
Unusual Case Presentation of Systemic Lupus Erythematosus in a Young Woman

Abstract
:1. Introduction
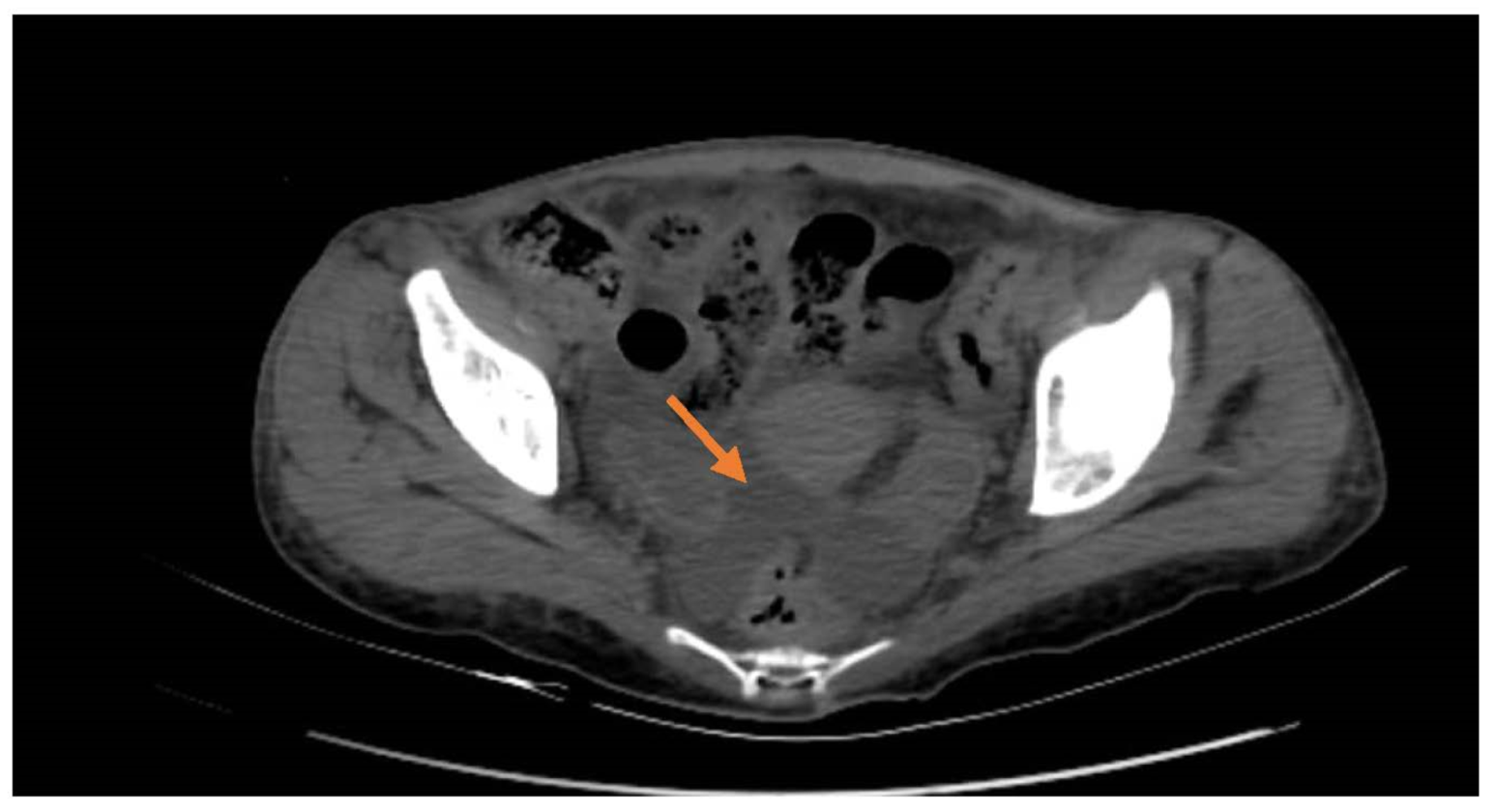
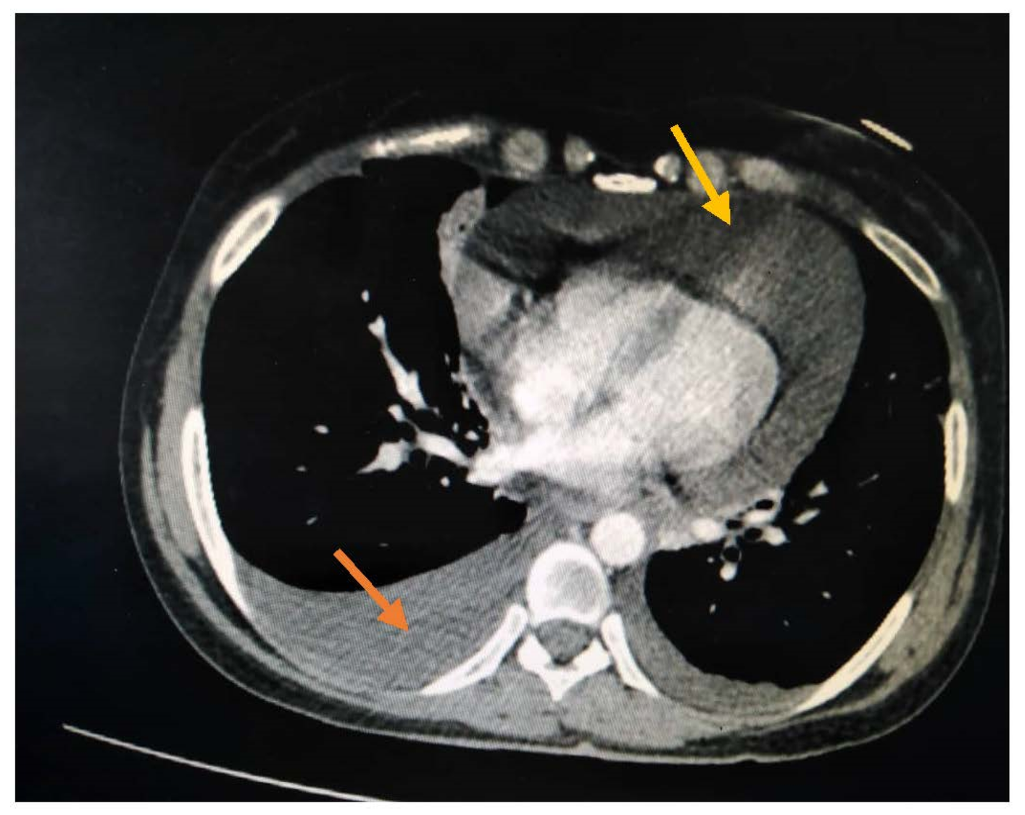
2. Case Presentation
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Man, B.L.; Mok, C.C. Serositis related to systemic lupus erythematosus: Prevalence and outcome. Lupus 2005, 14, 822–826. [Google Scholar] [CrossRef] [PubMed]
- Martinez, D.; Lowe, R. Case report: Systemic lupus erythematosus (SLE) serositis mimicking acute cholecystitis. Clin. Radiol. 1991, 44, 434–435. [Google Scholar] [CrossRef]
- Almousa, S.; Ahmad, T.; Hamdan, S.; Katt, N. Lupus erythematosus tumidus (LET) with autoimmune thyroid dysfunction (AITD) as the first presentation of systemic lupus erythematosus: A case report and review of the literature. Egypt. Rheumatol. 2020, 42, 245–250. [Google Scholar] [CrossRef]
- Hammami, S.; Bdioui, F.; Ouaz, A.; Loghmari, H.; Mahjoub, S.; Saffar, H. Successful treatment of massive ascites due to lupus peritonitis with hydroxychloroquine in old- onset lupus erythematosus. Pan. Afr. Med. J. 2014, 18, 165. [Google Scholar] [CrossRef] [PubMed]
- Cheng, W.; Balachandar, R.; Mistry, P. Cardiac tamponade: An initial presentation of SLE. BMJ Case Rep. 2013, 2013, bcr2013200011. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cook, S.G. Ascites as the Presenting Sign of Systemic Lupus Erythematosus. Cureus 2022, 14, e23231. [Google Scholar] [CrossRef] [PubMed]
- Liang, Y.; Leng, R.-X.; Pan, H.-F.; Ye, D.-Q. The prevalence and risk factors for serositis in patients with systemic lupus erythematosus: A cross-sectional study. Rheumatol. Int. 2016, 37, 305–311. [Google Scholar] [CrossRef] [PubMed]
- Tian, D.G.; Jacobs, A.K.; Benjamin, E.J. A 19-year-old female with tamponade and systemic lupus erythematosus (SLE). Int. J. Cardiol. 2015, 179, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Ryu, S.; Fu, W.; Petri, M.A. Associates and predictors of pleurisy or pericarditis in SLE. Lupus Sci. Med. 2017, 4, e000221. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, E.A.; Rodriguez, V.R.; Otero, D.; Larsen, M. SLE Ascites: An Uncommon Initial Presentation: 954. Am. J. Gastroenterol. 2015, 110, S408. [Google Scholar] [CrossRef]
- Lepore, L.; Facchini, S.; Codrich, D.; Pelizzo, G.; Messineo, A.; Ventura, A. Acute Abdomen: The Presenting Sign of Systemic Lupus Erythematosus in Childhood. J. Pediatr. Gastroenterol. Nutr. 2002, 35, 570–572. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Parameter | Admission | Discharge | Reference Value |
|---|---|---|---|
| WBC | 1500 | 4930 | 4–9 C/uL |
| Lymphocytes | 0.3 | 1.4 | 1.18–3.74 C/uL |
| Hemoglobin | 7.7 | 9.7 | 11.2–15.7 G/dL |
| Platelets | 224 | 281 | 182–370 C/uL |
| ESR | 67 | 43 | Up to 15 mm/1 h |
| CRP | 84.3 | 0.4 | 0–5 mg/L |
| Creatinine | 47 | 42.5 | 45–120 umol/L |
| Alt | 20.5 | 20 | 5–40 U/I |
| Ast | 23.1 | 21 | 5–40 U/I |
| LDH | 712 | 400 | 230–460 U/L |
| Indirect bilirubin | 2.5 | 0.7 | 0.2–0.8 mg/dL |
| Reticulocytes | 7.98 | 0.7 | 0.5–1.5% |
| Coombs direct | Positive | ||
| ANA | Homogeneous 1/320 | Less than 1/100 | |
| Anti-dsDNA | 250 | Up to 25 U/mL | |
| Protein 24 h urine | 562 | 0–150 mg/24 h | |
| TSH | 11.54 | 4.7 | 0.35–5.1 uIU/mL |
| HBsAg | Negative | ||
| Anti HCV | Negative | ||
| C4 | 0.04 | 0.15–0.45 g/L | |
| C3 | 0.28 | 0.8–2 g/L | |
| ENA screen | Negative | Negative | |
| APL antibodies | Negative | Negative |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Almousa, S.; Wannous, H.; Khedr, K.; Qasem, H. Unusual Case Presentation of Systemic Lupus Erythematosus in a Young Woman. Rheumato 2022, 2, 93-97. https://doi.org/10.3390/rheumato2040013
Almousa S, Wannous H, Khedr K, Qasem H. Unusual Case Presentation of Systemic Lupus Erythematosus in a Young Woman. Rheumato. 2022; 2(4):93-97. https://doi.org/10.3390/rheumato2040013
Chicago/Turabian StyleAlmousa, Samaher, Hala Wannous, Kamar Khedr, and Heba Qasem. 2022. "Unusual Case Presentation of Systemic Lupus Erythematosus in a Young Woman" Rheumato 2, no. 4: 93-97. https://doi.org/10.3390/rheumato2040013