Diet Quality, Nutritional Adequacy and Anthropometric Status among Indigenous Women of Reproductive Age Group (15–49 Years) in India: A Narrative Review


Abstract
:1. Introduction
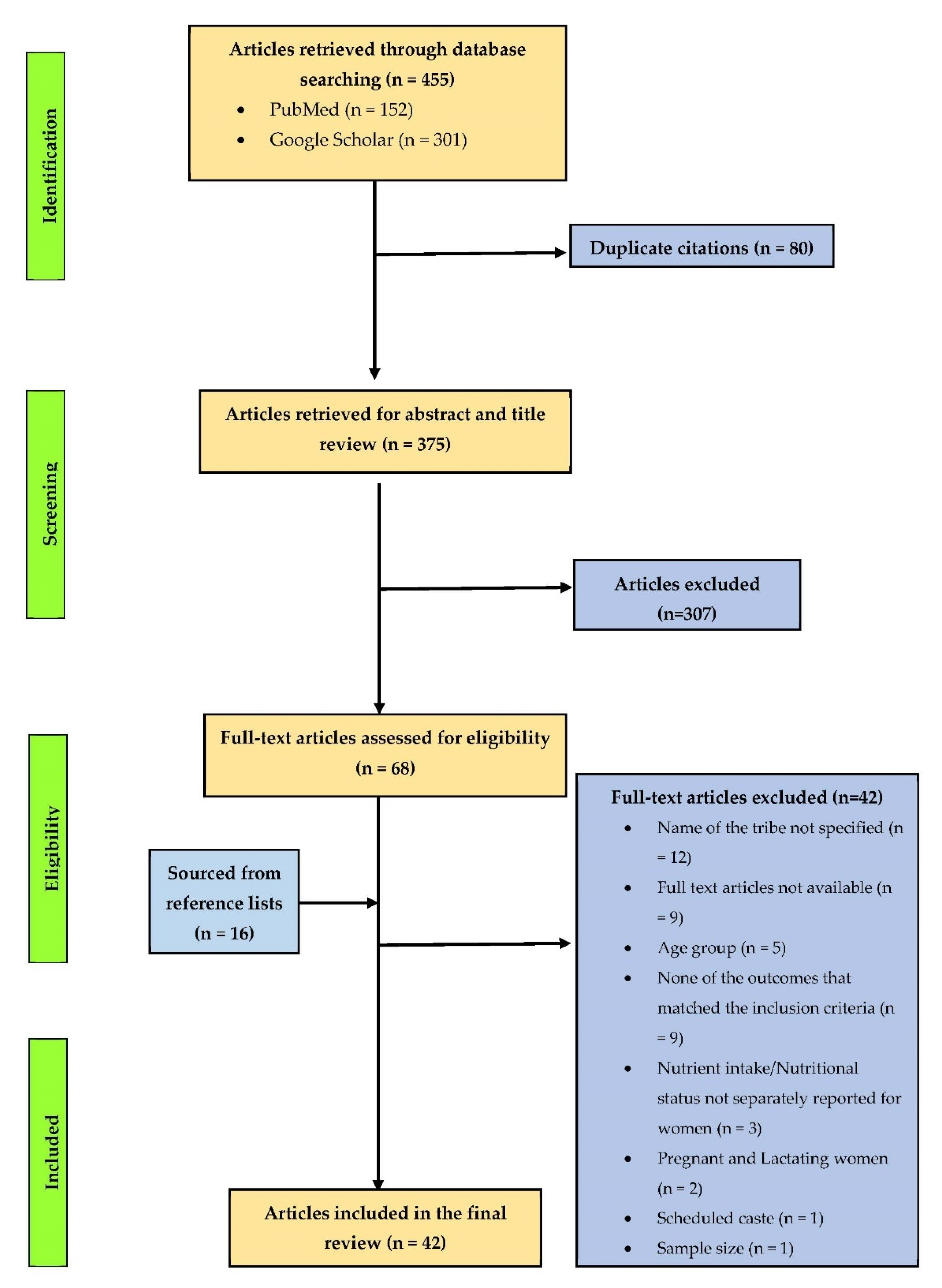
2. Materials and Methods
3. Results and Discussion
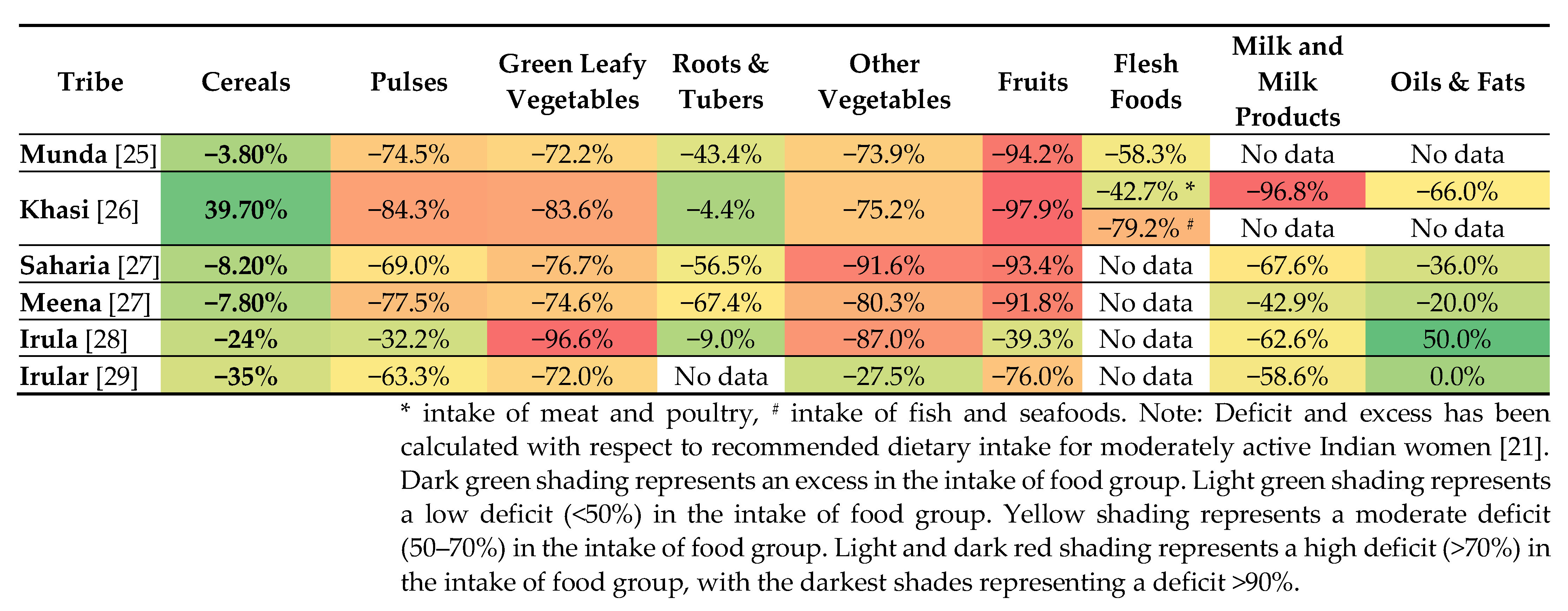
3.1. Food Group Consumption in Indigenous Women of India
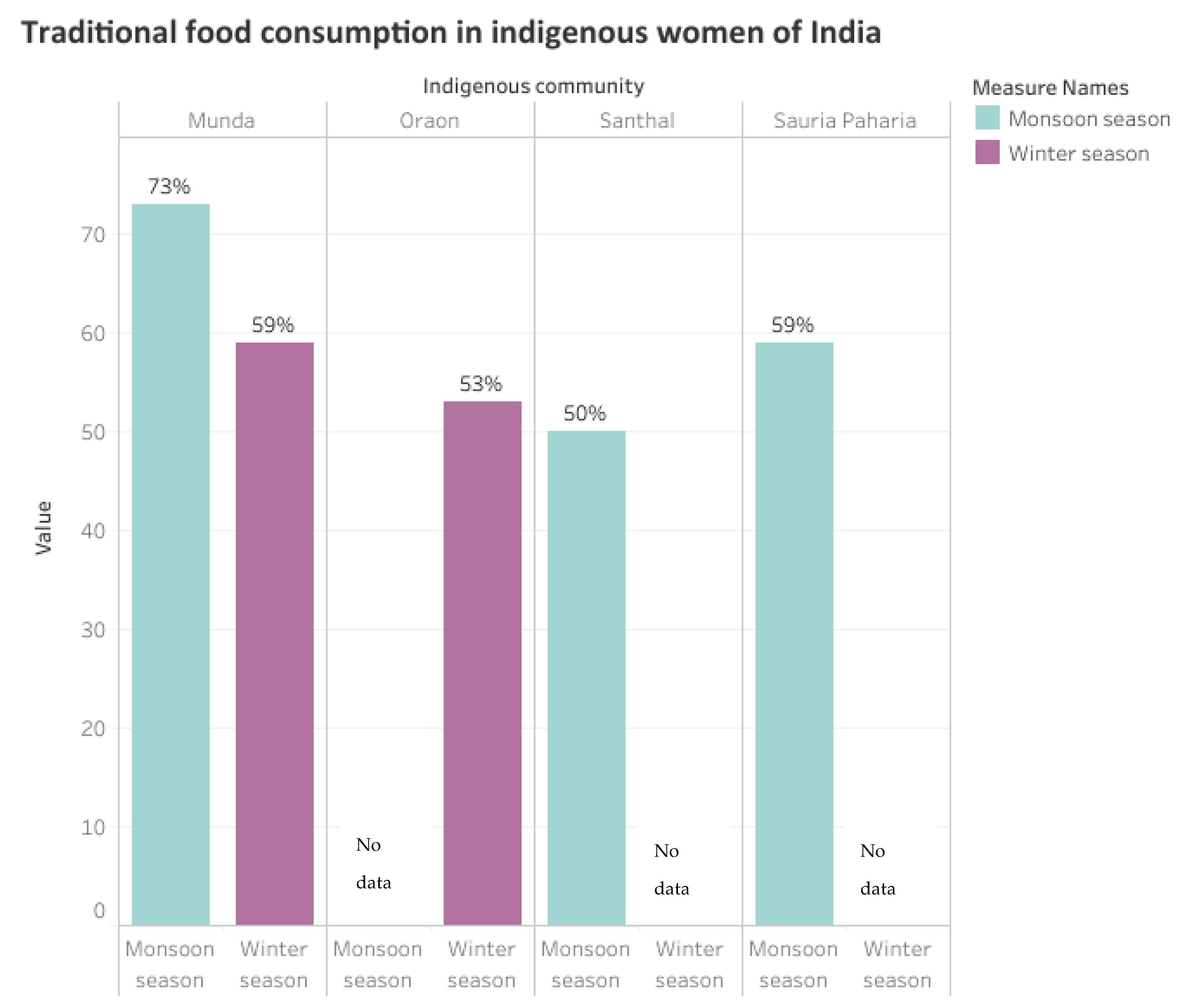
3.2. Traditional Food Consumption in Indigenous Women of India
3.3. Dietary Diversity of Indigenous Women in India
3.4. Nutrient Intake of Indigenous Women in India
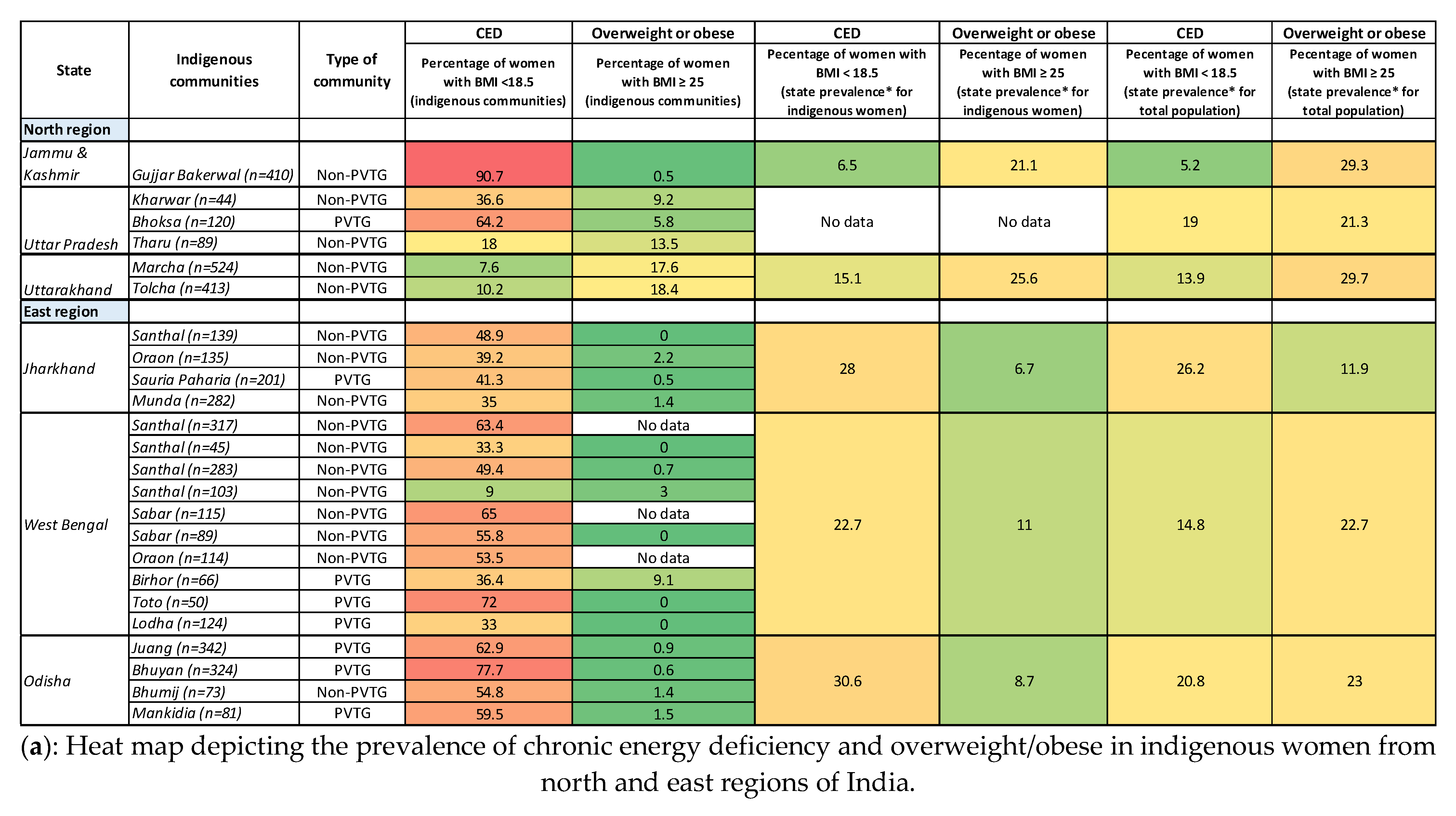
3.5. Nutritional Status of Indigenous Women in India
4. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kuhnlein, H.V.; Erasmus, B.; Spigelski, D.; Burlingame, B. Indigenous Peoples’ Food Systems & Well-Being: Interventions & Policies for Healthy Communities; Food and Agriculture Organization of the United Nations, McGill University, Eds.; Food and Agriculture Organization of the United Nations: Rome, Italy; Centre for Indigenous Peoples’ Nutrition and Environment: Ste-Anne-de-Bellevue, QC, Canada, 2013; ISBN 978-92-5-107433-6. [Google Scholar]
- Census of India Website: Office of the Registrar General & Census Commissioner, India. 2011. Available online: http://censusindia.gov.in/ (accessed on 29 September 2019).
- World Bank. India: Food Security and Nutrition in Tribal Areas; World Bank: Washington, DC, USA, 2014. [Google Scholar]
- Ministry of Tribal Affairs, Government of India. Available online: https://tribal.nic.in/ (accessed on 14 June 2020).
- Ministry of Tribal Affairs. Annual Report 2021–2022; Ministry of Tribal Affairs, Government of India: New Delhi, India, 2022.
- MoHFW; Ministry of Tribal Affairs. Tribal Health in India: Bridging the Gap and a Roadmap for the Future; Ministry of Health and Family Welfare & Minsitry of Tribal Affairs, Government of India: New Delhi, India, 2019.
- Negi, D.P.; Singh, D.M.M. Tribal Health in India: A Need For a Comprehensive Health Policy. Int. J. Health Sci. 2019, 9, 299–305. [Google Scholar]
- Ghosh-Jerath, S.; Kapoor, R.; Barman, S.; Singh, G.; Singh, A.; Downs, S.; Fanzo, J. Traditional Food Environment and Factors Affecting Indigenous Food Consumption in Munda Tribal Community of Jharkhand, India. Front. Nutr. 2021, 7, 357. [Google Scholar] [CrossRef]
- Ghosh-Jerath, S.; Kapoor, R.; Singh, A.; Downs, S.; Barman, S.; Fanzo, J. Leveraging Traditional Ecological Knowledge and Access to Nutrient-Rich Indigenous Foods to Help Achieve SDG 2: An Analysis of the Indigenous Foods of Sauria Paharias, a Vulnerable Tribal Community in Jharkhand, India. Front. Nutr. 2020, 7, 61. [Google Scholar] [CrossRef] [PubMed]
- Ghosh-Jerath, S.; Singh, A.; Magsumbol, M.S.; Kamboj, P.; Goldberg, G. Exploring the Potential of Indigenous Foods to Address Hidden Hunger: Nutritive Value of Indigenous Foods of Santhal Tribal Community of Jharkhand, India. J. Hunger Environ. Nutr. 2016, 11, 548–568. [Google Scholar] [CrossRef] [Green Version]
- NNMB. Diet and Nutritional Status of Tribal Population and Prevalence of Hypertension among Adults; National Institute of Nutrition, Indian Council of Medical Research: Hyderabad, India, 2009. [Google Scholar]
- NIN. Dietary Guidelines for Indians—A Manual; National Institute of Nutrition, Indian Council of Medical Research: Hyderabad, India, 2011. [Google Scholar]
- Mandal, P. Tribal Life in India: Defining, Structure and other Details. Available online: https://www.yourarticlelibrary.com/tribes/tribal-life-in-india-defining-structure-and-other-details/35161 (accessed on 15 June 2022).
- Bhasin, V. Status of Tribal Women in India. Stud. Home Community Sci. 2007, 1, 1–16. [Google Scholar] [CrossRef]
- Mitra, A. The status of women among the scheduled tribes in India. J. Socio-Econ. 2008, 37, 1202–1217. [Google Scholar] [CrossRef]
- Sharma, K. Gender Dimensions of Poverty and Food Security: A Case Study of Palamu District of Jharkhand. Indian J. Public Adm. 2019, 65, 171–188. [Google Scholar] [CrossRef]
- Agrawal, P.K.; Agrawal, S. To what extent are the indigenous women of Jharkhand, India living in disadvantageous conditions: Findings from India’s National Family Health Survey. Asian Ethn. 2010, 11, 61–80. [Google Scholar] [CrossRef]
- Agrawal, S. Disadvantageous situation of tribal women and children of Orissa, India: A special reference to their health and nutritional status. J. Community Nutr. Health 2013, 2, 3–14. [Google Scholar]
- UNICEF. Maternal and Perinatal Death Inquiry and Response; UNICEF: New Delhi, India, 2009. [Google Scholar]
- International Institute of Population Sciences (IIPS) National Family Health Survey (NFHS-5), 2019–2021; IIPS: Mumbai, India, 2022.
- ICMR-NIN. Nutrient Requirements for Indians: A Report of the Expert Group, 2020; ICMR-National Institute of Nutrition, Department of Health Research, Ministry of Health and Family Welfare, Government of India: Hyderabad, India, 2020.
- Torheim, L.E.; Ferguson, E.L.; Penrose, K.; Arimond, M. Women in Resource-Poor Settings Are at Risk of Inadequate Intakes of Multiple Micronutrients. J. Nutr. 2010, 140, 2051S–2058S. [Google Scholar] [CrossRef] [Green Version]
- James, W.P.; Ferro-Luzzi, A.; Waterlow, J.C. Definition of chronic energy deficiency in adults. Report of a working party of the International Dietary Energy Consultative Group. Eur. J. Clin. Nutr. 1988, 42, 969–981. [Google Scholar] [PubMed]
- WHO Expert Consultation Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet Lond. Engl. 2004, 363, 157–163. [CrossRef] [PubMed]
- Ghosh-Jerath, S.; Kapoor, R.; Bandhu, A.; Singh, A.; Downs, S.; Fanzo, J. Indigenous Foods to Address Malnutrition: An Inquiry into the Diets and Nutritional Status of Women in the Indigenous Community of Munda Tribes of Jharkhand, India. Curr. Dev. Nutr. 2022, 6, nzac102. [Google Scholar] [CrossRef] [PubMed]
- Chyne, D.A.L.; Meshram, I.I.; Rajendran, A.; Kodali, V.; Getti, N.; Roy, P.; Kuhnlein, H.V.; Longvah, T. Nutritional status, food insecurity, and biodiversity among the Khasi in Meghalaya, North-East India. Matern. Child. Nutr. 2017, 13 (Suppl. 3), e12557. [Google Scholar] [CrossRef] [Green Version]
- Chishty, S.; Singh, N. Nutritional status of tribal women (Saharia and Meena), Baran district of Rajasthan, India. Nutr. Food Sci. 2018, 48, 922–939. [Google Scholar] [CrossRef]
- Padmavathi, C.; Ramadas, V.S. Impact of education programme among the irula tribals at neelampathy. Int. J. Food Nutr. Sci. 2012, 1, 42–51. [Google Scholar]
- Sujatha, P. Analysis of nutrition and reproductive health status of tribal women in Kancheepuram District. Int. J. Res. Humanit. Sci. 2017, 2, 95–101. [Google Scholar]
- Ghosh-Jerath, S.; Kapoor, R.; Singh, A.; Downs, S.; Goldberg, G.; Fanzo, J. Agroforestry diversity, indigenous food consumption and nutritional outcomes in Sauria Paharia tribal women of Jharkhand, India. Matern. Child. Nutr. 2020, 17, e13052. [Google Scholar] [CrossRef]
- Pingali, P.; Mittra, B.; Rahman, A. The bumpy road from food to nutrition security—Slow evolution of India’s food policy. Glob. Food Secur. 2017, 15, 77–84. [Google Scholar] [CrossRef]
- Desai, S.; Vanneman, R. Enhancing Nutrition Security via India’s National Food Security Act: Using an Axe instead of a Scalpel? India Policy Forum Pap. India Policy Forum Conf. 2015, 11, 67. [Google Scholar]
- Ellena, R.; Nongkynrih, K.A. Changing gender roles and relations in food provisioning among matrilineal Khasi and patrilineal Chakhesang Indigenous rural People of North-East India. Matern. Child. Nutr. 2017, 13, e12560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Welthungerlife India: Making Food a Right for All. Available online: https://www.globalhungerindex.org/case-studies/2016-india.html (accessed on 28 September 2019).
- Raghunathan, K.; Headey, D.; Herforth, A. Affordability of nutritious diets in rural India. Food Policy 2021, 99, 101982. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.; Sunder, N.; Pingali, P.L. Are Women in Rural India Really Consuming a Less Diverse Diet? Food Nutr. Bull. 2020, 41, 318–331. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.; Pingali, P.L.; Pinstrup-Andersen, P. Women’s empowerment in Indian agriculture: Does market orientation of farming systems matter? Food Secur. 2017, 9, 1447–1463. [Google Scholar] [CrossRef] [Green Version]
- Devi, P.; Suresh Kumar, P. Traditional, ethnic and fermented foods of different tribes of Manipur. IJTK 2012, 11, 70–77. [Google Scholar]
- Tamang, J.P.; Thapa, N. Some nonfermented ethnic foods of Sikkim in India. J. Ethn. Foods 2014, 1, 29–33. [Google Scholar] [CrossRef]
- Mao, A.A.; Odyuo, N. Traditional fermented foods of the Naga tribes of Northeastern, India. Indian J. Tradit. Knowl. 2007, 6, 37–41. [Google Scholar]
- Das, G.; Patra, J.K.; Singdevsachan, S.K.; Gouda, S.; Shin, H.-S. Diversity of traditional and fermented foods of the Seven Sister states of India and their nutritional and nutraceutical potential: A review. Front. Life Sci. 2016, 9, 292–312. [Google Scholar] [CrossRef] [Green Version]
- Govindasamy, K.; Banerjee, B.B.; Milton, A.A.P.; Katiyar, R.; Meitei, S. Meat-based ethnic delicacies of Meghalaya state in Eastern Himalaya: Preparation methods and significance. J. Ethn. Foods 2018, 5, 267–271. [Google Scholar] [CrossRef]
- Ghosh-Jerath, S.; Singh, A.; Magsumbol, M.S.; Lyngdoh, T.; Kamboj, P.; Goldberg, G. Contribution of indigenous foods towards nutrient intakes and nutritional status of women in the Santhal tribal community of Jharkhand, India. Public Health Nutr. 2016, 19, 2256–2267. [Google Scholar] [CrossRef] [Green Version]
- Ghosh-Jerath, S.; Singh, A.; Lyngdoh, T.; Magsumbol, M.S.; Kamboj, P.; Goldberg, G. Estimates of Indigenous Food Consumption and Their Contribution to Nutrient Intake in Oraon Tribal Women of Jharkhand, India. Food Nutr. Bull. 2018, 39, 581–594. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deol, T. No Meat, More Wheat: How Tribal Diets Are Changing in Madhya Pradesh. Available online: https://www.downtoearth.org.in/news/food/no-meat-more-wheat-how-tribal-diets-are-changing-in-madhya-pradesh-82878 (accessed on 17 May 2022).
- Jadhav, A. The Dilemma of Drink in India’s Tribal Areas. Available online: https://www.downtoearth.org.in/blog/health/the-dilemma-of-drink-in-india-s-tribal-areas-67407#:~:text=There%20is%20a%20belief%20among,flowers%20to%20local%20alcohol%20makers (accessed on 24 October 2019).
- Phansalkar, S. Dairy Farming in Tribal Regions Holds Enormous Promise. Available online: https://www.villagesquare.in/dairy-farming-in-tribal-regions-holds-enormous-promise/#:~:text=Dairy%20industry%20does%20provide%20huge,them%20and%20for%20the%20country (accessed on 24 April 2019).
- Kasimba, S.; Covic, N.; Motswagole, B.; Laubscher, R.; Claasen, N. Consumption of Traditional and Indigenous Foods and Their Contribution to Nutrient Intake among Children and Women in Botswana. Ecol. Food Nutr. 2019, 58, 281–298. [Google Scholar] [CrossRef] [PubMed]
- Kuhnlein, H. Why Are Indigenous Peoples’ Food Systems Important and Why Do They Need Documentation? In Indigenous Peoples’ Food Systems: The Many Dimensions of Culture, Diversity and Environment for Nutrition and Health; Food and Agriculture Organization of the United Nations; Centre for Indigenous Peoples’ Nutrition and Environment: Rome, Italy, 2009; pp. 1–7. [Google Scholar]
- Settee, P.; Shukla, S. Indigenous Food Systems: Concepts, Cases, and Conversations; Canadian Scholars: Toronto, ON, Canada, 2020; ISBN 978-1-77338-109-1. [Google Scholar]
- Kapoor, R.; Sabharwal, M.; Ghosh-Jerath, S. Indigenous Foods of India: A Comprehensive Narrative Review of Nutritive Values, Antinutrient Content and Mineral Bioavailability of Traditional Foods Consumed by Indigenous Communities of India. Front. Sustain. Food Syst. 2022, 6, 696228. [Google Scholar] [CrossRef]
- Ghosh-Jerath, S.; Singh, A.; Kamboj, P.; Goldberg, G.; Magsumbol, M.S. Traditional Knowledge and Nutritive Value of Indigenous Foods in the Oraon Tribal Community of Jharkhand: An Exploratory Cross-sectional Study. Ecol. Food Nutr. 2015, 54, 493–519. [Google Scholar] [CrossRef] [Green Version]
- Bhattacharjee, L.; Kothari, G.; Priya, V.; Nandi, B.K. The Bhil Food System: Links to Food Security, Nutrition and Health. In Indigenous Peoples’ Food Systems: The Many Dimensions of Culture, Diversity and Environment for Nutrition and Health; Food and Agriculture Organization of the United Nations; Centre for Indigenous Peoples’ Nutrition and Environment: Rome, Italy, 2009; pp. 209–230. [Google Scholar]
- Mishra, A. Shift in Tribal Food Habits: From Sustainable to Non-Sustainable. Available online: https://www.pradan.net/sampark/wp-content/uploads/2019/09/Shift-in-Tribal-Food-Habits-From-Sustainable-to-Nonsustainable.pdf (accessed on 2 September 2017).
- David, P. In the Nilgiris, an Inheritance of Malnutrition. Available online: https://ruralindiaonline.org/en/articles/in-the-nilgiris-an-inheritance-of-malnutrition/#:~:text=A%20malnourished%20mother%20will%20produce,the%20next%20generation%20of%20Adivasis.%E2%80%9D (accessed on 1 May 2022).
- FAARM. Project—Living Farms. Available online: https://livingfarms.wordpress.com/project-overview/ (accessed on 4 June 2022).
- VAAGDHARA. Tribal Women Are Using Indigenous Seeds to Fight Climate Change & Sustain Their Livelihood. Available online: https://vaagdhara.org/tribal-women-using-indigenous-seeds-to-fight-climate-change/#:~:text=%E2%9C%95-,Tribal%20women%20are%20using%20indigenous%20seeds,climate%20change%20%26%20sustain%20their%20livelihood&text=Green%20revolution%20that%20began%20in,high%20yielding%20varieties%20of%20crops (accessed on 25 June 2022).
- Mission for Integrated Development of Horticulture (MIDH). Available online: https://midh.gov.in/ (accessed on 24 February 2021).
- MoWCD. Bharatiya POSHAN Krishi Kosh. Available online: Pib.gov.in/Pressreleaseshare.aspx?PRID=1595250 (accessed on 6 March 2021).
- Sonne, L. The Policy Environment for Food, Agriculture and Nutrition in India:Taking Stock and Looking Forward. Available online: https://opendocs.ids.ac.uk/opendocs/bitstream/handle/20.500.12413/13096/Policy_environment_for_food_agriculture_and_nutrition_in_India.pdf?sequence=1&isAllowed=y (accessed on 15 July 2017).
- FAO. Minimum Dietary Diversity for Women; FAO: Rome, Italy, 2021. [Google Scholar]
- Nongrum, M.S.; Pawera, L.; Mawroh, B. Dietary diversity and its determinants among Khasi and Garo indigenous women (15 to 49 years) in Meghalaya, northeast India. Nutr. Health 2021, 28, 249–256. [Google Scholar] [CrossRef] [PubMed]
- Pandey, D.K.; Momin, K.C.; Dubey, S.K.; Adhiguru, P. Biodiversity in agricultural and food systems of jhum landscape in the West Garo Hills, North-eastern India. Food Secur. 2022, 14, 791–804. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.; Sunder, N.; Pingali, P.L. Market Access, Production Diversity, and Diet Diversity: Evidence From India. Food Nutr. Bull. 2020, 41, 167–185. [Google Scholar] [CrossRef] [PubMed]
- Longvah, T.; Khutsoh, B.; Meshram, I.I.; Krishna, S.; Kodali, V.; Roy, P.; Kuhnlein, H.V. Mother and child nutrition among the Chakhesang tribe in the state of Nagaland, North-East India. Matern. Child. Nutr. 2017, 13 (Suppl. 3), e12558. [Google Scholar] [CrossRef] [Green Version]
- Singh, S.; Singh, L.B.; Singh, D.R.; Chand, S.; Zamir Ahmed, S.K.; Singh, V.N.; Dam Roy, S. Indigenous underutilized vegetables for food and nutritional security in an island ecosystem. Food Secur. 2018, 10, 1173–1189. [Google Scholar] [CrossRef]
- Bhagowalia, P.; Headey, D.; Kadiyala, S. Agriculture, Income, and Nutrition Linkages in India: Insights from a Nationally Representative Survey; IFPRI Discussion Paper: Washington, DC, USA, 2012. [Google Scholar]
- Nandi, R.; Nedumaran, S.; Ravula, P. The interplay between food market access and farm household dietary diversity in low and middle income countries: A systematic review of literature. Glob. Food Secur. 2021, 28, 100484. [Google Scholar] [CrossRef]
- Ludwig, T. An Egg for an Egg and a Bean for a Bean? How Production Diversity Determines Dietary Diversity of Smallholder Farmers in Rural India; ZEF—Discussion Papers on Development Policy No. 247; Center for Development Research: Bonn, Germany, 2018. [Google Scholar]
- Swaminathan, S.; Vaz, M.; Kurpad, A.V. Protein intakes in India. Br. J. Nutr. 2012, 108, S50–S58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamid, T.; Vaida, N. A study on nutritional status of scheduled tribe (Gujjar and Bakerwal) women of Kashmir. Int. J. Home Sci. 2017, 3, 203–205. [Google Scholar]
- Wani, M.; Jan, S. A study on nutritional and health status of adult Gujjar women of Bandipora district of Kashmir. Int. J. Home Sci. 2016, 2, 332–335. [Google Scholar]
- Das, M. Study of Nutritional Status of Korku Tribes in Betul District of Madhya Pradesh. Stud. Tribes Tribals 2010, 8, 31–36. [Google Scholar] [CrossRef]
- Lamba, A.; Garg, V. Nutrition Profile of the Tribal (Bhoksa) Women in Bijnor District, Uttar Pradesh. Int. J. Sci. Res. (IJSR) 2018, 7, 82–84. [Google Scholar]
- Meshram, I.; Balakrishna, N.; Sreeramakrishna, K.; Rao, K.M.; Kumar, R.H.; Arlappa, N.; Manohar, G.; Reddy, C.G.; Ravindranath, M.; Kumar, S.S.; et al. Trends in nutritional status and nutrient intakes and correlates of overweight/obesity among rural adult women (≥18–60 years) in India: National Nutrition Monitoring Bureau (NNMB) national surveys. Public Health Nutr. 2016, 19, 767–776. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- International Institute of Population Sciences (IIPS). National Family Health Survey (NFHS-4), 2015–2016; IIPS: Mumbai, India, 2017. [Google Scholar]
- Gulati, A.; Roy, R. Linkage Between Agriculture, Poverty and Malnutrition in India. In Revitalizing Indian Agriculture and Boosting Farmer Incomes; Gulati, A., Roy, R., Saini, S., Eds.; Springer: Singapore, 2021; pp. 39–74. ISBN 9789811593352. [Google Scholar]
- Varadharajan, K.S.; Thomas, T.; Kurpad, A.V. Poverty and the state of nutrition in India. Asia Pac. J. Clin. Nutr. 2013, 22, 326–339. [Google Scholar] [CrossRef]
- Pankaj, A.; Tankha, R. Empowerment Effects of the NREGS on Women Workers: A Study in Four States. Econ. Polit. Wkly. 2010, 45, 45–55. [Google Scholar]
- Breitkreuz, R.; Stanton, C.-J.; Brady, N.; Pattison-Williams, J.; King, E.D.; Mishra, C.; Swallow, B. The Mahatma Gandhi National Rural Employment Guarantee Scheme: A Policy Solution to Rural Poverty in India? Dev. Policy Rev. 2017, 35, 397–417. [Google Scholar] [CrossRef] [Green Version]
- Ghosh, J. Assessing poverty Alleviation Strategies for their impact on Poor Women: A Study with Special Reference to India. Soc. Chang. 1999, 29, 333–334. [Google Scholar] [CrossRef]
- Sudarshan, R.M.; Bhattacharya, R.; Fernandez, G. Women’s Participation in the NREGA: Some Observations from Fieldwork in Himachal Pradesh, Kerala and Rajasthan. IDS Bull. 2010, 41, 77–83. [Google Scholar] [CrossRef]
- Vemireddy, V.; Pingali, P.L. Seasonal time trade-offs and nutrition outcomes for women in agriculture: Evidence from rural India. Food Policy 2021, 101, 102074. [Google Scholar] [CrossRef] [PubMed]
- Toppo, S. A comparative study on health status of Oraon and Munda rural areas Tribal women. Food Sci. Res. J. 2016, 7, 250–258. [Google Scholar] [CrossRef]
- Ghosh-Jerath, S.; Singh, A.; Bhattacharya, A.; Ray, S.; Yunus, S.; Zodpey, S.P. Dimensions of nutritional vulnerability: Assessment of women and children in Sahariya tribal community of Madhya Pradesh in India. Indian J. Public Health 2013, 57, 260. [Google Scholar] [CrossRef]
- Garnaik, D.; Devadarshini, C.; Jena, D. Nutritional status of tribal women of Kandhamal district, Odisha. Pharma Innov. J. 2019, 8, 105–107. [Google Scholar]
- Dash, K.; Adhikari, A. Comparison of nutritional status between Santal tribal women and Bengali women of Purba Medinipur, West Bengal. Indian J. Biol. Sci. 2017, 23, 24–33. [Google Scholar]
- Hebert, J.R.; Gupta, P.C.; Bhonsle, R.B.; Murti, P.R.; Mehta, H.; Verghese, F.; Aghi, M.; Krishnaswamy, K.; Mehta, F.S. Development and testing of a quantitative food frequency questionnaire for use in Kerala, India. Public Health Nutr. 1998, 1, 123–130. [Google Scholar] [CrossRef] [Green Version]
- Goswami, M. Body Mass Index and Chronic Energy Deficiency of Adult Bhuyans: A Vulnerable Tribal Group of Keonjhar and Anugul Districts of Odisha, India. Indian J. Phys. Anthropol. Hum. Genet. 2012, 31, 39–47. [Google Scholar]
- Goswami, M. Anthropometric Characteristics and Chronic Energy Deficiency of the Mankidias—A PTG of Northern Odisha, India. Stud. Tribes Tribals 2015, 13, 88–93. [Google Scholar] [CrossRef]
- Kanrar, P.; Goswami, M. Sociodemographic Profile, Reproductive Health and Nutritional Status Among the Juangs—A Particularly Vulnerable Tribal Group of Odisha, India. Orient. Anthropol. 2020, 20, 135–149. [Google Scholar] [CrossRef]
- Sengupta, P. Capsulation of the global fitness status and body composition of the young Toto women: The smallest tribal community of India. Perform. Enhanc. Health 2016, 5, 4–9. [Google Scholar] [CrossRef]
- Deo, M.G.; Pawar, P.V.; Kanetkar, S.R.; Kakade, S.V. Prevalence and risk factors of hypertension and diabetes in the Katkari tribe of coastal Maharashtra. J. Postgrad. Med. 2017, 63, 106–113. [Google Scholar] [CrossRef] [PubMed]
- Bharali, N.; Mondal, N.; Singh, K.N. Prevalence of Undernutrition, Overweight and Obesity among Nyishi tribal women of Arunachal Pradesh, Northeast India. Hum. Biol. Rev. 2017, 6, 63–78. [Google Scholar]
- Barbhuïya, A.F.G.İ.; Das, R. Gender differences in nutritional status among the adult Meiteis of Cachar district of Assam, India. Eurasian J. Anthropol. 2014, 4, 36–44. [Google Scholar]
- Mungreiphy, N.K.; Kapoor, S. Socioeconomic changes as covariates of overweight and obesity among Tangkhul Naga tribal women of Manipur, north-east India. J. Biosoc. Sci. 2010, 42, 289–305. [Google Scholar] [CrossRef]
- Damman, S.; Eide, W.B.; Kuhnlein, H.V. Indigenous peoples’ nutrition transition in a right to food perspective. Food Policy 2008, 33, 135–155. [Google Scholar] [CrossRef]
- Fernández, C.I. Nutrition Transition and Health Outcomes Among Indigenous Populations of Chile. Curr. Dev. Nutr. 2020, 4, nzaa070. [Google Scholar] [CrossRef] [Green Version]
- McCartan, J.; van Burgel, E.; McArthur, I.; Testa, S.; Thurn, E.; Funston, S.; Kho, A.; McMahon, E.; Brimblecombe, J. Traditional Food Energy Intake among Indigenous Populations in Select High-Income Settler-Colonized Countries: A Systematic Literature Review. Curr. Dev. Nutr. 2020, 4, nzaa163. [Google Scholar] [CrossRef]
- Bhandari, S.; Ghosh, M.; Bose, K. Socio-demographic characteristics and prevelance of undernutrition among adult Sabars of Bankura District, West Bengal, India. Int. J. Adv. Life Sci. Res. 2019, 2, 1–10. [Google Scholar] [CrossRef]
- Das, S.; Bose, K. Body Mass Index and Chronic Energy Deficiency among Adult Santals of Purulia District, West Bengal, India. J. Hum. Sci. 2010, 7, 488–503. [Google Scholar]
- Das, S.; Mahata, M. Nutritional profile of adult Birhors of Purulia: A Particularly Vulnerable Tribal Group of, West Bengal, India. Asian Acad. Res. J. Multidiscip. 2013, 1, 262–276. [Google Scholar]
- Ghosh, M.; Bhandari, S.; Bose, K. Anthropometric Characteristics and Nutritional Status of Adult Sabars of Bankura District, West Bengal. Hum. Biol. Rev. 2018, 7, 13. [Google Scholar]
- Goswami, M.; Dash, B.; Dash, N.C. Nutritional Status of the Bhumija of Baleswar, Orissa. Indian Anthropol. 2010, 40, 55–70. [Google Scholar] [CrossRef]
- Jaiswal, A. A Study on Body Mass Index and Prevalence of Chronic Energy Deficiency among Adult Kharwar Tribes of India. Glob. J. Anthropol. Res. 2015, 2, 50–55. [Google Scholar] [CrossRef]
- Sarmah, C. Ageing and Nutritional Status among Three Communities 51 of Lakhimpur District, Assam. Indian J. Gerontol. 2014, 28, 51–69. [Google Scholar]
- Oniang’o, R.; Mukudi, E. Nutrition and Gender; Nutrition: A Foundation for Development: Geneva, Switzerland, 2002. [Google Scholar]
- Ministry of Tribal Affairs. Annual Report 2019-2020; Ministry of Tribal Affairs, Government of India: New Delhi, India, 2020.
- Bellamy, C. The State of the World’s Children; UNICEF: New York, NY, USA, 1998; ISBN 978-0-19-829401-6. [Google Scholar]
- NITI Aayog. Nourishing India-National Nutrition Strategy; NITI Aayog: New Delhi, India, 2017. [Google Scholar]
- Sethi, V.; Bhattacharjee, S.; Sinha, S.; Daniel, A.; Lumba, A.; Sharma, D.; Bhanot, A. Delivering Essential Nutrition: Interventions for Women in Tribal Pockets of Eastern India. Econ. Polit. Wkly. 2019, 54, 43–51. [Google Scholar]
- Shrivastava, S. Why Undernutrition Persists in India’s Tribal Population. Available online: https://thewire.in/health/why-undernutrition-persists-in-indias-tribal-population (accessed on 25 September 2018).
- Ministry of Tribal Affairs. ALEKH-A Learning Endeavour for Knowledge in Healthcare; Ministry of Tribal Affairs, Government of India: New Delhi, India, 2020.
- Narain, J.P. Health of tribal populations in India: How long can we afford to neglect? Indian J. Med. Res. 2019, 149, 313–316. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine. Dietary Reference Intakes: Applications in Dietary Assessment; National Academies Press: Washington, DC, USA, 2000; ISBN 978-0-309-07183-3. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Tribe | N | EAR a | Energy (kcal/d) | Protein (g/d) | Vitamin A (µg/d) | Vitamin C (mg/d) | Thiamine (mg/d) | Riboflavin (mg/d) | Niacin (mg/d) | Folate (µg/d) | Vitamin B12 (mg/d) | Iron (mg/d) | Calcium (mg/d) | Zinc (mg/d) | Dietary Assessment Method | Random Sample |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 2130 | 36 | 390 | 55 | 1.4 | 2 | 12 | 180 | 2 | 15 | 800 | 11 | |||||
| Jammu & Kashmir | ||||||||||||||||
| Gujjar Bakerwal [71] | 410 | Mean | 1421 | 40.2 | - | - | - | - | - | - | - | 7.9 | 277 | - | 1 | No |
| SD | 264 | 7.3 | 2.3 | 152.9 | ||||||||||||
| Gujjar [72] | 50 | Mean | 1862 | 39.4 | - | - | - | - | - | - | - | 7.8 | 337.3 | - | 1 | No |
| SD | 1461 | 12.8 | 4.4 | 292.6 | ||||||||||||
| Jharkhand | ||||||||||||||||
| Santhal [43] | 147 | Mean | 1969 | 43.5 | 923.5 | 98.9 | 0.9 | 0.6 | 20.9 | 85.8 | 0.2 | 13.9 | 325.3 | 7.8 | 1 | Yes |
| SD | 778 | 18.9 | 1364.8 | 115.9 | 0.6 | 0.3 | 8.7 | 65.9 | 0.1 | 18.9 | 578.1 | 3.2 | ||||
| Oraon [44] | 138 | Mean | 2365 | 58.3 | 146.4 | 61.6 | 0.7 | 0.6 | 27.2 | 100 | 0.1 | 10.1 | 277.3 | 9.6 | 1 | Yes |
| SD | 918 | 40.3 | 207.6 | 46.5 | 0.3 | 0.3 | 13.7 | 56.4 | 0.5 | 8.9 | 171.03 | 3.8 | ||||
| Oraon [84] | 100 | Mean | 2092 | 41.2 | 219 | 25.5 | - | - | - | - | - | 20.5 | 288.7 | - | 1 | Yes |
| SD | 34 | 4.03 | 2.03 | 1.63 | - | - | - | - | - | 1.4 | 7.1 | - | ||||
| Munda [84] | 100 | Mean | 2179 | 38.9 | 231.2 | 27.5 | - | - | - | - | - | 21.6 | 305.5 | - | 1 | Yes |
| SD | 38 | 4.9 | 10.2 | 1.4 | - | - | - | - | - | 1.1 | 3.2 | - | ||||
| Munda [25] | 282 | Mean | 1495 | 35.6 | 68.7 | 48.9 | 0.5 | 0.4 | 7.2 | 114.2 | - | 7 | 120.7 | 5.6 | 1 | Yes |
| SD | 269.3 | 5.3 | 34.7 | 9 | 0.5 | 0.2 | 1.5 | 13.9 | - | 1.7 | 7.6 | 1 | ||||
| Sauria Paharia [30] | 204 | Mean | 1092 | 31.6 | 15.7 | 12.4 | 0.3 | 0.2 | 5.3 | 79.4 | - | 5.2 | 90.6 | 4.4 | 1 | Yes |
| SD | 86.3 | 3.5 | 27.6 | 82.8 | 0.1 | 0.1 | 0.7 | 22.9 | - | 1.5 | 19.4 | 0.6 | ||||
| Madhya Pradesh | ||||||||||||||||
| Saharia [85] | 209 | Mean | 1478 | 51.7 | 45 (20, 79) * | 6 (2, 13) * | 1.9 | 0.7 | 17.3 | 55.2 | - | 20.5 | 254 | - | 1 | Yes |
| Korku [73] | 602 | Mean | 1822 | 37.7 | 93 | 16.9 | 0.7 | 0.6 | 9.2 | - | - | 15.7 | 170.3 | - | 2 | No |
| Meghalaya | ||||||||||||||||
| Khasi [26] | 47 | Mean | 1890 | 59.2 | 191.2 | 33.4 | 0.7 | 0.5 | 13.1 | - | - | 13.8 | 322.8 | - | 1 | Yes |
| SD | 438.3 | 29.3 | 279 | 31.7 | 0.4 | 0.2 | 3.9 | 10.9 | 385.2 | |||||||
| Odisha | ||||||||||||||||
| Desia Khond [86] | 80 | Mean | 2225 | 33.46 | 134.5 | 10.1 | 0.9 | 0.6 | 10.7 | 47.4 | 0.15 | 13.7 | 195.3 | 4.8 | 1 | Yes |
| SD | 262 | 11.17 | 228 | 15.6 | 0.3 | 0.53 | 6.6 | 15.1 | 0.42 | 4.9 | 56.7 | 1.3 | ||||
| Rajasthan | ||||||||||||||||
| Saharia [27] | 93 | Mean | 1335 | 42.2 | 291 | 23.4 | 1.6 | 0.7 | 13.1 | 168 | 0.5 | 16.1 | 438.5 | 6.9 | 1 | No |
| SD | 287 | 10.4 | 281 | 19.5 | 0.4 | 0.2 | 3.3 | 54 | 0.1 | 4.7 | 154.3 | 1.9 | ||||
| Meena [27] | 92 | Mean | 1386 | 44.4 | 442 | 26.1 | 1.5 | 0.8 | 12.8 | 166.9 | 0.2 | 15.3 | 531.2 | 6.7 | 1 | No |
| SD | 252 | 8.2 | 397 | 18.9 | 0.1 | 0.2 | 2.3 | 60.3 | 0.1 | 3.2 | 203.5 | 1.3 | ||||
| Tamil Nadu | ||||||||||||||||
| Irula [28] | 30 | Mean | 1830 | 35.2 | 558 | 20 | 0.4 | 0.7 | 8 | 48 | - | 12 | 158 | - | 2 | No |
| Uttar Pradesh | ||||||||||||||||
| Bhoksa [74] | 120 | Mean | 1638 | 42.4 | - | - | - | - | - | - | - | 13.8 | 335 | - | 1 | Yes |
| SD | 243 | 6.81 | 2.8 | 176.4 | ||||||||||||
| West Bengal | ||||||||||||||||
| Santhal [87] | 45 | Mean | 2180 | 18 | - | - | - | - | - | - | - | - | - | - | 3 | Yes |
| SD | 472 | 2 | - | - | - | - | - | - | - | - | - | - | ||||
| Tribe | Energy | Protein | Vitamin A | Vitamin C | Thiamine | Riboflavin | Niacin | Folate | Vitamin B12 | Iron | Calcium | Zinc |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Jammu & Kashmir | ||||||||||||
| Gujjar Bakerwal [71] | High risk | Low risk | No data | No data | No data | No data | No data | No data | No data | High risk | High risk | No data |
| Gujjar [72] | High risk | Low risk | No data | No data | No data | No data | No data | No data | No data | High risk | High risk | No data |
| Jharkhand | ||||||||||||
| Santhal [43] | High risk | Low risk | Low risk | Low risk | High risk | High risk | Low risk | High risk | High risk | High risk | High risk | High risk |
| Oraon [44] | Low risk | Low risk | High risk | Low risk | High risk | High risk | Low risk | High risk | High risk | High risk | High risk | High risk |
| Oraon [84] | High risk | Low risk | High risk | High risk | No data | No data | No data | No data | No data | Low risk | High risk | No data |
| Munda [84] | Low risk | Low risk | High risk | High risk | No data | No data | No data | No data | No data | Low risk | High risk | No data |
| Munda [25] | High risk | High risk | High risk | High risk | High risk | High risk | High risk | High risk | High risk | High risk | High risk | |
| Sauria Paharia [30] | High risk | High risk | High risk | High risk | High risk | High risk | High risk | High risk | High risk | High risk | High risk | |
| Madhya Pradesh | ||||||||||||
| Saharia [85] | High risk | Low risk | High risk | High risk | Low risk | High risk | Low risk | High risk | No data | Low risk | High risk | No data |
| Korku [73] | High risk | Low risk | High risk | High risk | High risk | High risk | High risk | No data | No data | Low risk | High risk | No data |
| Meghalaya | ||||||||||||
| Khasi [26] | High risk | Low risk | High risk | High risk | High risk | High risk | Low risk | No data | No data | High risk | High risk | No data |
| Odisha | ||||||||||||
| Desia Khond [86] | Low risk | High risk | High risk | High risk | High risk | High risk | High risk | High risk | High risk | High risk | High risk | High risk |
| Rajasthan | ||||||||||||
| Saharia [27] | High risk | Low risk | High risk | High risk | Low risk | High risk | Low risk | High risk | High risk | Low risk | High risk | High risk |
| Meena [27] | High risk | Low risk | Low risk | High risk | Low risk | High risk | Low risk | High risk | High risk | Low risk | High risk | High risk |
| Tamil Nadu | ||||||||||||
| Irula [28] | High risk | High risk | Low risk | High risk | High risk | High risk | High risk | High risk | No data | High risk | High risk | High risk |
| Uttar Pradesh | ||||||||||||
| Bhoksa [74] | High risk | Low risk | No data | No data | No data | No data | No data | No data | No data | High risk | High risk | High risk |
| West Bengal | ||||||||||||
| Santhal [87] | Low risk | High risk | No data | No data | No data | No data | No data | No data | No data | No data | No data | No data |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kapoor, R.; Sabharwal, M.; Ghosh-Jerath, S. Diet Quality, Nutritional Adequacy and Anthropometric Status among Indigenous Women of Reproductive Age Group (15–49 Years) in India: A Narrative Review. Dietetics 2023, 2, 1-22. https://doi.org/10.3390/dietetics2010001
Kapoor R, Sabharwal M, Ghosh-Jerath S. Diet Quality, Nutritional Adequacy and Anthropometric Status among Indigenous Women of Reproductive Age Group (15–49 Years) in India: A Narrative Review. Dietetics. 2023; 2(1):1-22. https://doi.org/10.3390/dietetics2010001
Chicago/Turabian StyleKapoor, Ridhima, Manisha Sabharwal, and Suparna Ghosh-Jerath. 2023. "Diet Quality, Nutritional Adequacy and Anthropometric Status among Indigenous Women of Reproductive Age Group (15–49 Years) in India: A Narrative Review" Dietetics 2, no. 1: 1-22. https://doi.org/10.3390/dietetics2010001