
Survey of Australian Dietitians Contemporary Practice and Dietetic Interventions in Overweight and Obesity: An Update of Current Practice
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
3.1. Demographics and Service Profiles of Respondents
3.2. Use of Dietitians Australia Best Practice Guidelines for the Management of Overweight and Obesity
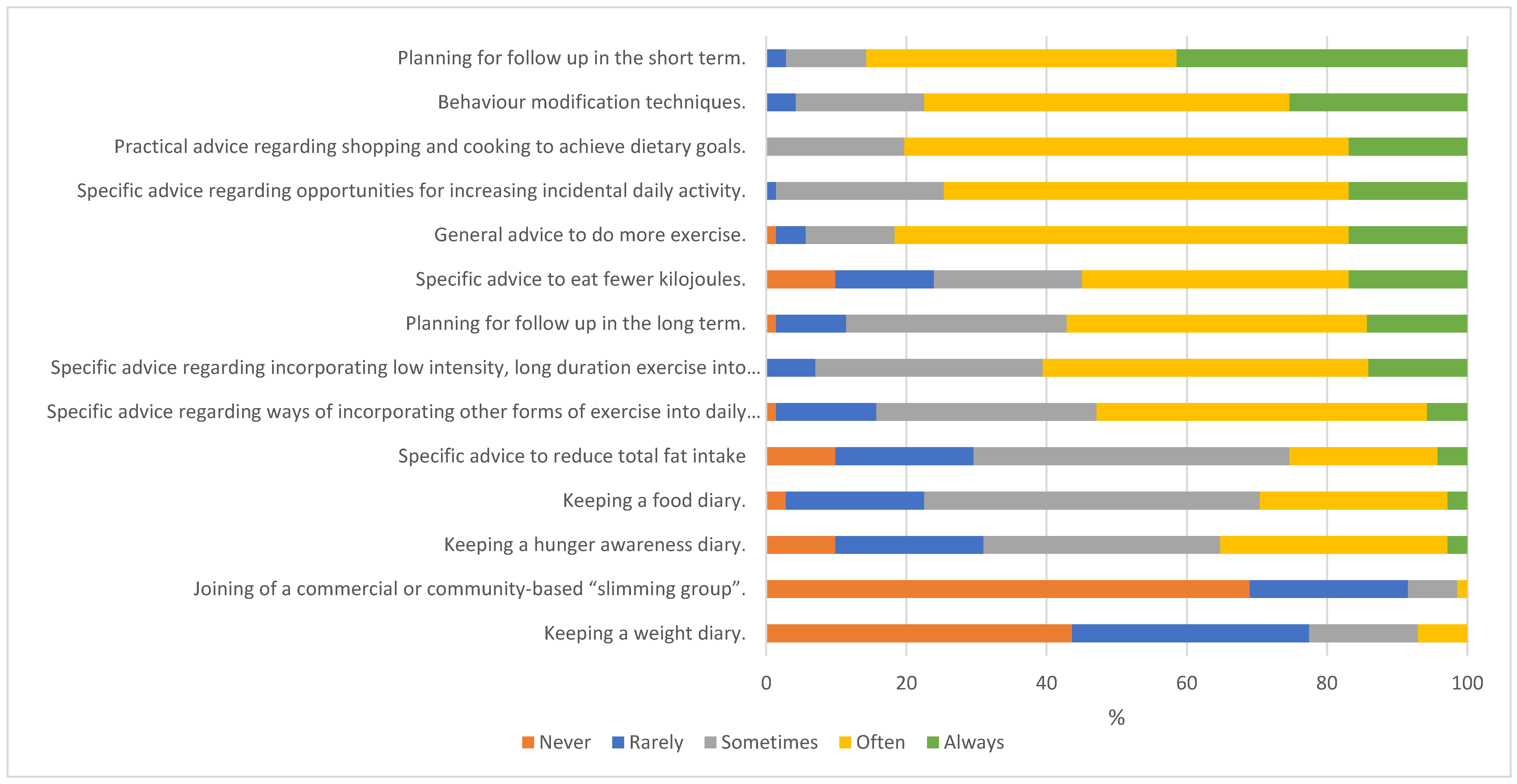
3.3. Current Dietetic Practice
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Australian Institute of Health and Welfare. Risk Factors to Health; Australian Institute of Health and Welfare: Canberra, Australia, 2017. [Google Scholar]
- Australian Institute of Health and Welfare. Australian Burden of Disease Study: Impact and causes of illness and death in Australia 2015. In Australian Burden of Disease Series no. 19. Cat. no. BOD 22; Australian Institute of Health and Welfare: Canberra, Australia, 2019. [Google Scholar]
- Williams, L.T.; Barnes, K.; Ball, L.; Ross, L.J.; Sladdin, I.; Mitchell, L.J. How Effective Are Dietitians in Weight Management? A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Healthcare 2019, 7, 20. [Google Scholar] [CrossRef] [PubMed]
- Collins, C. Survey of dietetic management of overweight and obesity in comparison with best practice criteria. Nutr. Diet. 2003, 60, 177–184. [Google Scholar]
- Collins, C.; Neve, M.; Palmer, M. DAA Best Practice Guidelines for the Treatment of Overweight and Obesity in Adults—Report to Inform the 2011 Revision of the 2005 Guidelines; Dietitians Association of Australia, The University of Newcastle: Canberra, Australia, 2012. [Google Scholar]
- Campbell, K.; Crawford, D. Management of obesity: Attitudes and practices of Australian dietitians. Int. J. Obes. 2000, 24, 701–710. [Google Scholar] [CrossRef] [PubMed]
- National Health and Medical Research Council. The Clinical Practice Guidelines for the Management of Overweight and Obesity in Adults, Adolescents and Children in Australia; National Health and Medical Research Council: Melbourne, Australia, 2013. [Google Scholar]
- Dietitians Australia. DA Best Practice Guidelines for the Treatment and Prevention of people with Overweight & Obesity in Adults; Dietitians Australia: Canberra, Australia, 2012. [Google Scholar]
- Wharton, S.; Lau, D.C.; Vallis, M.; Sharma, A.M.; Biertho, L.; Campbell-Scherer, D.; Adamo, K.; Alberga, A.; Bell, R.; Boulé, N.; et al. Obesity in adults: A clinical practice guideline. Can. Med. Assoc. J. 2020, 192, E875. [Google Scholar] [CrossRef] [PubMed]
- Dietitians Australia. Media Release—Supporting People of All Sizes to Thrive: Call to Update Clinical Practice Guidelines. 2021. Available online: https://dietitiansaustralia.org.au/about-us/media-centre/supporting-people-all-sizes-thrive-call-update-clinical-practice-guidelines-media-release (accessed on 4 March 2021).
- Dietitians Australia. Annual Report 2020–2021. 2022. Available online: https://dietitiansaustralia.org.au/sites/default/files/2022-05/Annual-Report-2020-21.pdf (accessed on 20 November 2022).
- Dietitians Australia. Annual Report 2020. 2020. Available online: https://dietitiansaustralia.org.au/wp-content/uploads/2020/10/DA-Annual-Report-2019-20.pdf (accessed on 13 November 2021).
- Ball, L.; Larsson, R.; Gerathy, R.; Hood, P.; Lowe, C. Working profile of Australian private practice Accredited Practising Dietitians. Nutr. Diet. 2013, 70, 196–205. [Google Scholar] [CrossRef]
- Morsali, M.; Poorolajal, J.; Shahbazi, F.; Vahidinia, A.; Doosti-Irani, A. Diet Therapeutics Interventions for Obesity: A Systematic Review and Network Meta-Analysis. J. Res. Health Sci. 2021, 21, e00521. [Google Scholar] [CrossRef] [PubMed]
- Tsai, A.G.; Wadden, T.A. The evolution of very-low-calorie diets: An update and meta-analysis. Obesity 2006, 14, 1283–1293. [Google Scholar] [CrossRef] [PubMed]
- Johnston, B.C.; Kanters, S.; Bandayrel, K.; Wu, P.; Naji, F.; Siemieniuk, R.A.; Ball, G.D.C.; Busse, J.W.; Thorlund, K.; Guyatt, G.; et al. Comparison of Weight Loss Among Named Diet Programs in Overweight and Obese Adults: A Meta-analysis. JAMA 2014, 312, 923–933. [Google Scholar] [CrossRef] [PubMed]
- Schutz, D.D.; Busetto, L.; Dicker, D.; Farpour-Lambert, N.; Pryke, R.; Toplak, H.; Widmer, D.; Yumuk, V.; Schutz, Y. European Practical and Patient-Centred Guidelines for Adult Obesity Management in Primary Care. Obes. Facts 2019, 12, 40–66. [Google Scholar]
- Epstein, R.M.; Street, R.L., Jr. The values and value of patient-centered care. Ann. Fam. Med. 2011, 9, 100–103. [Google Scholar] [CrossRef] [PubMed]
- Bischoff, S.C.; Boirie, Y.; Cederholm, T.; Chourdakis, M.; Cuerda, C.; Delzenne, N.M.; Deutz, N.E.; Fouque, D.; Genton, L.; Gil, C.; et al. Towards a multidisciplinary approach to understand and manage obesity and related diseases. Clin. Nutr. 2017, 36, 917–938. [Google Scholar] [CrossRef]
- Rich, K.; Murray, K.; Smith, H.; Jelbart, N. Interprofessional practice in health: A qualitative study in psychologists, exercise physiologists, and dietitians. J. Interprof. Care 2021, 35, 682–690. [Google Scholar] [CrossRef]
- Tapsell, L.C.; Lonergan, M.; Martin, A.; Batterham, M.J.; Neale, E.P. Interdisciplinary lifestyle intervention for weight management in a community population (HealthTrack study): Study design and baseline sample characteristics. Contemp. Clin. Trials 2015, 45 Pt B, 394–403. [Google Scholar] [CrossRef]
- Sharma, A.M.; Bélanger, A.; Carson, V.; Krah, J.; Langlois, M.; Lawlor, D.; Lepage, S.; Liu, A.; Macklin, D.A.; MacKay, N.; et al. Perceptions of barriers to effective obesity management in Canada: Results from the ACTION study. Clin. Obes. 2019, 9, e12329. [Google Scholar] [CrossRef] [PubMed]
- Iwabu, M.; Yamauchi, T.; Shimomura, I.; Eguchi, K.; Ogawa, Y. Perceptions, attitudes and barriers to obesity management: Japanese data from the ACTION-IO study. J. Diabetes Investig. 2021, 12, 845–858. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Completers (n = 80) | Non-Completers (n = 98) | Chi-Squared p-Value | ||
|---|---|---|---|---|
| Question | Responses | N (%) | N (%) | |
| Which Dietitians Australia Branch do you belong to? | Number of responses | 75/80 | 80/98 | 0.26 |
| Northern Territory | 0 (0) | 2 (2.0) | ||
| Queensland | 16 (21.3) | 12 (12.2) | ||
| New South Wales | 21 (28.0) | 24 (24.5) | ||
| Victoria | 22 (29.3) | 24 (24.5) | ||
| South Australia | 5 (6.7) | 2 (2.0) | ||
| Tasmania | 1 (1.3) | 0 (0) | ||
| Western Australia | 8 (10.7) | 6 (6.1) | ||
| Australian Capital Territory | 0 (0) | 4 (4.1) | ||
| Overseas | 2 (2.7) | 4 (4.1) | ||
| What is your membership status? | Number of responses | 75/80 | 78/98 | 0.047 |
| Member with dietetic qualifications and APD | 75 (100) | 74 (75.5) | ||
| Member with dietetic qualifications and no APD | 0 (0) | 4 (4.1) | ||
| How would you describe your geographical location? | Number of responses Metropolitan or large urban area Regional Rural/remote | 75/80 | 78/98 | 0.16 |
| 47 (62.7) | 59 (60.2) | |||
| 22 (29.3) | 13 (13.3) | |||
| 6 (8.0) | 6 (6.1) | |||
| How many years have you been a practising dietitian? | Number of responses | 75/80 | 78/98 | 0.09 |
| <5 years | 37 (49.3) | 23 (23.5) | ||
| 5–10 years | 11 (14.7) | 24 (24.5) | ||
| 11–15 years | 7 (9.3) | 12 (12.2) | ||
| >15 years | 20 (26.7) | 19 (19.4) | ||
| Are you currently working? | Number of responses | 74/80 | 78/98 | 0.08 |
| Full time (>20 h/week) | 47 (63.5) | 53 (54.0) | ||
| Part time (up to 20 h/week) | 27 (36.5) | 21 (21.4) | ||
| Not currently working | 0 (0) | 4 (4.1) | ||
| What is your current employment status? | Number of responses | 75/80 | 78/98 | 0.22 |
| Employed in Australia as a dietitian | 70 (93.3) | 62 (63.3) | ||
| Employed in Australia but not in nutrition or dietetics | 1 (1.3) | 2 (2.0) | ||
| Overseas | 2 (2.7) | 6 (6.1) | ||
| Not employed but looking for work | 0 (0) | 2 (2.1) | ||
| Not employed and not looking for work | 0 (0) | 1 (1.0) | ||
| Other | 2 (2.7) | 5 (5.1) | ||
| In what area of practice do you manage clients with overweight and obesity? | Number of responses | 75/80 | 78/98 | 0.43 |
| Community nutrition | 15 (20.0) | 18 (18.4) | ||
| Government department/NGO | 3 (4.0) | 3 (3.1) | ||
| Public Hospital | 15 (20.0) | 8 (8.2) | ||
| Private hospital | 1 (1.33) | 3 (3.1) | ||
| Aged care | 0 (0) | 2 (2.1) | ||
| Private practice | 35 (46.7) | 34 (34.7) | ||
| Research/education | 0 (0) | 1 (1.0) | ||
| Other | 6 (8.0) | 9 (9.2) | ||
| What proportion of work do you spend time working in the area of overweight or obesity? | Number of responses | 75/80 | 78/98 | 0.21 |
| <10% | 7 (9.3) | 10 (10.2) | ||
| 10–25% | 12 (16.0) | 13 (13.3) | ||
| 26–50% | 20 (26.7) | 22 (22.4) | ||
| 51–75% | 26 (34.7) | 15 (15.3) | ||
| 76–100% | 10 (13.3) | 18 (18.4) | ||
| Do you work with other members of a multidisciplinary team? | Number of responses | 74/80 | 16/98 | 0.36 |
| Yes | 63 (85.1) | 15 (15.3) | ||
| No | 11 (14.9) | 1 (1.0) | ||
| What other services are provided within your multidisciplinary team? (a),(b) | Number of responses | 62/63 | 10/15 | |
| Psychologist | 34 (54.8) | 7 (7.1) | 0.37 | |
| Physiotherapist | 37 (59.7) | 4 (4.1) | 0.24 | |
| Gym instructors | 3 (4.8) | 1 (1.0) | 0.51 | |
| General Practitioner | 31 (50.0) | 6 (6.1) | 0.56 | |
| Exercise physiologists | 33 (53.2) | 6 (6.1) | 0.69 | |
| Social workers | 18 (29.0) | 0 (0) | 0.049 | |
| Other | 24 (38.7) | 3 (3.1) | 0.60 | |
| Are you a member of any obesity interest groups (Dietitians Australia or other)? | Number of responses | 74/80 | 78/98 | 0.07 |
| No | 47 (63.5) | 38 (38.8) | ||
| Yes | 27 (36.5) | 40 (40.8) | ||
| What obesity interest groups are you apart of? (a),(b),(c) | DA National Obesity Interest Group | 18 (72.0) | 24 (24.5) | 0.95 |
| ANZOS | 2 (8.0) | 2 (2.0) | 0.77 | |
| OSSANZ | 3 (12.0) | 3 (3.1) | 0.72 | |
| Other | 5 (20.0) | 7 (7.1) | 0.91 | |
| Does your service use the clinical guidelines for obesity management? | Number of responses | 75/80 | 75/98 | 0.19 |
| Yes | 40 (53.3) | 36 (36.7) | ||
| No | 23 (30.7) | 18 (18.4) | ||
| Unsure | 12 (16.0) | 21 (21.4) | ||
| What year did your service start using the clinical guidelines for obesity management? (c) | Number of responses | 22/40 | 12/36 | 0.40 |
| 1980–2000 | 0 (0) | 1 (1.0) | ||
| 2001–2011 | 2 (9.2) | 1 (1.0) | ||
| 2012–2017 | 12 (54.6) | 4 (4.1) | ||
| 2018–2020 | 8 (36.4) | 6 (6.1) |
| Completers Only (n = 80) | All Respondents (n = 91) | ||
|---|---|---|---|
| N (%) | N (%) | ||
| Services dietary approach (a) | Number of responses | 74/80 | 91/91 |
| General healthy eating | 57 (77.0) | 68 (74.7) | |
| Set energy level plan | 21 (28.4) | 25 (27.5) | |
| Formulated meal plan | 12 (16.2) | 17 (18.7) | |
| General advice on low fat eating | 14 (18.9) | 18 (19.8) | |
| Specific low fat eating plan | 0 (0) | 2 (2.2) | |
| Non-diet approach with specific focus to reduce energy intake | 40 (54.1) | 49 (53.9) | |
| Non-diet approach eating behaviour goals | 42 (56.8) | 55 (60.4) | |
| Very low energy diet | 32 (43.2) | 38 (41.8) | |
| Meal replacements | 18 (24.3) | 20 (22.0) | |
| Health at Every Size | 26 (35.1) | 36 (39.6) | |
| Other | 6 (8.1) | 7 (7.7) | |
| How specific dietary strategies or interventions selected for clients (a) | Number of responses | 74/80 | 91/91 |
| Client preference | 56 (75.7) | 68 (74.7) | |
| Client past dieting experience | 41 (55.4) | 51 (56.0) | |
| Dietitian practitioner experience | 35 (47.3) | 39 (42.9) | |
| Based on program/service philosophy | 9 (12.2) | 11 (12.1) | |
| As requested by medical referral | 14 (18.9) | 17 (18.7) | |
| Method negotiated by practitioner with client | 50 (67.6) | 61 (67.0) | |
| Other | 4 (5.4) | 4 (4.4) | |
| Client outcome measures used to monitor progress (up to 6 months follow up) of clients (a),(b) | Number of responses | 74/80 | 85/91 |
| Weight/BMI | 56 (75.7) | 63 (74.1) | |
| Waist circumference | 25 (33.8) | 30 (35.3) | |
| Waist to hip ratio | 5 (6.8) | 5 (5.9) | |
| Metabolic indicators | 51 (68.9) | 61 (71.8) | |
| Diet improvements | 70 (94.6) | 80 (94.1) | |
| Exercise levels | 52 (70.3) | 60 (70.6) | |
| Quality of life | 51 (68.9) | 60 (70.6) | |
| CBT related changes | 11 (14.9) | 12 (14.1) | |
| Achievement of goals | 55 (74.3) | 62 (72.9) | |
| Clothing size | 25 (33.8) | 27 (31.8) | |
| Blood pressure | 16 (21.6) | 18 (21.2) | |
| Fitness level, aerobic capacity, muscle mass, VO2max | 6 (8.1) | 8 (9.4) | |
| Patient attendance | 20 (2.0) | 23 (27.1) | |
| Patient satisfaction | 34 (46.0) | 40 (47.1) | |
| Medication | 14 (18.9) | 20 (23.5) | |
| Psychological/ body image changes | 24 (32.4) | 28 (32.9) | |
| Other | 5 (6.7) | 5 (5.9) | |
| After an initial consultation/session, how many times the client is reviewed before discharge | Number of responses | 74/80 | 84/91 |
| They are not reviewed | 1 (1.4) | 1 (1.2) | |
| 1–2 times | 11 (14.9) | 12 (14.3) | |
| 3–5 times | 16 (21.6) | 18 (21.4) | |
| 6–9 times | 3 (4.1) | 3 (3.6) | |
| 10 times | 2 (2.7) | 3 (3.6) | |
| Other, please specify | 7 (9.5) | 8 (9.5) | |
| Variable/dependent on client needs | 34 (46.0) | 39 (46.4) | |
| After an initial consultation/session, the period of time clients would be followed up/reviewed | Number of responses | 74/80 | 84/91 |
| Initial consultations given only | 1 (1.4) | 1 (1.2) | |
| <2 weeks | 5 (6.8) | 6 (7.1) | |
| 2 weeks–1 month | 41 (55.4) | 46 (54.8) | |
| 2–3 months | 7 (9.5) | 10 (11.9) | |
| 4–6 months | 3 (4.1) | 3 (3.6) | |
| 7–12 months | 4 (5.4) | 4 (4.8) | |
| >1 year | 2 (2.7) | 3 (3.6) | |
| Other | 11 (14.9) | 11 (13.1) |
| Completers Only | All Respondents | ||
|---|---|---|---|
| N (%) | N (%) | ||
| Enablers to practice (a) | Resources | 54 (73.0) | 60 (74.1) |
| Access to a multidisciplinary team | 53 (71.6) | 58 (71.6) | |
| Supportive referrers/medical staff | 38 (51.4) | 42 (51.9) | |
| CPD activities done/personal level of experience | 47 (63.5) | 51 (63.0) | |
| Physical environment | 16 (21.6) | 17 (21.0) | |
| Length of time available for sessions | 53 (71.6) | 58 (71.6) | |
| Referral system/mechanism/ access | 29 (39.2) | 32 (39.5) | |
| Patient characteristics or support | 29 (39.2) | 33 (40.7) | |
| Access to data for patient management | 43 (58.1) | 48 (59.3) | |
| Other | 1 (1.4) | 1 (1.2) | |
| Barriers to practice (a) | Time (relative to workload) | 37 (50.7) | 38 (47.5) |
| Resources (e.g., referral system, facilities, tools) | 17 (23.3) | 19 (23.8) | |
| Lack of staff (either dietitian or multidisciplinary) | 19 (26.0) | 20 (25.0) | |
| Management related (e.g., not a priority of the service) | 17 (23.3) | 17 (21.3) | |
| Characteristics of the population group | 27 (37.0) | 30 (37.5) | |
| Lack of knowledge with regard to best practice management | 8 (11.0) | 10 (12.5) | |
| Referrer related issues | 14 (19.2) | 16 (20.0) | |
| Lack of skills either psychological, counselling or physical activity | 14 (19.2) | 18 (22.5) | |
| No evidence of treatment effectiveness | 10 (13.7) | 10 (12.5) | |
| There are no barries | 13 (17.8) | 13 (16.3) | |
| Other | 8 (11.0) | 8 (10.0) | |
| Gaps in skills limiting the provision of effective dietetic treatment (a) | Behavioural therapy/modification or psychological assessment or motivation or stages of change | 41 (56.9) | 46 (59.0) |
| Knowledge of best practice-guidelines, follow-up, dealing with specific populations | 21 (29.2) | 22 (28.2) | |
| Resource related, e.g., time, computer, facilities | 15 (20.8) | 17 (21.8) | |
| Physical activity related | 13 (18.1) | 16 (20.5) | |
| Client assessment prior to and during therapy, including anthropometric assessment OR goal setting | 8 (11.1) | 8 (10.3) | |
| Personal interest (lack of) | 10 (13.9) | 10 (12.8) | |
| No perceived gaps | 8 (11.1) | 8 (10.3) | |
| Other | 3 (4.2) | 4 (5.1) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Clarke, E.D.; Haslam, R.L.; Baldwin, J.N.; Burrows, T.; Ashton, L.M.; Collins, C.E. Survey of Australian Dietitians Contemporary Practice and Dietetic Interventions in Overweight and Obesity: An Update of Current Practice. Dietetics 2023, 2, 57-70. https://doi.org/10.3390/dietetics2010006
Clarke ED, Haslam RL, Baldwin JN, Burrows T, Ashton LM, Collins CE. Survey of Australian Dietitians Contemporary Practice and Dietetic Interventions in Overweight and Obesity: An Update of Current Practice. Dietetics. 2023; 2(1):57-70. https://doi.org/10.3390/dietetics2010006
Chicago/Turabian StyleClarke, Erin D., Rebecca L. Haslam, Jennifer N. Baldwin, Tracy Burrows, Lee M. Ashton, and Clare E. Collins. 2023. "Survey of Australian Dietitians Contemporary Practice and Dietetic Interventions in Overweight and Obesity: An Update of Current Practice" Dietetics 2, no. 1: 57-70. https://doi.org/10.3390/dietetics2010006