [CrossRef] [Green Version]
- Escárcega, R.O.; Garcia-Carrasco, M.; Jara, L.J.; Cervera, R. Accelerated Atherosclerosis in Systemic Lupus Erythematosus: Perspectives towards Decreasing Cardiovascular Morbidity and Mortality. Lupus 2009, 18, 383–386. [Google Scholar] [CrossRef] [Green Version]
- Sule, S.; Fivush, B.; Neu, A.; Furth, S. Increased Hospitalizations and Death in Patients with ESRD Secondary to Lupus. Lupus 2012, 21, 1208–1213. [Google Scholar] [CrossRef] [Green Version]
- Hachiya, A.; Karasawa, M.; Imaizumi, T.; Kato, N.; Katsuno, T.; Ishimoto, T.; Kosugi, T.; Tsuboi, N.; Maruyama, S. The ISN/RPS 2016 classification predicts renal prognosis in patients with first-onset class III/IV lupus nephritis. Sci. Rep. 2021, 11, 1525. [Google Scholar] [CrossRef]
- Weening, J.J.; D’Agati, V.D.; Schwartz, M.M.; Seshan, S.V.; Alpers, C.E.; Appel, G.B.; Balow, J.E.; Bruijn, J.A.; Cook, T.; Ferrario, F.; et al. The Classification of Glomerulonephritis in Systemic Lupus Erythematosus Revisited. J. Am. Soc. Nephrol. 2004, 15, 241–250. [Google Scholar] [CrossRef]
- Houssiau, F.A.; Lauwerys, B.R. Current management of lupus nephritis. Best Pract. Res. Clin. Rheumatol. 2013, 27, 319–328. [Google Scholar] [CrossRef]
- Ramachandran, R.; Sulaiman, S.; Chauhan, P.; Ulasi, I.; Onu, U.; Villaneuva, R.; Alam, M.R.; Akhtar, F.; Vincent, L.; Aulakh, G.S.; et al. Challenges in Diagnosis and Management of Glomerular Disease in Resource-Limited Settings. Kidney Int. Rep. 2022, 7, 2141–2149. [Google Scholar] [CrossRef]
- Htay, H.; Alrukhaimi, M.; Ashuntantang, G.E.; Bello, A.K.; Bellorin-Font, E.; Gharbi, M.B.; Braam, B.; Feehally, J.; Harris, D.C.; Jha, V.; et al. Global access of patients with kidney disease to health technologies and medications: Findings from the Global Kidney Health Atlas project. Kidney Int. Suppl. 2018, 8, 64–73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kwon, O.C.; Park, J.H.; Park, H.-C.; Jung, S.M.; Lee, S.-W.; Song, J.J.; Park, Y.-B.; Park, M.-C. Non-histologic factors discriminating proliferative lupus nephritis from membranous lupus nephritis. Thromb. Haemost. 2020, 22, 138. [Google Scholar] [CrossRef]
- Petri, M.; Orbai, A.-M.; Alarcón, G.S.; Gordon, C.; Merrill, J.T.; Fortin, P.R.; Bruce, I.N.; Isenberg, D.; Wallace, D.J.; Nived, O.; et al. Derivation and validation of the Systemic Lupus International Collaborating Clinics classification criteria for systemic lupus erythematosus. Arthritis Rheum. 2012, 64, 2677–2686. [Google Scholar] [CrossRef]
- Kuan, W.; Li, E.; Tam, L.-S. Lupus organ damage: What is damaged in Asian patients? Lupus 2010, 19, 1436–1441. [Google Scholar] [CrossRef]
- Sit, J.K.K.; Chan, W.K.Y. Risk factors for damage in childhood-onset systemic lupus erythematosus in Asians: A case control study. Pediatr. Rheumatol. 2018, 16, 56. [Google Scholar] [CrossRef] [Green Version]
- Abujam, B.; Gupta, A.; Suri, D.; Rawat, A.; Singh, S. Trends and predictors of mortality in childhood onset lupus in a single North-Indian centre over 23 years: A retrospective study. Ann. Rheum. Dis. 2016, 34, 554–559. [Google Scholar]
- Mina, R.; Von Scheven, E.; Ardoin, S.P.; Eberhard, B.A.; Punaro, M.; Ilowite, N.; Hsu, J.; Klein-Gitelman, M.; Moorthy, L.N.; Muscal, E.; et al. Consensus treatment plans for induction therapy of newly diagnosed proliferative lupus nephritis in juvenile systemic lupus erythematosus. Arthritis Care Res. 2011, 64, 375–383. [Google Scholar] [CrossRef]
- Sule, S.D.; Moodalbail, D.G.; Burnham, J.; Fivush, B.; Furth, S.L. Predictors of Kidney Disease in a Cohort of Pediatric Patients with Lupus. Lupus 2015, 24, 862–868. [Google Scholar] [CrossRef] [Green Version]
- Hisham, F.A.; Tharwat, S.; Samra, N.E.; Mostafa, N.; Nassar, M.K.; El-Desoky, M.M. High Mobility Group Box Protein 1 (HMGB1) Serum and Urinary Levels and Gene Polymorphism in Egyptian Patients with Systemic Lupus Erythematosus: A Possible Relation to Lupus Nephritis. Lupus 2022, 31, 1777–1785. [Google Scholar] [CrossRef]
- Kwon, O.C.; Lee, J.S.; Ghang, B.; Kim, Y.-G.; Lee, C.-K.; Yoo, B.; Hong, S. Predicting eventual development of lupus nephritis at the time of diagnosis of systemic lupus erythematosus. Semin. Arthritis Rheum. 2018, 48, 462–466. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Workflow process for feature selection, model training and evaluation. SVM-RFE: Support vector machine classification- Recursive Feature Elimination; SVM_Linear: Support vector machine with linear kernel; SVM_Radial: Support vector machine with radial kernel; Knn: K nearest neighbors; RF: random forest; Rpart: decision-tree Rpart.
Figure 1.
Workflow process for feature selection, model training and evaluation. SVM-RFE: Support vector machine classification- Recursive Feature Elimination; SVM_Linear: Support vector machine with linear kernel; SVM_Radial: Support vector machine with radial kernel; Knn: K nearest neighbors; RF: random forest; Rpart: decision-tree Rpart.

Figure 2.
Recursive Feature Elimination with cross validation. A combination of 11 variables, namely (1) gender, (2) ethnicity, (3) fever, (4) nephrotic, (5) hypertension, (6) Urine RBC, (7) C3, (8) C4, (9) duration of illness, (10) serum albumin, and (11) urine protein had the highest accuracy of 79.4% in predicting proliferative lupus nephritis. After the 11 variables, the accuracy decreases with the increase in the number of variables.
Figure 2.
Recursive Feature Elimination with cross validation. A combination of 11 variables, namely (1) gender, (2) ethnicity, (3) fever, (4) nephrotic, (5) hypertension, (6) Urine RBC, (7) C3, (8) C4, (9) duration of illness, (10) serum albumin, and (11) urine protein had the highest accuracy of 79.4% in predicting proliferative lupus nephritis. After the 11 variables, the accuracy decreases with the increase in the number of variables.

Figure 3.
Receiver Operating Curves (ROC) curves of the five models. The performance of the support vector machine (SVM) with linear kernel model (SVM-Linear), support vector machine (SVM) with radial kernel model (SVM-Radial), K nearest neighbors (Knn) model, random forest (RF) model, and decision-tree Rpart (Rpart) model visualized using Receiver Operating Curves (ROC) curves. The decision-tree Rpart model performs the best based on highest AROC value (69.9%), followed by the SVM-Radial model, the SVM-Linear model, the Knn model and lastly the Random Forest model.
Figure 3.
Receiver Operating Curves (ROC) curves of the five models. The performance of the support vector machine (SVM) with linear kernel model (SVM-Linear), support vector machine (SVM) with radial kernel model (SVM-Radial), K nearest neighbors (Knn) model, random forest (RF) model, and decision-tree Rpart (Rpart) model visualized using Receiver Operating Curves (ROC) curves. The decision-tree Rpart model performs the best based on highest AROC value (69.9%), followed by the SVM-Radial model, the SVM-Linear model, the Knn model and lastly the Random Forest model.

Figure 4.
Confusion matrixes of the five models. Confusion matrix reporting the number of (A) support vector machine (SVM) with linear kernel model (SVM-Linear), (B) support vector machine (SVM) with radial kernel model (SVM-Radial), (C) K nearest neighbors (Knn) model, (D) random forest (RF) model, and (E) decision-tree Rpart (Rpart) to predict proliferative lupus nephritis among jSLE patients (n = 194; 70 training set: 30 test set with nested cross validation) using the 11 variables identified from recursive feature elimination. Category 0: no lupus nephritis and non-proliferative lupus nephritis; Category 1: proliferative lupus nephritis.
Figure 4.
Confusion matrixes of the five models. Confusion matrix reporting the number of (A) support vector machine (SVM) with linear kernel model (SVM-Linear), (B) support vector machine (SVM) with radial kernel model (SVM-Radial), (C) K nearest neighbors (Knn) model, (D) random forest (RF) model, and (E) decision-tree Rpart (Rpart) to predict proliferative lupus nephritis among jSLE patients (n = 194; 70 training set: 30 test set with nested cross validation) using the 11 variables identified from recursive feature elimination. Category 0: no lupus nephritis and non-proliferative lupus nephritis; Category 1: proliferative lupus nephritis.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Demographic characteristics of Malaysian children with SLE.
| Characteristics | No. of Participating Patients, n = 194 (%) |
|---|---|
| Gender | |
| Female | 165 (85.5) |
| Female: Male Ratio | 5.5:1 |
| Female: Male Ratio based on age: | |
| 0–5 years old | 2.7:1 |
| 6–12 years old | 7.8:1 |
| 13–18 years old | 23.4:1 |
| Median age (years, IQR) | |
| At diagnosis | 11.7 (9.0–15.3) |
| At data collection | 15.0 (13.4–20.0) |
| Duration of illness, median | |
| Onset of symptoms to diagnosis (months, IQR) | 2 (0–64) |
| Diagnosis to data collection (years, IQR) | 3 (0–13) |
| Ethnicity | |
| Malay | 133 (68.9) |
| Chinese | 45 (23.3) |
| Indians | 10 (5.2) |
| Others | 5 (2.6) |
| SLICC index at diagnosis | |
| Median (range) score | 20 (1–61) |
SLE: Systemic Lupus Erythematosus; IQR: interquartile range; SLICC: Systemic Lupus International Collaborating Clinics.
Table 2.
Clinical features at diagnosis of 194 Malaysian children with SLE.
| Characteristics | Our Cohort n = 194 (%) |
|---|---|
| Clinical features | |
| Fever | 172 (89.1) |
| Lethargy | 132 (68.4) |
| LOA | 124 (64.2) |
| LOW | 97 (50.3) |
| Alopecia | 80 (41.4) |
| Vasculitic rash | 133 (68.9) |
| Livedo Reticularis | 10 (5.2) |
| Myositis/Myopathy | 53 (27.5) |
| Headache | 37 (19.2) |
| Eye manifestation | 18 (9.3) |
| Hypertension | 52 (26.9) |
| Nephrotic Syndrome | 32 (16.6) |
| Nephritic Syndrome | 21 (10.9) |
LOA: loss of appetite; LOW: loss of weight; CNS: central nervous system.
Table 3.
Prevalence of SLICC Classification Criteria in jSLE cases at diagnosis.
| Characteristics | Our Cohort n = 194 (%) |
|---|---|
| Clinical and laboratory features | |
| Acute cutaneous lupus | 124 (64.2) |
| Chronic cutaneous lupus | 25 (13) |
| Oral ulcers | 87 (45.1) |
| Nonscarring alopecia | 78 (40.4) |
| Synovitis | 66 (34.2) |
| Serositis | 32 (16.6) |
| Renal disorder | 66 (34.2) |
| Neurologic | 53 (27.5) |
| Hemolytic anemia | 40 (20.7) |
| Leukopenia or Lymphopenia | 101 (52.3) |
| Thrombocytopenia | 77 (39.9) |
| Immunological features | |
| Anti-nuclear Antibodies | 190 (98.4) |
| Anti-dsDNA antibodies | 141 (73.1) |
| Anti-smith antibodies | 60 (31.1) |
| Low complement | 171 (88.6) |
| Direct Coombs tests | 148 (76.7) |
Table 4.
Performance evaluation of proposed models by means of sensitivity, specificity, and accuracy.
Table 4.
Performance evaluation of proposed models by means of sensitivity, specificity, and accuracy.
| Models | Sensitivity (%) | Specificity (%) | Accuracy (%) |
|---|---|---|---|
| SVM-Linear | 93.62 | 27.78 | 75.38 |
| SVM-Radial | 95.74 | 33.33 | 78.46 |
| Knn | 88.89 | 45.00 | 75.38 |
| RF | 91.11 | 50.00 | 78.46 |
| Rpart | 78.72 | 61.11 | 73.85 |
SVM-Linear: Support vector machine (SVM) with linear kernel; SVM-Radial: Support vector machine (SVM) with radial kernel; Knn: K nearest neighbors; RF: random forest; Rpart: decision-tree Rpart.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Lim, S.C.; Chan, E.W.L.; Mandal, S.S.; Tang, S.P. A Preliminary Predictive Model for Proliferative Lupus Nephritis in Juvenile Systemic Lupus Erythematosus. Rheumato 2023, 3, 86-97. https://doi.org/10.3390/rheumato3010007
AMA Style
Lim SC, Chan EWL, Mandal SS, Tang SP. A Preliminary Predictive Model for Proliferative Lupus Nephritis in Juvenile Systemic Lupus Erythematosus. Rheumato. 2023; 3(1):86-97. https://doi.org/10.3390/rheumato3010007
Chicago/Turabian StyleLim, Sern Chin, Elaine Wan Ling Chan, Shikriti Suprakash Mandal, and Swee Ping Tang. 2023. "A Preliminary Predictive Model for Proliferative Lupus Nephritis in Juvenile Systemic Lupus Erythematosus" Rheumato 3, no. 1: 86-97. https://doi.org/10.3390/rheumato3010007