
A Case of Rheumatoid Meningitis


{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
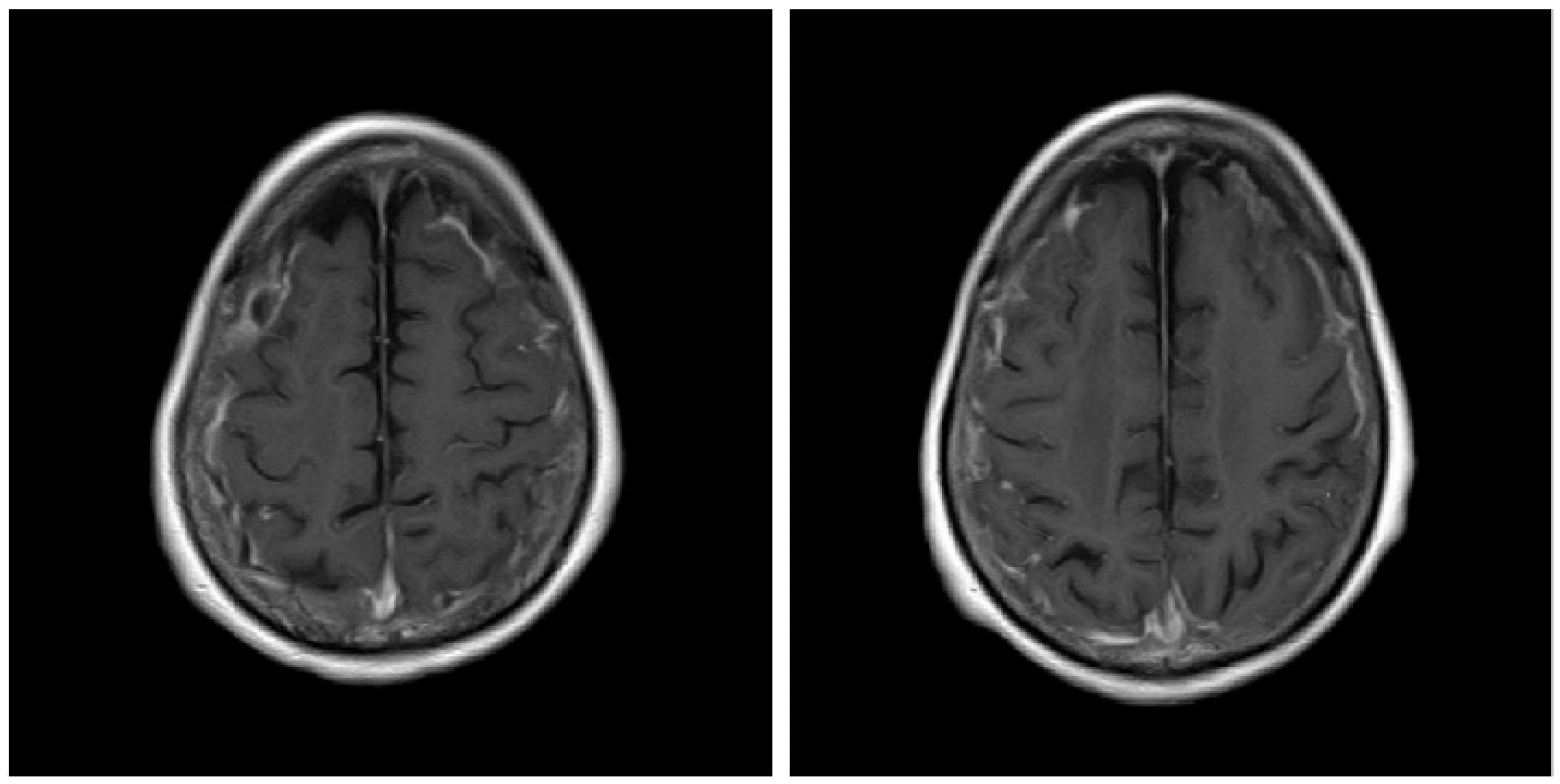
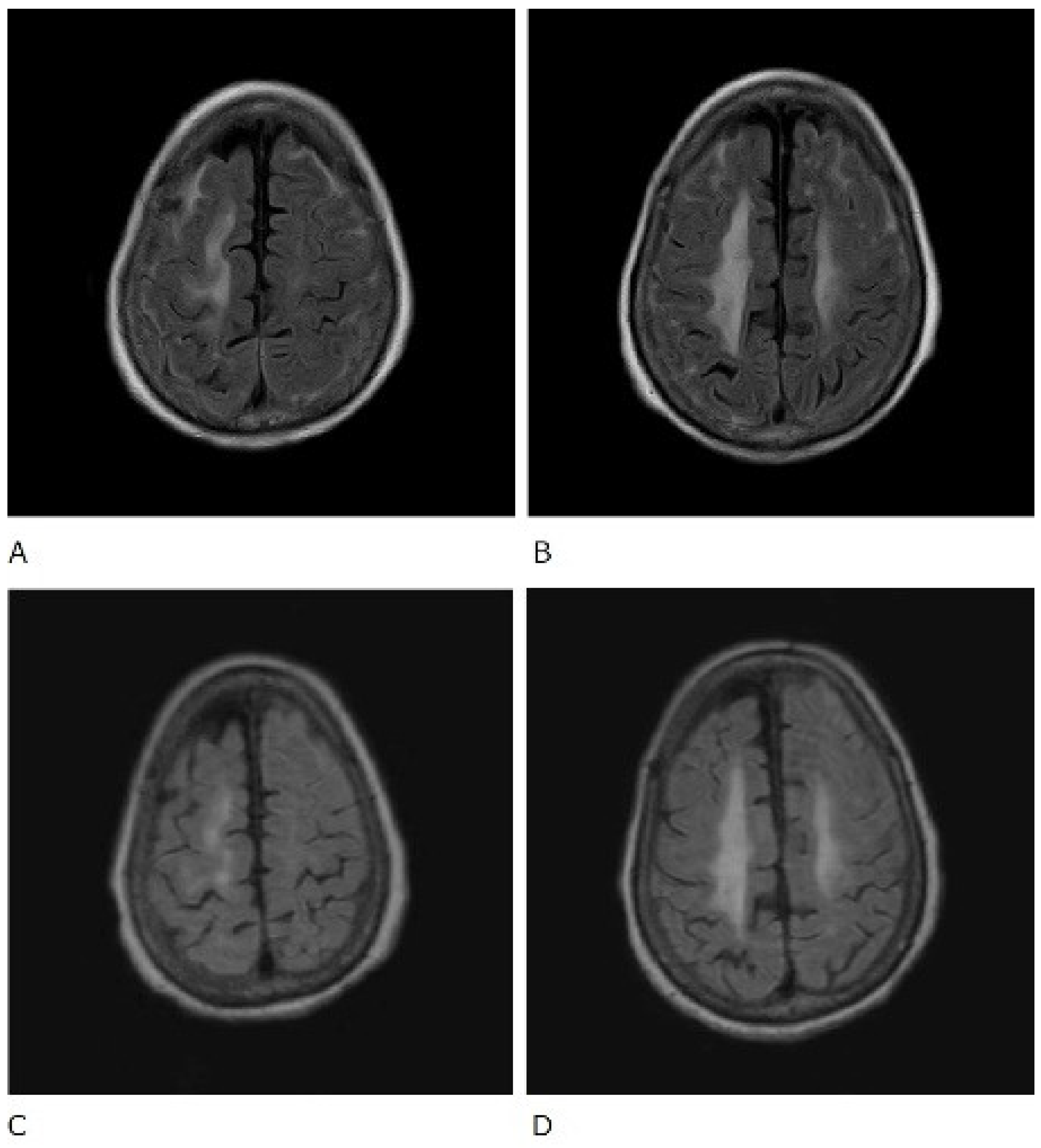
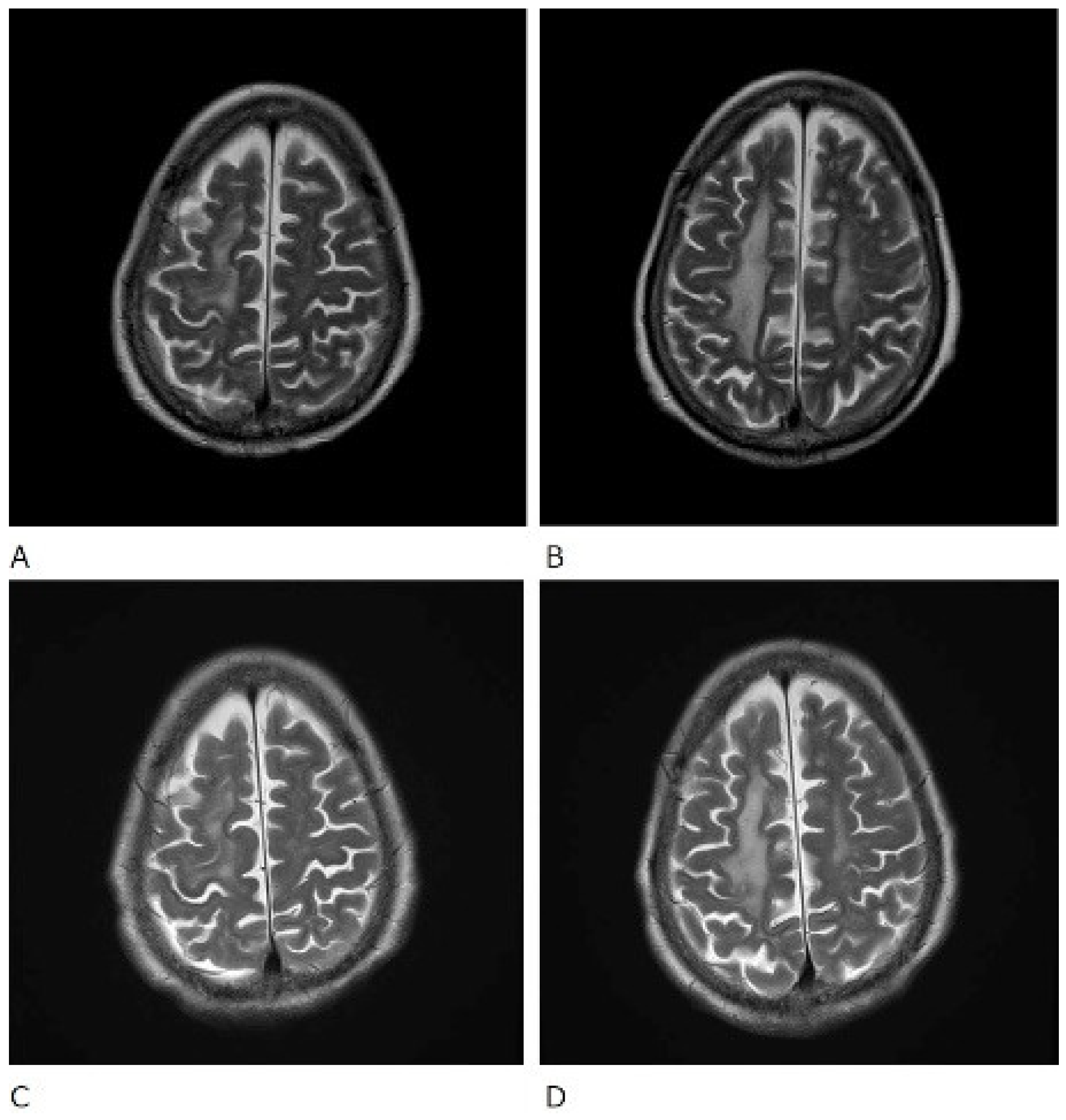
2. Case Presentation
3. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Servioli, M.J.; Chugh, C.; Lee, J.M.; Biller, J. Rheumatoid meningitis. Front. Neurol. 2011, 2, 84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bathon, J.M.; Moreland, L.W.; DiBartolomeo, A.G. Inflammatory central nervous system involvement in rheumatoid arthritis. Semin. Arthritis Rheum. 1989, 18, 258–266. [Google Scholar] [CrossRef]
- Abe, T.; Mishima, K.; Uchino, A.; Sasaki, A.; Tanahashi, N.; Takao, M. A case of anti-cyclic citrullinated peptides antibody positive rheumatoid meningitis without arthritis at the onset of neurological symptoms. Rinsho Shinkeigaku (Clin. Neurol.) 2016, 56, 627–632. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Padjen, I.; Mayer, M.; Habek, M.; Kolenc, D.; Dotlic, S. Redefining a diagnosis: From meningeal plasma cell granuloma to rheumatoid meningitis. Report of a patient follow-up. Neurol. Sci. 2015, 36, 1047–1048. [Google Scholar] [CrossRef] [PubMed]
- Jones, S.E.; Belsey, N.A.; McLoud, T.C.; Mullins, M.E. Rheumatoid meningitis: Radiologic and Pathilogic Correlation. Am. J. Roentgenol. 2006, 186, 1181–1183. [Google Scholar] [CrossRef] [PubMed]
- Trabelsi, M.; Romand, X.; Gilson, M.; Vaillant, M.; Guerne, P.A.; Hayem, G.; Bertolini, E.; Baillet, A.; Gaudin, P. Rheumatoid Meningitis a Rare Extra-Articular Manifestation of Rheumatoid Arthritis: Report of 6 Cases and Literature Review. J. Clin. Med. 2020, 9, 1625. [Google Scholar] [CrossRef] [PubMed]
- Lee Ching, C.; Kenyon, L.; Berk, M.; Park, C. Rheumatoid meningitis sine arthritis. J. Neuroimmunol. 2019, 328, 73–75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, S.J.; Ho Park, Y.; Kim, J.A.; Han, J.H.; Choe, G.; Kim, S. Pearls & Oy-sters: Asymmetric meningeal involvement is a common feature of rheumatoid meningitis. Case Rep. 2017, 88, e108–e110. [Google Scholar]
- Parsons, A.M.; Aslam, F.; Grill, M.F.; Aksamit, A.J.; Goodman, B.P. Rheumatoid Meningitis: Clinical Characteristics, Diagnostic Evaluation, and Treatment. Neurohospitalist 2020, 10, 88–94. [Google Scholar] [CrossRef] [PubMed]
- Yamashita, K.; Terasaki, Y.; Sakaguchi, M.; Nakatsuji, Y.; Yoshizaki, K.; Mochizuki, H. A case of rheumatoid meningitis presented with generalized seizure in whom MRI images were helpful for the diagnosis. Rinsho Shinkeigaku (Clin. Neurol.) 2015, 55, 926–931. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shimada, K.; Matsui, T.; Kawakami, M. Diffuse chronic leptomeningitis with seropositive rheumatoid arthritis: Report of case successfully treated as rheumatoid leptomeningitis. Mod. Rheumatol. 2009, 19, 556–562. [Google Scholar] [CrossRef] [PubMed]
- Chou, R.C.; Henson, J.W.; Tian, D. Successful treatment of rheumatoid meningitis with cyclophosphamide but not infliximab. Ann. Rheum. 2006, 65, 1114–1116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kato, T.; Hoshi, K.; Sekijima, Y. Rheumatoid meningitis: An autopsy report and review of the literature. Clin. Rheumatol. 2003, 22, 475–480. [Google Scholar] [CrossRef] [PubMed]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tomizuka, T.; Kikuchi, H.; Asako, K.; Kono, H. A Case of Rheumatoid Meningitis. Rheumato 2022, 2, 69-73. https://doi.org/10.3390/rheumato2030009
Tomizuka T, Kikuchi H, Asako K, Kono H. A Case of Rheumatoid Meningitis. Rheumato. 2022; 2(3):69-73. https://doi.org/10.3390/rheumato2030009
Chicago/Turabian StyleTomizuka, Takafumi, Hirotoshi Kikuchi, Kurumi Asako, and Hajime Kono. 2022. "A Case of Rheumatoid Meningitis" Rheumato 2, no. 3: 69-73. https://doi.org/10.3390/rheumato2030009